
Abstract
Risk stratification and treatment intensification, based on minimal residual disease (MRD) mensurement, changed the prognosis of pediatric patients with acute lymphocytic leukemia (ALL). The main aim of this study was to investigate whether peripheral blood (PB) MRD measurement at day 8 (D8) could predict the risk stratification category determined by bone marrow (BM) MRD at day 15 (D15). The study was performed prospectively, in a cohort of 40 children with B-lineage ALL, adopting the protocol of the Brazilian Cooperative Group of the Treatment Childhood Leukemia (GBTLI-2009). MRD was detected by flow cytometry (FC) using a simplifed panel that can reliably identify MRD at early phases of induction therapy. Upon diagnosis, the proportion of low and high-risk patients, was 24:16 (60%:40%). The main result of our study demonstrated the potential of D8 MRD in anticipating of week the risk stratification of high-risk patients as determined by D15 BM MRD. In these patients D8 MRD level of 1% was able to segregate high risk fast responders from high risk slow responders (p = 0.0097). This result could represent an opportunity for early treatment intensification, as already performed in some protocols.
Similar content being viewed by others

Introduction
The recent increase in survival rates observed in acute lymphocytic leukemia (ALL) is due to advances in diagnosis, identification of critical prognostic factors and definition of treatment according to risk groups1,2,3. At diagnosis, the most important parameters for risk stratification, with minor differences across different therapy protocols, are age, white blood cell count, immunophenotype, presence of lymphoblasts in the central nervous system and molecular analysis of chromosomal abnormalities4,5. In addition, early response to induction chemotherapy is also a critical prognostic factor.
Historically, therapeutic response was assessed mostly by morphological count of blasts in peripheral blood (PB) and bone marrow (BM). However, due to the fact that patients in morphologic remission may present morphologically undetectable amounts of residual leukemic cells, referred as “Minimal Residual Disease” (MRD), different strategies using flow cytometric or molecular techniques have been used to detect these cells in the last decades5,6,7. MRD measurement is actually superior to other traditional markers of disease and based in its result, is possible to optimize chemotherapy, minimizing toxicity and decreasing risk of relapse3,4,5,8,9.
Current ALL protocols associate morphological analysis with MRD measurement to evaluate treatment response on both early and late time-points, providing more timely and accurate prognostic information of treatment outcome2,4,10. However, on day 8 (D8), the earliest time point of assessment of therapeutic response, most protocols use morphological analysis of PB for risk stratification, with good and poor responses defined as PB leukemic blast counts below and above 1,000/mm3, respectively11. In order to refine this D8 evaluation, the Children’s Oncology Group (COG) protocol adopted MRD analysis to guide treatment in this earliest time point, with positive outcomes on treatment response1. However, MRD evaluation at D8 has not been widely adopted and several protocols still rely on morphological analysis. Here, we present the results of an independent study to evaluate the impact of D8 MRD measurement on risk stratification in a prospective cohort of 40 patients with ALL.
Patients and Methods
Study design and definitions
From January 2014 to January 2015, all children newly diagnosed with B-lineage ALL and admitted for treatment at our institution, which is the only institution that provides care for children with leukemia in the State of Amazonas in northern Brazil, were recruited for this study. T-lineage ALL and AML were excluded by immunophenotypical criteria based in a broad panel of monoclonal antibodies at diagnosis. The characterization of genetic abnormalities in bone marrow samples was performed by conventional cytogenetics at diagnosis. As per protocol definitions, alterations indicating the presence t(9;22) which is associated with BCR-ABL1, or t(4;11), which is associated with MLL rearranged were defined as high risk cytogenetic abnormalities.
After admission, parents/legal guardians were invited to participate and provided written informed consent. The study was approved by the Committee of Ethics in Research of the Hematology and Hemotherapy Foundation of Amazonas (HEMOAM) and performed in accordance with the Declaration of Helsinki. Diagnosis was based on morphological and immunophenotypical criteria and patients were treated according to the guidelines of the Brazilian Cooperative Group for the Treatment of Childhood Leukemia (GBTLI-2009) (supplementary Figures 1 and 2). Patients were initially stratified as low or high risk at diagnosis according to clinical and laboratory criteria shown in Table 1.
Then, during induction, patients were restratified according to response to chemotherapy. As shown in Fig. 1, low risk patients at diagnosis were restratified as true low risk, intermediate low risk or high risk slow responders. On the other hand, high risk patients at diagnosis were restratified as high risk fast responders or high risk slow responders.

Restratification during induction.
Risk restratification criteria at days 8 and 15 of induction therapy, according to Brazilian Cooperative Group for the Treatment of Childhood Leukemia 2009 (GBTLI 2009).
Laboratory analysis and interpretation
During induction, PB samples were obtained at D8 and BM samples at day 15 (D15) to measure MRD by flow cytometry (FC) according to previously published criteria2,3,10. Briefly, MRD measurement was performed using 4-colour flow cytometry analyzer (FacsCalibur, Becton Dickinson, San Jose, CA, USA) using simplified FC panel of monoclonal antibodies that can be used into non-regenerative phases of treatment3 (Table 2). This simplified flow cytometric assay is based on expression of CD19, CD10 and CD34 antigens, that can reliably identify MRD at early phases of remission induction therapy. According to Coustan-Smith et al., normal lymphoid progenitors (CD19, CD10, and/or CD34) are exquisitely sensitive to corticosteroids and other antileukemic drugs. Therefore, cells with this phenotype detected early in treatment of patients with B-lineage ALL should be leukemic rather than normal cell3.
The number of residual leukemic cells was calculated as the percentage of blasts present within the total of nucleated cells counted. After gating on CD19 cells with lymphoid morphology (as defined by their forward and side light-scattering properties), we determined the percentages of CD19 cells expressing CD10 and/or CD34. Sensitivity, determined upon dilutions of leukemic blasts in normal BM or PB, was 0,01%. Morphology was analyzed at the same time points by an investigator blinded to MRD results.
Based on BM MRD at D15, patients were assigned to different risk stratification groups, according to GBTLI-2009 criteria, presented above12. Next, the association between PB MRD at D8 and risk stratification at D15 was examined.
Statistical analysis
Descriptive statistics were used to report demographical and clinical data. Data are expressed as median, ranges, means and SD. Differences in continuous variables were analyzed using the Mann-Whitney test. Categorical variables were compared using the Fisher’s exact test. A p value less than or equal to 0.05 was considered statistically significant. All statistical analyses were performed using the GraphPad Prism Software (GraphPad Prism Software Inc. San Diego, California, USA).
Results
Our study population, which represents all children treated for ALL during the study period in the State of Amazonas, Brazil, consisted of 40 patients (23 males; 17 females) with a median age of 3.5 years (range 1–17). Additional social-demographic, clinical and laboratorial characteristics of the patients are shown in Tables 3 and 4.
Upon diagnosis, the proportion of low and high-risk patients, based on GBTL-2009 criteria was 24:16 (60%:40%). A flowchart of enrolled patients is shown in Fig. 2. At D8, PB MRD data was available for 35 out of 40 patients, with the five remaining patients evaluated only by morphology at this time-point. Although at D8 manual blast count all patients presented less than 1,000 blasts/mm3, PB MRD levels revealed a more heterogenous response in terms of MRD levels, with 68,5% of the patients presenting MRD between 0,01% and 10%; 20% presenting MRD ≥10% and only 11,4% pesenting negative (MRD ≤0,01%) (Fig. 2).

Comparison of manual blast count and MRD levels at day 8.
Flowchart of the comparative analysis between manual blast count and PB MRD detected by flow cytometry (MRD-FC) at day 8.
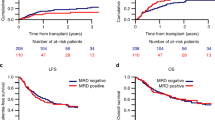
Finally, we assessed whether PB MRD measurement at D8 could predict the risk stratification category determined by BM MRD at D15, thereby anticipating this important information (Fig. 3). In Fig. 3A, PB MRD at D8 from low-risk patients (at diagnosis) is compared between the three risk stratification groups, as determined by levels of BM MRD at D15 (as previously detailed). Similar PB MRD levels at D8 were observed between patients from intermediate low risk and high risk. In contrast, the two patients assigned to the “true low risk” category by BM MRD at D15 were negative for PB MRD at D8 (Fig. 3A). Unfortunately, the low number of patients in this category precluded a formal statistical analysis. In Fig. 3B, PB MRD at D8 from high-risk patients (at diagnosis) is compared to fast and slow responders, according to D15 MRD (Fig. 1). Interestingly, a statistically significant difference of PB MRD levels could be detected at D8 (P = 0.0097). Of note, all high risk slow responders presented MRD level below 1% at D8.

Comparison of Day 8 MRD-FC with Day 15 MRD risk groups.
Patients stratified as low risk at diagnosis (3A) were reclassified as true low risk, intermediate low risk, or high risk according to MRD levels at day 15, based on the GBTLI-2009 protocol. Patients stratified as high risk at diagnosis (3B) were reclassified as fast or slow responders, according to MRD levels at day 15, based on the GBTLI-2009 protocol. Minimal residual disease measured by flow cytometry at day 8 (MRD-FC D8) for each of these subgroups is showed.
Discussion
Risk stratification and selected treatment intensification based on MRD detection have changed the prognosis of ALL patients11. However, at D8, most protocols still use morphological criteria to evaluate treatment response, leaving more sensitive techniques for later time-points. However, the feasibility and potential benefits of using MRD measurement as early as D8 have been demonstrated by the COG group in 2008. This group demonstrated that patients who had high levels of D8 PB MRD (>1%) had a poor outcome even if they cleared their BM of MRD by the end of induction, especially in high risk patients1. Here, we aimed to evaluate whether the anticipation of MRD measurement from D15 to D8, using PB samples, could add relevant information to the management of patients with ALL and thereby validate the COG findings in an independent cohort treated with a different protocol.
Our study was performed prospectively, in a population of consecutive patients, from a single center responsible for the treatment of all patients with ALL in the State of Amazonas, Brazil, an area with approximately 4 million inhabitants. The study was conducted in a relatively short time span and all patients adopted the same treatment guidelines. The main result of our study was the demonstration that D8 MRD measured in PB samples could anticipate in one week the risk stratification of high-risk patients with ALL that was later determined by BM MRD, at D15. This result could represent an opportunity for early treatment intensification, as already performed in some protocols.
The potential of D8 MRD measurement to refine risk stratification during early phases of ALL treatment was clearly evident for patients that were classified as high-risk according to GBTLI criteria at diagnosis. In these patients D8 MRD level of 1% was able to segregate high risk fast from slow responders as early as at D8 in our population. A similar finding was described in a study of childhood ALL in the UK, which identifed the same MRD-FC level at D8 to segregate high risk from low risk pacients13.
In our low-risk patients this finding could not be confirmed, maybe due to the limited number of patients in this group. However, the fact that none of the patients from the “true low-risk” group presented PB MRD at D8 suggests that this strategy could also be informative in this group, which should be confirmed in additional studies.
Our study highlights the potential of D8 MRD measured in PB samples for anticipating in one week the risk stratification of high-risk patients with ALL, as determined by BM MRD at D15. This result could represent an opportunity for early treatment intensification, as already performed in some protocols. However, due to the short follow-up and relatively limited number of patients we are not able to test the impact of these results in clinically-relevant outcomes such as event-free and overall survival. We are following this population currently and increasing the cohort to obtain this data. Validation in a larger cohort of patients is still required. Based on future results, it will be possible to evaluate if treatment intensification, based on D8 MRD, should be incorporated to the Brazilian protocol schedule.
“Furthermore, another limitation of our study is the limited genetic characterization of our population, which was based only on conventional cytogenetics. It has been shown that the identification of additional submicroscopic genetic alterations and the use of more sensitive techniques could further improve the stratification of childhood ALL, an issue that is still under investigation in prospective studies14. However, several recent studies about childhood ALL still rely only on clinical, hematological and cytogenetic parameters for risk stratification15,16,17,18. In addition, limitations in the access to molecular biology techniques in some areas of Brazil (which is likely to be the case of a large proportion of treatment centers around the globe), also preclude the immediate adoption of some diagnostic tools in ongoing protocols. Therefore, while we acknowledge that it is not possible to rule out that the incorporation of more sensitive genetic markers could have changed our results, we believe that the well-established power of cytogenetics to define prognosis in childhood ALL19,20,21,22 and its widespread use in several recent reported clinical trials, makes this possibility less likely.
In conclusion, our results validate, in an independent population using a different protocol, that MRD measurement at D8 of induction therapy in children with ALL can anticipate the information obtained by MRD only at D15 for high-risk patients.
Additional Information
How to cite this article: Salina, T. D. C. et al. Role of peripheral blood minimum residual disease at day 8 of induction therapy in high-risk pediatric patients with acute lymphocytic leukemia. Sci. Rep. 6, 31179; doi: 10.1038/srep31179 (2016).
References
Borowitz, M. J. et al. Clinical significance of minimal resisual disease in chidhood acute lymphoblastic leukemia and its relationship to other prognostic factors: a Children’s Oncology Group study. Blood. 111, 5477–5485 (2008).
Coustan Smith, E. et al. Prognostic importance of measuring early clearance of leukemic cells by flow cytometry in childhood acute lymphoblastic leukemia. Blood. 100, 52–58 (2002).
Coustan-Smith E. et al. A simplified flow cytometric assay identifies children with acute lymphoblastic leukemia who have a superior clinical outcome. Blood. 108, 97–102 (2006).
Schultz, K. R. et al. Risk-and response-based classification of childhood B-precursor acute ymphoblastic leukemia: a combined analysis of prognostic markers from the Pediatric Oncology Group (POG) and Children’s Cancer Group (CCG). Blood. 100, 926–935 (2007).
Silverman L. Childhood acute lymphoblastic leukemia: currently applied prognostic factors in. Siop education book international society of paediatric oncology 2nd edn. (ed. Boston: SIOP), 18–24 (2010).
Adin-Cinar, S., Kucuksezer, U. C. & Deniz, G. Implications os minimal residual disease by flow cytometry in pediatric acute leukemias. Internation trends in immunyty. 4, 51–61 (2013).
Basso, G. et al. Risk of relapse of childhood acute lymphoblastic leukemia is predicted by flow cytometric measurement of residual disease on day 15 bone marrow. Journal of Clinical Oncology. 31, 5168–5174 (2009).
Delbuono, E., Maekawa, M. R., Latorre, M. R., Petrilli, A. S., Braga, J. A. & Lee, M. L. Simplified flow cytometric assay to detect minimal residual disease in childhood with acute lymphoblastic leukemia. Revista Brasileira de Hematologia e Hemoterapia. 30, 281–286 (2008).
Ryan, J. et al. Minimal residual disease detection in childhood acute lymphoblastic leukaemia patients at multiple time-points reveals high levels of concordance between molecular and immunophenotypic approaches. British Journal of Haematology. 144, 107–115 (2008).
Coustan Smith E. et al. New markers for minimal residual disease detection in acute lymphoblastic leukemia. Blood. 117, 6267–6275 (2011).
Van Dongen, J. M., Van der Velden, V. H. J., Bruggemann, M. & Orfao, A. Minimal residual disease diagnostics in acute lymphoblastic leukemia: need for sensitive, fast and standardized technologies. Blood. 125, 3996–4008 (2015).
Sociedade Brasileira de Oncologia Pediátrica. Protocolo Brasileiro de tratamento da leucemia linfóide aguda na infância GBTLI LLA-2009. São Paulo: Campinas, 1–347 (2011).
Duncan, M. E. & Goldacre, M. J. Analysis of early disease response in childhood acute lymphblastic leukaemia: can peripheral blood replace bone marrow analysis? British Journal of Haematology. 161, 738–751 (2013).
Cooper, S. L. & Brown, P. A. Treatment of Pediatric Acute Lymphoblastic Leukemia. Pediatric clinics of North America. 62, 61–73 (2015).
Oskarsson, T. et al. Relapsed childhood acute lymphoblastic leukemia in the Nordic countries: prognostic factors, treatment and outcome. Haematologica. 101, 68–76 (2016).
Schrappe, M. et al. Outcomes after induction failure in childhood acute lymphoblastic leukemia. N Engl J Med. 15, 1371–1381 (2012).
Tower R. L. et al. Dose intensification of methotrexate and cytarabine during intensified continuation chemotherapy for high-risk B-precursor acute lymphoblastic leukemia: POG 9406: a report from the Children’s Oncology Group. J Pediatr Hematol Oncol. 36, 353–361 (2014).
Vora, A. et al. Augmented post-remission therapy for a minimal residual disease-defined high-risk subgroup of children and young people with clinical standard-risk and intermediate-risk acute lymphoblastic leukaemia (UKALL 2003): a randomized controlled trial. Lancet Oncol. 15, 809–18 (2014).
Moorman, A. V. et al. Prognostic effect of chromosomal abnormalities in childhood B-cell precursor acute lymphoblastic leukaemia: results from the UK Medical Research Council ALL97/99 randomised trial. Lancet Oncol. 11, 429–438 (2010).
Bradstock, K. F. et al. Immunological monitoring of residual disease in treated thymic acute lymphoblastic leukaemia. Leuk Res. 5, 301–309 (1981).
Hauel, M. & Matthes, T. Minimal residual disease monitoring: the new standard for treatment evaluation of haematological malignances? The European Journal of Medical Sciences. 144, 1–10 (2014).
Ratei, R. et al. Monitoring treatment response of childhood precursor B-cell acute lymphoblastic leukemia in the AIEOP-BFM-ALL 2000 protocol with multiparameter flow cytometry: predictive impact of early blast reduction on the remission status after induction. Leukemia researh. 23, 528–34 (2009).
Acknowledgements
The study was approved by the local Institutional Review Board and performed in accordance with the Declaration of Helsinki. All parents/legal guardians were invited to participate and provided written informed consent.
Author information
Authors and Affiliations
Contributions
T.D.d.C.S.: designed the study, assisted patients, recorded clinical and laboratory data, analyzed the results and drafted the manuscript. Y.A.F. and E.B.A.: performed laboratorial analyses. C.M.F.: analyzed the results. E.V.d.P., M.T.M.: analyzed the results and drafted the manuscript. L.d.M.P.: designed the study and analyzed the results. All authors reviewed and approved the manuscript.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Electronic supplementary material
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Salina, T., Ferreira, Y., Alves, E. et al. Role of peripheral blood minimum residual disease at day 8 of induction therapy in high-risk pediatric patients with acute lymphocytic leukemia. Sci Rep 6, 31179 (2016). https://doi.org/10.1038/srep31179
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep31179
This article is cited by
-
Minimal/Measurable Residual Disease Detection in Acute Leukemias by Multiparameter Flow Cytometry
Current Hematologic Malignancy Reports (2018)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
