
Abstract
Design
This was a randomised clinical trial (note that the initial screening used a cluster randomised in part design).
Intervention
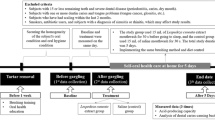
A total of 176 children (7-9 years old) with high MS scores were randomised into equal groups. For 6 months the xylitol group chewed five times during the day, 11.6 grams of a mixed gum containing 36.6% xylitol and other polyols (34.5%). while the control group chewed an identical dose of a non xylitol gum sweetened with a mixture of different polyols (71.1%).
Outcome measure
At baseline, 3 months, 6 months and 9 months (3 months after chewing) children were assessed for both plaque acidogenicity (after sucrose challenge) and salivary MS.
Results
Statistically significant differences were found between both groups at 3, 6 and 9 months, in ‘area under the curve’ (AUC) graphs, with lower plaque pH values in the xylitol group at 3 and 6 months and decreasing difference at 9 months. There was no significant difference between the maximum pH fall in both groups, and only small differences in minimum pH values at 3 and 6 months. There was significantly lower MS level in the xylitol compared with the control group. In addition there was a significant relationship between changes in MS levels, and changes in AUC.
Conclusions
This randomised clinical trial suggests that the use of high-dose xylitol chewing gum has beneficial effects on plaque pH and MS in children at high risk of caries.
Similar content being viewed by others

Commentary
This paper adds to published research1, 2, 3, 4 demonstrating the relationship between xylitol consumption, reductions in plaque acidogenicity and MS levels.
Campus uses MS levels as a measure of dental caries risk and there is good evidence to suggest that MS is a risk factor for both early childhood caries5 and dental caries generally.6 The theory is that by reducing MS levels, dental caries will also be reduced. However the relationship between the presence of MS and caries is still controversial. The recent European Commission regulation (http://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:L:2009:283:0022:0029:EN:PDF) for example ruled that 100% xylitol chewing gum had been shown to reduce plaque, but did not include MS as a stated risk factor. Dental caries is multifactorial, the carious process can occur without these bacteria.7
Xylitol's ability to reduce plaque acidogenesis is important in reducing dental caries risk, as acidogenicity increases the risk of demineralisation.8
In Campus's paper, a mixed xylitol-sorbitol product was used as the intervention product. This differs from comparable studies, where a 100% xylitol product was used.1, 2, 3 Sorbitol is possibly not the ideal control in this type of study as it is not inert, and may actually have a stimulating effect.7, 9 The European Commission has also considered the use of products where xylitol is mixed with other polyols and advised there was insufficient evidence that these mixed products reduced caries.5 The actual product chosen in this study may be one explanation for the although statistically significant, relatively small decrease in MS levels within the xylitol group.
The investigators chose a consumption frequency of five times per day, higher than the more commonly used frequency of three times per day. It is possible that this increased frequency had an effect on compliance.
Any clinical trial needs to reach the standard suggested by the newly updated CONSORT guidelines (www.consort-statement.org). Such transparent reporting is needed to ensure readers can judge the reliability and validity of trial findings.10 Within this study a power calculation was provided, the products were coded to ensure participants and investigators were unaware of allocations. A flow diagram was included accounting for all drop outs and exclusions. Performance bias was avoided due to blinding of products. Retention rates within this study were also very high.
The authors advise that the research was double blinded, but randomisation was performed by the authors. This possible lack of concealment, with no explanation of how the actual random allocation sequence was implemented could have led to selection bias. No registration number or trial registry was provided, nor details of where the full protocol can be accessed. Baseline demographics and clinical characteristics of each group were also not presented. If the screened participants or the actual selected groups were, for example, of differing socio-economic status, this may have implications for the results, (external validity). It is not clear whether the participants were habitual xylitol consumers, which can affect short term studies involving the microbial flora and plaque.11 In order to measure compliance, parents were asked to return empty blister packs, but it may have been of additional use to ask parents to return unused product. P values, the mean and standard error (SE) are presented, but written as mean +/− SE. Presenting results in this manner should perhaps be avoided. By using the +/− symbol it is actually showing a 67% confidence interval, which can add to confusion in the interpretation of results.12
To conclude, this paper provides additional evidence of the efficacy of xylitol in reducing caries risk. It is important for randomised controlled trials to continue to strive to meet all of CONSORT standards, and for studies to demonstrate not only the efficacy of xylitol in reducing risk factors but also in reducing actual dental caries.
Practice points
-
Doses of 5 grams or more of xylitol2, 13 at a frequency of at least three times per day14 can be a useful adjunct to reduce caries risk in children: however its protective effect is lost once chewing is discontinued.
-
MS levels are only part of the dental caries risk. Practitioners should look for well designed randomised controlled trials involving xylitol that demonstrate not only a reduction in caries risk factors, but an actual reduction in tooth decay.
References
Spleith CH, Alkilzy M, Schmitt J, Berndt C, Welk A . Effect of xylitol and sorbitol on plaque acidogenesis. Quintessence Int 2009; 40: 279–285.
Holgerson PL, Stecksén-Blicks C, Sjöström, I, Twetman S . Effect of xylitol-containing chewing gums on interdental plaque-pH in habitual xylitol consumers. Acta Odontol Scand 2005; 63: 233–238.
Söderling E, Mäkinen KK, Chen C-Y, Pape Jr HR, Loesche W, Mäkinen P-L . Effect of sorbitol, xylitol, and xylitol/sorbitol chewing gums on dental plaque. Caries Res 1989; 23: 378–384.
Holgerson PL, Sjöström I, Stecksén-Blicks C, Twetman S . Dental plaque formation and salivary mutans streptococci in schoolchildren after use of xylitol-containing chewing gum. Int J Paediatr Dent 2007; 17: 79–85.
Parisotto TM, Steiner-Oliveira C, Silva CM, Rodrigues LK, Nobre-dos-Santos M . Early childhood caries and mutans streptococci: a systematic review. Oral Health Prev Dent 2010; 8: 59–70.
Tanzer JM, Livingston J, Thompson AM . The microbiology of primary dental caries in humans. J Dent Educ 2001; 65: 1028–1037.
Nyvad B, Kilian M . Microflora associated with experimental root surface caries in humans. Infect Immun 1990; 58: 1628–1633.
Cagetti MG, Campus G, Sale S, Cocco F, Strohmenger L, Lingström P . Association between interdental plaque acidogenicity and caries risk at surface level: a cross sectional study in primary dentition. Int J Paediatr Dent 2010 Aug 20. [Epub ahead of print]
Soderling E . Xylitol, mutans streptococci, and dental plaque. Adv Dent Res 2009; 21: 74–78.
Moher D, Hopewell S, Schulz KF, et al. CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomised trials. Br Med J 2010; 340: c869.
Söderling E, Trahan L, Tammiala-Salonen T, Häkkinen L . Effects of xylitol, xylitol-sorbitol, and placebo chewing gums on the plaque of habitual xylitol consumers. Eur J Oral Sci 1997; 105: 170–177.
Petrie A, Sabin C . Medical statistics at a glance. 3rd ed. Blackwell Publishing 2009.
Milgrom P, Ly KA, Roberts MC, Rothen M, Mueller G, Yamaguchi GK . Mutans streptococcal dose response to xylitol chewing gum. J Dent Res 2006; 85: 177–181.
Ly KA, Milgrom P, Roberts MC, Yamaguchi DK, Rothen M, Mueller G . Linear response of mutans streptococci to increasing frequency of xylitol chewing gum use: a randomized controlled trial. BMC Oral Health 2006; 6: 6.
Author information
Authors and Affiliations
Additional information
Address for correspondence: Dr Guglielmo Campus, Dental Institute, University of Sassari, Sassari, Italy. E-mail: gcampus@uniss.it
Campus G, Cagetti MG, Sacco G, Solinas G, Mastroberardino S. Six months of daily high-dose xylitol in high-risk school children: a randomized clinical trial on plaque pH and salivary mutans streptococci. Caries Res 2009; 43: 455–461.
Rights and permissions
About this article
Cite this article
Duane, B. Xylitol gum, plaque pH and mutans streptococci. Evid Based Dent 11, 109–110 (2010). https://doi.org/10.1038/sj.ebd.6400755
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ebd.6400755
