
Abstract
Study design:
Retrospective analysis.
Objectives:
In patients with spinal cord injury, limitations in upper extremity (UE) motor function are cited as a reason for the lack of adherence to clean intermittent catheterization (CIC). By examining the UE function in spinal cord injury (SCI) patients, we aim to provide insight into why CIC 'dropout' occurs and determine a more appropriate target percentage for CIC in this patient population.
Setting:
United States centers participating in National Spinal Cord Injury Database (NSCID).
Methods:
We assessed discharge data from the 2006 to 2012 NSCID. Neurologic motor scores for C5 to C8 (involved in UE movement) were transformed into a binary variable consisting of the ability ('strong') or the inability ('weak') to achieve active motion against resistance. We generated an algorithm based on expert opinion and published literature to categorize a person’s ability to perform CIC by the UE function alone.
Results:
Of the 4481 patients evaluated, 77.3% were unable to volitionally void. Of this subset, 58.8% were categorized as able to catheterize, 12.9% as possibly able, 4.3% as only able with surgical assistance and 23.3% as unable. Among patients discharged with an indwelling catheter, 33.4% had adequate UE function for CIC. Among patients performing CIC at discharge, 14.1% had inadequate UE function for self-catheterization.
Conclusions:
CIC dropout may occur at least, in part, because of inadequate UE motor function. In a 'best-case' scenario, ~76% of patients with SCI who cannot volitionally void could potentially perform CIC given appropriate assistance.
Similar content being viewed by others


Introduction
Roughly 270 000 persons in the United States have sustained a spinal cord injury (SCI), with an estimated 12 000 new cases occurring annually.1 The majority of patients with SCI have bladder dysfunction because of their injury, with over 75% unable to volitionally void.2 As Lapides et al.3 published their seminal work in 1972, clean intermittent catheterization (CIC) has been championed as the 'gold standard' in what patients and physicians should strive to achieve for neurogenic bladder management.3 Compared with indwelling catheters, condom catheters and reflex voiding, there are significantly fewer complications in persons performing CIC.4, 5, 6 However, many patients with SCI have difficulty in performing CIC. This includes patients with (a) limited upper extremity (UE) motor function, (b) anatomic limitations that make accessing the urethra difficult (e.g., females or obese persons) and (c) limited functional bladder capacity (due to detrusor overactivity or poor bladder compliance). Thus, in many instances, CIC may not be feasible from a functional or a social standpoint.
To regain bladder independence, many patients frequently opt for indwelling urethral or suprapubic urinary catheters. Although nearly 60% of patients who are unable to volitionally void after SCI are performing CIC at the time of discharge from rehabilitation, only half of this subset continue to do so at 5-year follow-up.2 Although urologic surgical intervention can help patients with incontinence or certain anatomic problems, UE function is in most instances irreparable.
The purpose of this study is to provide an in-depth look at the UE motor function in the SCI population at the time of discharge from rehabilitation, with additional attention to other anatomic factors such as gender and body mass index (BMI) that might affect self-catheterization. From this information, we hope to provide insight into why CIC 'dropout' occurs and to more accurately determine a 'true' target percentage for CIC in the SCI population.
Patients and methods
We assessed Form I data for the years 2006 to 2012 from the National Spinal Cord Injury Database (NSCID), a large database that includes medical and demographic data on patients with SCI in designated Model Spinal Cord Injury Systems facilities in the United States.7 Form I is administered during a patient’s initial rehabilitation process, before discharge from an in-patient rehabilitation service. As part of the evaluation, a complete neurologic motor exam is administered at the time of discharge, including a separate assessment of the left and right side from C5 to C8. The motor scores for each side and level are graded individually from 0 to 5 (0=total paralysis; 1=palpable or visible contraction; 2=active movement, full range of motion with gravity eliminated; 3=active movement, full range of motion against gravity; 4=active movement, full range of motion against moderate resistance; 5=active movement, full range of motion against full resistance). Form I additionally includes patient demographics, patient health information and bladder management method at discharge.
We transformed the neurologic motor scores at levels C5 to C8 (involved in the control of movement of the UEs) into a binary variable, consisting of the ability or the inability to achieve active motion against moderate or full resistance and reclassified them as 'strong' (manual muscle test grade 4 or 5) and 'weak' (manual muscle test grade 0, 1, 2 or 3), respectively. Using these scores and expert opinion, we characterized a person’s ability to self-catheterize based only on UE motor strength. This was categorized as follows: (a) able to catheterize, (b) possibly able to catheterize, (c) able to catheterize only with reconstructive surgical intervention (e.g., catheterizable stoma construction or tendon transfer surgery) and (d) unable to catheterize even with reconstructive surgical intervention. Our algorithm for classifying the ability to perform CIC is shown in Figure 1.

Algorithm for the ability to self-catheterize based on UE motor strength scores.
Patients were excluded from the study if a motor examination was not recorded before discharge or if a patient was younger than 13 years of age. Cross-sectional associations among demographic characteristics, health characteristics and bladder management methods were tested using the χ2 test. All data manipulation and statistics were performed using Stata version 12.1 (StataCorp, College Station, TX, USA).
Results
Form I data were available for 5018 patients in the NSCID for the years 2006 to 2012. After exclusions, a total of 4481 patients were evaluated, including 1016 (22.7%) patients who were able to volitionally void and 3465 (77.3%) patients who were unable to volitionally void. Demographic characteristics and overall SCI levels were similar between all patients and the subgroup of patients who were unable to volitionally void at discharge (Table 1). A significant difference in bladder management at the time of discharge was noted on the basis of American Spinal Injury Association Impairment Scale. Greater than 85% of patients able to void volitionally at discharge were classified as American Spinal Injury Association Impairment Scale D, whereas <20% of patients who were discharged with a non-volitional bladder management were classified as American Spinal Injury Association Impairment Scale D (P<0.001).
The bladder management of patients unable to volitionally void at the time of discharge from rehabilitation is shown in Table 2. The percentage of individuals whose bladder was managed with an indwelling catheter was higher in women compared with that in men (42.9% vs 29.3%, P<0.001), whereas the percentage of individuals whose bladder was managed with CIC was lower in women compared with that in men (49.5% vs 61.5%, P<0.001). For patients who were unable to volitionally void, CIC (59.2%) was more commonly used compared with indwelling catheterization (31.9%) or condom catheterization (2.5%).
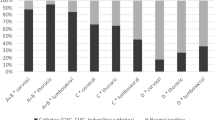
On the basis of our assessment of an individual’s UE function, patients who were discharged performing CIC were more likely to have adequate UE function to self-catheterize compared with those discharged with an indwelling catheter (72.0% vs 33.4%, P<0.001) (Table 3). It is notable, however, that of patients discharged with an indwelling catheter more than one-third had adequate UE function for CIC, with an additional 17.1% possibly able to perform CIC and another 6.4% potentially able to catheterize with surgical intervention. Thus, a total of 56.9% of patients discharged with an indwelling catheter had UE function that did not preclude bladder management with CIC. Conversely, in the group performing CIC at discharge, 14.1% had inadequate UE function for self-catheterization and another 3% would be unable to self-catheterize without surgical intervention.
Among all patients who could not volitionally void at discharge from rehabilitation, 58.8% were able to catheterize by our UE function criteria alone, 12.9% were possibly able to catheterize and 4.3% would be able to catheterize with surgical assistance. Only 23.3% of these patients would be completely unable to independently perform CIC on the basis of UE function criteria.
BMI and gender were also evaluated as potential barriers to CIC. Among SCI patients who could not volitionally void, 22.6% were classified as obese, morbidly obese or super obese. Female patients were more likely to be obese (BMI 30 kg m−2 or more) compared with male patients (30.5% vs 20.7%, P<0.001) (Table 4). BMI appeared to have a significant impact on bladder management at discharge. In women with BMI >25 kg m−2 (overweight, obese or morbidly/super obese), the rate of CIC bladder management decreased significantly, and the rate of IC bladder management increased significantly (P<0.001 for both). In men, increases in BMI had no significant association with the choice of bladder management at hospital discharge. In addition, there was no statistical difference in the UE function between males and females or among different classifications of BMI (P>0.05 for all groups) (data not shown).
In a 'best-case' scenario among SCI patients who could not volitionally void at the time of discharge and based on our algorithm were classified as able, possibly able or only able to catheterize with surgical assistance, ~76% had the UE function to potentially perform CIC given appropriate patient motivation, an adequate home support system and prosthetic or surgical assistance (i.e. tenodesis aids, tendon transfer, construction of catheterizable stoma). Conversely, in a 'worst-case' scenario assuming all females, all obese or morbidly/super obese males and anyone with non-optimal hand function (possibly able to catheterize or able to catheterize only with surgical assistance) could not catheterize independently, only ~38% of SCI patients could potentially perform CIC.
Discussion
Although CIC is widely accepted as the bladder management method with lowest long-term morbidity, the fact that up to 50% of patients abandon its use within 5 years of follow-up suggests that investigation must be carried out to understand why this occurs. On the basis of previous data, inadequate UE function is a significant barrier to a patient’s adopting of CIC8 and might have a prominent role in this 'dropout'. In our study, 58.8% of SCI patients who are unable to volitionally void possess the UE function adequate enough to independently perform CIC, whereas 23.3% lack the UE function to self-catheterize. These rates are similar to the actual bladder management at discharge from rehabilitation for these patients (59% CIC, 32% indwelling catheter). It is notable, however, that our UE function algorithm proposes that up to 14% of patients discharged home with CIC for bladder management are likely unable to self-catheterize and another 3% would require surgical intervention to successfully self-catheterize. This suggests that CIC 'dropout' may be, in part, because of a patient’s physical inability to independently perform self-catheterization. These UE function data also suggest that the percentage of patients discharged with an indwelling catheter for bladder management has the potential to be decreased, as >33% of these patients have adequate UE function to perform CIC and another 23% are possibly able or able with surgical assistance.
Although the UE function was similar in male and female SCI patients, the 10% difference in CIC and IC rates between the groups suggests that anatomic issues also affect the adoption of CIC. Our subanalysis suggests that BMI may further have a role in this difference, as significantly more female SCI patients were classified as obese or morbidly/super obese as compared with males. Although an increase in BMI does not significantly affect CIC adoption in men, women were significantly affected once their BMI exceeded 25 kg m−2.
This study was also intended to help quantify a reasonable proportion of SCI patients who could be discharged on CIC. On the basis of the UE function alone, our results suggest that a number approaching 60% is reasonable. However, with more effective intervention, this number could be increased to 75%. Prior studies have suggested that modalities such as occupational therapy training, hand-grip aids, tendon transfer surgery and catheterizable stoma construction are effective9, 10, 11, 12, 13 but often underutilized.14 Importantly, the UE function is not the only barrier patients have to the adoption of CIC. Anatomic considerations (gender, BMI),2, 13 uncontrolled incontinence15 and cognitive impairment following concomitant brain injury16 may also affect the adoption and continuance of CIC. Thus, increased attention to these areas is necessary.
Our findings and conclusions can be criticized from the perspective that a standard algorithm for the UE function necessary to perform self-catheterization has not been previously constructed nor tested. Thus, we mainly rely on expert opinion for our categorization scheme. However, the reported CIC rates in a recent small case series compared favorably with our algorithm (C4—unable to do CIC, C5—36.4% CIC, C6—66.7% CIC and C7—85.7% CIC).17
The NCSID does not contain data for several characteristics that influence the choice of the bladder management method, including uncontrolled urinary incontinence, patient motivation, adequate home support system and comprehensive brain injury data that could affect one’s cognitive ability to independently perform CIC. The NCSID also cannot account for varying institutional policies regarding the engagement and motivation of patients to perform CIC, which might provide alternative reasons for discharge of patients with adequate UE motor function on a bladder management other than CIC. Finally, longitudinal follow-up of patients to assess whether a poor UE function is indeed a risk factor for CIC 'dropout' has not yet been performed.
Despite these limitations, our study is the first to comprehensively evaluate the UE motor function and its relation to bladder management in the SCI population. This study is further strengthened by a large number of patients and includes data from complete and standardized motor strength exams. As the NCSID encompasses ~15% of the SCI population of the United States, the study sample is also highly representative.1
Conclusion
CIC dropout may occur at least, in part, because of inadequate UE motor function. Future follow-up will be needed to further validate this concept. In a 'best-case' scenario, ~76% of SCI patients who cannot volitionally void could potentially perform CIC given appropriate assistance.
DATA ARCHIVING
There were no data to deposit.
References
Spinal cord injury facts and figures at a glance. J Spinal Cord Med 2013; 36: 170–171.
Cameron AP, Wallner LP, Tate DG, Sarma AV, Rodriguez GM, Clemens JQ . Bladder management after spinal cord injury in the United States 1972 to 2005. J Urol 2010; 184: 213–217.
Lapides J, Diokno AC, Silber SJ, Lowe BS . Clean, intermittent self-catheterization in the treatment of urinary tract disease. J Urol 1972; 107: 458–461.
Ord J, Lunn D, Reynard J . Bladder management and risk of bladder stone formation in spinal cord injured patients. J Urol 2003; 170: 1734–1737.
Weld KJ, Dmochowski RR . Effect of bladder management on urological complications in spinal cord injured patients. J Urol 2000; 163: 768–772.
Bennett CJ, Young MN, Adkins RH, Diaz F . Comparison of bladder management complication outcomes in female spinal cord injury patients. J Urol 1995; 153: 1458–1460.
Spinal Cord Injury Information Network. National Spinal Cord Injury Database. Available at: http://www.spinalcord.uab.edu/show.asp?durki=24480 Accessed on 26 August 2015.
Yilmaz B, Akkoc Y, Alaca R, Erhan B, Gunduz B, Yildiz N et al. Intermittent catheterization in patients with traumatic spinal cord injury: obstacles, worries, level of satisfaction. Spinal cord 2014; 52: 826–830.
Adler US, Kirshblum SC . A new assistive device for intermittent self-catheterization in men with tetraplegia. J Spinal Cord Med 2003; 26: 155–158.
Bernuz B, Guinet A, Rech C, Hugeron C, Even-Schneider A, Denys P et al. Self-catheterization acquisition after hand reanimation protocols in C5–C7 tetraplegic patients. Spinal Cord 2011; 49: 313–317.
Gregersen H, Lybaek M, Johannesen IL, Leicht P, Nissen UV, Biering-Sorensen F . Satisfaction with upper extremity surgery in individuals with tetraplegia. J Spinal Cord Med 2014; 38: 161–169.
Hakenberg OW, Ebermayer J, Manseck A, Wirth MP . Application of the Mitrofanoff principle for intermittent self-catheterization in quadriplegic patients. Urology 2001; 58: 38–42.
Walsh K, Troxel SA, Stone AR . An assessment of the use of a continent catheterizable stoma in female tetraplegics. BJU Int 2004; 94: 595–597.
Bryden AM, Wuolle KS, Murray PK, Peckham PH . Perceived outcomes and utilization of upper extremity surgical reconstruction in individuals with tetraplegia at model spinal cord injury systems. Spinal Cord 2004; 42: 169–176.
Afsar SI, Yemisci OU, Cosar SN, Cetin N . Compliance with clean intermittent catheterization in spinal cord injury patients: a long-term follow-up study. Spinal Cord 2013; 51: 645–649.
Seth JH, Haslam C, Panicker JN . Ensuring patient adherence to clean intermittent self-catheterization. Patient Prefer Adher 2014; 8: 191–198.
Kriz J, Relichova Z . Intermittent self-catheterization in tetraplegic patients: a 6-year experience gained in the spinal cord unit in Prague. Spinal Cord 2014; 52: 163–166.
Acknowledgements
This work was supported, in part, by Grant No. H133A110002 from the National Institute on Disability and Rehabilitation Research, Office of Special Education and Rehabilitation Services, United States Department of Education, Washington DC. The authors certify that all applicable institutional and governmental regulations concerning the ethical use of human volunteers were followed during the course of this research.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Zlatev, D., Shem, K. & Elliott, C. How many spinal cord injury patients can catheterize their own bladder? The epidemiology of upper extremity function as it affects bladder management. Spinal Cord 54, 287–291 (2016). https://doi.org/10.1038/sc.2015.169
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2015.169
This article is cited by
-
Sex differences in urological management during spinal cord injury rehabilitation: results from a prospective multicenter longitudinal cohort study
Spinal Cord (2023)
-
Preoperative occupational therapy in children with neurogenic bladder: improving independence with bladder management and self-catheterization
Current Bladder Dysfunction Reports (2022)
-
Intermittent catheterisation for individuals with disability related to spinal cord injury in Tanzania
Spinal Cord Series and Cases (2020)
-
Volitional Voiding After Spinal Cord Injury—Who Will and Who Will Not
Current Bladder Dysfunction Reports (2017)
