
Abstract
Objectives:
To assess the role of anxiety, depressive mood and religious coping in erectile function among Iranian patients with spinal cord injury (SCI).
Setting:
Brain and Spinal Cord Injury Repair Research Center, Neuroscience Institute, Tehran University of Medical Sciences, Tehran, Iran.
Methods:
A sample of N=93 men with SCI participated in this cross-sectional study. Levels of anxiety and depressive mood were assessed using the Hospital Anxiety and Depression Scale. Religious coping strategies were measured using the 14-items Brief Coping Questionnaire. Erectile function was assessed using the International Index of Erectile Function. The joint effect of anxiety, depressive mood and religious coping strategies on erectile function was assessed by performing stepwise multiple linear regression analyses.
Results:
The mean age of the SCI patients was 37.8 years with a mean post-injury time of 4.6 years. Multivariate regression analyses indicated that age (B=−0.27, 95% CI=−0.47 to −0.07), education (B for higher education=0.63, 95% CI=0.24 to 1.02), the American Spinal Injury Association impairment scale (B for complete impairment=−3.36, 95% CI=−3.82 to −2.89), anxiety (B=−3.56, 95% CI=−5.76 to −1.42), positive religious coping (B=0.30, 95% CI=0.03 to 0.57), negative religious coping (B=−0.56, 95% CI=−0.82 to −0.29) and the duration of injury (B=−0.25, 95% CI=−0.22 to −0.29) were all independent factors influencing erectile function in SCI patients.
Conclusion:
Overall, the results indicated that SCI patients who use positive religious coping strategies had better erectile function compared with individuals who applied negative religious coping strategies. Furthermore, higher levels of anxiety, greater impairment and longer duration of injury turned out to be risk factors for erectile dysfunction.
Similar content being viewed by others

Introduction
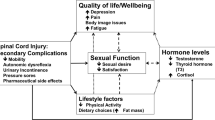
Spinal cord injuries (SCIs) can have detrimental effects on various aspects of life for affected individuals.1, 2 Apart from severely impacting on overall quality of life, SCI also impacts on sexual quality of life by reducing sexual function and the sensation of the genital organs.3, 4 SCI predominantly affects males aged between 18 and 45 years.5 Previous studies have shown that male sexual dysfunctions are very common among SCI patients, with erectile dysfunction (ED) being the most prevalent complaint.6, 7, 8 ED is an important public health problem defined as the persistent inability to achieve and maintain an erection sufficient for satisfactory sexual activity.9 A vast amount of literature has identified ED as a frequent consequence of SCI.10, 11 It has been recognized that SCI, its level and lesion severity can significantly affect both types of erection—the reflexogenic and the psychogenic erection—and consequently alter a patient’s overall erectile ability.12 Therefore, improvement of sexual functioning in patients suffering from SCI is considered a central issue during the post-SCI rehabilitation process, eventually leading to an overall improvement of their quality of life.13
Identification of risk factors of ED in this specific patient cohort is an important step for the development of appropriate and holistic prevention and treatment programs. Previous studies have shown that—among others—higher levels of anxiety and depressive mood are considered risk factors for male sexual dysfunction in patients with SCI.14, 15 This particularly seems to be the case in SCI patients also reporting significant medical comorbidities, which can lead to increased pain expectation, discomfort, anticipation of sexual distress, anxiety related to genital function or an altered body image.16 Moreover, depressed SCI patients frequently suffer from loss of energy and loss of overall and sexual interest and decreased self-esteem, which can lead to various types of male sexual dysfunction, although loss of sexual desire has been the most frequent complaint reported.8, 10
Patients with SCI have to deal with multiple challenges. To adapt and cope with the distressing situation or event, they apply a variety of coping strategies,1, 2, 17 some of which have shown to be beneficial, whereas others tend to act dysfunctionally.18 Religious coping is one such beneficial strategy and is considered an active coping mechanism frequently used in individuals suffering from all sorts of bodily disabilities1, 19 and often leading to a higher quality of life. The use of such positive religious coping strategies might be similarly helpful in patients with SCI when being confronted with injury-related sexual impairment. Two broad religious coping patterns have been suggested in the literature: positive (adaptive) and negative (maladaptive) religious coping strategies. Positive religious coping is related to a secure relationship with a supportive God, whereas negative religious coping describes a less secure relationship with God who presents itself distant and punishing.20
Given the beneficial role of religious coping in other patient groups having to deal with bodily disabilities, we hypothesized that there would be a relationship between depressive mood, anxiety and religious coping with erectile dysfunction in patients with SCI. Therefore, the aim of the present study was to investigate the influence of comorbid anxiety and depressive mood in patients suffering from SCI on their erectile function by considering the usefulness of positive religious coping in dealing with the injury. For this, the effects of religious coping on erectile functioning and sexual quality were explored.
Materials and methods
Patients and settings
Male patients with SCI participated in this cross-sectional study conducted in Tehran, Iran. Participants were recruited consecutively from the Brain and Spinal Cord Research Center—an academic referral center. Individuals were included if they were male and at least 18 years of age at the time of study. To avoid potential biases resulting from the influence of certain medical comorbidities known to cause male sexual dysfunction, patients suffering from diabetes mellitus, cardiovascular diseases, hypertension, rheumatic diseases and kidney disease were excluded from this study.21 A total of 100 patients with SCI were approached. Seven patients declined to participate in the study for personal reasons, resulting in a final sample of N=93 individuals with SCI meeting the inclusion criteria. Demographic and injury-related characteristics were obtained through interviews (self-report), neurologic examinations and hospital records. The study was approved by the Institutional Review Board of the Brain and Spinal Cord Injury Research Center in Neuroscience Institute, Tehran University of Medical Sciences, Tehran, Iran. All the patients provided written informed consent before entering the study.
Measures
Demographic and injury-related characteristics of the men participating in the study were collected using study-specific questionnaires. SCI severity was classified according to the American Spinal Injury Association (ASIA) assessment protocol into complete (ASIA grade A) vs incomplete (ASIA grades B and E) SCI.22 All the patients were rated by a neurosurgeon who was blinded to the study aims.
To assess religious coping strategies, the 14-item self-report Brief Religious Coping Questionnaire was used.23 The questionnaire consists of two subscales including positive and negative religious coping. Items are rated on a four-point Likert-type scale ranging from 1 (strongly disagree) to 4 (strongly agree), resulting in a total score ranging from 7 to 28 for each subscale.23 The inventory has been validated in an Iranian population sample and has demonstrated excellent psychometric properties.24
ED was assessed using the short version of the International Index of Erectile Function—the IIEF-5.25 The IIEF-5 contains five items assessing the presence and severity of ED over the past 6 months. Each item is scored on a five-point Likert-type scale ranging from 1 to 5, with higher scores indicating better erectile functioning. IIEF-5 scores range from 5 to 25. The presence and severity of ED was classified based on the IIEF-5 total score into absent (>21), mild (17–21), mild/moderate (12–16), moderate (8–11) and severe (<8). The psychometric properties of the Iranian version of the IIEF-5 have been previously demonstrated.26
Anxiety and depressive mood were assessed using the Hospital Anxiety and Depression Scale.27 The questionnaire consists of 14 items, each rated on a four-point Likert-type scale ranging from 0 (absence of symptoms) to 3 (severe symptoms), resulting in a maximum score of 21. An Iranian version of Hospital Anxiety and Depression Scale exists and has shown to have adequate psychometric properties.27
Statistical analysis
The total IIEF-5 score was considered as the main erectile functioning outcome variable. The level of significance was set at 5%. The B coefficient and 95% confidence intervals were reported as indicators of any association between the dependent and the independent variables. Negative values indicated a negative relationship, whereas positive values indicated a positive relationship between the variables. Normality of the variables was tested using the Kolmogorov–Smirnov test. Logarithmic transformation was used to convert non-normally distributed variables. Stepwise multivariate linear regression analyses were performed to assess the magnitude and significance of the associations between anxiety, depressive mood, religious coping and erectile functioning. To identify the factors affecting erectile functioning, univariate analyses (that is, Pearson’s product moment correlations) were performed before running the multivariate linear regressions. Pearson’s product moment correlations were used to identify the factors (using P-value <0.15) to be included in the multivariate model. A P-value <0.05 was considered statistically significant unless stated otherwise. All statistical analyses were performed using SAS version 9.1.3 (SAS Institute Inc., Cary, NC, USA).
Results
Sample characteristics are shown in Table 1. The mean age of the participants was 37.76 years (s.d.=9.2, ranging from 19 to 63 years). Overall, SCI patients reported more positive religious coping than negative religious coping (mean of 24.3, s.d.=3.5 vs 14.90, s.d.=3.7). In addition, the participants reported slightly higher levels of anxiety than depressive mood (mean=7.79, s.d.=4.0 vs 7.41, s.d.=3.2). Eighteen (19.4%) patients reported having completed a higher education and 11 (11.8%) patients were employed. Almost half of the patients (51.6%) suffered from a complete SCI according to the AIS (ASIA Impairment Scale) A (Table 1). On the basis of the IIEF-5 classification for ED, only 29% (n=27) of the patients did not suffer from ED, whereas mild, mild/moderate, moderate and severe ED was reported by 14% (n=13), 7.7% (n=7), 8.7% (n=8) and 41% (n=38), respectively.
Pearson's product correlations revealed significant correlations between erectile functioning and depression (r=−0.30, P=0.003), anxiety (r=−0.38, P=0.003), positive religious coping (r=0.25, P=0.031), negative religious coping (r=−0.215, P=0.038), AIS (r=−0.22, P=0.032), age (r=−0.25, P=0.016), injury duration (r=0.20, P=0.05) and education (r=0.30, P=0.004; data not shown).
Similarly, when entered into the multivariate regression model, significant independent effects of age (B=−0.27, 95% CI=−0.47 to −0.07), education (B for higher education=0.63, 95% CI=0.24 to 1.02), ASIA (B for complete impairment=−1.76, 95% CI=−2.24 to −1.28), anxiety (B=−3.59, 95% CI=−5.75 to −1.42), positive religious coping (B=0.30, 95% CI=0.03 to 0.57), negative religious coping (B=−0.56, 95% CI=−0.82 to −0.30) and depression (B=−0.75, 95% CI=−1.30 to −0.20) on erectile function could be detected (Table 2).
Discussion
Studies investigating the risk factors for ED in men with SCI are scarce, and the majority of the existing studies have focused on demographic variables and injury-related factors such as injury level, severity, distress and so on.2, 14, 16 The aim of the present study was to explore how psychological comorbidities (that is, anxiety and depressive mood), as well as religious coping, influence SCI patients’ erectile functioning. Previous research has shown that religiousness as an individual coping strategy can have a significant influence on the rehabilitation process and the re-establishment of overall quality of life in patients with SCI.28, 29 This may also be true for their sexual quality of life and erectile function, although this specific aspect has received little attention in previous research.
Religious coping
According to our findings, positive religious coping was associated with less erectile dysfunction, with men reporting being more religious, also reporting less erectile impairment and dysfunction—independent of the injury level and severity, as well as psychological comorbidities. SCI patients may use spiritual coping to deal with their disability and its effects on erectile dysfunction. However, the strength of the association was small, and therefore the results have to be interpreted with caution and replicated in larger samples as it could reflect unmeasured confounding and/or measurement error. Nevertheless, our results are somewhat in accordance with findings from a previous study reporting a positive association between spirituality, life satisfaction and overall quality of life in people with spinal cord injury, and our findings are justifiable.28
Associations between sexual problems and more general sexual behaviors with religiosity have also been investigated in several other studies. Gudorf,30 for example, reported people with sexual dismorphism to be more engaged in religious beliefs and behaviors compared with people with a ‘normal’ sexual appearance. Less engagement in risky sexual behaviors among religious people compared with non-religious people may also explain the important implications of religiosity in coping with sexual dysfunctions.31, 32
Anxiety and depressive mood
Apart from religious coping, we were also able to observe a significant association between anxiety and depressive mood and erectile function in men with SCI. It has been repeatedly shown that depressive mood and anxiety levels are high in patients with SCI.2, 16 Equally, both have been shown to act as important factors influencing men’s sexual function.33, 34 It has been argued that psychological factors are more important for a satisfying sex life and the quality of the relationship in patients with spinal paraplegia.35 Molina-Leyva et al.,36 for example, suggest that when secondary psychological problems in individuals suffering from chronic physiologic conditions are present, very often this may also negatively affect sexual functioning. In other words, in people with psychosis or other psychological disorders, sexual activity may be decreased because of their impaired mental health. In addition, physically handicapped individuals reporting sexual impairment often tend to become sexually isolated—therefore further aggravating and extending the problem.37 In people with SCI, the limited mobility and inappropriate coping with the situation can cause anxiety/depressive mood, which may be further enhanced by additional disease-related impairments such as sexual problems. Another mechanism that may underlie the link between sexual disability and anxiety/depressive mood might be attributable to social relations—especially romantic relationships—in people suffering from SCI. Several studies have shown that people with sexual problems receive lower degree of social support from their friends or social networks than healthy people.38, 39 The mediating role of religious coping on depressive mood and anxiety in such people has also been confirmed in previous studies.29, 40
Age, education and AIS levels
In this study, we were also able to observe an association between erectile function and age. Erectile dysfunction was found to be an age-dependent problem with prevalences increasing as function of age.41, 42 Interestingly, the more time had passed since the injury, the less erectile problems were reported. This is in accordance with the findings from another study reporting a positive association between time since injury and sexual satisfaction.43 This can be explained by the fact that patients with SCI may take some time to adapt to the situation and to learn more problem-focused strategies to deal with their condition and related sexual problems.
We also found an association between AIS level and erectile function. Again, this result is consistent with previous studies showing significant relationships between the degree of the injury and the location and sexual functioning.44, 45 In addition, it has been reported that AIS level affects other dimensions of sexual function in men with SCI. Therefore, it was determined that men with incomplete SCI were more likely to experience orgasm compared with men with complete SCI.46
Our results also showed that the level of education was a significant contributing factor to sexual functioning in men with SCI. Again, results from a previous study showed that patients with greater improvement in sexual function after time also report higher levels of education.47 This could be explained by the fact that as the level of education is one of the personality-related predisposing factors for help-seeking behaviors and a healthier lifestyle, the well-educated patients are more likely to have help-seeking behavior for sexual function.
Limitations
The results have to be considered in light of a number of limitations. First, we used a consecutive sample, and therefore our findings may not be generalizable to all people with SCI. Using a randomized, multicenter study with larger samples may overcome this limitation in future studies. Second, we designed a cross-sectional study, which is inherently limited for detecting causal relationships. Thus, future research should consider using longitudinal studies to better understand the direction and nature of these associations. Finally, we used self-report measures to investigate sexual function and other variables such as anxiety, depressive mood and religious coping. Recall or information bias, as well as social desirability, may have confounded our results; however, for socially sensitive topics such as sexual behavior, using these scales is inevitable.
Conclusion
Significant associations between religious coping, anxiety and depressive mood and erectile functioning in men with SCI could be observed. This is the first study to demonstrate the importance of religiosity in coping with sexual disabilities resulting from SCI. Further research is needed to understand how religious coping may influence the adjustment to chronic conditions, especially in those with physical disabilities related to spinal cord damage.
Data archiving
There were no data to deposit.
References
Harvey L . Management of Spinal Cord Injuries: a Guide for Physiotherapists. Churchill Livingstone: Philadelphia, PA, USA. 2008.
Craig A, Tran Y, Middleton J . Psychological morbidity and spinal cord injury: a systematic review. Spinal Cord 2009; 47: 108–114.
Elliott SL . Problems of sexual function after spinal cord injury. Prog Brain Res 2006; 152: 387–399.
Dahlberg A, Alaranta HT, Kautiainen H, Kotila M . Sexual activity and satisfaction in men with traumatic spinal cord lesion. J Rehabil Med 2007; 39: 152–155.
Johnson RD . Descending pathways modulating the spinal circuitry for ejaculation: effects of chronic spinal cord injury. Prog Brain Res 2006; 152: 415–426.
Anderson KD . Targeting recovery: priorities of the spinal cord-injured population. J Neurotrauma 2004; 21: 1371–1383.
Brown DJ, Hill ST, Baker HW . Male fertility and sexual function after spinal cord injury. Prog Brain Res 2006; 152: 427–439.
Anderson KD, Borisoff JF, Johnson RD, Stiens SA, Elliott SL . The impact of spinal cord injury on sexual function: concerns of the general population. Spinal Cord 2007; 45: 328–337.
NIH Consensus Conference. Impotence. NIH Consensus Development Panel on Impotence. JAMA 1993; 270: 83–90.
Anderson KD, Borisoff JF, Johnson RD, Stiens SA, Elliott SL . Long-term effects of spinal cord injury on sexual function in men: implications for neuroplasticity. Spinal Cord 2007; 45: 338–348.
Alexander MS, Bodner D, Brackett NL, Elliott S, Jackson AB, Sonksen J et al. Development of international standards to document sexual and reproductive functions after spinal cord injury: preliminary report. J Rehabil Res Dev 2007; 44: 83–90.
Ramos AS, Samso JV . Specific aspects of erectile dysfunction in spinal cord injury. Int J Impot Res 2004; 16 (Suppl 2): S42–S45.
Fisher TL, Laud PW, Byfield MG, Brown TT, Hayat MJ, Fiedler IG . Sexual health after spinal cord injury: a longitudinal study. Arch Phys Med Rehabil 2002; 83: 1043–1051.
Hancock KM, Craig AR, Dickson HG, Chang E, Martin J . Anxiety and depression over the first year of spinal cord injury: a longitudinal study. Paraplegia 1993; 31: 349–357.
Cobo Cuenca AI, Sampietro-Crespo A, Virseda-Chamorro M, Martin-Espinosa N . Psychological impact and sexual dysfunction in men with and without spinal cord injury. J Sex Med 2015; 12: 436–444.
Bancroft J, Janssen E . The dual control model of male sexual response: a theoretical approach to centrally mediated erectile dysfunction. Neurosci Biobehav Rev 2000; 24: 571–579.
Babamohamadi H, Negarandeh R, Dehghan-Nayeri N . Coping strategies used by people with spinal cord injury: a qualitative study. Spinal Cord 2011; 49: 832–837.
Crisp CC, Vaccaro CM, Pancholy A, Kleeman S, Fellner AN, Pauls R . Is female sexual dysfunction related to personality and coping? An exploratory study. Sex Med 2013; 1: 69–75.
Johnstone B, Glass BA, Oliver RE . Religion and disability: clinical, research and training considerations for rehabilitation professionals. Disabil Rehabil 2007; 29: 1153–1163.
Thune-Boyle IC, Stygall JA, Keshtgar MR, Newman SP . Do religious/spiritual coping strategies affect illness adjustment in patients with cancer? A systematic review of the literature. Soc Sci Med 2006; 63: 151–164.
Burnett AL . Erectile dysfunction. J Urol 2006; 175 (3 Pt 2): S25–S31.
American Spinal Injury Association and International Medical Society of Paraplegia International Standards for Neurological Classification of Spinal Cord Injury, 6th edn. ASIA: Chicago, IL, USA. 2006.
Pargament KI, Koenig HG, Perez LM . The many methods of religious coping: development and initial validation of the RCOPE. J Clin Psychol 2000; 56: 519–543.
Rohani C, Khanjari S, Abedi HA, Oskouie F, Langius-Eklof A . Health index, sense of coherence scale, brief religious coping scale and spiritual perspective scale: psychometric properties. J Adv Nurs 2010; 66: 2796–2806.
Ziaei T, Salehi M, Azarbayejani A, Tavakol HK, Shabani M . A comparison of sexual self-concept between blind and physically-motor disabled people. J Sex Med 2015; 12: 349–349.
Pakpour AH, Zeidi IM, Yekaninejad MS, Burri A . Validation of a translated and culturally adapted Iranian version of the International Index of Erectile Function. J Sex Marital Ther 2014; 40: 541–551.
Montazeri A, Vahdaninia M, Ebrahimi M, Jarvandi S . The Hospital Anxiety and Depression Scale (HADS): translation and validation study of the Iranian version. Health Qual Life Outcomes 2003; 1: 14.
Brillhart B . A study of spirituality and life satisfaction among persons with spinal cord injury. Rehabil Nurs 2005; 30: 31–34.
Rahnama P, Javidan AN, Saberi H, Montazeri A, Tavakkoli S, Pakpour AH et al. Does religious coping and spirituality have a moderating role on depression and anxiety in patients with spinal cord injury? A study from Iran. Spinal Cord 2015; 53: 870–874.
Gudorf CE . The erosion of sexual dimorphism: challenges to religion and religious ethics. J Am Acad Relig 2001; 69: 863–891.
Moreau C, Trussell J, Bajos N . Religiosity, religious affiliation, and patterns of sexual activity and contraceptive use in France. Eur J Contracept Reprod Health Care 2013; 18: 168–180.
Njus DM, Bane CM . Religious identification as a moderator of evolved sexual strategies of men and women. J Sex Res 2009; 46: 546–557.
Hayes RD, Dennerstein L, Bennett CM, Sidat M, Gurrin LC, Fairley CK . Risk factors for female sexual dysfunction in the general population: exploring factors associated with low sexual function and sexual distress. J Sex Med 2008; 5: 1681–1693.
Burri A, Spector T, Rahman Q . The etiological relationship between anxiety sensitivity, sexual distress, and female sexual dysfunction is partly genetically moderated. J Sex Med 2012; 9: 1887–1896.
Kreuter M, Sullivan M, Siosteen A . Sexual adjustment and quality of relationship in spinal paraplegia: a controlled study. Arch Phys Med Rehabil 1996; 77: 541–548.
Molina-Leyva A, Almodovar-Real A, Carrascosa JC, Molina-Leyva I, Naranjo-Sintes R, Jimenez-Moleon JJ . Distribution pattern of psoriasis, anxiety and depression as possible causes of sexual dysfunction in patients with moderate to severe psoriasis. An Bras Dermatol 2015; 90: 338–345.
Maart S, Jelsma J . The sexual behaviour of physically disabled adolescents. Disabil Rehabil 2010; 32: 438–443.
Peleg-Sagy T . With a little help from my friends self and social support in predicting sexual dissatisfaction among female medical students. J Sex Med 2015; 12: 263–263.
Bryant-Davis T, Ullman SE, Tsong YY, Gobin R . Surviving the storm: the role of social support and religious coping in sexual assault recovery of african american women. Violence Against Women 2011; 17: 1601–1618.
Marini I, Glover-Graf NM . Religiosity and spirituality among persons with spinal cord injury: attitudes, beliefs, and practices. Rehabil Couns Bull 2011; 54: 82–92.
Lewis RW, Fugl-Meyer KS, Bosch R, Fugl-Meyer AR, Laumann EO, Lizza E et al. Epidemiology/risk factors of sexual dysfunction. J Sex Med 2004; 1: 35–39.
Garos S, Kluck A, Aronoff D . Prostate cancer patients and their partners: differences in satisfaction indices and psychological variables. J Sex Med 2007; 4: 1394–1403.
Lombardi G, Del Popolo G, Macchiarella A, Mencarini M, Celso M . Sexual rehabilitation in women with spinal cord injury: a critical review of the literature. Spinal Cord 2010; 48: 842–849.
Sipski ML, Alexander CJ, Rosen R . Sexual arousal and orgasm in women: effects of spinal cord injury. Ann Neurol 2001; 49: 35–44.
Biering-Sorensen F, Sonksen J . Sexual function in spinal cord lesioned men. Spinal Cord 2001; 39: 455–470.
Sipski M, Alexander CJ, Gomez-Marin O . Effects of level and degree of spinal cord injury on male orgasm. Spinal Cord 2006; 44: 798–804.
Sharma SC, Singh R, Dogra R, Gupta SS . Assessment of sexual functions after spinal cord injury in Indian patients. Int J Rehabil Res 2006; 29: 17–25.
Acknowledgements
We thank all patients who participated in the study. AB reports an Ambizione personal career fellowship from the Swiss National Science Foundation.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Pakpour, A., Rahnama, P., Saberi, H. et al. The relationship between anxiety, depression and religious coping strategies and erectile dysfunction in Iranian patients with spinal cord injury. Spinal Cord 54, 1053–1057 (2016). https://doi.org/10.1038/sc.2016.7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2016.7
This article is cited by
-
Anxiety Levels and Sexual Functions of Patients Performing Clean Intermittent Catheterization
Sexuality and Disability (2021)
