
Abstract
Introduction:
Pregnancies in women with spinal cord injury (SCI) are at greater risk of morbidity and mortality. Although pregnancy after SCI is well elaborated in the literature, SCI occurring during pregnancy is rarely reported. Abrupt changes in the body physiology because of SCI and the resulting disability add a risk to maternal and fetal well-being. Not only is the burden of care increased but there is also a higher risk of developing pressure ulcers, urinary tract infections, autonomic instability, intrauterine growth retardation and venous thromboembolism.
Case Presentation:
We report a case of a 32-year-old lady who had a traumatic SCI at C6 level during the second trimester of her pregnancy. She was admitted to a tertiary care rehabilitation facility after 2 months of her injury. This case highlights the comprehensive approach toward her management, including rehabilitation, spinal intervention and obstetrical care. To the best of our knowledge, this is the first case report of its kind from the Middle East.
Discussion:
Multi-system involvement due to SCI during pregnancy results in intense physiological changes that affect the treatment options for anesthesia, surgery, labor and comprehensive rehabilitation. This case report emphasizes the need for well-equipped, specialized centers for similar patients in developing health systems and aims to increase the awareness for management of SCI during pregnancy using a comprehensive approach.
Similar content being viewed by others

Introduction
The management of pregnancy and labor in women with spinal cord injury (SCI) has received more attention by investigators and clinicians in recent years. Most of the data relate to reproductive health and obstetrical management of patients who already have an SCI before conceiving.1 Very few cases have been reported in the literature regarding individuals who sustain an SCI during their pregnancy.2 In addition to normal physiological changes of pregnancy, these patients undergo further physiological changes as a result of neurological injury. Sudden autonomic changes, immobility due to paralysis and psychological problems can impose threatening effects on pregnancy and its outcomes. In contrast, women with chronic SCI who have already adjusted to the physiological changes of SCI can plan their pregnancies under medical supervision. Acute SCI during pregnancy requires simultaneous management of trauma, obstetrical monitoring and rehabilitation care. The entire treatment can be considered under the umbrella of rehabilitation due to the holistic impact of injury on the patient.
Motor vehicle accidents account for 35–50% of spinal cord injuries.2 Specific data regarding SCI in the Kingdom of Saudi Arabia (KSA) is very limited as there is no national SCI registry. Overall, KSA has the highest auto accident rate among all Gulf countries.3 A hospital-based study from KSA showed that 79.2% of patients admitted with SCI were a result of motor vehicle accidents.4 SCI affects the young adults of KSA with a male to female ratio of 9:1;5 the incidence in pregnant women specifically is unknown.
This case highlights a comprehensive approach toward the management of SCI during pregnancy, including rehabilitation, spinal intervention and obstetrical care. It emphasizes the need for well-equipped specialized centers for similar patients in developing health systems, and aims to increase the awareness for management of SCI during pregnancy using a comprehensive approach.
Case presentation
A 32-year-old female school teacher with no known medical illness, G1 P0 A0, was involved in a motor vehicle accident during the second trimester of her pregnancy. She was an unrestrained passenger at the time of the accident. Her trauma resulted in C6-C7 fracture dislocation which was initially managed conservatively at a local hospital. The fetus remained safe during the trauma as evidenced by the obstetrical evaluation during initial assessment. At 2 months post injury and 27 weeks of gestation, she was admitted for inpatient rehabilitation with a diagnosis of C6 ASIA Impairment Scale grade B. Documentation regarding duration of spinal shock in the previous hospital was deficient; however, she had exaggerated deep-tendon reflexes and positive bulbocavernous reflexes, and preserved S4 and S5 sacral sensations at the time of admission to rehabilitation. Considering the obstetrical needs of the patient, a comprehensive interdisciplinary rehabilitation plan was established. At the time of admission, she was totally dependent in all the activities of daily living, transfers and mobility. Her main functional limitations were due to incomplete spastic tetraplegia, depression, bilateral heel pressure ulcers, and bowel and bladder incontinence. She had incomplete tetraplegia with C6 motor and sensory level. There was grade II spasticity (according to Modified Ashworth Scale) in lower limbs involving hip adductors, knee flexors and ankle planter flexors. Her spasticity in lower limbs and maternal body habitus due to pregnancy affected her nursing care, including positioning, bed mobility, transfers and perineal hygiene. Ultrasound evaluation showed a single viable fetus in cephalic presentation consistent with 27 weeks of gestation and normal amniotic fluid. Radiological evaluation of the cervical spine showed complete anterolisthesis of C6 over C7 causing spinal cord compression and bilateral locked facet joints.
The initial management was focused on the unstable cervical spine, psychological support, pressure ulcer management and fetal well-being. A multidisciplinary approach was considered that included a comprehensive rehabilitation program, neurosurgical management and obstetrical care. She received physical therapy, occupational therapy, art therapy and psychological support. Initially, because of her unstable spine, only bed-side maintenance exercises were initiated to prevent complications of prolonged immobility. She remained on heparin for prophylaxis for venous thromboembolism as well as mechanical prophylaxis, with compression stockings and intermittent pneumatic compression devices. Her heel pressure ulcers were managed conservatively by dressing, positioning and improving nutrition. Lower extremity spasticity was well controlled with Baclofen 25 mg thrice daily and Tizanidine 2 mg thrice daily. Suprapubic catheterization was carried out during the early third trimester of pregnancy after a urethral injury secondary to catheter pull during transfers. To avoid recurrent urethral injuries, a suprapubic catheter was considered for long-term bladder management.
After 2 weeks of admission, cervical spine decompression, C7 corpectomy and C6-T1 internal fixation were performed by an anterior approach followed by provision of cervical collar. Our patient, not reported to have had autonomic dysreflexia (AD) earlier, had three episodes of AD during her cervical spine fixation that was performed under general anesthesia. Her blood pressure went up to 170/100 mm Hg from a preoperative baseline blood pressure of 90/60 mm Hg. She was considered to be at high risk for AD. Postoperatively, her hospital course was complicated with urinary tract infection and post-operative chest infection requiring treatment with antibiotics. She was closely followed-up by obstetricians with serial examinations, ultrasounds and cardiotocography. Because of her impaired body sensations and relatively spared sensation in hands, she was taught about manual palpation of fetal movements using her hands. Considering her as high risk for AD, an elective caesarian section was carried out under spinal anesthesia that remained uneventful. She delivered a premature baby boy weighing 1.7 kg at 35 weeks of gestation without complications, with APGAR score 8 (Figure 1). There were no perioperative surgical complications. After initial neonatal care, the baby remained healthy. A close bonding between the mother and her infant was encouraged during her rehabilitation course. The infant stayed with the mother throughout the rehabilitation course and was kept on formula feed due to concerns of side effects of medications being used by the patient. A female relative stayed with the patient and her infant to look after them. There was a considerable improvement in the patient’s mood and motivation.

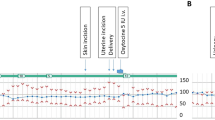
Graphical presentation of ultrasound findings for gestational age (GA) and estimated fetal birth weight. (EFW). At 34 weeks of gestation, EFW for this patient was below the 10th percentile (1.7 Kg). Neonates with women with SCI are at an increased risk for low birth weight.
With active participation in the therapy sessions, the patient showed functional improvement, especially in her upper extremities. At the time of discharge, she was modified, independent in eating and required minimal assistance in grooming and upper body dressing. She remained totally dependent in lower body dressing, bathing, toileting and transfers. She was trained in using a joystick-controlled power wheelchair and was provided with medical bed, air mattress, transfer hoist, wrist-hand orthosis and ankle-foot orthosis. Continence was achieved with suprapubic catheter and a regular bowel program. Sexuality and fertility issues were discussed with the patient and her partner. Family members were trained for assistance in provision of care to the patient and baby at home. A long-term plan for psycho-social support and vocational services were arranged before the patient’s discharge. She did not wish to resume her teaching career after discharge as she wanted to focus on taking care of her child. She was scheduled for continued follow-up as an outpatient.
Discussion
Pregnancies in women with SCI have a high risk of morbidity and mortality.6 Moreover, sudden changes in the body physiology due to SCI and the resulting disability add a risk to maternal and fetal well-being. The burden of care is increased in pregnant patients sustaining an acute SCI when compared with patients with chronic SCI who conceive long after their acute injury. For our patient, considering her medical, surgical, obstetrical and rehabilitation needs, a comprehensive treatment plan was established, including inpatient rehabilitation.
Surgical stabilization of spine is safe in pregnancy.7 It is of considerable importance that during the diagnostic evaluation of spine, the fetus is shielded from the radiation exposure.1 One of the preventable complications of SCI is pressure ulcers, and these should be equally preventable during pregnancy. Immobility, spasticity and poor positioning contribute to formation of pressure ulcers in patients with SCI. Weight gain during pregnancy is an additional risk factor. Medical bed, air mattress, seating arrangement and wheelchair may require modifications accordingly. It is preferable in third trimester to avoid rest in supine position, which causes aortocaval compression. A lateral tilt position may optimize uterine perfusion.1
Pregnant women at baseline are five times more likely to have venous thromboembolism. SCI population has added risk of decreased mobilization. Selection of anti-coagulation medications is usually based upon its placental permeability. Heparin is the anti-coagulant of choice for prophylaxis and treatment of venous thromboembolism because it does not cross placenta. In general population, the risk of asymptomatic bacteriuria leading to pyelonephritis during pregnancy is reported to be 65%.8 There is an increased risk of urinary tract infection in pregnant SCI patients with neurogenic bladder and poor perineal hygiene. urinary tract infection is independently associated with intrauterine growth restriction, preeclampsia, preterm delivery and cesarean delivery.9 Hence, it remains as one of the most important preventable complications in pregnant patients. Clean intermittent catheterizations or suprapubic catheterization are feasible options. Since anti-cholinergic medications are pregnancy category B, they can be considered for neurogenic bladder management with clean intermittent catheterizations. After discussing treatment options with our patient, she preferred to have a suprapubic catheterization because of hip adductor spasticity interfering with positioning and lack of caregiver willingness to continue clean intermittent catheterizations after discharge.
Significant increase in spasticity is reported during pregnancy in patients with tetraplegia. Increased spasticity can be a symptom of labor and AD.10 Spasticity can not only cause discomfort, but also interfere with positioning, hygiene, transfers and sleep. The potential benefits warranted the use of Baclofen and Tizanidine despite potential risks in pregnancy because spasticity was interfering with skin care and perineal hygiene. Chances of skin complications and urine infections to complicate her pregnancy were considered to be high. Infections, reciprocally, can also increase spasticity and result in poor functional outcomes. Non-pharmacological measures including stretching, range of motion exercises, positioning and orthoses did not produce the desired therapeutic effects in controlling her spasticity. So, pharmacological treatment was considered, and it led to an improvement in her spasticity and facilitated positioning, bed mobility, transfers, and bowel and bladder management. Since Baclofen is pregnancy category C, frequent monitoring and evaluation of fetus was carried out, and the obstetrician was also involved in decision making of starting anti-spasticity medications.
One of the threatening complications in SCI is AD. AD is characterized by a sudden increase in blood pressure; AD develops in individuals with a neurologic level of spinal cord injury at or above the sixth thoracic vertebral level (T6) in response to an autonomic imbalance in the spinal cord nervous system. Pregnancy must be considered high risk for patients prone to AD.7 First-line treatment is removal of noxious stimuli followed by the use of medications to treat high blood pressure. It can be challenging to differentiate if the AD is due to uterine contractions or other noxious stimuli.2 In case it occurs because of uterine contractions, the blood pressure elevation occurs most often during the stimulus time and may be accompanied by headache, which subsides between contractions.
One of the challenges during labor is to differentiate AD from preeclampsia, as clinical presentation of both conditions is similar. The typical presentation of preeclampsia may be different from the typical triad of hypertension, proteinuria and edema, which makes the diagnosis more challenging; however, there are certain features of preeclampsia that can help to differentiate it from AD. It is reported that preeclampsia essentially never occurs before 24 weeks of gestation. In AD, unlike preeclampsia, there is increase in blood pressure and other symptoms usually during contraction of the uterus that subside with relaxation.11 AD during labor and delivery can be controlled by regional anesthesia.8 If regional anesthesia is not available or AD occurs despite regional anesthesia, hypertension can be managed with short-acting antihypertensive medications. If despite all measures it is not possible to manage AD during labor, it is recommended to proceed for cesarean section.11 During the start of labor, the SCI patients may not perceive uterine contractions due to impaired sensations. Hence they must be instructed to monitor uterine contractions by palpating their abdomen if hand function is preserved. Close obstetrical supervision is required in SCI patients with risk factors. The mode of delivery in SCI women is based upon standard obstetrical indications; however, chronic SCI patients may have pelvic deformities resulting in contracted pelvis that may interfere with labor. Regular monitoring of the cervix for effacement, dilation and progression of labor is needed. Because of poor abdominal muscle strength, vaginal delivery may require forceps assistance during the second stage of labor. Duration of spinal shock and absence of reflex activity may also have profound effects on labor.
Direct or indirect fetal injury can take place by several mechanisms during maternal traumatic injury. A survey including 45 women who were injured during pregnancy showed that there were 5 spontaneous abortions (11%), 5 children with ‘marked disability or malformation’ (11%), 1 death due to prematurity and 1 stillbirth due to placenta previa.1 Neonates of women with SCI are at increased risk for low birth weight and infant death.6 There is increased frequency of premature labor in patients with SCI especially with upper thoracic and cervical SCI that necessitates hospital admission. In 6-9 months after injury, menses usually return to normal and subsequent fertility is not altered.7 Additionally, in the presence of a major trauma like SCI, other injuries may often be overlooked, including mild traumatic brain injury, fractures of extremities and blunt trauma to chest or abdomen. A concomitant traumatic brain injury can cause hormonal disturbance and impaired cognitive and communication skills, which may affect the pregnancy and render the need of modification of rehabilitation program.
There are few non-clinical unique aspects of the case report. The patient was rehabilitated at the ministry of health hospital in Saudi Arabia, where Saudi patients receive treatment free of cost. Therefore, there were no financial obligations on the patients and family. Moreover, the average length of stay for rehabilitation of individuals with tetraplegia is around 6 months, which is far more than the international average. It is mainly due to lack of early referrals for rehabilitation and shortage of facilities offering comprehensive rehabilitation across the country. Saudi women prefer female therapists in situations where physical contact is required during exercise therapy. This is mainly due to religious, cultural and personal preferences. For the same reasons, female patients are not placed in shared rooms with males, and they are looked after by female nurses. Wherever possible, there are separate wards, gyms, pools, dining rooms and treatment areas for women in a hospital setting. There remains a high demand of female rehabilitation clinicians and health care providers in the country.
Conclusion
SCI occurring during pregnancy is a rare event that can affect maternal and fetal outcomes. This case highlights the need for specialized rehabilitation centers in developing health systems where traumatic SCI is on a rise. It is deemed important to increase the awareness among treating clinicians for understanding the unique challenges of SCI and its management during pregnancy. Acute inpatient rehabilitation is a suitable setting where other medical and surgical disciplines can provide coordinated care. In the developing world, safety precautions during traveling should be an integral part of counseling for pregnant women and their families.
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
Baker ER, Cardenas DD . Pregnancy in spinal cord injured women. Arch Phys Med Rehabil 1996; 77: 501–507.
Groves CC, Poudel MK, Baniya M, Rana C, House DR . Descriptive study of earthquake-related spinal cord injury in Nepal. Spinal Cord 2017; 55: 705–710.
Al-Arabi KM, Al-Sebai MW . Epidemiological survey of spinal cord injury: a study of 377 patients. Ann Saudi Med 1992; 12: 269–273.
Ansari S, Akhdar F, Mandoorah M, Moutaery K . Causes and effects of road traffic accidents in Saudi Arabia. Public Health 2000; 114: 37–39.
Alshahri SS, Cripps RA, Lee BB, Al-Jadid MS . Traumatic spinal cord injury in Saudi Arabia: an epidemiological estimate from Riyadh. Spinal Cord 2012; 50: 882–884.
Signore C, Spong CY, Krotoski D, Shinowara NL, Blackwell SC . Pregnancy in women with physical disabilities. Obstet Gynecol 2011; 117: 935–947.
Cross LL, Meythaler JM, Tuel SM, Cross AL . Pregnancy following spinal cord injury. West J Med 1991; 154: 607–611.
Cross LL, Meythaler JM, Tuel SM, Cross AL . Pregnancy, labor and delivery post spinal cord injury. Paraplegia 1992; 30: 890–892.
Mazor-Dray E, Levy A, Schlaeffer F, Sheiner E . Maternal urinary tract infection: is it independently associated with adverse pregnancy outcome? J Matern Fetal Neonatal Med 2009; 22: 124–128.
Desmond J . Paraplegia: problems confronting the anaesthesiologist. Can Anaesth Soc J 1970; 17: 435–451.
Burns AS, Jackson AB . Gynecologic and reproductive issues in women with spinal cord injury. Phys Med Rehabil Clin North Am 2001; 12: 183–199.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Poster presentation at 19th Annual Saudi Neuroscience Symposium, Dammam, Saudi Arabia Nov 2011 by Ahmad Zaheer Qureshi (First Author).
Rights and permissions
About this article

Cite this article
Qureshi, A., Ullah, S., AlSaleh, A. et al. Spinal cord injury during the second trimester of pregnancy. Spinal Cord Ser Cases 3, 17052 (2017). https://doi.org/10.1038/scsandc.2017.52
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/scsandc.2017.52
