
Abstract
Knowledge on the molecular mechanisms underlying metastasis colonization in Non-Small Cell Lung Cancer (NSCLC) remains incomplete. A complete overview integrating driver mutations, primary tumour heterogeneity and overt metastasis lacks the dynamic contribution of disseminating metastatic cells due to the inaccessibility to the molecular profiling of Circulating Tumour Cells (CTCs). By combining immunoisolation and whole genome amplification, we performed a global gene expression analysis of EpCAM positive CTCs from advanced NSCLC patients. We identified an EpCAM+ CTC-specific expression profile in NSCLC patients mostly associated with cellular movement, cell adhesion and cell-to-cell signalling mediated by PI3K/AKT, ERK1/2 and NF-kB pathways. NOTCH1 emerged as a driver connecting active signalling pathways, with a reduced number of related candidate genes (NOTCH1, PTP4A3, LGALS3 and ITGB3) being further validated by RT-qPCR on an independent cohort of NSCLC patients. In addition, these markers demonstrated high prognostic value for Progression-Free Survival (PFS). In conclusion, molecular characterization of EpCAM+ CTCs from advanced NSCLC patients provided with highly specific biomarkers with potential applicability as a “liquid biopsy” for monitoring of NSCLC patients and confirmed NOTCH1 as a potential therapeutic target to block lung cancer dissemination.
Similar content being viewed by others


Introduction
Cancer is a major public health concern in developed countries with lung cancer as the leading cause responsible for 19.4% of cancer deaths worldwide1. Of those, Non-Small Cell Lung Cancer (NSCLC) accounts for 85% of all cases and encompasses high genetic and histological heterogeneity2. Clinically, treatment alternatives attains a 54% 5-year survival when disease is localized but only 4% when disease is diagnosed once metastasis has occurred3. In this scenario, and despite of the increase in survival during the last decade due to the incorporation of new drugs and better treatment selection4, NSCLC remains an incurable disease in the metastatic setting. Since more than 58% of patients present locally advanced or metastatic disease at the moment of diagnosis3, strategies to understand and target the metastatic process constitute a priority in NSCLC.
Circulating Tumour Cells (CTCs) represent a principal component of the step-wise process of metastasis in which tumour cells escape from the primary tumour, invade the vascular and lymphatic systems, and incorporate into the circulation. Some of these cells are able to survive in the absence of physical substrate until, eventually, reattach at a distant organ and colonize it. Only recently, expanded CTCs ex vivo from early stage lung cancer have been observed to carry the same genetic alterations as primary tumors5; and when transplanted CTCs have been able to generate new tumour masses in mouse model while maintaining the genetic and biological characteristics of the origin tumor6. Moreover, CTCs enumeration has proven to correlate with poor prognosis in several cancers including NSCLC7,8.
To this regard, CTC evaluation allows readily “liquid biopsy” meanwhile access to surgical and/or biopsy specimens is often insufficient and fails to reflect tumour dynamics, heterogeneity or even drug sensitivity. Therefore, CTCs represent a powerful tool for disease management in agreement with the importance of developing non-invasive biomarkers to monitor tumour dynamics at real-time9.
In this work we present a methodology for the recovery of EpCAM positive CTCs from advanced NSCLC patients, followed by whole genome amplification and gene expression array analysis to characterize this metastatic population. Although EpCAM expression is frequently lost during cancer progression in NSCLC, EpCAM expression in CTCs correlates with poorer outcome in previous studies8, while EpCAM negative CTCs failed to prove prognostic value in lung cancer10. As from these data we were able to describe a panel of genes specifically expressed in CTCs from advanced NSCLC patients, and to improve our understanding on the biology of the subpopulation of CTCs in NSCLC. Moreover, we characterized NOTCH1 as main signalling pathway that illustrate their fate, and identified potential biomarkers with clinical significance.
Results
Immunoisolation and molecular profiling of CTC from advanced NSCLC patients
The presence of CTCs in advanced NSCLC was assessed by combining EpCAM-based immunoisolation and RT-qPCR analysis of GAPDH in a series of 42 advanced NSCLC patients (Supplementary Table S1) and 16 healthy donors. GAPDH has been stated as a reference marker of global cellularity when normalized to the recovery of CD45 as a marker of the non-specific isolated lymphocytes11, herein demonstrating the presence of an additional population in advanced NSCLC patients (p < 0.001; Fig. 1a). Also consistently, CD45 expression showed no significant differences when evaluated for both groups revealing same unspecific recovery in patients and controls (data not shown) and no power was observed for early progression in the cohort of patients (AUROC: 0.522) while GAPDH presented an AUROC 0.747 (Fig. 1b). Additionally, when CD45 gene expression was assessed in the remaining cellular fraction upon CTC immunoisolation no significant differences were found between patients and controls, revealing that CTC specific gene expression is not associated with differential expression in the non-CTC population11.

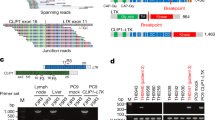
CTC detection and gene expression profiling.
(a) GADPH expression in CTC immunoisolated from advanced NSCLC patient (n = 42) and control (n = 16) groups. (b) AUROC curve for GAPDH and CD45 detection for RT-qPCR. Unspecific-isolated lymphocytes do not predict early progression (<4 months). (c) Principal component dot plot for differential distribution of NSCLC patients and healthy donors based on gene expression microarray. NSCLC patients are grouped constituting a particular population. (d) Schematic workflow for CTC gene expression profiling.
Molecular profiling of CTCs in advanced NSCLC was approached by subtracting the background of unspecific immunoisolation from healthy donors (n = 4) to the global gene expression profile of EpCAM-based immunoisolated CTCs from patients (n = 10; Supplementary Table S2), as described by Barbazan et al.11. Experimental workflow for CTC isolation and enrichment, RNA extraction, whole transcriptome amplification and array hybridization is depicted in Fig. 1d. Total RNA from CTCs was amplified, complementary DNA was hybridized onto Agilent gene expression microarray, and raw data was pre-processed as described in Material and Methods, resulting in 2,392 spots (7.01%) that accomplished the quality criteria. Average signal was 60,889 units being 76,597 and 16,979 units the average signal for patient and control groups respectively. Upon normalization 1,810 probes with expression greater than 211 in at least 8 patients and 2 controls were considered for any further analysis. Assuming Delta parameter to 2.46 for median False Discovery Rate (FDR) = 0 rendered 853 differentiated probes; being considered only the 305 probes with log2 ratio greater than 1.5 (Supplementary Table S3). In addition, 8 probes uniquely detected in patients’ samples, with a raw signal meeting the quality criteria, were included into subsequent analysis (Supplementary Table S4). Principal Component Analysis (PCA) revealed effective discrimination between patients and control samples, NSCLC patients being defined by their pathologic status (Fig. 1c).
Biology of CTC isolated from advanced NSCLC patients
Bioinformatic analysis with Ingenuity Pathway Analysis (IPA) software was performed to interpret the biology of NSCLC CTCs. Consistently with an actively disseminating subpopulation of tumour cells, the main molecular and cellular functions represented by the set of CTC-specific genes were related to cellular movement, cell death and survival and cellular development, cellular growth and proliferation, mainly orchestrated by PI3K/AKT, ERK1/2 and NF-kB pathways. GeneCodis3 ontology analysis also highlighted cell adhesion, developmental functions, extracellular matrix organization and an active transduction and transport activity (data not shown). Interestingly, NOTCH1 was identified as an important actor orchestrating this functional network (Fig. 2a and b). The biological and functional relevance of NOTCH1 within this metastatic population was further confirmed by RT-qPCR (Fig. 2c) in the series of 42 NSCLC patients (Supplementary Table S1). In addition, we assessed the expression of HES1, a downstream target gene of NOTCH1, whose expression was found to be significantly increased in patients (p = 0.041; Fig. 2d), in correlation with that of NOTCH1 (Fig. 2e). Moreover, we further assessed the functional relevance of Notch1 in the subpopulation of CTC in NSCLC by studying the impact of Notch1 pathway inhibition on clonogenic assay, as an indirect measure of the metastatic potential of CTC. As shown in Fig. 2f, the γ-secretase inhibitor DAPT significantly reduced the ability of A549 cells to grow in the absence of substrate at different concentrations in vitro (p = 0.031).

CTC expression profile analysis and NOTCH1 validation.
(a) Cellular functions and biological networks by IPA for CTC from advanced NSCLC patients. (b) Interaction network for cell movement, cell death and survival, cell development and cell growth and proliferation according to CTC expression profile. NOTCH1 is identified as a main actor orchestrating the network. (c) Validation of specific NOTCH1 gene expression in CTC from advanced NSCLC patients (n = 42) as compared to controls (n = 16). (d) HES1 gene expression is significantly increased in NSCLC patients compared to controls. (e) NOTCH1 correlates with his effector protein HES1 in NSCLC CTCs. (f) Clonogenic assay for A549 adenocarcinoma cells treated with the γ-secretase inhibitor DAPT (n = 6).
We finally screened the expression levels of LGALS3 (Galectin-3), ITGB3 (Integrin beta-3) and PTP4A3 (Protein tyrosine phosphatase type IVA 3), associated with the identified NOTCH1 network, in CTC immunoisolated from NSCLC patients. RT-qPCR evaluation showed a significant increased expression of the selected three candidate genes in the series of CTCs immunoisolated from patients with advanced NSCLC when compared to healthy donors (p < 0.05; Supplementary Figure S1). All these results confirmed the relevance of NOTCH1 in NSCLC dissemination and validated the bioinformatics analysis and biological information of the gene expression profiling of EpCAM+ CTCs immunoisolated from advanced NSCLC patients.
Prognostic significance of Notch1 network in CTCs from NSCLC
CTC gene expression profiling from advanced NSCLC patients also provided with diagnostic and prognostic markers with potential clinical impact in patient management. Univariate Cox regression analysis showed prognostic utility for NOTCH1 (p = 0.034), PTP4A3 (p = 0.003), LGALS3 (p = 0.044) and ITGB3 (p = 0.046) to predict Progression-Free Survival, and that for ITGB3 (p = 0.006) for Overall Survival. The poor prognosis groups were defined within the restrictive 33% of patients with the highest RT-qPCR signal for each biomarker (Supplementary Table S5, upper panel). Moreover, GAPDH proved clinical value to predict PFS (p < 0.001) and OS (p < 0.001) as expected for an indirect evaluator of the CTC burden (Supplementary Table S5, upper panel). Additionally, the presence of bone metastasis was identified as the only clinical parameter with prognostic significance in series of 42 advanced NSCLC patients (Supplementary Table S5, lower panel).
Kaplan-Meier analysis confirmed the prognostic value of NOTCH1, PTP4A3, LGALS3, ITGB3, and GAPDH biomarkers for PFS (Fig. 3), and that for GAPDH and ITGB3 for OS (Supplementary Figure S2). We further generated a logistic model with the panel of CTC-biomarkers in order to improve their diagnostic and prognostic value. For this, linear regression with a 67% good prognosis versus 33% poor prognosis cut-off for each biomarker as previously defined, demonstrated the best performance with an AUROC value of 0.772 for the combination of GAPDH, NOTCH1 and PTP4A3 in early progression (Fig. 4a). Accordingly, the prognostic value of the panel of CTC-biomarkers improved for PFS and OS when defined as a cumulative variable for the markers included in the logistic model (Fig. 4b,c).

Kaplan-Meier curves of validated biomarkers for Progression-Free Survival (PFS).
Statistical significance determined by log rank test (p < 0.05).

Prognosis and diagnosis value for the accumulation of biomarkers and logistic model.
(a) Linear regression model for GAPDH + NOTCH1 + PTP4A3 biomarkers. (b and c) Kaplan-Meier analysis grouping patients according to the marrkers included in the regression model for (b) PFS and (c) OS.
Finally, multivariate analysis including the panel of five CTC-biomarkers in combination with the presence of bone metastasis resulted in GAPDH, NOTCH1 and PTP4A3 as independent predictors of PFS (Table 1, upper panel); GAPDH and ITGB3 showed predictive value for OS (Table 1, upper panel). When referred to the cumulative variable of the logistic model CTC-biomarker panel, predictive value was achieved for PFS and OS, as well as bone metastasis (Table 1, lower panel).
Discussion
Research on circulating tumour cells (CTCs) has rapidly increased in the last years in response to the clinical need of new alternative tools for the management of patients candidate for personalized therapeutic strategies12. Traditionally, efforts have been devoted to understand the mechanisms underlying cancer progression mainly focused on primary and metastatic carcinomas; but little is known about the “fluid phase” of cancer as the relevant actor of tumour dissemination and lethality13. This is particularly relevant in NSCLC, where most cases result inoperable and biopsies are rarely obtainable. The analysis and characterization of CTCs in NSCLC patients represent a particularly attractive strategy for real-time patient monitoring to support treatment decisions14,15.
CTCs exist in extreme rarity in blood; therefore their analysis requires highly sensitive methods. In the last decade a number of technologies, not only restricted to immunoisolation, have become available16. Most of the commonly used strategies for CTC detection showed promising results in NSCLC, although the amount of data available is limited compared to other tumour types17,18. For instance, studies with the FDA-approved CellSearch system demonstrated utility for CTC detection with high levels of CTCs at baseline correlating with poor survival rates19,20; although heterogeneity in EpCAM expression could limit its applicability in NSCLC patients21. To this regard, we must also consider that EpCAM is frequently overexpressed in NSCLC, suggesting an implication of EpCAM in carcinogenesis22. In addition, EpCAM positivity was confirmed in our series of samples showing strong immunostaining in well-differentiated tumour areas while positivity was moderate in poorly differentiated tumour areas (Supplementary Figure S3). In this work, we focus on EpCAM-positive CTC from advanced NSCLC patients, and we approached their global gene expression profiling to better understand their biology and to identify and validate CTC-biomarkers with clinical utility in NSCLC.
Previous studies on CTC gene expression in NSCLC approached PCR-based technologies analysing subsets of genes from CTC enriched samples23,24. We combined CTC immunoisolation, whole genome amplification and gene-expression profiling. The specific NSCLC-derived CTCs expression profile is mainly associated with cellular movement, cell adhesion and differentiation, and cell-to-cell signalling linked to PI3K/AKT, ERK1/2 and NF-kB pathways, previously associated with lung cancer and metastasis25,26; and NOTCH1 playing an important role on the whole functional network. Of note, among genes related to cell adhesion we could find tenascin R (TNR) or mucin 4 (MUC4), previously associated with lung cancer aggressiveness and dissemination27,28.
Notch signalling is emerging as a valuable molecular pathway for targeting therapies in NSCLC. Clinical studies indicate that 30% of NSCLC cases have increased Notch1 signaling29 and this activity seems to be critical for driving cancer cell migration and metastasis due to repression of cell adhesion molecules, resulting in loss of cell-to-cell adhesion, protection against hypoxic conditions and promotion of a stem-like signature30. Recent studies have demonstrated that Notch signalling plays an important role in lung cancer initiation via crosstalk with transcription factors enhancing epithelial-to-mesenchymal transition (EMT)31. Further, dysregulation of Notch signalling as a common feature of NSCLC correlating with poor prognosis has been associated with TGF-β and EMT32. Related to this, Notch1 related EMT promotion has been associated with an increased EpCAM expression33. Of note, Notch signalling inhibition resulting in a non-significant decreased EpCAM expression (Supplementary Figure S3), did not altered the efficiency of EpCAM-based immunoisolation of CTC (Supplementary Figure S3). These results indicate that EpCAM-based immunoisolation is effective to purify CTC from NSCLC patients, the excess of antibody coupled beads are in excess being able to balance the variations in EpCAM expression due to Notch1-related EMT or the presence of poorly differentiated tumour cells (Supplementary Figure S3). Similarly, no differences in Notch1 were found between CTC-EpCAM positive immunoisolated from adenocarcinoma or squamous cell carcinoma origins (data not shown), although specific studies should be performed to address the impact of histology or mutational profiles associated with smoking34. Also accordingly, HES1 downstream target of NOTCH1, strongly correlated in the CTCs immunoisolated from advanced NSCLC patients, further suggesting the functional involvement of Notch pathway and the potential therapeutic value of Notch pathway-directed drugs such as γ-secretase inhibitors or ADAM inhibitors in advanced NSCLC35,36.
In addition to NOTCH1, with demonstrated prognostic value in NSCLC37, validated genes involved in the identified CTC-network have also been described during NSCLC progression. The expression of the growth/adhesion-regulatory lectin galectin-3 in stage II NSCLC is indicative of a poor prognosis38,39, playing a role in cell motility, invasion, and metastasis40. Similarly, PTP4A3 expression in NSCLC has been described upregulated in correlation with advanced clinical stage and distant metastasis linked to microvascular and lymphatic vessel formation41. Finally, ITGB3 has been recently described as mediator of NSCLC promotion in the context of K-ras addiction42, and whose inhibition by miR-9843 or miR let-7c44 prevented proliferation, migration and invasion in NSCLC.
The promising results obtained with the panel of CTC-biomarkers in NSCLC both for detection of metastatic disease and classification into favourable and unfavourable outcome guarantee further analysis in a large multicenter study including therapy monitoring.
In conclusion, we demonstrated that the combination of CTC immunoisolation and gene expression analyses represents an adequate strategy to: a) identify highly specific and sensitive CTC biomarkers with independent diagnosis and prognosis value and potential applicability in the management of advanced NSCLC patients; b) reveals NOTCH1 as a conducting factor in the biology of EpCAM positive CTCs and a potential therapeutic target to impair metastasis dissemination in NSCLC.
Material and Methods
Patient selection
Participants included in the study were diagnosed with advanced stage (unresectable stage III or IV) NSCLC on the basis of the International Association for the Study of Lung Cancer (IASLC)/ American Thoracic Society (ATS)/European Respiratory Society (ERS) classification criteria. Blood samples were collected before the initiation of chemotherapy, in accordance to the guidelines and protocols approved by the Institutional Ethical Committee (Galician Clinical Research Ethics Committee, SERGAS; code 2008/277), and signed informed consent was obtained from all participants. Candidates who had received chemotherapy previously to the study were not included.
CTCs evaluation cohort included 42 NSCLC patients with distant metastasis diagnosed in 36 cases (Supplementary Table S1). Microarray gene-expression analysis was conducted in an independent set of patients and healthy age-matched donors. Distant metastasis was present in 8 out of 10 patients at the moment of recruitment (Supplementary Table S2).
CTC immunoisolation, profiling and Significance Analysis Microarray
CTC isolation was performed from 7.5 ml of peripheral blood from advanced NSCLC patients or healthy donors using the EpCAM-based CELLectionTM Epithelial Enrich Dynabeads® kit (Invitrogen, Dynal; Oslo, Norway) according to manufacturers’ instructions. Isolated CTCs were resuspended in RNA later® (Ambion; Foster City, CA, USA) and preserved at −80°C until use.
Total RNA extraction, Complete Whole Transcriptome Amplification (WTA2, Sigma Aldrich) and gene expression array was performed as described by Barbazan et al.11. Briefly, total RNA was extracted with the QIAmp viral RNA mini kit (Qiagen, Valencia, CA, USA) specifically designed for very low cellularity samples. Subsequent pure RNA was then subjected to Complete Whole Transcriptome Amplification PCR for 20 cycles using the maximum amount of RNA; Cy3 labelling and hybridization onto Agilent 4 × 44 k gene expression arrays. Upon hybridization, signal was captured and submitted to Significance Analysis for Microarray to identify differentially expressed genes (Supplementary Material and Methods S1).
Ingenuity Pathway Analysis (IPA) and Gene Ontology analysis
Gene set characterizing CTC population was analysed with IPA software for representative biological pathways and functions in our data set. 204 probes were identified as annotated genes (66.6%). Fisher’s exact test was applied to calculate p value of biological related functions.
Additionally, CTC specific gene signature was submitted to gene ontology analysis using GeneCodis3 open access software45. Singular enrichment Gene Ontology tool was used to obtain a broad overview of the main biological processes involved in the CTC profile; of which 193 probes belonged to annotated genes (61.1%). Hypergeometrical test (p < 0.05) and FDR correction were used as stated in the software.
Preamplification and quantitative Real-Time PCR validation
CTCs were isolated from an independent set of patients and total RNA was extracted with the QIAmp viral RNA mini kit (Qiagen; Valencia, CA, USA) as previously stated. Complementary DNA (cDNA) was obtained using SuperScript III reverse transcriptase (Invitrogen; Carlsbad, CA, USA) adding 11 μl of total RNA per reaction. Because of very low cellularity of the samples, cDNA was subjected to 14x pre-amplification cycles (TaqMan® PreAmp Master Mix Kit, Applied Biosystems; Foster City, CA, USA) to increase sensibility and stability. Finally, pre-amplified 1:10 diluted cDNA was subjected to TaqMan RT-qPCR for candidate genes associated with Notch1 network by IPA (Supplementary Table S4). GAPDH, a reference gene previously used for CTC quantification in peripheral blood and indirect evidence of cellularity11,46, and HES1 as a downstream gene of NOTCH1 (Supplementary Material and Methods S1) were also included. Mean threshold cycle (depicted as 40-Ct) for every candidate gene was normalized to CD45, a lymphocyte specific marker that allows the quantification of non-specific isolation and that have been previously used to discriminate the population of CTCs from the total of nucleated cells isolated in blood11,47,48. Samples were run in duplicate and all plates included negative controls.
Cell culture
The human NSCLC cell line A549 was obtained from the American Type Culture Collection. A549 cells were maintained in Dulbecco’s Modified Eagle Medium (DMEM) with 10% FBS (Invitrogen). Cells were kept at 37 °C under a humidified atmosphere with 5% CO2. Mycoplasma test was conducted routinely.
Soft agar assay and Notch1 inhibition
Soft agar assays were conducted on 96-well plates with a base layer of 0.6% low melting point agarose and an upper layer of 0.3% low melting point agarose containing 5 × 103 cells per well. Upper and lower layer were constituted in 2% FBS DMEM.
Inhibition of Notch1 was approached by the addition of 100 μl of the γ-secretase inhibitor, DAPT (CAS 208255-80-5, Santa Cruz Biotechnology, Dallas, TX, USA; IC50: 115 nM), or its vehicle (DMSO) at different concentrations in FBS-free DMEM. Proliferation was measured five days later by AlamarBlue® Cell Viability Reagent (DAL1025, ThermoFisher). Significance was evaluated by Wilcoxon signed rank test (p < 0.05).
Statistical validation and clinical database contrast
Validation analysis was performed using two-tailed Mann-Whitney U-test. Clinical evaluation of validated markers was approached following the REMARK recommendations49. Progression-Free Survival (PFS) and Overall Survival (OS) were analysed using Kaplan-Meier analysis and differences were examined by log rank test. Univariate and multivariate analyses were performed using Cox regression statistics. Bivariate correlation analysis was routinely carried out according Pearson statistic. p < 0.05 values were considered statistically significant.
Additional Information
How to cite this article: Mariscal, J. et al. Molecular Profiling of Circulating Tumour Cells Identifies Notch1 as a Principal Regulator in Advanced Non-Small Cell Lung Cancer. Sci. Rep. 6, 37820; doi: 10.1038/srep37820 (2016).
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
Ferlay, J. et al. Cancer incidence and mortality patterns in Europe: Estimates for 40 countries in 2012. Eur. J. Cancer 49, 1374–1403 (2013).
Travis, W. D., Brambilla, E. & Riely, G. J. New pathologic classification of lung cancer: Relevance for clinical practice and clinical trials. J. Clin. Oncol. 31, 992–1001 (2013).
Siegel, R. L., Miller, K. D. & Jemal, A. Cancer statistics, 2016. CA Cancer J Clin 66, 7–30 (2016).
Berge, E. M. & Doebele, R. C. Targeted therapies in non-small cell lung cancer: emerging oncogene targets following the success of epidermal growth factor receptor. Semin. Oncol. 41, 110–125 (2014).
Zhang, Z. et al. Expansion of CTCs from early stage lung cancer patients using a microfluidic co-culture model. Oncotarget 5, 12383–12397 (2014).
Hodgkinson, C. L. et al. Tumorigenicity and genetic profiling of circulating tumor cells in small-cell lung cancer. Nat. Med. 20, 897–903 (2014).
Lou, J. et al. Quantification of rare circulating tumor cells in non-small cell lung cancer by ligand-targeted PCR. PLoS One 8, e80458 (2013).
Muinelo-Romay, L. et al. Evaluation of Circulating Tumor Cells and Related Events as Prognostic Factors and Surrogate Biomarkers in Advanced NSCLC Patients Receiving First-Line Systemic Treatment. Cancers (Basel). 6, 153–165 (2014).
Lianidou, E. S., Strati, A. & Markou, A. Circulating tumor cells as promising novel biomarkers in solid cancers. Crit. Rev. Clin. Lab. Sci. 51, 160–71 (2014).
de Wit, S. et al. The detection of EpCAM+ and EpCAM− circulating tumor cells. Sci. Rep. 5, 12270 (2015).
Barbazán, J. et al. Molecular characterization of circulating tumor cells in human metastatic colorectal cancer. PLoS One 7, e40476 (2012).
Becker, T. M. et al. New frontiers in circulating tumor cell analysis: A reference guide for biomolecular profiling toward translational clinical use. Int. J. Cancer 134, 2523–2533 (2014).
Alix-Panabières, C., Pantel, K., Alix-Panabier̀es, C. & Pantel, K. Circulating tumor cells: Liquid biopsy of cancer. Clin. Chem. 59, 110–8 (2013).
Han, Y., Su, C. & Liu, Z. Methods for detection of circulating cells in non-small cell lung cancer. Front. Biosci. Landmark Ed. 19, 896–903 (2014).
Pesta, M., Kulda, V., Narsanska, A., Fichtl, J. & Topolcan, O. May CTC technologies promote better cancer management? EPMA J. 6, 1 (2015).
Esmaeilsabzali, H., Beischlag, T. V., Cox, M. E., Parameswaran, A. M. & Park, E. J. Detection and isolation of circulating tumor cells: principles and methods. Biotechnol. Adv. 31, 1063–1084 (2013).
O’Flaherty, J. D. et al. Circulating tumour cells, their role in metastasis and their clinical utility in lung cancer. Lung Cancer 76, 19–25 (2012).
Alama, A., Truini, A., Coco, S., Genova, C. & Grossi, F. Prognostic and predictive relevance of circulating tumor cells in patients with non-small-cell lung cancer. Drug Discov. Today 19, 1671–1676 (2014).
Hofman, V. et al. Detection of circulating tumor cells as a prognostic factor in patients undergoing radical surgery for non-small-cell lung carcinoma: Comparison of the efficacy of the CellSearch AssayTM and the isolation by size of epithelial tumor cell method. Int. J. Cancer 129, 1651–1660 (2011).
Krebs, M. G. et al. Analysis of circulating tumor cells in patients with non-small cell lung cancer using epithelial marker-dependent and -independent approaches. J. Thorac. Oncol. 7, 306–315 (2012).
Lecharpentier, A. et al. Detection of circulating tumour cells with a hybrid (epithelial/mesenchymal) phenotype in patients with metastatic non-small cell lung cancer. Br. J. Cancer 105, 1338–1341 (2011).
Went, P. et al. Frequent high-level expression of the immunotherapeutic target Ep-CAM in colon, stomach, prostate and lung cancers. Br. J. Cancer 94, 128–35 (2006).
Devriese, L. A. et al. Circulating tumor cell detection in advanced non-small cell lung cancer patients by multi-marker QPCR analysis. Lung Cancer 75, 242–247 (2012).
Zhu, W.-F. et al. Prognostic value of EpCAM/MUC1 mRNA-positive cells in non-small cell lung cancer patients. Tumour Biol. 35, 1211–1219 (2014).
Winslow, M. M. et al. Suppression of lung adenocarcinoma progression by Nkx2-1. Nature 473, 101–104 (2011).
Geng, J. et al. EZH2 promotes tumor progression via regulating VEGF-A/AKT signaling in non-small cell lung cancer. Cancer Lett. 359, 275–287 (2015).
Majhi, P. D. et al. Pathobiological implications of MUC4 in non-small-cell lung cancer. J. Thorac. Oncol. 8, 398–407 (2013).
Zhan, J., Han, Q. & Wang, K. Development of antibody therapeutics for small cell lung cancer. Expert Opin. Investig. Drugs 22, 235–244 (2013).
Westhoff, B. et al. Alterations of the Notch pathway in lung cancer. Proc. Natl. Acad. Sci. USA 106, 22293–22298 (2009).
Wael, H. et al. Notch1 signaling controls cell proliferation, apoptosis and differentiation in lung carcinoma. Lung Cancer 85, 131–140 (2014).
Yuan, X. et al. Notch signaling and EMT in non-small cell lung cancer: biological significance and therapeutic application. J. Hematol. Oncol. 7, 87 (2014).
Deskin, B., Lasky, J., Zhuang, Y. & Shan, B. Requirement of HDAC6 for activation of Notch1 by TGF-β1. Sci. Rep. 6, 31086 (2016).
Bao, B. et al. Notch-1 induces epithelial-mesenchymal transition consistent with cancer stem cell phenotype in pancreatic cancer cells. Cancer Lett. 307, 26–36 (2011).
Mäki-Nevala, S. et al. Hot spot mutations in Finnish non-small cell lung cancers. Lung Cancer 99, 102–10 (2016).
Xie, M., He, J., He, C. C.-S. & Wei, S.-H. S. γ secretase inhibitor BMS-708163 reverses resistance to EGFR inhibitor via the PI3K/Akt pathway in lung cancer. J. Cell. Biochem. 116, 1019–1027 (2015).
Moellering, R. E. et al. Direct inhibition of the NOTCH transcription factor complex. Nature 462, 182–188 (2010).
Yuan, X. et al. Meta-analysis reveals the correlation of Notch signaling with non-small cell lung cancer progression and prognosis. Sci. Rep. 5, 10338 (2015).
Puglisi, F. et al. Galectin-3 expression in non-small cell lung carcinoma. Cancer Lett. 212, 233–239 (2004).
Szöke, T. et al. The role of microvascularization and growth/adhesion-regulatory lectins in the prognosis of non-small cell lung cancer in stage II. Eur. J. Cardiothorac. Surg. 31, 783–7 (2007).
O’Driscoll, L. et al. Galectin-3 expression alters adhesion, motility and invasion in a lung cell line (DLKP), in vitro. Anticancer Res. 22, 3117–3125 (2002).
Ming, J., Liu, N., Gu, Y., Qiu, X. & Wang, E.-H. PRL-3 facilitates angiogenesis and metastasis by increasing ERK phosphorylation and up-regulating the levels and activities of Rho-A/C in lung cancer. Pathology 41, 118–26 (2009).
Symonds, J. M., Ohm, A. M., Tan, A. & Reyland, M. E. PKCδ regulates integrin α V β 3 expression and transformed growth of K-ras dependent lung cancer cells. Oncotarget 7, 17905–17919 (2016).
Ni, R., Huang, Y. & Wang, J. miR-98 targets ITGB3 to inhibit proliferation, migration, and invasion of non-small-cell lung cancer. Onco. Targets. Ther. 8, 2689–97 (2015).
Zhao, B. et al. MicroRNA let-7c inhibits migration and invasion of human non-small cell lung cancer by targeting ITGB3 and MAP4K3. Cancer Lett. 342, 43–51 (2014).
Tabas-Madrid, D., Nogales-Cadenas, R. & Pascual-Montano, A. GeneCodis3: A non-redundant and modular enrichment analysis tool for functional genomics. Nucleic Acids Res. 40, 478–483 (2012).
Muscarella, L. A. et al. Gene expression of somatostatin receptor subtypes SSTR2a, SSTR3 and SSTR5 in peripheral blood of neuroendocrine lung cancer affected patients. Cell. Oncol. (Dordr). 34, 435–41 (2011).
Isobe, K. et al. Clinical significance of circulating tumor cells and free DNA in non-small cell lung cancer. Anticancer Res. 32, 3339–44 (2012).
Barbazán, J. et al. A logistic model for the detection of circulating tumour cells in human metastatic colorectal cancer. J. Cell. Mol. Med. 16, 2342–9 (2012).
Popat, S. & Houlston, R. S. Re: Reporting recommendations for tumor marker prognostic studies (REMARK). J. Natl. Cancer Inst. 97, 1855–1856 (2005).
Acknowledgements
We thank the patients for their willingness to participate in the study. This work was funded by InveNNta (Innovation in Nanomedicine); Operational Programme for Cross-border Cooperation: Spain-Portugal (POCTEP) and European Regional Development Fund (ERDF). Javier Mariscal is recipient of a fellowship from Escola de Doutoramento Internacional Campus Vida of the University of Santiago de Compostela. Laura Muinelo-Romay is supported by ISCIII as Responsible of the Liquid Biopsy Analysis Unit. The funders had no role in the study design, data collection and analysis, decision to publish or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
J.M., M.A.-N. and A.A. carried out the immunoisolation, processing and analysis of samples. J.M., M.A.-N., L.M.-R., J.B., M.V., A.G.-T., M.A.C.d.C., R.L.-L. and M.A. participated in the design of the study, interpretation of data and critical revision of the manuscript. L.M.-R., M.V., C.R., E.B., F.B., R.L.-L. and M.A. contributed to the design and organization of human sample collection. T.G.-C. performed the histopathological analysis.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Electronic supplementary material
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Mariscal, J., Alonso-Nocelo, M., Muinelo-Romay, L. et al. Molecular Profiling of Circulating Tumour Cells Identifies Notch1 as a Principal Regulator in Advanced Non-Small Cell Lung Cancer. Sci Rep 6, 37820 (2016). https://doi.org/10.1038/srep37820
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep37820
This article is cited by
-
Numerical Study on Separation of Circulating Tumor Cell Using Dielectrophoresis in a Four-Electrode Microfluidic Device
Journal of Shanghai Jiaotong University (Science) (2023)
-
Prognostic and therapeutic significance of circulating tumor cells in patients with lung cancer
Cellular Oncology (2020)
-
An integrated flow cytometry-based platform for isolation and molecular characterization of circulating tumor single cells and clusters
Scientific Reports (2018)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
