
Key Points
-
Helps clinicians recognise a feasible and minimally invasive therapeutic option for management of crown-root fractured teeth.
-
Provides advice on how to achieve the desired outcomes of modified crown lengthening surgery.
-
Provides evidence-based support to save and restore subgingival crown-root fractured teeth through modified crown lengthening surgery combined with endodontic treatment and post and core restoration.
-
Helps in the understanding of factors that affect the periodontal health of teeth after modified crown lengthening surgery and crown restoration.
Abstract
Objectives To evaluate long-term outcomes of modified crown lengthening procedures for crown-root fractured teeth, and to analyse factors that affect the periodontal health of the treated teeth.
Methods The present study retrospectively analysed data from 22 patients (13 males and 9 females) who had presented with crown-root fractured teeth and received modified crown lengthening procedures combined with crown restoration for ≥13 months. In total, 26 crown-root fractured teeth were treated and examined for plaque index, probing depth, bleeding index, bleeding on probing, mobility and the crown margin location. The contralateral tooth and ipsilateral teeth mesial and distal to the treated tooth were used as controls. Data were assessed descriptively or analysed statistically with Mann-Whitney-U test at α=0.05.
Results Recorded periodontal indices revealed stable periodontal status in 25 of 26 treated teeth with the mean values for aesthetic and functional VAS scores at 9.5. A negative correlation was observed between the subgingival crown margin location and the bleeding index.
Conclusions The modified crown lengthening procedure is a feasible and minimally invasive therapeutic option for management of crown-root fractured cases.
Similar content being viewed by others

Introduction
Dentists always encounter challenges in the management of crown-root fractured cases.1,2,3,4 In most instances, oblique crown-root subgingival fracture lines located in close proximity to or below the alveolar bone crest that might result in violation of biological width imply considerable challenges for subsequent restorative procedures.5 The violation of biological width may lead to periodontal disease with resulting bone resorption to create space for an attachment and gingival crevice and thus the resulting bone contours may be unfavourable and conducive to further periodontal breakdown. To ensure long-term periodontal and functional stability, at least 3 mm of sound root structures above the alveolar bone, which would satisfy both the biologic width and 1 to 2 mm gingival crevice, should be surgically created before restoring the crown-root fractured tooth.6,7 Several techniques have been proposed for clinical crown lengthening such as gingivectomy, apically positioned flap surgery, and osseous surgery,6,7,8,9,10,11 but all have some limitation in terms of function or aesthetics. The most common method is surgical crown lengthening.12,13,14,15,16 However, the osteotomy procedure of traditional crown lengthening surgery always sacrifices the bony support of both treated and adjacent teeth, and creates unpleasant aesthetic outcomes such as 'black triangle' formation and unfavourable crown-to-root ratio results.6,8,16
Melker and Richardson16 presented a surgical procedure of reshaping the existing tooth surface in combination with conservative removal of the supporting alveolar bone to create the width needed for the restoration to be biologically acceptable, and proposed that this procedure accomplishes several goals: (1) minimum supporting bone is removed; (2) deleterious root surface anatomy, such as grooves, concavities, and cementoenamel projections, is diminished; (3) a smooth root surface that is more biologically acceptable to soft tissue is created; (4) Class I and II furcation lesions may be decreased or eliminated; and (5) improved gingival contours and space for restorative materials can be created in situations in which close root proximity is present. Hu and colleagues modified the conventional crown lengthening surgery using odontoplasty and osteotomy procedures to manage and preserve seven severe crown-root fractured teeth.17 The data from periodontal indices indicated good to excellent outcomes after an average 17-month recall. Recently, da Cruz et al.18 recalled 14 extensive crown destruction cases after crown lengthening procedure combined with odontoplasty for a mean period of 13.6 months and reported a success rate higher than 85%.
The aim of this study was to observe the long-term effects of modified crown lengthening surgery combined with endodontic treatment and post and core restoration of crown-root fractured cases, and to analyse factors that affect the periodontal health of the treated teeth.
Materials and methods
Patient collection
The research was conducted in full accordance with the World Medical Association Declaration of Helsinki and approved by the Medical Ethical Committee for Human Investigations of Peking University Health Science Centre, Beijing, China (number PKUSSIRB-2012067). Patients recruited in the investigation were informed of the characteristics of the study and provided signed informed consent.
This retrospective study was conducted from January 2004 to December 2011 and included 22 patients (13 males and 9 females) who were registered in the Department of Periodontics with a total of 26 crown-root fracture teeth. All patients were seeking dental care because of tooth fracture and were referred to the periodontist for crown lengthening surgery. Consultation and certainty of a favourable prognosis as well as agreement upon the treatment plan were achieved between practitioners and the patient's preference for the approach instead of other possible options was established. Each patient received initial periodontal therapy including oral hygiene instructions, scaling and root planing, and removal of marginal irritants. All fractured teeth had undergone endodontic treatment before the periodontal surgery procedure. After performing all treatment procedures, patients were scheduled for regular periodontal supportive treatment.
Patient age ranged from 24 to 58 years with a mean of 41.6 years of age. According to the location of traumatic incidence, fifteen (58%) of the fractured teeth were maxillary incisors, three (12%) were premolars, and eight (31%) were molars. In all cases, the fracture lines extended obliquely with an approximate 2 to 6 mm subgingival involvement. The contralateral tooth and ipsilateral teeth mesial and distal to the treated tooth were used as controls.
Surgical and restorative procedures
A modified crown lengthening procedure17 was implemented and a schematic drawing of the procedure is shown in Figure 1. All of the modified crown lengthening surgeries were performed by one periodontist (WH). Surgical procedures of a representative case are presented in Figure 2. The proposed amount of gingival tissue removal varied with depth of the subgingival fractures. Regarding the incision design, the preoperative width of keratinised tissue was used as a parameter to decide and estimate the postoperative keratinised tissue width.19 When the estimated postoperative keratinised tissue width via soft tissue excision was greater than 3 mm, indicating that the treated teeth with subgingival restorative margins possessed enough keratinised tissue to maintain periodontal health after modified crown lengthening surgery,20 the proposed amount of gingival tissue resection technique with internal bevel incision was selected. If the estimated postoperative keratinised tissue width was less than 3 mm while the preoperative keratinised tissue width was greater than 3 mm, minimal gingival tissue resection technique with internal bevel incision leaving no less than 3 mm of keratinised tissue was used. For teeth whose preoperative keratinised tissue width was equal or less than 3 mm, no gingival tissue resection technique with crevicular incision combined with apically positioned flap procedures was performed.21 Full thickness flaps on the buccal and lingual aspects were elevated to expose the alveolar crest. Thorough debridement of all granulation and epithelial tissue was accomplished to allow unobstructed visualisation of the underlying bony architecture and root fracture configuration (Fig. 2c). According to the principle of root reshaping and conservative removal of the supporting alveolar bone, round surgical burs were used to remove enough alveolar bone to expose the subcrestal root fracture and conduct the necessary osteoplasty (Fig. 2d). A coarse diamond bur was used to eliminate the fractured edge followed by a superfine diamond bur to refine and smooth the root surface of the fractured tooth (Fig. 2e). Finally, the edge or sharp margin of the fracture was eliminated, which allowed a new biologically favourable environment for the future restorative procedure to be established. The flap was repositioned using 4.0 non-resorbable silk sutures (Fig. 2f) and protected by periodontal dressing. Patients were instructed to refrain from tooth-brushing at the surgical sites for 14 days and use a 0.12% chlorhexidine gluconate oral rinse twice daily. At 7 days post-surgery the sutures were removed. Patients resumed normal oral hygiene protocol 14 days postoperatively. All treated teeth were restored with crown margins located either equigingivally or subgingivally 3 to 6 months after periodontal surgery.

a) The normal biological width is 2 mm; b) A scenario with the bottom of tooth fracture surface 1 mm below the alveolar crest; c) The crown and root ratio would be unfavourable if the conventional crown lengthening was applied; d) Minimum alveolar bone height will be reduced to expose the bottom of the tooth fracture surface and then the root surface is reshaped by the modified crown lengthening

a and b) A representative crown-root fracture case before surgery; c) The underlying bony architecture and root fracture anatomy after flap elevation, the tooth fracture line was 1.0 mm below the alveolar crest; d) Removal of 2 mm of alveolar bone with a medium and small round bur; e) Redefinition and finishing of the surface of the teeth with a superfine diamond bur; f) Suturing using non-resorbable silk suture
Questionnaire and clinical examination
Twenty-two patients were recalled periodically and the treated teeth were examined for subjective symptoms such as pain, bleeding on brushing, gingival swelling, mobility, exudate, discomfort during mastication, oral hygiene habits, status of the supportive periodontal therapy, medical history, and the Visual Analogue Scales (VAS) for aesthetic and functional assessment of treated teeth.22 The full score of the VAS was 10, a 10 cm straight line was used, the left side '0' represented 'extremely dissatisfied', and the other side '10' represented 'extremely satisfied'. Subjects made a mark on the line according to their own degree of satisfaction with the aesthetics and function of the teeth. The distance between the '0' and the mark represented the VAS score. If the score was 8 or higher it was interpreted as patients being very satisfied with their teeth.
Treated teeth and control teeth were examined for the following periodontal health parameters. All measurements were conducted by one examiner (MZ):
-
Plaque Index (PLI): Plaque accumulation was quantified at the buccal and lingual sides.23
-
Probing Depth (PD): PD was recorded for each tooth at 6 sites (mesiobuccal, buccal, distobuccal, distolingual, lingual, mesiolingual) using Williams probe. Only the maximum value on the reshaped and non-reshaped side was used for statistical analysis.
-
Bleeding Index (BI): Gingival inflammation at buccal and lingual sides on all treated teeth was quantified using the BI. The examiner placed a Williams periodontal probe gently into the gingival sulcus or periodontal pockets at buccal and lingual sides on all treated teeth, then took out the probe and waited for 30 seconds; each side was assessed and given a score of 0 to 5 according to the gingival inflammation and bleeding.24
-
Bleeding on Probing (BOP): Presence of BOP was recorded 30 seconds after the measurement of PD. Recordings were made on the buccal and lingual surfaces with '1' when BOP was present and “0” when BOP was absent.
-
Mobility: Mobility was divided into 3 degrees according to Newman et al.25
-
Location of the crown margin (LCM): LCM was recorded at 6 sites (mesiobuccal, buccal, distobuccal, distolingual, lingual, mesiolingual) using Williams probe with “0” if the crown margin was equal to the gingival margin. Subgingival crown margin was recorded as a negative value. Supragingival crown margin was recorded as a positive value. Only the maximum value on both the reshaped and non-reshaped side was recorded and used for statistical analysis.
-
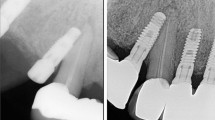
Radiographical findings: Parallel digital X-rays were taken at the final recall appointment in order to observe the density of the lamina dura, changes in the periodontal ligament, verify possible hidden root fractures, and any pathological changes in the periapical areas.
Statistical analyses
The defect tooth distribution and the location of the subgingival fracture before the surgery were subjects of frequency analyses. The VAS scores for the aesthetics and function of the treated teeth were calculated. Differences in the indices (PLI, PD, BOP, mobility) between the reshaped and non-reshaped sites of treated teeth, and the corresponding sides of controls were analysed statistically using Mann-Whitney-U tests with level of significance at α=0.05. The relationships of the recorded indices of the treated teeth were examined using partial correlation analysis.
Results
The average follow-up period was 42.7 months with a range from 24 to 84 months. All treated teeth were still in function except for one left maxillary central incisor where a repeated accidental root fracture was reported and the tooth was extracted after the 4-year recall. The mean and standard deviation of the VAS scores for aesthetics and function of the treated teeth are shown in Table 1. The mean values for the treated teeth were 9.5 for both aesthetic and functional aspects. All definitive crowns were intact without any abnormal findings and no marginal caries was detected during the last recall visit. Data analysis revealed a predominance of low PLI scores and high frequency of BOP for all treated teeth. The majority (96%) of sites displayed PD in the range of 1-3 mm. Only 3 out of 26 teeth had Grade I tooth mobility. Parallel radiographic assessment of the treated teeth revealed consistent density of the lamina dura, no pathological changes in the periapical regions, and no obvious reduction of the bone crest height.
No statistically significant differences in periodontal indices were observed between reshaped and non-reshaped sides of the treated teeth (P >0.05). Statistically significant differences in BOP were determined between the treated teeth and controls at the corresponding sides (P <0.05). However, no statistically significant differences were observed between treated teeth and controls for any of the other periodontal indices (Table 2). With respect to crown margin location, 88 (56%) sites were equal to or above the free gingival margin and 68 (44%) sites were located at 1.5-3.0 mm subgingivally. For the subgingival extension of the crown margin, the mean and standard deviation at the middle site of the reshaped side was 1.2 ± 0.8 mm with range 0 mm to 3.0 mm. Partial correlation analysis showed that the crown margin location and the bleeding index were negatively correlated (r = −0.417, P < 0.05), which indicated that the deeper the subgingival location of the crown margin, the higher the bleeding index. Plaque index and probing depth were not significantly correlated with the bleeding index (Table 3).
Discussion
Results of this retrospective study indicate that the treatment outcomes of the crown-root fractured teeth receiving modified crown lengthening surgery followed by endodontic treatment and post and core restoration are favourable. All the crown-root fracture teeth recruited were permanent teeth. Patient age ranged from 24 to 58 years and all decided to retain the affected tooth and restore the defect. Endodontic therapy is usually necessary not only to eliminate the unsupported tooth structure and local infection but also to provide a solid base for future procedures.26 Because of the reshaping of the root surface and conservative removal of the supporting alveolar bone, a biologically acceptable configuration of remaining root structure is established. Therefore, a better crown-to-root ratio and favourable aesthetic outcomes for successful restorative procedures were achieved.
Owing to the application of a reshaping procedure to eliminate the fracture line from the root surface, the integrity and strength of the remaining root structure may be compromised, especially after crown preparation procedure. Sorrentino et al.27 used three-dimensional finite element analysis to evaluate the location of the maximum stress in defective root structure models, and found that the location and the amount of stress will change accordingly and move apically. In the present study, one tooth was extracted due to a repeated accidental root fracture 4 years after surgical and restorative procedures. The horizontal root fracture in this case was located 0.5 mm apically to a cast post. This fracture incidence may have been related to stress concentration and pre-existing incomplete fracture before the surgery.
All patients were satisfied with the aesthetics of the treated teeth except for one patient who gave a low score (5.4). This patient complained of colour mismatch of the metal-ceramic crown with the adjacent teeth after the 68-month recall, rather than of gingival margin disharmony related to the modified crown lengthening procedure. In two patients, the VAS scores of the function of the treated teeth were 6.6 and 6.9 respectively. These particular teeth had the worst pre-operative condition in the study, with fracture line located 6 mm below the gingival crest before surgery. The latter tooth was a maxillary right central incisor, which the patient used carefully as the biomechanical condition of the treated tooth was worse than that of natural teeth.
It is a well-known fact that the location of the crown margin and periodontal health are closely related. Flores-de-Jacoby et al.28 studied the effect of crown margin location on periodontal health for a 1 year period and found that crowns with subgingival margins had a negative impact on periodontal parameters. A negative correlation (r = −0.417) between subgingival margin location and bleeding index was determined in this study. Therefore, there should be no reason for more than 0.5 to 1 mm subgingival extension for the consideration of aesthetics or retention. The reshaping of root surface during modified crown lengthening facilitated relocation of the future restorative margin in the occlusal direction. This could aid in placement of the restorative margin equigingivally or supragingivally after the modified crown lengthening procedure.
Given that the present study is a retrospective clinical study with a relatively small sample size rather than a randomised controlled prospective study, restricted patient selection criteria and limiting recruitment of cases might have resulted in some degree of bias in terms of patient selection. However, findings of this study do provide positive support for management of crown-root fractured teeth. The results of periodontal observation of treated teeth with monitoring for over 2 years indicate that the modified crown lengthening is a clinically feasible and minimally invasive treatment option for crown-root fractured teeth. In addition, the results of the present study provide evidence-based support to empower the profession to save and restore compromised teeth with appropriate surgical and restorative procedures.
Conclusions
Within the limitations of this study, the following conclusions may be drawn:
Crown-root fractured teeth managed with a modified crown lengthening procedure after an average of 42.7 months recall revealed no significant changes of periodontal indices compared to natural control teeth.
The modified crown lengthening procedure is a clinically feasible and minimally invasive surgical treatment option for management of crown-root fractured teeth.
References
Caldas A F, Jr, Burgos ME . A retrospective study of traumatic dental injuries in a Brazilian dental trauma clinic. Dent Traumatol 2001; 17: 250–253.
Eichelsbacher F, Denner W, Klaiber B, Schlagenhauf U . Periodontal status of teeth with crown-root fractures: results two years after adhesive fragment reattachment. J Clin Periodontol 2009; 36: 905–911.
Chung M P, Wang S S, Chen C P, Shieh Y S . Management of crown-root fracture tooth by intra-alveolar transplantation with 180-degree rotation and suture fixation. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010; 109: 126–130.
Goenka P, Marwah N, Dutta S . A multidisciplinary approach to the management of a subgingivally fractured tooth: a clinical report. J Prosthodont 2011; 20: 218–223.
Francisco Palomo D, Raymond A, Kopczyk D . Rationale and methods for crown lengthening. JADA 1978; 96: 257–260.
Bragger U, Lauchenauer D, Lang N P . Surgical lengthening of the clinical crown. J Clin Periodontol 1992; 19: 58–63.
de Waal H, Castellucci G . The importance of restorative margin placement to the biologic width and periodontal health. Part II. Int J Periodont Rest Dent 1994; 14: 70–83.
Padbury A, Jr, Eber R, Wang H L . Interactions between the gingiva and the margin of restorations. J Clin Periodontol 2003; 30: 379–385.
Wagenberg B D, Eskow R N, Langer B . Exposing adequate tooth structure for restorative dentistry. Int J Periodont Rest Dent 1989; 9: 322–331.
Pontoriero R, Carnevale G . Surgical crown lengthening: a 12-month clinical wound healing study. J Periodontol 2001; 72: 841–848.
Bensimon GC . Surgical crown-lengthening procedure to enhance esthetics. Int J Periodont Rest Dent 1999; 19: 332–341.
Parashis A, Tripodakis A . Crown lengthening and restorative treatment in mutilated molars. Quintessence Int 1994; 25: 167–172.
Huynh-Ba G, Bragger U, Lang N P . Surgical lengthening of the clinical crown: a periodontal concept for reconstructive dentistry. Perio Pract Today 2007; 4: 193–201.
Landi L, Manicone P, Piccinelli S, Raia R, Marinotti F, Scutella F . Determining osseous resection during surgical crown lengthening in the esthetic zone with the use of a radiographic and surgical template. Quintessence Dent Tech 2004; 101–113.
Fakhry A . Enhancing restorative, periodontal, and esthetic outcomes through orthodontic extrusion. Eur J Esthet Dent 2007; 2: 312–320.
Melker D, Richrdson C R . Root reshaping: an integral component of periodontal surgery. Int J Periodont Rest Dent 2001; 21: 297–304.
Hu W J, Li L S, Zhang H, Peng D . Root reshaping in combination of conservative osseous resection: a modified technique for surgical crown lengthening. J Peking University (Health Sci) 2008; 40: 83–87.
da Cruz M K, Martos J, Silveira L F, Duarte P M, Neto J B . Odontoplasty associated with clinical crown lengthening in management of extensive crown destruction. J Conserv Dent 2012; 15: 56–60.
Haempton T J, Dominici J T . Contemporary crown-lengthening therapy: a review. J Am Dent Assoc 2010; 141: 647–55.
Scheyer E T, Sanz M, Dibart S . Periodontal soft tissue non-root coverage procedures: a consensus report from the AAP Regeneration Workshop. J Periodontol 2015; 86: S73–S76.
Pippin DJ . Fate of pocket epithelium in an apically positioned flap. J Clin Periodontol 1990; 17: 385–391.
Han J, Xiong G Z, Gang W D . The clinical research of levobupivacaine in the extraction of impacted mandibular wisdom teeth. J Clin Stomatol 2011; 27: 621–623.
Silness J, Loe H . Periodontal disease in pregnancy. II. Correlation between oral hygiene and periodontal condition. Acta Odontol Scand 1964; 22: 121–135.
Mazza J E, Newman M G, Sims T N . Clinical and antimicrobial effect of stannous fluoride on periodontitis. J Clin Periodontol 1981; 8: 203–212.
Newman M G, Takei H H, Klokkenold P R, Carranza F A . Carranza's Clinical Periodontology. 10th Edition. St Louis: Saunders Elsevier, 2006.
Moule A J, Moule C A . The endodontic management of traumatized permanent anterior teeth: a review. Aust Dent J 2007; 52: S122–S137.
Sorrentino R, Aversa R, Ferro V et al. Three-dimensional finite element analysis of strain and stress distributions in endodontically treated maxillary central incisors restored with different post, core and crown materials. Dent Mater 2007; 23: 983–993.
FloresdeJacoby L, Zafiropoulos G G, Ciancio S . Effect of crown margin location on plaque and periodontal health. Int J Periodont Rest Dent 1989; 9: 197–205.
Acknowledgements
Study supported in part by the Capital foundation for Clinical Characteristics and Application Research, Grant #Z131107002213174. The authors would like to thank Dr. Hollie Walsh for her assistance in the preparation of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Zhen, M., Wang, C., Hu, WJ. et al. Periodontal evaluation of crown-root fractured teeth following modified crown lengthening surgery. Br Dent J 222, 21–25 (2017). https://doi.org/10.1038/sj.bdj.2017.25
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.2017.25
This article is cited by
-
Success rate of fractured teeth receiving modified crown lengthening surgery and restorations
BMC Oral Health (2022)
-
The management of a complicated crown-root fracture incorporating modified crown-lengthening surgery
British Dental Journal (2021)
