
Abstract
Though depressive symptoms are common in patients with schizophrenia, they are often left untreated and are associated with a high relapse rate, suicidal ideation, increased mortality, reduced social adjustment, and poor quality of life. The present study aims to elucidate the association between depressive symptoms and fronto-temporal activities during a cognitive task in patients with schizophrenia. The fronto-temporal activities of 41 Japanese patients with schizophrenia was evaluated during a verbal fluency task using 52-channel near-infrared spectroscopy (NIRS). Depressive symptoms were assessed using the depression/anxiety component of the Positive and Negative Syndrome Scale (PANSS) five-factor model. The depression/anxiety component of the PANSS five-factor model was negatively correlated with activities of the ventrolateral prefrontal cortex (PFC), right dorsolateral PFC, and left temporal regions. Our findings suggest that reduced fronto-temporal activities on NIRS during a verbal fluency task is related to depressive symptom severity in patients with schizophrenia.
Similar content being viewed by others


Introduction
The Positive and Negative Syndrome Scale (PANSS) is widely used in the clinical assessment of schizophrenia. Originally, it was divided into three scales: positive, negative, and general psychopathology1. However, subsequent factorial analyses indicated the existence of other components. Recently, multiple-factor models of the PANSS have been used to evaluate the multidimensional symptoms of schizophrenia2,3. Among these, the so-called depressive or anxio-depressive dimension has been frequently used. Evidence collected using this model does not vary from clinical observations. Indeed, depressive symptoms are among the earliest and most frequent signs of schizophrenia onset4,5, and around 70% of patients with chronic schizophrenia without a major depressive disorder show some signs of depressive symptoms6. Depressive symptoms in schizophrenia are known to have detrimental consequences such as a high relapse rate, suicidal ideation, increased mortality, reduced social adjustment, and poor quality of life4,7,8,9. Despite the clinical importance of depressive symptoms in patients with schizophrenia, little is known regarding the underlying neurobiological mechanism.
Numerous studies have mostly used functional magnetic resonance imaging (fMRI) and electroencephalography methods to reveal the neural correlates of positive10,11 or cognitive12,13 symptoms in schizophrenia. Multichannel near-infrared spectroscopy (NIRS), a functional neuroimaging technology widely used in recent years, can measure hemodynamic changes over the surface of the cortices of the bilateral fronto-temporal regions14. This technique enables the detection of spatiotemporal characteristics of brain function by measuring the concentrations of oxygenated haemoglobin (oxy-Hb) and deoxygenated haemoglobin (deoxy-Hb), which are assumed to reflect the regional cerebral blood volume as demonstrated by good correlations with fMRI signals15. Numerous studies performed using this technique have consistently shown that, during a verbal fluency task (VFT), oxy-Hb change in the fronto-temporal brain regions is significantly lower in patients with schizophrenia than in healthy controls16,17,18. Further, NIRS measurement during a VFT has been shown to be a useful clinical auxiliary laboratory test for the differential diagnosis of depressive states9. Many investigators have reported an association between NIRS signals and clinical symptoms of schizophrenia, suggesting that the fronto-temporal hemodynamic responses during the VFT are related to positive, negative, or general psychopathology symptoms18,19,20. However, these studies did not examine depressive symptoms. Use of specific neurobiological markers (e.g., NIRS) in addition to the five-factor model of PANSS assessment might improve the evaluation of depressive symptoms. Therefore, investigating the five-factor model of PANSS is important for understanding the depressive symptoms of schizophrenia. In this study, we investigated the association between depressive symptoms and fronto-temporal hemodynamic responses during a VFT in patients with schizophrenia using the five-factor model of the PANSS.
According to a review by Drevets21, a complex relationship exists between depressive symptom severity and frontal lobe function, i.e., the metabolic activity in the orbital cortex and ventrolateral prefrontal cortex (PFC). Noda et al.22 recently described an association between VFT-related oxy-Hb change in the right dorsolateral PFC and severity of depressive symptoms in patients with major depressive disorder (MDD). These studies suggest that abnormal functions of the PFC are mood-dependent22,23,24. Based on the preliminary results of previous neuroimaging studies in patients with MDD, we hypothesize that the severity of depressive symptoms would be associated with abnormal PFC hemodynamic responses during a VFT in patients with schizophrenia. Structural brain imaging and neuropsychological studies have provided indirect support of the notion that depressed mood in schizophrenia may have at least partially overlapping neurobiology with major depressive disorder, such as volumetric abnormalities of the frontal and temporal lobes25 as well as attentional impairment26. The findings of Kohler et al.25,26 offer further support to the notion that depressed mood, regardless of its aetiology, involves similar brain systems, namely the frontal cortex, which is also required for attentional processing. In the present study, considering the consistent finding of attenuated oxy-Hb changes during VFT in the fronto-temporal regions in patients with schizophrenia, we hypothesized that oxy-Hb changes during VFT as measured using NIRS may act as objective indicators of depressive symptom severity.
Results
General Demographics
The participants’ demographic data are presented in Table 1.
Mean Hb changes during the VFT
The mean oxy-Hb levels during the task period were significantly higher than the pre-task baseline for 37 channels (ch2, ch9, ch12, ch13, ch15, ch19 to ch26, ch28 to ch30, and ch32 to 52; 52-channel FDR-corrected p < 0.05) in participants with schizophrenia.
The mean deoxy-Hb levels during the task period were significantly higher than those for the pre-task baseline for 28 channels (ch20, ch23 to ch25, ch28 to ch36, and ch38 to 52; 52-channel FDR-corrected p < 0.05) in participants with schizophrenia.
Correlation between the mean Hb changes and clinical symptoms
No significant correlation was found between changes in mean oxy-Hb in any channel and the total, positive, negative, and general psychopathology scores of the PANSS (52-channel FDR-corrected p > 0.05).
Mean oxy-Hb changes were significantly negatively correlated with depression/anxiety component scores in the ventrolateral PFC (ch23, ch34, and ch50; 52-channel FDR-corrected p < 0.05; rho: −0.48 to −0.43), right dorsolateral PFC (ch24, 52-channel FDR-corrected p < 0.05; rho = −0.44), and left temporal (ch42 and ch52; 52-channel FDR-corrected p < 0.05; rho: −0.47 to −0.46) regions (Fig. 1). However, there was no significant correlation between mean oxy-Hb and scores in any of the other four dimensions (52-channel FDR-corrected p > 0.05).

The task design of the verbal fluency task (VFT).
No significant correlation was observed in any channel between changes in mean deoxy-Hb and component five-factor PANSS scores in participants with schizophrenia (52-channel FDR-corrected p > 0.05).
All six channels that were significantly correlated with depression/anxiety component scores significantly contributed to depression/anxiety component scores, as revealed by multiple regression analyses (β = −0.517 to −0.340; p < 0.05; Table 2). Age, task performance on the VFT, GAF score, duration of illness, and daily dosage of antipsychotic drugs did not significantly contribute to cortical activity. Premorbid IQ and gender significantly contributed to one channel each (ch23 and ch52, respectively; Table 2).
Discussion
In this study, we measured changes in Hb concentration in the PFC and temporal cortex during a VFT by using 52-channel NIRS imaging. To our knowledge, this is the first study performed using multi-channel NIRS to identify the relationship between VFT-related hemodynamic responses in the fronto-temporal regions and depressive symptoms in patients with schizophrenia. Notably, ventrolateral PFC, right dorsolateral PFC, and left temporal hemodynamic responses during the VFT were correlated with depression/anxiety component scores of the PANSS, even after controlling for VFT performance and demographic factors. These results suggest an association between fronto-temporal activities and depression/anxiety symptom severity in patients with schizophrenia; further, NIRS imaging may be helpful in understanding the neural basis of depressive symptoms.
According to a review by Drevets21, a complex relationship exists between depression symptom severity and metabolic activity in the orbital cortex and ventrolateral PFC. Noda et al.22 recently described an association between VFT-related oxy-Hb change in the right dorsolateral PFC and severity of depressive symptoms in patients with MDD. Even in the absence of direct effects of anxiety on performance, some studies have shown that anxiety may be associated with prefrontal activity27,28,29. A study performed using fMRI observed that lower dorsolateral and ventrolateral PFC activities27 corresponded to higher state anxiety, whereas lower dorsolateral and ventral PFC activities corresponded to higher trait anxiety27,30. A study on generalized anxiety disorder revealed that more severe anxiety symptoms are associated with decreased activities of the ventrolateral PFC in response to emotional stimuli31. The findings of these studies indicate that abnormal PFC function is associated with pathological depression/anxiety. In the present study, we observed that oxy-Hb change during VFT was negatively correlated with depression/anxiety component scores of the PANSS in the ventrolateral PFC and right dorsolateral PFC regions. The depression/anxiety component consists of 5 items, i.e., somatic concern (G1), anxiety (G2), feelings of guilt (G3), depression (G6), and preoccupation (G15), and focuses on emotional distress as a unique symptom of schizophrenia32. Emotional distress is comprehensively described as the reaction of an individual to external and internal stressors and is characterized by a mixture of sub-threshold distress symptoms such as obsessiveness, depression, hostility, hypersensitivity, anxiety, and paranoid ideation33,34. Myin Germeys35 indicated that increased emotional reactivity is negatively correlated with cognitive impairment in patients with schizophrenia. Data on emotional processes suggest a common neural network involving the PFC, amygdala, insula, basal ganglia, and anterior cingulate36,37. The PFC, specifically the ventrolateral PFC, is a brain area that is critical for the integration of emotional information and the regulation of the intensity of emotional responses38,39. Cognitive control processes supported by the dorsolateral PFC have indeed been revealed to modulate the prediction, generation, interpretation, or regulation of emotions and to translate affectively valenced motivational states into goal-oriented behavior40,41. This general pattern of reduced prefrontal signalling in the context of maintaining affective information is consistent with a body of evidence indicating that schizophrenia is associated with reduced dorsolateral PFC signals during cognitive control and working memory tasks42. Ursu et al.41 suggested that schizophrenia is characterized by a failure of prefrontal circuitry supporting the link between emotion and goal-directed behaviour, arguing that the failure of this mechanism may contribute to deficits in processes related to emotion-cognition interaction. Anticevic and Corlett43 argue that this cardinal “emotional” symptom of psychosis can, at least in part, be conceptualized as a breakdown in the interaction of emotion and cognition. Taken together, these findings suggest that the hemodynamic response observed in the PFC region during the VFT in the present study was associated with depressive symptoms. The functional properties of the PFC are particularly important from a clinical point of view, since they may provide insight into to improve depressive symptoms in subjects with schizophrenia.
In the present study, we further observed that oxy-Hb change during VFT was negatively correlated with depression/anxiety component scores in the left superior temporal cortical region. Structural brain imaging and neuropsychological studies have indirectly shown that depressed mood in schizophrenia and MDD may have at least partially overlapping neurobiology, such as volumetric abnormalities of the temporal lobe and anterior cingulate8,44. A very recent NIRS imaging study observed that oxy-Hb change during VFT in the left temporal regions is associated with depression symptom severity in patients with bipolar disorder43. Therefore, fronto-temporal activity as measured using NIRS may be associated with depression/anxiety symptoms, irrespective of diagnosis.
Depressive symptoms are particularly ubiquitous in the disease process or clinical staging of various psychiatric disorders45. Depressive symptoms that fulfil the operational diagnostic criteria for a depressive episode/major depression can also occur at any stage of schizophrenia, and depressive symptoms in schizophrenia are known to have detrimental consequences such as a high relapse rate, suicidal ideation, increased mortality, reduced social adjustment, and poor quality of life4,7,8,9. Despite the clinical significance of depressive symptoms in patients with schizophrenia, little is known regarding the underlying neurobiological correlates. The results of the present study indicate that fronto-temporal activities measured using NIRS are significantly correlated with depressive symptoms in patients with schizophrenia. Whether the similar finding can be obtained across diagnostic categories is beyond the scope of the study and awaits further studies using patients with various psychiatric diseases.
Interestingly, a correlation was observed only between five-factor model PANSS scores and neural activity in the PFC. Significant relationships were not observed between the original form of PANSS scores (positive, negative, and general psychopathology) and NIRS data. The present finding is consistent with those of previous studies on patients with schizophrenia indicating that the hemodynamic response in the PFC during a cognitive task was related to the five-factor model of the PANSS, but not to the severity of symptoms as evaluated using the conventional PANSS subscales46,47. Marumo et al.46 reported an association between disorganization factor scores and less pronounced changes in deoxy-Hb levels in the PFC region during a category fluency task. Further, Nishimura et al.47 indicated an association between less pronounced changes in oxy-Hb levels in the PFC region during a Go/NoGo task and excitement factor scores as assessed by the five-factor model of the PANSS in patients with schizophrenia. Dysregulation in such distributed neural systems is thought to cause diverse symptoms such as disturbances in perception (hallucinations) and belief (delusions) and emotional dysfunction (amotivation and anhedonia), as well as severe deficits in complex cognitive operations such as working memory, long-term memory, and executive functioning43,48. Taken together, these findings indicate that NIRS imaging maybe helpful in understanding the neural basis of the five-factor model of the PANSS, and that the five-factor model scores of schizophrenic patients may better reflect PFC dysfunction, which is a plausible neural basis of schizophrenia, than the conventional PANSS subscales used for the evaluation of these patients.
The results of the present study must be interpreted with caution due to certain limitations. First, multi-channel NIRS has limited spatial resolution, unlike fMRI and positron emission tomography. Second, because the analysis was based on cross-sectional data, causality could not be determined. Longitudinal studies are required to assess the cause-and-effect relationships. Third, our sample size was not large and is thus subject to type II errors. Further studies involving larger numbers of patients with schizophrenia are required. Further limitations include lack of reliable information on the proportion of patients who met the DSM criteria for current/past MDD and possible confounding effects of different types and dosages of medications. Future longitudinal investigations should be conducted while monitoring diagnoses of depression and medications. Indeed, medication usage may have influenced the results of the present study. Though only three patients in the study were taking antidepressants, all patients were taking antipsychotics at the time of evaluation, the effects of which should not be ignored. However, we found no significant relationship between chlorpromazine equivalent dosage of daily antipsychotic drugs and depression/anxiety component scores (rho = 0.192; p > 0.05). Although antipsychotic dosage levels exhibited significant negative correlations with oxy-Hb changes in two channels (ch10: rho = −0.421, p = 0.020; ch13: rho = 0.404, p = 0.012), those channels (ch23, ch24, ch34, ch42, ch50, and ch52) in which we observed significant correlation between oxy-Hb changes and depression/anxiety component scores were not among these two channels. Therefore, we suspect that the effect of medication on the results may be minimal.
In conclusion, despite these limitations, our results revealed that fronto-temporal activity measured by NIRS is significantly correlated with the PANSS five-factor model in patients with schizophrenia. Such a result may be particularly relevant for the depression/anxiety component and suggests that assessment and training for fronto-temporal activities might improve outcomes in patients with schizophrenia. Further studies with larger sample sizes are required to verify our findings. If confirmed, our findings may allow investigators to evaluate the potential of NIRS as a neuroimaging biomarker for the assessment of depression/anxiety components in patients with schizophrenia.
Materials and Methods
Subjects
Forty-one Japanese patients with schizophrenia who were outpatients at the Tottori University Hospital were included in the study (Table 1). All patients were diagnosed by experienced psychiatrists (A.M., M.I., or I.N.) based on the criteria specified in the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV, American Psychiatric Association 1994)49 by using the Mini-International Neuropsychiatric Interview50. All patients were receiving treatment with antipsychotics, anxiolytics, and/or antiparkinsonian agents during the study. Fourteen patients were taking olanzapine; 10, aripiprazole; eight, blonanserin; four, quetiapine; three, risperidone; and two, perospirone. The exclusion criteria were as follows: any comorbid neurological illness, previous traumatic brain injury with any known cognitive consequences or loss of consciousness lasting more than 5 min, a history of electroconvulsive therapy, and alcohol/substance abuse or addiction.
All participants provided written informed consent and were recruited from January 2008 to December 2012 on the basis of consecutive referrals. All participants were right-handed according to the Edinburgh Handedness Inventory51 and were native Japanese speakers. Premorbid IQ was estimated using the Japanese version of the National Adult Reading Test52. The study was approved by the Ethics Committee of the Tottori University Faculty of Medicine (approval No., 885), and the investigation was conducted in accordance with the latest version of the Declaration of Helsinki.
Clinical evaluation
On the day of the NIRS experiment, psychiatric symptoms and global functioning were evaluated by the same psychiatrist (A.M., M.I., or I.N.) using the PANSS1 and the Global Assessment of Functioning scale (GAF; American Psychiatric Association, 1994)49, respectively. We used a five-factor model of PANSS as proposed by Lindenmayer et al.32. The component subscales of this model were as follows: positive (total scores of P1, P5, P6, and G9), negative (total scores of N1, N2, N3, N4, N6, and G16), excitement (total scores of P4, P7, G4, and G14), depression/anxiety (total scores of G1, G2, G3, G6, and G15), and cognitive (total scores of P2, N5, G5, G10, and G11).
Cognitive task
The task procedure was similar to that of Takizawa et al.9. Hb changes were measured during the VFT (letter version). Each subject sat in a comfortable chair during the NIRS measurements and was instructed to minimize movement of the head, strong biting, and eye blinking to avoid artefacts. The 160-s block-design VFT contained three different periods: a 30-s pre-task period, 60-s task period, and 70-s post-task period (Fig. 2). For the pre- and post-task baseline periods, participants were instructed to repeat consecutively the five Japanese vowels (a, i, u, e, and o) aloud. Hb change was calculated as the difference in concentration between the syllable-repeating condition in the pre-task baseline period and the verbal fluency condition in the task period. The subjects were required to repeat syllables during the baseline periods in the VFT, instead of remaining silent as in other studies. This procedure enables one to differentiate between the utterance process and the word-generating process17.The contrast between the verbal fluency condition and vocalization condition was used to increase the specificity for verbal fluency of the readout from the NIRS. During the task period, participants were instructed to generate as many Japanese words beginning with a designated syllable as possible. The three sets of initial syllables (A: /to/, /se/, /o/; B: /a/, /ki/, /ha/; C: /na/, /i/, /ta/) were presented in a counterbalanced order among the participants, and each syllable was changed every 20 s during the 60-s task. The total number of correct words generated during the VFT was adopted as the measure of task performance.

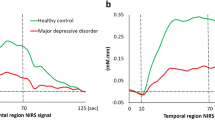
(a) Brain area in yellow corresponds to the near-infrared spectroscopy (NIRS) channels in which mean oxy-Hb changes show significant correlation with depression/anxiety component scores (Spearman’s correlation coefficient; false discovery rate (FDR)-corrected p < 0.05). The locations of NIRS channels were probabilistically estimated and anatomically labelled in the standard Montreal Neurological Institute brain space in accordance with Tsuzuki et al.57. (b) Scatter diagrams depicting the relationship between depression/anxiety component scores and mean oxy-Hb changes in channels 24 (right dorsolateral prefrontal cortex (PFC)), 34 (right ventrolateral PFC), 50 (left ventrolateral PFC), and 52 (left superior temporal cortical).
NIRS methodology
A 52-channel NIRS (ETG-4000; Hitachi Medical Co.) machine was used to measure changes in Hb concentration. The NIRS probe comprised 3 × 11 arrays with 17 emitters and 16 detectors. The NIRS probe machine was placed on the fronto-temporal region of each participant, with the midcolumn of the probe located over the Fpz and the lowest probes located along the T3-Fp1-Fpz-Fp2-T4 line, in accordance with the international 10–20 System used in electroencephalography. The distance between pairs of source-detector probes was set at 3 cm, and each measurement area between the pairs of probes was defined as a “channel” (ch). The machine measures activities along the light path at a depth of 2–3 cm below the scalp, which corresponds well with the surface of the cerebral cortex53,54. According to the LONI Probabilistic Brain Atlas (LPBA40)55, NIRS channels can record bilateral functional hemodynamics within the frontal, temporal, and parietal cortices. Similar to our previous study9,56, we anatomically labelled NIRS channels only after the LPBA region of highest probability was determined. The spatial information from each channel was estimated using the functions from the Functional Brain Science Laboratory at the Jichi Medical University in Japan (http://www.jichi.ac.jp/brainlab/virtual_reg.html)57.
NIRS measures change in both oxy-Hb and deoxy-Hb at two wavelengths (695 and 830 nm) of infrared light, based on the modified Beer–Lambert law58. In this NIRS system, these Hb values include a differential path length factor (DPF); therefore, Hb concentrations from baseline to activation periods were recorded. The relative changes in Hb concentration were indicated as millimoles per millimetre.
The sampling frequency was 10 Hz. To examine VFT-related activities, data for Hb changes were analysed according to the “integral mode”: the pre-task baseline was determined as the mean across 10-s just before the task period, while the post-task baseline was determined as the mean across 5-s, 50-s after the task period. Assuming that task-related activities returns to a pre-task baseline level at a constant interval, linear fitting was performed using the Hb data obtained between the pre-task and post-task baselines. The same procedure has been often used in NIRS studies9,17,18 (Fig. 2). A moving-average method, involving the use of a 5-s window, was applied to remove any short-term motion artefacts. In addition, noise related to body-movement artefacts (no signal, high frequency, and low frequency) were rejected using the algorithm published by Takizawa et al.9,18.
The mean changes in oxy-Hb (as opposed to those in deoxy-Hb) were measured during the VFT as an index of cortical activity because oxy-Hb better reflects this activity and shows stronger correlations with blood oxygenation level-dependent signals as measured by fMRI15,59,60, although the analyses of the mean changes in deoxy-Hb are also presented.
Statistical Analysis
Statistical analyses were performed using SPSS 19.0 software (Tokyo, Japan).
The mean Hb changes of the pre-task baseline period and that of the task period were compared using paired two-tailed t-tests for each channel to confirm the activities area during the VFT.
Because the Shapiro–Wilk test revealed that the original three-factor (positive, negative, and general psychopathology) and five-factor components of the PANSS are not normally distributed, Spearman’s correlation coefficients (r) were calculated to explore the relationships between mean Hb changes during the VFT and the original three-factor and five-factor components of the PANSS. In addition, to elucidate the independent contributions of the depressive symptom components of the PANSS to mean Hb changes in those channels that showed significant correlations, we performed stepwise multiple regression analyses. In these analyses, the mean Hb changes were the dependent variables, and other potential confounding variables were controlled, such as age, gender (dummy parameterized, male = 1, female = 0), premorbid IQ, task performance on the VFT, Global Assessment of Functioning (GAF) score, duration of illness, and daily dosage of antipsychotic drugs used in the analyses of schizophrenia, with a probability of F for a conservative entry and removal criteria of 0.05 and 0.2, respectively. For significant findings, effect sizes were indicated using the standardized regression coefficient (β). Statistical significance was set at p < 0.05, and multiple comparisons among the 52 channels were corrected using the false discovery rate (FDR) method61.
Additional Information
How to cite this article: Pu, S. et al. Associations between depressive symptoms and fronto-temporal activities during a verbal fluency task in patients with schizophrenia. Sci. Rep. 6, 30685; doi: 10.1038/srep30685 (2016).
References
Kay, S. R., Fiszbein, A. & Opler, L. A. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull. 13, 261–276 (1987).
Emsley, R., Rabinowitz, J. & Torreman, M. RIS-INT-35 Early Psychosis Global Working Group. The factor structure for the Positive and Negative Syndrome Scale (PANSS) in recent-onset psychosis. Schizophr Res. 61, 47–57 (2003).
Watanabe, K. et al. Associations between five-factor model of the Positive and Negative Syndrome Scale and plasma levels of monoamine metabolite in patients with schizophrenia. Psychiatry Res. 230, 419–423 (2015).
an der Heiden, W., Könnecke, R., Maurer, K., Ropeter, D. & Häfner, H. Depression in the long-term course of schizophrenia. Eur Arch Psychiatry Clin Neurosci. 255, 174–184 (2005).
Yung, A. R. & McGorry, P. D. The prodromal phase of first-episode psychosis: past and current conceptualizations. Schizophr Bull. 22, 353–370 (1996).
Zisook, S., Nyer, M., Kasckow, J., Golshan, S., Lehman, D. & Montross, L. Depressive symptom patterns in patients with chronic schizophrenia and subsyndromal depression. Schizophr Res. 86, 226–233 (2006).
Häfner, H., Löffler, W., Maurer, K., Hambrecht, M. & an der Heiden, W. Depression, negative symptoms, social stagnation and social decline in the early course of schizophrenia. Acta Psychiatr Scand. 100, 105–118 (1999).
Kumari, V. et al. Mapping Depression in Schizophrenia: A Functional Magnetic Resonance Imaging Study. Schizophr Bull. pii: sbv186. [Epub ahead of print] (2015).
Takizawa, R. et al. Neuroimaging-aided differential diagnosis of the depressive state. Neuroimage. 85, Pt 1, 498–507 (2014).
Badcock, J. C. & Hugdahl, K. Cognitive mechanisms of auditory verbal hallucinations in psychotic and non-psychotic groups. Neurosci Biobehav Rev. 36, 431–438 (2012).
Fletcher, P. C. & Frith, C. D. Perceiving is believing: a Bayesian approach to explaining the positive symptoms of schizophrenia. Nat Rev Neurosci. 10, 48–58 (2009).
Glahn, D. C. et al. Beyond hypofrontality: a quantitative meta-analysis of functional neuroimaging studies of working memory in schizophrenia. Hum Brain Mapp. 25, 60–69 (2005).
Minzenberg, M. J., Laird, A. R., Thelen, S., Carter, C. S. & Glahn, D. C. Meta-analysis of 41 functional neuroimaging studies of executive function in schizophrenia. Arch Gen Psychiatry. 66, 811–822 (2009).
Strangman, G., Boas, D. A. & Sutton, J. P. Non-invasive neuroimaging using near-infrared light. Biological Psychiatry. 52, 679–693 (2002).
Sato, H. et al. A NIRS-fMRI investigation of prefrontal cortex activity during a working memory task. Neuroimage 83, 158–173 (2013).
Ehlis, A. C., Herrmann, M. J., Plichta, M. M. & Fallgatter, A. J. Cortical activation during two verbal fluency tasks in schizophrenic patients and healthy controls as assessed by multi-channel near-infrared spectroscopy. Psychiatry Res. 156, 1–13 (2007).
Suto, T., Fukuda, M., Ito, M., Uehara, T. & Mikuni, M. Multichannel near-infrared spectroscopy in depression and schizophrenia: cognitive brain activation study. Biol Psychiatry. 55(5), 501–511 (2004).
Takizawa, R. et al. Reduced frontopolar activation during verbal fluency task in schizophrenia: a multi-channel near-infrared spectroscopy study. Schizophr Res. 99, 250–262 (2008).
Koike, S. et al. Different hemodynamic response patterns in the prefrontal cortical sub-regions according to the clinical stages of psychosis. Schizophr Res. 132, 54–61 (2011).
Pu, S. et al. Self-reported social functioning and prefrontal hemodynamic responses during a cognitive task in schizophrenia. Psychiatry Res. 234, 121–129 (2015).
Drevets, W. C. Neuroimaging studies of mood disorders. Biol Psychiatry. 48, 813–829 (2000).
Noda, T. et al. Frontal and right temporal activations correlate negatively with depression severity during verbal fluency task: a multi-channel near-infrared spectroscopy study. Frontal and right temporal activations correlate negatively with depression severity during verbal fluency task: a multi-channel near-infrared spectroscopy study. J Psychiatr Res. 46, 905–912 (2012).
Bench, C. J., Frackowiak, R. S. & Dolan, R. J. Changes in regional cerebral blood flow on recovery from depression. Psychol Med. 25, 247–261 (1995).
Mayberg, H. S., Lewis, P. J., Regenold, W. & Wagner, H. N. Jr. Paralimbic hypoperfusion in unipolar depression. J Nucl Med. 35, 929–934 (1994).
Kohler, C., Swanson, C. L., Gur, R. C., Mozley, L. H. & Gur, R. E. Depression in schizophrenia: II. MRI and PET findings. Biol Psychiatry. 43, 173–180 (1998a).
Kohler, C., Gur, R. C., Swanson, C. L., Petty, R. & Gur, R. E. Depression in schizophrenia: I. Association with neuropsychological deficits. Biol Psychiatry. 43, 165–172 (1998b).
Bishop, S. J. Trait anxiety and impoverished prefrontal control of attention. Nat Neurosci. 12, 92–98 (2009).
Righi, S., Mecacci, L. & Viggiano, M. P. Anxiety, cognitive self-evaluation and performance: ERP correlates. J Anxiety Disord. 23, 1132–1138 (2009).
Bishop, S., Duncan, J., Brett, M. & Lawrence, A. D. Prefrontal cortical function and anxiety: controlling attention to threat-related stimuli. Nat Neurosci. 7, 184–188 (2004).
Indovina, I., Robbins, T. W., Núñez-Elizalde, A. O., Dunn, B. D. & Bishop, S. J. Fear-conditioning mechanisms associated with trait vulnerability to anxiety in humans. Neuron. 69, 563–571 (2011).
Monk, C. S. et al. Ventrolateral prefrontal cortex activation and attentional bias in response to angry faces in adolescents with generalized anxiety disorder. Am J Psychiatry. 163, 1091–1097 (2006).
Lindenmayer, J. P., Bernstein-Hyman, R. & Grochowski, S. Five-factor model of schizophrenia. Initial validation. J Nerv Ment Dis. 182, 631–638 (1994).
Derogatis, L. R. & Coons. H. L. Self-report measures of stress in Handbook of Stress 2nd edn, 200–233 (The Free Press, New York, 1993).
Dohrenwend, B. P., Shrout, P. E., Egri, G. & Mendelsohn, F. S. Nonspecific psychological distress and other dimensions of psychopathology. Measures for use in the general population. Arch Gen Psychiatry. 37, 1229–1236 (1980).
Myin-Germeys, I., Krabbendam, L., Jolles, J., Delespaul, P. A. & van Os, J. Are cognitive impairments associated with sensitivity to stress in schizophrenia? An experience sampling study. Am J Psychiatry. 159, 443–449 (2002).
Davidson, R. J. & Irwin, W. The functional neuroanatomy of emotion and affective style. Trends Cogn Sci. 3, 11–21 (1999).
Dolan, R. J. Emotion, cognition, and behavior. Science. 298, 1191–1194 (2002).
Cabeza, R. & Nyberg, L. Imaging cognition II: An empirical review of 275 PET and fMRI studies. J Cogn Neurosci. 12, 1–47 (2000).
Fuster, J. The Prefrontal Cortex. (Raven Press, New York, 1989).
Ochsner, K. N. & Gross, J. J. The cognitive control of emotion. Trends Cogn Sci. 9, 242–249 (2005).
Ursu, S. et al. Prefrontal cortical deficits and impaired cognition-emotion interactions in schizophrenia. Am J Psychiatry. 168, 276–285 (2011).
Van Snellenberg, J. X., Torres, I. J. & Thornton, A. E. Functional neuroimaging of working memory in schizophrenia: task performance as a moderating variable. Neuropsychology. 20, 497–510 (2006).
Anticevic, A. & Corlett, P. R. Cognition-emotion dysinteraction in schizophrenia. Front Psychol. 3, 392 (2012).
Mikawa, W., Tsujii, N., Akashi, H., Adachi, T., Kirime, E. & Shirakawa, O. Left temporal activation associated with depression severity during a verbal fluency task in patients with bipolar disorder: a multichannel near-infrared spectroscopy study. J Affect Disord. 173, 193–200 (2015).
Häfner H., Maurer K., Trendler G., an der Heiden W. & Schmid t M. The early course of schizophrenia and depression*. Eur Arch Psychiatry Clin Neurosci. 255, 167–173 (2005).
Marumo, K. et al. Functional abnormalities in the left ventrolateral prefrontal cortex during a semantic fluency task, and their association with thought disorder in patients with schizophrenia. Neuroimage. 85 Pt 1, 518–526 (2014).24. Mayberg, H.S., Lewis, P.J., Regenold, W., Wagner, H.N. Jr. Paralimbic hypoperfusion in unipolar depression. J Nucl Med. 35, 929-934 (1994).
Nishimura, Y., Takizawa, R., Muroi, M., Marumo, K., Kinou, M. & Kasai, K. Prefrontal cortex activity during response inhibition associated with excitement symptoms in schizophrenia. Brain Res. 1370, 194–203 (2011).
Barch, D. M. & Ceaser, A. Cognition in schizophrenia: core psychological and neural mechanisms. Trends Cogn Sci. 16, 27–34 (2012).
American Psychiatric Association. Diagnostic and statistical manual of mental disorders (DSM-IV, 1994). (American Psychiatric Association, 1994).
Sheehan, D. V. et al. The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. 59, 22–33 (1998).
Oldfield, R. C. The assessment and analysis of handedness: the Edinburgh inventory. Neuropsychologia. 9, 97–113 (1971).
Matsuoka, K., Uno, M., Kasai, K., Koyama, K. & Kim, Y. Estimation of premorbid IQ in individuals with Alzheimer’s disease using Japanese ideographic script (Kanji) compound words: Japanese version of National Adult Reading Test. Psychiatry Clin Neurosci. 60, 332–339 (2006).
Okada, E. & Delpy, D. T. Near-infrared light propagation in an adult head model. II. Effect of superficial tissue thickness on the sensitivity of the near-infrared spectroscopy signal. Appl Opt. 42, 2915–2922 (2003).
Toronov, V. et al. Investigation of human brain hemodynamics by simultaneous near-infrared spectroscopy and functional magnetic resonance imaging. Med Phys. 28, 521–527 (2001).
Shattuck, D. W. et al. Construction of a 3D probabilistic atlas of human cortical structures. Neuroimage. 39, 1064–1080 (2008).
Pu, S. et al. Prefrontal activation predicts social functioning improvement after initial treatment in late-onset depression. J Psychiatr Res. 62, 62–70 (2015).
Tsuzuki, D., Jurcak, V., Singh, A. K., Okamoto, M., Watanabe, E. & Dan, I. Virtual spatial registration of stand-alone fNIRS data to MNI space. Neuroimage. 34, 1506–1518 (2007).
Yamashita, Y., Maki, A., Ito,Y., Watanabe, E. & Koizumi, H. Noninvasive near-infrared topography of human brain activity using intensity modulation spectroscopy. Optical Engineering. 35, 1046–1049 (1996).
Hoshi, Y., Kobayashi, N. & Tamura, M. Interpretation of near-infrared spectroscopy signals: a study with a newly developed perfused rat brain model. J. Appl. Physiol. 90, 1657–1662 (2001).
Strangman, S., Culver, J. P., Thompson, J. H. & Boas, D. A. A quantitative comparison of simultaneous BOLD fMRI and NIRS recording during functional brain activation. Neuroimage. 17, 719–731 (2002).
Singh, A. K. & Dan, I. Exploring the false discovery rate in multichannel NIRS. Neuroimage. 33, 542–549 (2006).
Acknowledgements
We would like to thank the participants for their valuable involvement in the study. This research was supported by an Intramural Research Grant for Neurological and Psychiatric Disorders from the NCNP (National Center of Neurology and Psychiatry) (No. 23-10 and 26-3 to K.K. and S.P.) and by the Takeda Science Foundation (No. 2014 to S.P.). The authors would also like to thank Hitachi Medical Corporation for the ETG-4000 equipment, and the skilled technical and methodical support provided.
Author information
Authors and Affiliations
Contributions
S.P., K.N., A.M., M.I., I.N. and K.K. were involved in the collection of the data. S.P. wrote the manuscript. S.P., K.N. and K.K. supervised the entire project. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Pu, S., Nakagome, K., Miura, A. et al. Associations between depressive symptoms and fronto-temporal activities during a verbal fluency task in patients with schizophrenia. Sci Rep 6, 30685 (2016). https://doi.org/10.1038/srep30685
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep30685
This article is cited by
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
