
Abstract
Left atrial (LA) strain can reflect LA remodeling and is reduced in atrial fibrillation (AF) patients with prior stroke. This study sought to examine the ability of LA strain in predicting subsequent stroke event in AF and also evaluated whether E/LA strain could predict cardiovascular (CV) events in these patients. In 190 persistent AF patients, we performed comprehensive echocardiography with assessment of LA strain. There were 69 CV events including 19 CV death, 32 hospitalizations for heart failure, 3 myocardial infarctions and 15 strokes during an average follow-up of 29 months. Multivariate analysis showed old age, chronic heart failure, increased left ventricular (LV) mass index and increased E/LA strain were associated with CV events and decreased LA strain was associated with subsequent stroke event. The addition of E/LA strain and LA strain to a model containing CHA2DS2-VASc score and LV function significantly improved the values in predicting CV events and subsequent stroke event, respectively. In conclusion, E/LA strain and LA strain were respectively useful in predicting CV events and subsequent stroke event in AF. E/LA strain and LA strain could provide incremental values for CV outcome and subsequent stroke outcome prediction over conventional clinical and echocardiographic parameters in AF, respectively.
Similar content being viewed by others

Introduction
Atrial fibrillation (AF) is the most common form of cardiac arrhythmia and patients with AF are associated with an increased risk of stroke, heart failure and cardiovascular (CV) mortality1,2. The traditionally echocardiographic parameters associated with an increased risk of stroke are increased left atrial (LA) dimension, decreased LA appendage flow velocity and proof of thrombi or spontaneous echo contrast3,4.
Two-dimensional echocardiographic speckle tracking can accurately measure left ventricular strain and strain rate5,6. This imaging method has also been used for the assessment of LA function7,8. LA remodeling, including structural, functional and electrical changes is frequently noted in patients with AF. Severely impaired LA strain may reflect more advanced LA remodeling9,10. LA strain is also correlated with LA fibrosis in patients irrespective of the presence of AF or not11,12. Additionally, LA strain is significantly reduced in AF patients with prior stroke compared to those without prior stroke13. LA strain and LA volume may provide complementary information on structural changes of the left atrium, but it is speculated that LA strain may be a more sensitive parameter of changes in LA wall structure. However, there is no study to evaluate whether LA strain is a useful predictor of subsequent stroke in patients with AF. In addition, several echocardiographic combination indices generated by the ratio of transmitral E-wave velocity (E) to left ventricular diastolic parameters can effectively predict CV outcomes14,15,16,17. LA strain has been demonstrated to be associated with left ventricular diastolic function18. We hypothesize the combination index, E/LA strain, is also a useful parameter in predicting CV events in AF patients. Hence, this study was designed to investigate whether E/LA strain and LA strain could respectively predict adverse CV events and subsequent stroke event in patients with AF.
Methods
Study patients
This observational cohort study prospectively and consecutively included patients with persistent AF referred for echocardiographic examinations at Kaohsiung Municipal Hsiao-Kang Hospital from April 2010 to June 2012. Persistent AF was defined as AF lasting for at least 7 days. Patients with moderate and severe mitral stenosis (n = 5), moderate and severe aortic stenosis or regurgitation (n = 4), severe mitral regurgitation (n = 5) and inadequate echocardiographic visualization (n = 11) were excluded. Additionally, four patients who had no beat fulfilling the requirements of index beat in the stored cardiac cycles were also excluded. Finally, 190 AF patients were included in this study. The study protocol was approved by our Institutional Review Board and all enrolled patients gave written, informed consent.
Echocardiographic evaluation
The echocardiographic examination was performed by one experienced cardiologist with a VIVID 7 (General Electric Medical Systems, Horten, Norway). The cardiologist was blinded to the clinical data. Pulsed tissue Doppler imaging was obtained with the sample volume placed at the lateral and septal corners of the mitral annulus from the apical 4-chamber view. Early diastolic mitral annulus velocity (E’) was averaged from septal and lateral ones. The wall filter settings were adjusted to exclude high-frequency signals and the gain was minimized. Left ventricular ejection fraction (LVEF) was measured using the modified Simpson’s method. Left atrial volume was measured using the biplane area-length method19. Left atrial volume index (LAVI) was calculated by dividing left atrial volume by body surface area.
LA strain measurement
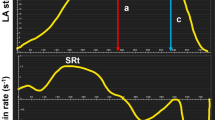
The endocardial border was manually defined using a point-and-click technique. An epicardial surface tracing was automatically generated by the system, creating a region of interest, which was manually adjusted to cover the full thickness of left atrium. Time-strain plot was produced automatically by the software. Global LA strain during the reservoir phase was estimated by taking the average of longitudinal strain data obtained from the apical four-chamber and two chamber projections10,13,20. Data from a total of 12 LA segments (annular, mid and superior segments along the septal, lateral, anterior and inferior LA walls using apical four-chamber and two-chamber images) were averaged to determine global longitudinal LA strain at the end of left ventricular ejection (LA reservoir phase). Assessment of LA strain was accepted if at least four of the six LA segments in each view could be measured clearly. We used cine loops to determine which beat would be calculated. The raw ultrasonic data, including 15 consecutive beats from the apical four-chamber and two-chamber views, was recorded and analyzed offline using EchoPAC software (EchoPAC version 08; GE-Vingmed Ultrasound AS GE Medical Systems).
Left ventricular dimensions, LVEF, LAVI and LA strain were measured from the index beat method21,22. Because their measurements were easy and rapid, the E, E-wave deceleration time and E’ were obtained from five beats23 and then averaged for later analysis. If the cardiac cycle length was too short to complete the diastolic process, this beat was skipped. Thus, the selection of E, E-wave deceleration time and E’ was not always consecutive. In addition, heart rate was determined from five consecutive beats.
Collection of demographic, medical and laboratory data
Demographic and medical data including age, gender and history of diabetes mellitus, hypertension, coronary artery disease, stroke and chronic heart failure were obtained from medical records or interviews with patients. Laboratory data including total cholesterol and triglyceride were also collected. In addition, information regarding patient medications during the study period was obtained from medical records.
Definition of CV events
CV events were defined as CV mortality, hospitalization for heart failure, myocardial infarction and stroke. Hospitalization for heart failure was defined as admission due to dyspnea with chest radiographic evidence of pulmonary congestion and treatment with intravenous diuretics. CV events were ascertained and adjudicated by two cardiologists with disagreement resolved by adjudication from a third cardiologist from the hospital course and medical record. If patients had multiple CV events, only the first event was coded. However, if patients died after episodes of heart failure, myocardial infarction, or stroke during the same admission, they were coded as CV death. In patients reaching the study end points, they were followed until the first episode of adverse events. The other patients were followed until March 2014.
Statistical analysis
SPSS 18.0 software (SPSS, Chicago, IL, USA) was used for statistical analysis. Data were expressed as mean ± standard deviation, percentage, or median (25th–75th percentile) for follow-up period. Continuous and categorical variables among groups were compared by one-way analysis of variance (ANOVA) followed by a post hoc test adjusted with a Bonferroni correction and Chi-square test, respectively. The relationship between two continuous variables was assessed by a bivariate correlation method (Pearson’s correlation). The significant variables in the univariate analysis were selected for multivariate analysis. Time to the adverse events and covariates of risk factors were modeled using a Cox proportional hazards model with forward selection. A significant improvement in model prediction was based on the −2 log likelihood ratio statistic, which followed a difference in −2 log likelihood value and the P value was based on the incremental value compared with the previous model. Kaplan-Meier survival plots were calculated from baseline to time of adverse events and compared using the log-rank test. Stepwise multiple linear regression analysis was employed to identify the determinants of LA strain and E/LA strain. All tests were 2-sided and the level of significance was established as P < 0.05.
Results
Table 1 shows the comparison of clinical and echocardiographic characteristics according to the tertile of LA strain. There were significant differences in the age, prevalence of coronary artery disease and chronic heart failure, CHA2DS2-VASc score, heart rate, anticoagulant use, LAVI, left ventricular end-systolic and end-diastolic dimensions, LVEF, E’, E/E’ and LA strain among patients with different tertiles.
The follow-up period to CV events was 29 (25th–75th percentile: 18–36) months in all patients. Sixty-nine CV events were documented during the follow-up period, including CV death (n = 19), hospitalization for heart failure (n = 32), myocardial infarction (n = 3) and stroke (n = 15). A Cox proportional hazards regression analysis for CV events is shown in Table 2. In the multivariate analysis, old age, the presence of chronic heart failure, increased LVMI and increased E/LA strain (hazard ratio [HR], 1.182; 95% confidence interval [CI], 1.086 to 1.286; P < 0.001) were independently associated with increased CV events.
The follow-up period to subsequent stroke event was 30 (25th–75th percentile: 23–41) months in all patients. Eighteen subsequent stroke events were documented during the follow-up period. A Cox proportional hazards regression analysis for subsequent stroke event is shown in Table 3. In the multivariate analysis, only decreased LA strain (HR, 0.844; 95% CI, 0.745 to 0.955; P = 0.007) was independently associated with increased subsequent stroke event.
To find the appropriate cut-off values to E/LA strain and LA strain as predictors of the outcomes, we created several models using different cut-off values of E/LA strain and LA strain. Using the −2 log likelihood value to select the model with the best performance, the model using E/LA strain >6.00 m and LA strain <16.50% had the best performance in predicting the adverse events. Figure 1 illustrates the Kaplan-Meier curves for CV event-free survival and subsequent stroke-free survival in study patients.

Kaplan-Meier analysis of cardiovascular (CV) event-free survival according to the ratio of transmitral E-velocity (E) to left atrial (LA) strain <6.00 or >6.00 m/s (A) and of subsequent stroke event-free survival according to LA strain >16.50 or <16.50% (B).
The incremental values of E/LA strain and LA strain in outcome prediction are shown in Table 4. The addition of E/LA strain and LA strain to a Cox model containing CHA2DS2-VASc score, LAVI, LVEF and E/E’ significantly improved the values in predicting CV events and subsequent stroke event respectively. However, the addition of LA strain and E/LA strain to a Cox model containing CHA2DS2-VASc score, LAVI, LVEF and E/E’ did not improve the values in predicting CV events and subsequent stroke event, respectively.
Discussion
In the present study, we evaluated the association of E/LA strain with CV events and LA strain with subsequent stroke event in patients with AF. We found that increased E/LA strain and decreased LA strain were independently associated with an increase in CV events and subsequent stroke event in AF, respectively. The E/LA strain and LA strain could respectively add significant incremental values beyond the conventional clinical and echocardiographic parameters in prediction of CV events and subsequent stroke event.
Diastolic dysfunction increases left ventricular filling pressure and is the primary mechanism responsible for the clinical findings of heart failure. Echocardiography is the most valuable tool for the noninvasive evaluation of diastolic function24. Several approaches on the basis of Doppler modalities have been proposed as useful methods for the evaluation of left ventricular diastolic function25,26. By combining these parameters with those obtained from the mitral flow curve, a more precise estimation of left ventricular filling pressure has been achieved27,28. E/E’ was reported to be related well to mean pulmonary capillary wedge pressure28 and the ratio of E to global diastolic strain rate had also been proposed as a marker of elevated left ventricular filling pressure29. Ersbøll M et al. showed the ratio of E to global early diastolic strain rate (E’sr) was independently associated with an adverse outcome in patients with myocardial infarction14. Our previous study also showed that E/E’sr was a useful parameter in predicting adverse cardiac events in AF17. LA strain has demonstrated to be associated with left ventricular diastolic function18. Hence, E/LA strain should be a good parameter in the evaluation of left ventricular filling pressure. In fact, the present study showed increased E/LA strain was highly correlated with increased E/E’, a good parameter of left ventricular filling pressure28, in the multivariate analysis. The LA strain has been reported to be useful in predicting CV prognosis in AF patients with acute embolism30. In the present study, although decreased LA strain and increased E/LA strain were associated with CV events in the univariate analysis, only E/LA strain was still associated with adverse CV events after multivariate analysis. Furthermore, the addition of E/LA strain, but not LA strain, to a Cox model consisting of conventional clinical and echocardiographic parameters could cause an improvement in prediction of adverse CV events. Hence, the combination index, E/LA strain, might be more useful in predicting poor CV prognosis in AF patients than LA strain.
Several traditionally echocardiographic parameters including increased LA dimension, decreased LA appendage flow velocity and proof of thrombi or spontaneous echo contrast were associated with an increased risk of stroke3,4. Recently, LA strain was reported to decrease proportionately with increasing CHADS2 score and was an independent predictor of prior stroke13,31. Shih et al. found decreased LA strain and strain rate were independently associated with prior stroke, but E and E/E’ were not13. The finding might indicate that stroke event was correlated better with LA-related parameters. However, this study was a cross-sectional study without long-term outcome data. In addition, it has also been proven that in patients with CHADS2 scores ≦1, LA strain is an independent predictor of prior stroke, when adjusted for LA size, LVEF and left ventricular mass32. In a recent observational study, LA strain provided incremental value for embolism risk stratification over CHA2DS2-VASc score in patients with AF30. In the present study, we similarly found decreased LA strain was correlated with increased CHA2DS2-VASc score in the univariate analysis and further found decreased LA strain was significantly associated with subsequent stroke event even after adjustment for many important echocardiographic parameters. In addition, the addition of LA strain to a Cox model consisting of conventional clinical and echocardiographic parameters could cause an improvement in prediction of subsequent stroke event. Hence, impaired LA strain may be useful in predicting subsequent stroke event in AF patients.
The underlying mechanism of the association between impaired LA strain and subsequent stroke event remains unclear. Previous studies have found there is an association among reduced LA strain, LA fibrosis, lower LA appendage flow velocity and LA appendage thrombus11,33. We hypothesize that LA fibrosis diminishes LA compliance during the LA reservoir phase, which causes blood flow stasis in the left atrium. Therefore, reduced LA strain may contribute to an increased risk for subsequent stroke. However, E/LA strain was not associated with subsequent stroke event, which might also indicate that LA strain itself predicted future stroke event better than parameters of left ventricular filling pressure. On the contrary, E/LA strain might predict future CV events better than LA strain itself because of the close association between E/LA strain and left ventricular filling pressure.
Study limitations
There were several limitations to this study. First, since the subjects of this study were already being evaluated for heart disease by echocardiography, it was susceptible to selection bias, making findings potentially less generalized and making study sample size relatively small. Second, two-dimensional speckle tracking echocardiography could generate LA strain and strain rate curves among different LA cycle phases. In this study, only longitudinal LA strain during the reservoir phase was measured and analyzed. Third, percentage of anticoagulant use was relatively low in our study. According to the literature published by Taiwan Stroke Registry34, only 28.3% were prescribed traditional anticoagulant agent among patients with AF. However, this condition may have gradually improved after new anticoagulant agent use in Taiwan. Finally, echocardiographic parameters in our study were analyzed only by a single operator without core lab readings and outcomes were obtained from medical records only.
Conclusions
In patients with AF, E/LA strain and LA strain were useful in predicting adverse CV events and subsequent stroke event, respectively. Additionally, E/LA strain and LA strain could respectively provide incremental values for CV outcome and subsequent stroke outcome prediction over conventional clinical and echocardiographic parameters in AF.
Additional Information
How to cite this article: Hsu, P.-C. et al. Prognostic role of left atrial strain and its combination index with transmitral E-wave velocity in patients with atrial fibrillation. Sci. Rep. 6, 17318; doi: 10.1038/srep17318 (2016).
References
Go, A. S. et al. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA 285, 2370–2375 (2001).
Feinberg, W. M. et al. Relationship between prothrombin activation fragment F1.2 and international normalized ratio in patients with atrial fibrillation. Stroke Prevention in Atrial Fibrillation Investigators. Stroke 28, 1101–1106 (1997).
Osranek, M. et al. Left atrial volume predicts cardiovascular events in patients originally diagnosed with lone atrial fibrillation: three-decade follow-up. Eur Heart J 26, 2556–2561 (2005).
Daniel, W. G. et al. Left atrial spontaneous echo contrast in mitral valve disease: an indicator for an increased thromboembolic risk. J Am Coll Cardiol 11, 1204–1211 (1988).
Mor-Avi, V. et al. Current and evolving echocardiographic techniques for the quantitative evaluation of cardiac mechanics: ASE/EAE consensus statement on methodology and indications endorsed by the Japanese Society of Echocardiography. J Am Soc Echocardiogr 24, 277–313 (2011).
Su, H. M. et al. Global left ventricular longitudinal systolic strain as a major predictor of cardiovascular events in patients with atrial fibrillation. Heart 99, 1588–1596 (2013).
Vianna-Pinton, R. et al. Two-dimensional speckle-tracking echocardiography of the left atrium: feasibility and regional contraction and relaxation differences in normal subjects. J Am Soc Echocardiogr 22, 299–305 (2009).
D’Andrea, A. et al. Different effects of cardiac resynchronization therapy on left atrial function in patients with either idiopathic or ischaemic dilated cardiomyopathy: a two-dimensional speckle strain study. Eur Heart J 28, 2738–2748 (2007).
Tops, L. F. et al. Left atrial strain predicts reverse remodeling after catheter ablation for atrial fibrillation. J Am Coll Cardiol 57, 324–331 (2011).
Vieira, M. J., Teixeira, R., Goncalves, L. & Gersh, B. J. Left Atrial Mechanics: Echocardiographic Assessment and Clinical Implications. J Am Soc Echocardiogr 27, 463–478 (2014).
Kuppahally, S. S. et al. Left atrial strain and strain rate in patients with paroxysmal and persistent atrial fibrillation: relationship to left atrial structural remodeling detected by delayed-enhancement MRI. Circ Cardiovasc Imaging 3, 231–239 (2010).
Her, A. Y. et al. Prediction of left atrial fibrosis with speckle tracking echocardiography in mitral valve disease: a comparative study with histopathology. Korean Circ J 42, 311–318 (2012).
Shih, J. Y. et al. Association of decreased left atrial strain and strain rate with stroke in chronic atrial fibrillation. J Am Soc Echocardiogr 24, 513–519 (2011).
Ersboll, M. et al. Early diastolic strain rate in relation to systolic and diastolic function and prognosis in acute myocardial infarction: a two-dimensional speckle-tracking study. Eur Heart J 35, 648–656 (2014).
Okura, H. et al. Tissue Doppler-derived index of left ventricular filling pressure, E/E’, predicts survival of patients with non-valvular atrial fibrillation. Heart 92, 1248–1252 (2006).
Moller, J. E., Sondergaard, E., Seward, J. B., Appleton, C. P. & Egstrup, K. Ratio of left ventricular peak E-wave velocity to flow propagation velocity assessed by color M-mode Doppler echocardiography in first myocardial infarction: prognostic and clinical implications. J Am Coll Cardiol 35, 363–370 (2000).
Hsu, P. C. et al. The Ratio of Early Mitral Inflow Velocity to Global Diastolic Strain Rate as a Useful Predictor of Cardiac Outcomes in Patients with Atrial Fibrillation. J Am Soc Echocardiogr (2014).
Wakami, K. et al. Correlation between left ventricular end-diastolic pressure and peak left atrial wall strain during left ventricular systole. J Am Soc Echocardiogr 22, 847–851 (2009).
Lang, R. M. et al. Recommendations for chamber quantification: a report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J Am Soc Echocardiogr 18, 1440–1463 (2005).
Motoki, H. et al. Assessment of left atrial mechanics in patients with atrial fibrillation: comparison between two-dimensional speckle-based strain and velocity vector imaging. J Am Soc Echocardiogr 25, 428–435 (2012).
Govindan, M. et al. Validation of echocardiographic left atrial parameters in atrial fibrillation using the index beat of preceding cardiac cycles of equal duration. J Am Soc Echocardiogr 24, 1141–1147 (2011).
Lee, C. S. et al. Measuring left ventricular peak longitudinal systolic strain from a single beat in atrial fibrillation: validation of the index beat method. J Am Soc Echocardiogr 25, 945–952 (2012).
Sohn, D. W. et al. Mitral annulus velocity in the evaluation of left ventricular diastolic function in atrial fibrillation. J Am Soc Echocardiogr 12, 927–931 (1999).
Nishimura, R. A. & Tajik, A. J. Evaluation of diastolic filling of left ventricle in health and disease: Doppler echocardiography is the clinician’s Rosetta Stone. J Am Coll Cardiol 30, 8–18 (1997).
Takatsuji, H. et al. A new approach for evaluation of left ventricular diastolic function: spatial and temporal analysis of left ventricular filling flow propagation by color M-mode Doppler echocardiography. J Am Coll Cardiol 27, 365–371 (1996).
Sohn, D. W. et al. Assessment of mitral annulus velocity by Doppler tissue imaging in the evaluation of left ventricular diastolic function. J Am Coll Cardiol 30, 474–480 (1997).
Gonzalez-Vilchez, F., Ares, M., Ayuela, J. & Alonso, L. Combined use of pulsed and color M-mode Doppler echocardiography for the estimation of pulmonary capillary wedge pressure: an empirical approach based on an analytical relation. J Am Coll Cardiol 34, 515–523 (1999).
Nagueh, S. F., Middleton, K. J., Kopelen, H. A., Zoghbi, W. A. & Quinones, M. A. Doppler tissue imaging: a noninvasive technique for evaluation of left ventricular relaxation and estimation of filling pressures. J Am Coll Cardiol 30, 1527–1533 (1997).
Kimura, K. et al. Speckle tracking global strain rate E/E’ predicts LV filling pressure more accurately than traditional tissue Doppler E/E’. Echocardiography 29, 404–410 (2012).
Obokata, M. et al. Left Atrial Strain Provides Incremental Value for Embolism Risk Stratification over CHADS-VASc Score and Indicates Prognostic Impact in Patients with Atrial Fibrillation. J Am Soc Echocardiogr (2014).
Saha, S. K. et al. Global left atrial strain correlates with CHADS2 risk score in patients with atrial fibrillation. J Am Soc Echocardiogr 24, 506–512 (2011).
Azemi, T., Rabdiya, V. M., Ayirala, S. R., McCullough, L. D. & Silverman, D. I. Left atrial strain is reduced in patients with atrial fibrillation, stroke or TIA and low risk CHADS(2) scores. J Am Soc Echocardiogr 25, 1327–1332 (2012).
Karabay, C. Y. et al. Left atrial deformation parameters predict left atrial appendage function and thrombus in patients in sinus rhythm with suspected cardioembolic stroke: a speckle tracking and transesophageal echocardiography study. Echocardiography 30, 572–581 (2013).
Hsieh, F. I. et al. Get With the Guidelines-Stroke performance indicators: surveillance of stroke care in the Taiwan Stroke Registry: Get With the Guidelines-Stroke in Taiwan. Circulation 122, 1116–1123 (2010).
Acknowledgements
The research presented in this article is supported by the grant from Kaohsiung Municipal Hsiao-Kang Hospital (kmhk-103-004), Kaohsiung Medical University, Kaohsiung, Taiwan.
Author information
Authors and Affiliations
Contributions
Dr. P.-C.H. and H.-M.S. take responsibility for the research, data, their analyses and interpretation and manuscript writing. Dr. W.-H.L., C.-Y.C., H.-H.L., C.-S.L. and H.-W.Y. take responsibility for the research, data and their analyses and interpretation. Dr. T.-H.L., W.-C.V., W.-T.L. and S.-H.S. critically revised the manuscript for important intellectual content.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Hsu, PC., Lee, WH., Chu, CY. et al. Prognostic role of left atrial strain and its combination index with transmitral E-wave velocity in patients with atrial fibrillation. Sci Rep 6, 17318 (2016). https://doi.org/10.1038/srep17318
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep17318
This article is cited by
-
Long-term prognostic value of left atrial longitudinal strain in an elderly community-based cohort
GeroScience (2023)
-
Ventricular-atrial coupling in subjects with normal, preserved, and reduced left ventricular ejection fraction: insights from cardiac magnetic resonance imaging
European Radiology (2023)
-
Assessment of atria function after percutaneous closure of atrial septal defect using 2D speckle tracking echocardiography
Journal of Echocardiography (2022)
-
Mitral early-diastolic inflow peak velocity (E)-to-left atrial strain ratio as a novel index for predicting elevated left ventricular filling pressures in patients with preserved left ventricular ejection fraction
Cardiovascular Ultrasound (2021)
-
Importance of left atrial mechanical function as a predictor of atrial fibrillation risk following cardiac surgery
The International Journal of Cardiovascular Imaging (2021)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
