
Key Points
-
Discusses advances in instrumentation, disinfection and root filling.
-
Provides tips for reducing the risk of instrument fracture, ensuring reliable apex locator readings, and removing intracanal obstructions.
-
Emphasises the importance of cuspal protection for endodontically treated posterior teeth.
-
Outlines contemporary (micro)surgical endodontic techniques and materials.
Abstract
The aim of this paper is to present the contemporary developments in root canal treatment, restoration of the endodontically treated tooth, and advanced endodontic procedures, such as root canal retreatment and surgical endodontics.
Similar content being viewed by others


Instrumentation
The aim of instrumentation is to create adequate space for disinfectants to penetrate the root canal system, remove inflamed and infected debris, and create a suitable shape for the subsequent root filling. Instrumentation can be carried out using a variety of file systems which may be manufactured from stainless steel (SS) or nickel-titanium (NiTi). Straightening of curved root canals can be a major problem with SS files, especially larger sized files (>ISO size 20). To help overcome this NiTi files may be used. Instrumentation using NiTi files was first described over 20 years ago1 and their popularity has steadily increased with most dental schools in the United Kingdom teaching their use.
The principle advantage of NiTi in endodontics is its super-elasticity. Compared to SS files of the same diameters, NiTi files are very flexible. This increased flexibility, even with increasing diameters, allows curved root canals to be easily instrumented without major transportation or other iatrogenic errors. NiTi files are also very efficient at removing dentine and their built-in taper allows the root canal to be machined to a predetermined shape (Fig. 1). The clinical benefits include shorter preparation time, fewer files are required to prepare the root canal, and there is less operator and patient fatigue.

(b) A root canal system which has been efficiently prepared with NiTi files, note that the curvatures have been maintained
The dental market is replete with many brands of NiTi files; the differences between brands include the cross-sectional shape, taper, tip sizes, and presence or absence of radial lands. The majority of NiTi files are manufactured by a grinding process; however, newer manufacturing processes allow blanks to be twisted into shape (eg Twisted Files, SybronEndo, Orange, CA, USA). It has been reported that these twisted NiTi files are more resistant to fatigue and fracture.2,3 Other new NiTi file systems use a reciprocation technique (eg WaveOne, DENTSPLY Maillefer, Ballaigues, Switzerland; & Reciproc, VDW, Bayerwaldstr, Germany). Files are rotated in a clockwise-anticlockwise movement using a specialised motor. The main benefit of these systems is root canal preparation using one single file in the majority of cases.
Regardless of which file system or material (NiTi or SS) is chosen, it is advisable to use a crown-down technique to:
-
Prevent pushing apically or extruding infected necrotic pulp and dentine
-
Eliminate coronal interferences, thus reducing the risk of iatrogenic errors
-
Introduce irrigants to the apical portions of the root canal at an early stage
-
Maintain working length during subsequent instrumentation
-
Improve tactile feedback during hand instrumentation of the apical portion of the root canal.
Despite manufacturers heavily advertising NiTi files, it must be stressed that NiTi files are not a panacea. Small sized hand files (≤ISO size 20) are still necessary to explore root canals and create a glide path for NiTi files. Major disadvantages of NiTi files include cost, unexpected fracture, and they cannot be used for all cases. The inappropriate use of any endodontic instrument, including NiTi files, may result in iatrogenic errors including fracture. There are several ways to reduce the risk of instrument fracture (Table 1, Fig. 2).

These motors allow the torque setting and RPM to be preset depending on the file system used. (b) Files should always be checked before and after removal from the root canal for signs of deformation
In 2007, the Chief Dental Officer in England issued guidance stating that endodontic reamers and files should be treated as single-use.4 Although this guidance was primarily concerned with reducing the risk of prion transmission, there was also a practical benefit with reduced risk of instrument fracture due to cyclical fatigue. In 2010, an update of this guidance was issued stating that endodontic files and reamers may be re-used on the same patient as long as the instruments were marketed as being re-useable and certain requirements were met with regards to cleaning and storage of these instruments.5
Traditionally, the working length of a root canal can be determined in several ways, eg tactile sensation, working length radiograph, or blood at the tip of paper points. The process of determining the working length by placing premeasured files into root canals and taking a parallel radiograph can sometimes be arduous, time consuming and inaccurate. Contemporary endodontics makes use of the electronic apex locator (EAL) which has superior accuracy in determining the working length when compared to traditional techniques.6 Depending on the generation and manufacturer, EALs work by detecting the distance from either the apical foramen or apical constriction in a circuit that measures either electrical resistance or impedance. It is not necessary to routinely take working length radiographs when EAL readings are consistently reliable (Table 2). This has the obvious benefit of reducing radiation exposure to patients.
Disinfection
The root canal system cannot be disinfected to a sufficient level by solely using endodontic files (NiTi or SS).7 The uniform nature of endodontic files prevents complete mechanical preparation of all surfaces or anatomical complexities of the root canal system. It has been shown that 35% or more of the root canal surface area is left unchanged after instrumentation.8 Instrumentation should therefore be supplemented with disinfection (Fig. 3). There are many newer irrigants on the market, including electrochemically activated water and ozonated water; however, there is a paucity of evidence to suggest they are superior to sodium hypochlorite which remains the gold standard. Sodium hypochlorite is antimicrobial and antibiofilm, and it dissolves organic tissue, ie necrotic pulp and microbes. In contemporary endodontics the effects of irrigants may be optimised by alternating and agitating the irrigant.

(b) A side-venting endodontic irrigant needle will help reduce the likelihood of a hypochlorite accident. (c) The EndoActivator cordless handpiece, energising the irrigant with a sonic or ultrasonic device will enhance the disinfection of the root canal system, a smooth polymer tip is placed in each canal and activated for 2-3 minutes
Alternating irrigants
A 'dual' or 'triple' irrigant approach combines the favourable properties of several irrigants. Our understanding of the individual properties of each irrigant is good; however, we are only starting to understand the interactions of these irrigants. Protocols vary on when to alternate irrigants and which should be used as the final rinse. A favoured method is alternating sodium hypochlorite, which removes organic material, with a chelating agent (eg ethylenediaminetetraacetic acid) or an organic acid (eg citric acid), which removes inorganic material. This facilitates removal of microbes, necrotic pulp and the smear layer, which is created during instrumentation of dentine. Removal of the smear layer is advocated as it may contain and protect microbes as well as prevent proper adaptation of root filling materials to the root canal wall.9
Chlorhexidine and iodine compounds (eg povidone-iodine and iodine-potassium-iodide) have also been advocated as additional irrigants for root canal (re)treatment due to their broad anti-microbial spectrum. It has been recently shown that alternating sodium hypochlorite with povidone-iodine had no accumulative influence on outcome of treatment, and alternating sodium hypochlorite with chlorhexidine solution significantly reduced the outcome of treatment.10 In addition concerns have been raised about allergic reactions to iodine compounds and the toxic and carcinogenic precipitate parachloroaniline, which forms after mixing sodium hypochlorite and chlorhexidine.11
Agitating irrigants
Most irrigants have poor surface tension and cannot completely flow within the anatomical complexities of the root canal system. In addition, air can become trapped in the apical portion of the root canal preventing apical irrigation (vapour lock concept). There are many agitation techniques and devices available to help circulate and replenish irrigants. These can be divided into manual and machine-assisted (Table 3).12 The most commonly used manual technique is syringe-needle positive pressure agitation. The risk of causing a 'hypochlorite accident' is reduced by using a premeasured side-venting needle and applying gentle pressure. Contemporary endodontics utilises passive ultrasonic irrigation (PUI) where ultrasonic energy is applied to a small file that floats passively within the root canal.13 The resulting acoustic microstreaming produces turbulence around the file which agitates the irrigant and improves its delivery (Fig. 3).
Root filling
Root filling aims to prevent reinfection of the disinfected root canal system, entomb any remaining microbes, and prevent entry of periapical tissue fluid into the root canal system, which may act as a nutritional supply for any remaining microbes. Gutta-percha (GP) used in conjunction with a root canal sealer are still the most widely used root filling materials. There are alternative polymer-based root filling materials which manufacturers claim can form a 'mono-block' root filling. However, there is no definitive evidence that one particular contemporary root filling material is significantly better in achieving healing of apical periodontitis. Broadly speaking root canals can be filled using either single cones, cold lateral compaction, or warm vertical compaction. It is more accurate to describe the technique as 'compaction' rather than 'condensation' as the density of the root filling material is not being altered.
Single cone technique
Historically, the single cone technique involved placement of silver points; however, these were shown to corrode due to poor apical seal.14 The single cone technique has regained popularity with the introduction of GP or polymer-based points which match the taper and tip size of the rotary NiTi master apical file. The single cone technique is simple and quick; however, this technique relies heavily on sealer to fill areas of the root canal system. Sealer is the weakest link in a root filling and so the ratio of sealer-to-root-filling should be kept low.
Cold lateral compaction
Cold lateral compaction is still the most widely used and taught technique. It is relatively cheap and well-adapted root fillings can be achieved; however, it can be time consuming and tiring. If carried out incorrectly, it can result in voids in the root filling and even vertical root fractures.
Warm vertical compaction
Contemporary heated techniques allow thermoplasticised root filling material to flow and be compacted within root canal irregularities, eg isthmuses and lateral canals. This ensures an optimal seal along the entire length of the root canal (Fig. 4). Warm vertical compaction is relatively quick; however, the equipment can be expensive and studies have shown that the incidence of over-extension is greater than when using cold lateral compaction.15

Warm vertical compaction in (a) a mandibular second molar with C-shaped root canal anatomy, and (b) in a maxillary central incisor with an internal resorption lesion
Root fillings should always be used in conjunction with a root canal sealer. The root canal sealer should seal any residual voids around the root filling material. Commonly used sealers may be broadly categorised as zinc oxide-eugenol based, epoxy resin based and calcium hydroxide based. More recently adhesive, silicone and calcium phosphate root canal sealers have been introduced onto the dental market. At present there is no good evidence to suggest that any particular type of sealer results in better outcome of endodontic treatment.
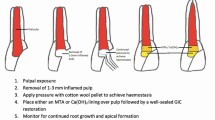
Immature teeth
Teeth with wide root canals, in particular immature teeth, are difficult to root fill as there is no taper or apical constriction (resistance form). Traditionally, these root canals were filled with several GP points which were heated together and inserted to form an impression of the root canal. Contemporary endodontics uses calcium silicate cements, eg mineral trioxide aggregate (MTA), to induce a barrier in the apical portion of wide canals using special delivery devices, ultrasonics, and endodontic pluggers. MTA is biocompatible, provides an excellent seal, and induces hard tissue healing (Fig. 5). The remaining mid-portion of the root canal is filled with heated GP. Composite is then placed into the cervical and coronal portion of the root canal to provide coronal seal. This also reduces the risk of root fracture of thin-walled immature teeth.16

An immature incisor tooth has been sealed with MTA, no instrumentation was required as the canal was wide enough to allow adequate disinfection, and there was adequate resistance form apically for retention of the root filling material
Root canal retreatment
Root canal retreatment is indicated in teeth with unsatisfactory root fillings when:
-
There are signs and/or symptoms of emerging, recurrent or persisting apical periodontitis
-
When the coronal restoration requires replacement
-
When internal bleaching is to be performed.17
It is important to find out the cause of post-treatment disease associated with an endodontically treated tooth. The clinician must identify any non-endodontic reason, eg root fracture, as root canal retreatment will be inappropriate and in these situations the tooth should be extracted. Endodontic causes of failure essentially revolve around existing infection or re-infection. In cases where there is post-treatment disease associated with a well-executed endodontic treatment, it is unlikely that root canal retreatment will improve the outcome; in these cases other treatment options should be considered including surgical endodontics or extraction. Post-treatment disease associated with a poorly endodontically-treated tooth may be as a result of not using rubber dam, poor access resulting in missed untreated root canals, inadequate instrumentation (eg working length not reached, poor taper), inadequate disinfection (eg insufficient volume and turnover, use of irrigant which has no antimicrobial action), inadequate root filling (eg root filling does not extend to within 2 mm of the radiographic apex, contains voids), and/or iatrogenic errors (eg fractured instrument, perforation, ledge) (Fig. 6). Other rarer causes of post-treatment disease include extraradicular infections eg periapical actinomycosis, cystic apical periodontitis, a foreign body reaction, or scar tissue healing;18 however, evidence in relation with these causes of post-treatment disease are contradictory.

(a) Poorly compacted root filling, note the voids. (b) An underextended root filling, note the unfilled apical portion of the root canals. (c) A separated instrument has prevented disinfection of the apical portion of the root canal system
Root canal retreatment is generally considered more difficult to carry out than root canal treatment as there are usually intracanal obstacles to overcome. These include:
-
Removal of root filling materials. Gross removal of gutta-percha or polymer based root filling materials can be achieved using Gates Gliddens drills and rotary nickel-titanium retreatment files. Solvents, such as chloroform, are effective at dissolving gutta-percha and certain root canal sealers. Their use should not be standard practice as they smear root filling material along the root canal walls and inside dentinal tubules19 and there are concerns over chloroform being possibly carcinogenic to humans20
-
Removal of other intracanal materials such as silver points, posts (cast, prefabricated, metal, fibre) or fractured instruments (files, spiral fillers, Gates Gliddens drills). There are a variety of techniques and equipment available to remove these obstructions. Contemporary endodontics mainly utilises specialised ultrasonic tips (Fig. 7) to retrieve these materials directly or after gently removing dentine around the material. Post removal trephines and extractors should be avoided if possible as they can weaken the remaining tooth structure
Figure 7 
Ultrasonic tips for use in root canal (re)treatment
-
Correction of iatrogenic errors such as ledges or perforations.

The success of root canal retreatment is dependent on the following (Fig. 8):
-
Locating all root canals
-
Negotiation, and subsequent instrumentation of the root canal(s) to the ideal working length
-
Adequate disinfection of the entire root canal system
-
Sealing (including the coronal seal) of the root canal system.

(b) An axial reconstructed image from a CBCT scan of the area revealed the presence of an uninstrumented fourth root canal. (c) Root canal retreatment was carried out, at the one year follow-up there was complete healing as the entire root canal system was adequately disinfected and sealed
Single-visit endodontic treatment
It is not possible to achieve a consistently microbe-free root canal system whether using traditional or contemporary endodontics. The aim of endodontic (re)treatment is to control infection by reducing the number of microbes below a threshold at which healing of the apical tissues is possible. Proponents of multi-visit endodontic treatment advocate the use of an interappointment medicament to fully eradicate infection within the root canal system. Calcium hydroxide is the gold standard interappointment medicament due to its antimicrobial and tissue dissolving capacity. However, it is difficult to place properly and fully remove,21,22 and concerns have been raised about long-term dressing with calcium hydroxide which may increase the risk of root fracture.23 In vitro evaluation of calcium hydroxide has shown it can alter the dentine matrix reducing the flexural strength of dentine.24 A recent study concluded that bacteria commonly involved in nosocomial infections are often retrieved in root canals with post-treatment endodontic disease; single-visit endodontics reduces the chances of this infection to occur.25
The current evidence appears to show that there is no significant difference in the outcome of treatment between single-visit and multiple-visit endodontic treatment,26,27,28,29 or incidence of post operative pain.30,31,32,33 The benefits of single-visit treatment are abundant (Table 4).
Restoration of the endodontically treated tooth
Restoration of the endodontically treated tooth is necessary to restore function, aesthetics, and also provide coronal seal and cuspal protection. Endodontically treated teeth are at an increased risk of fracture compared to vital teeth due to:
-
Loss of pulpal sensory feedback34
-
Loss of coronal tooth structure as a result of caries, previous restorations and access cavity preparation
-
Excessive irrigation35 and/or long-term interappointment dressing23
-
Loss of radicular tooth structure due to over-instrumentation or post preparation, especially cast metal post preparation.36
Placement of direct restorations, eg plastic restorations and when necessary fibre or metal posts, should be carried out be immediately after root canal treatment is completed. This is the ideal time as the clinician has immediate knowledge of the pulp chamber anatomy, the access cavity is readily accessible, the tooth is thoroughly disinfected, and the tooth is still under rubber dam isolation. If indirect restorations, eg crowns, are planned, these should be placed with the minimum of delay (Fig. 9). This can be within one to two weeks if the quality of the root canal filling is considered adequate. If there is early evidence of post-treatment disease or root canal treatment was compromised by iatrogenic errors, then the tooth should be restored with a provisional restoration, eg laboratory fabricated provisional crown, and any complex restorations should be delayed until there is evidence of healing.

(a) An endodontically treated tooth restored with a temporary IRM restoration, (b) placement of a well-adapted composite dowel core, (c) a metal-ceramic crown cemented into place will reduce the likelihood of the tooth fracturing in the future
Traditionally, endodontically treated molar teeth were restored with amalgam Nayyar cores and, when indicated, cast or prefabricated metal posts. Contemporary endodontics utilises adhesive materials and techniques, including composite-dowel cores and fibre posts, to restore endodontically treated teeth. The main benefits of adhesive restorations include:37
-
Immediate post-endodontic placement which gives the clinician direct control over the design of the restoration, and provides immediate coronal seal and cuspal protection
-
The ability to preserve and bond to tooth structure which would have otherwise been removed for placement of traditional non-adhesive materials
-
Similar modulus of elasticity to dentine when compared to metal restorations
-
Improved aesthetics
-
Reduced laboratory costs.
Traditionally, it was recommended that both endodontically treated premolars and molar teeth should be restored with cuspal coverage restorations (eg crowns) to improve their survival.38 Recent research suggests that, in the short-term (3-5 years), it is sufficient to restore endodontically treated premolar teeth with fibre posts and composite cores without the additional need for a crown.39,40,41 It is still recommended that endodontically treated molar teeth are restored with restorations that provide full coronal coverage.42
Surgical endodontics
Surgical endodontics, including incision and drainage, apical surgery, and replantation, is performed in cases with apical periodontitis when non-surgical approaches are technically difficult or impractical.17 Indications for surgical endodontics are given in Table 5.43
Surgical endodontics has been transformed by magnification, micro-instruments, ultrasonics, newer root-end filling materials and modern techniques to manage soft and hard tissues.44 It has been suggested that pre-operative surgical endodontic protocols should include smoking cessation advice45 and chlorhexidine rinsing46 to prevent surgical complications.
Traditionally, soft tissue management included broad based flaps with converging vertical incisions, supposedly to ensure optimal blood flow to the flap. This is no longer advocated as converging incisions sever supra-periosteal blood vessels. Contemporary flaps should have parallel vertical relieving incisions to minimise severing of these blood vessels and optimise soft tissue healing. Vertical incisions, not horizontal incisions, should also be applied when carrying out incision and drainage of a dental abscess. Patients now expect good aesthetics after surgery with gingival recession and loss of interdental papilla being unacceptable. The more skilled clinician may choose to perform a papilla-base incision to reduce the risk of interdental papilla loss.47
Traditionally, root-end resections were bevelled to aid direct vision for root-end cavity preparation with a bur. Bevelled resections are no longer encouraged as they expose a large number of dentinal tubules which may harbour microbes. Root-end preparation using a bur is also not advisable as there is a risk of transporting the root canal or causing a perforation. Contemporary root-end resection should be perpendicular to the long axis of the root. The root end can then be visualised using micro-mirrors under magnification and prepared using ultrasonic retro-tips (Fig. 10).

(b) A conventional scalpel blade (left) and a surgical micro-blade (right). (c) Ultrasonic tip for preparing root-end cavities
Amalgam is no longer favoured as the root-end filling material of choice.48 Contemporary root-end filling materials include Intermediate Restorative Material (IRM) and calcium silicate cements. The latter has an excellent sealing ability and induces hard tissue barrier formation; however, it is relatively expensive compared to IRM and not as straightforward to place (Fig. 11).

(c) A root-end cavity has been prepared with an ultrasonic tip and sealed with IRM. (d) One year follow-up reveals healing
Outcome of endodontic treatment
Traditionally, the outcome of root canal treatment was described as either a 'success' or a 'failure'. These terms can be ambiguous as they may be defined differently by the patient or the clinician. For example, a patient may feel that endodontic treatment has been a success as they are symptom-free; however, there may be a buccal sinus or an increased periapical radiolucency. Contemporary endodontics uses the clear terms 'healed', 'healing' or 'diseased' to describe the outcome of treatment. Outcome should be assessed clinically and radiographically for at least one year after root canal treatment.17 A healed outcome is defined as no signs or symptoms with no periapical radiolucency, and a diseased outcome is defined as presence of a new or increased periapical radiolucency with or without signs and symptoms.49 In healing cases where the periapical radiolucency is reduced or not increasing in size, then the patient should be reviewed annually for up to four years.
If a diseased outcome is apparent, then the options available are:
-
Keep the tooth under review
-
Root canal retreatment
-
Surgical endodontics
-
Extraction.
The chance of a healed outcome after non-surgical endodontic treatment, ie the chance of curing or preventing apical periodontitis, has been reported to be in the region of 75-95%. If loose criteria are used, ie survival of an endodontically treated tooth, then higher rates of 93-97% have been reported.42,50 Several factors have been shown to significantly improve the outcome of root canal treatment and retreatment: pre-operative absence of periapical radiolucency, a satisfactory root filling (no voids and extension to 2 mm within the radiographic apex), and a satisfactory coronal restoration.51,52 It has also been reported that the outcome of root canal retreatment is significantly better when the primary root canal treatment has not altered the morphology of the root canal system, eg transportation, strip perforations.53 The chance of a healed outcome after contemporary surgical endodontics can be as high as 95%. There is good clinical rationale and some evidence to suggest that the outcome of surgical endodontics can be improved by using contemporary microsurgical techniques, equipment and materials.
Conclusion
Contemporary endodontics still aims to eliminate microbes and prevent re-infection of the root canal system. Contemporary endodontic materials, instruments and equipment are available to the clinician still using traditional techniques. It is hoped that clinicians will develop their approach to endodontics by implementing contemporary techniques and, in doing so, the consistency, efficiency and predictability of endodontic treatment can be improved.
References
Walia H M, Brantley W A, Gerstein H . An initial investigation of the bending and torsional properties of Nitinol root canal files. J Endod 1988; 14: 346–351.
Gambarini G, Grande N M, Plotino G et al. Fatigue resistance of engine-driven rotary nickel-titanium instruments produced by new manufacturing methods. J Endod 2008; 34: 1003–1005.
Larsen C M, Watanabe I, Glickman G N, He J . Cyclic fatigue analysis of a new generation of nickel titanium rotary instruments. J Endod 2009; 35: 401–403.
Department of Health. Advice for dentists on re-use of endodontic instruments and variant CreutzfeldtJakob disease (vCJD). London UK: Department of Health, 2007. Gateway Reference Number 8100.
Department of Health. CDO update – March 2010. London UK: Department of Health, 2010. Gateway Reference Number 13748.
Gordon M P, Chandler N P . Electronic apex locators. Int Endod J 2004; 37: 425–437.
Dalton B C, Orstavik D, Phillips C, Pettiette M, Trope M . Bacterial reduction with nickel-titanium rotary instrumentation. J Endod 1998; 24: 763–767.
Peters O A, Schönenberger K, Laib A . Effects of four Ni-Ti preparation techniques on root canal geometry assessed by micro computed tomography. Int Endod J 2001; 34: 221–230.
Violich D R, Chandler N P . The smear layer in endodontics - a review. Int Endod J 2010; 43: 2–15.
Ng Y L, Mann V, Gulabivala K . A prospective study of the factors affecting outcomes of nonsurgical root canal treatment: part 1: periapical health. Int Endod J 2011; 44: 583–609.
Basrani B R, Manek S, Sodhi R N, Fillery E, Manzur A . Interaction between sodium hypochlorite and chlorhexidine gluconate. J Endod 2007; 33: 966–969.
Gu L S, Kim J R, Ling J, Choi K K, Pashley D H, Tay F R . Review of contemporary irrigant agitation techniques and devices. J Endod 2009; 35: 791–804.
van der Sluis L W, Versluis M, Wu M K, Wesselink P R . Passive ultrasonic irrigation of the root canal: a review of the literature. Int Endod J 2007; 40: 415–426.
Brady J M, del Rio C E . Corrosion of endodontic silver cones in humans: a scanning electron microscope and X-ray microprobe study. J Endod 1975; 1: 205–210.
Peng L, Ye L, Tan H, Zhou X . Outcome of root canal obturation by warm gutta-percha versus cold lateral condensation: a meta-analysis. J Endod 2007; 33: 106–109.
Lawley G R, Schindler W G, Walker W A 3rd, Kolodrubetz D . Evaluation of ultrasonically placed MTA and fracture resistance with intracanal composite resin in a model of apexification. J Endod 2004; 30: 167–172.
European Society of Endodontology. Quality guidelines for endodontic treatment: consensus report of the European Society of Endodontology. Int Endod J 2006; 39: 921–930.
Nair P N . On the causes of persistent apical periodontitis: a review. Int Endod J 2006; 39: 249–281.
Horvath S D, Altenburger M J, Naumann M, Wolkewitz M, Schirrmeister J F . Cleanliness of dentinal tubules following gutta-percha removal with and without solvents: a scanning electron microscopic study. Int Endod J 2009; 42: 1032–1038.
International Agency for Research on Cancer. IARC monographs on the evaluation of carcinogenic risks to humans. Volume 73: some chemicals that cause tumours of the kidney or urinary bladder in rodents, and some other substances. Lyons: IARC, 1999.
Ricucci D, Langeland K . Incomplete calcium hydroxide removal from the root canal: a case report. Int Endod J 1997; 30: 418–421.
Kim S K, Kim Y O . Influence of calcium hydroxide intracanal medication on apical seal. Int Endod J 2002; 35: 623–628.
Andreasen J O, Farik B, Munksgaard E C . Long-term calcium hydroxide as a root canal dressing may increase risk of root fracture. Dent Traumatol 2002; 18: 134–137.
Grigoratos D, Knowles J, Ng Y L, Gulabivala K . Effect of exposing dentine to sodium hypochlorite and calcium hydroxide on its flexural strength and elastic modulus. Int Endod J 2001; 34: 113–119.
Niazi S A, Clarke D, Do T, Gilbert S C, Mannocci F, Beighton D . Propioniobacterium acnes and Staphylococcus epidermidis isolated from refractory endodontic lesions are opportunistic pathogens. J Clin Microbiol 2010; 48: 3859–3869.
Sathorn C, Parashos P, Messer H H . Effectiveness of single-versus multiple-visit endodontic treatment of teeth with apical periodontitis: a systematic review and meta-analysis. Int Endod J 2005; 38: 347–355.
Gesi A, Hakeberg M, Warfvinge J, Bergenholtz G . Incidence of periapical lesions and clinical symptoms after pulpectomy-a clinical and radiographic evaluation of 1-versus 2-session treatment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006; 101: 379–388.
Molander A, Warfvinge J, Reit C, Kvist T . Clinical and radiographic evaluation of one-and two-visit endodontic treatment of asymptomatic necrotic teeth with apical periodontitis: a randomized clinical trial. J Endod 2007; 33: 1145–1148.
Figini L, Lodi G, Gorni F, Gagliani M . Single versus multiple visits for endodontic treatment of permanent teeth. Cochrane Database Syst Rev 2007; CD005296.
Sathorn C, Parashos P, Messer H . The prevalence of postoperative pain and flare-up in single-and multiple-visit endodontic treatment: a systematic review. Int Endod J 2008; 41: 91–99.
Ince B, Ercan E, Dalli M, Dulgergil C T, Zorba Y O, Colak H . Incidence of postoperative pain after single-and multi-visit endodontic treatment in teeth with vital and non-vital pulp. Eur J Dent 2009; 3: 273–279.
Iqbal M, Kurtz E, Kohli M . Incidence and factors related to flare-ups in a graduate endodontic programme. Int Endod J 2009; 42: 99–104.
Wang C, Xu P, Ren L, Dong G, Ye L . Comparison of post-obturation pain experience following one-visit and two-visit root canal treatment on teeth with vital pulps: a randomized controlled trial. Int Endod J 2010; 43: 692–697.
Randow K, Glantz P O . On cantilever loading of vital and non-vital teeth. An experimental clinical study. Acta Odontol Scand 1986; 44: 271–277.
Zhang K, Kim Y K, Cadenaro M et al. Effects of different exposure times and concentrations of sodium hypochlorite/ethylenediaminetetraacetic acid on the structural integrity of mineralized dentin. J Endod 2010; 36: 105–109.
Ikram O H, Patel S, Sauro S, Mannocci F . Micro-computed tomography of tooth tissue volume changes following endodontic procedures and post space preparation. Int Endod J 2009; 42: 1071–1076.
Mannocci F, Cavalli G, Gagliani M . Preface. In Mannocci F, Cavalli G, Gagliani M (eds). Adhesive restoration of endodontically treated teeth. London UK: Quintessence Publishing Co Ltd, 2008.
Sorensen J A, Martinoff J T . Intracoronal reinforcement and coronal coverage: a study of endodontically treated teeth. J Prosthet Dent 1984; 51: 780–784.
Mannocci F, Bertelli E, Sherriff M, Watson T F, Ford T R . Three-year clinical comparison of survival of endodontically treated teeth restored with either full cast coverage or with direct composite restoration. J Prosthet Dent 2002; 88: 297–301.
Mannocci F, Qualtrough A J, Worthington H V, Watson T F, Pitt Ford T R . Randomized clinical comparison of endodontically treated teeth restored with amalgam or with fiber posts and resin composite: five-year results. Oper Dent 2005; 30: 9–15.
Stavropoulou A F, Koidis P T . A systematic review of single crowns on endodontically treated teeth. J Dent 2007; 35: 761–767.
Salehrabi R, Rotstein I . Endodontic treatment outcomes in a large patient population in the USA: an epidemiological study. J Endod 2004; 30: 846–850.
Patel S . The first step: the endodontic treatment. In Mannocci F, Cavalli G, Gagliani M (eds). Adhesive restoration of endodontically treated teeth. pp 1–24. London UK: Quintessence Publishing Co Ltd, 2008.
Kim S, Kratchman S . Modern endodontic surgery concepts and practice: a review. J Endod 2006; 32: 601–623.
Duncan H F, Pitt Ford T R . The potential association between smoking and endodontic disease. Int Endod J 2006; 39: 843–854.
Velvart P, Peters C I, Peters O A . Soft tissue management: flap design, incision, tissue elevation, and tissue retraction. Endod Topics 2005; 11: 78–97.
Velvart P . Papilla base incision: a new approach to recession-free healing of the interdental papilla after endodontic surgery. Int Endod J 2002; 35: 453–460.
Frank A L, Glick D H, Patterson S S, Weine F S . Long-term evaluation of surgically placed amalgam fillings. J Endod 1992; 18: 391–398.
Friedman S . Expected outcomes in the prevention and treatment of apical periodontitis. In Ørstavik D, Pitt Ford T (eds). Essential endodontology: prevention and treatment of apical periodontitis, 2nd ed. pp 408–469. Oxford, UK: Blackwell Munksgaard Ltd, 2008.
Ng Y L, Mann V, Gulabivala K . Tooth survival following non-surgical root canal treatment: a systematic review of the literature. Int Endod J 2010; 43: 171–189.
Ng Y L, Mann V, Rahbaran S, Lewsey J, Gulabivala K . Outcome of primary root canal treatment: systematic review of the literature - Part 2. Influence of clinical factors. Int Endod J 2008; 41: 6–31.
Ng Y L, Mann V, Gulabivala K . Outcome of secondary root canal treatment: systematic review of the literature. Int Endod J 2008; 41: 1026–1046.
Gorni F G, Gagliani M M. The outcome of endodontic retreatment: a 2-yr follow-up. J Endod 2004; 30: 1–4.
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed paper
Rights and permissions
About this article
Cite this article
Patel, S., Barnes, J. Contemporary endodontics – part 2. Br Dent J 211, 517–524 (2011). https://doi.org/10.1038/sj.bdj.2011.1002
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.2011.1002
