
Abstract
Study design:
Retrospective study.
Objectives:
To determine the demographic and clinical characteristics of patients with cervical spinal cord injury (CSCI) admitted to a single Center.
Setting:
Turkish Armed Forces Rehabilitation Center, Ankara, Turkey.
Methods:
The medical records of all patients with spinal cord injury admitted from January 2009 to December 2013 were screened. Variables of each patient with cervical injury (CSCI), such as age at the time of injury, gender, etiology, degree and level of neurological impairment, associated injuries, surgical stabilization and length of rehabilitation stay (LOS), were analyzed.
Results:
In all, there were 804 patients with traumatic spinal cord injury (SCI) during the 5-year study period, of which 562 (69.9%) were paraplegic and the remaining 242 (30.1%) had a CSCI (C1–C8) and were included in the study. Among the CSCI patients, 80.6% were male (male:female ratio is 4.15:1), mean age at the time of injury was 32.58±14.71 years (range: 4–79 years), the largest age group was 16–30 years (n=117, 48.3%), followed by 31–45 years (n=70, 28.9%). Motor vehicle accident (MVA) was the most common cause of injury (49.2%), followed by falls (21.5%) and diving accidents (18.2%). Low CSCI (C5–8; 61.2%) and incomplete injury (55%) occured more often than high CSCI (C1–4) and complete injury. In total, 202 (83.5%) patients underwent surgical stabilization. Thirty-seven (15.3%) had associated injuries.
Conclusion:
The present findings show that most of the CSCI patients were aged 16–30 years. In addition, based on the frequency of the causes of injuries we think that prevention efforts should mainly focus on MVA, falls and diving accidents.
Similar content being viewed by others
Introduction
Cervical spinal cord injury (CSCI) is often more debilitating and with more catastrophic consequences if compared with other SCIs. The most devastating aspects of CSCI are represented by impairment of upper extremity function that is very important for independence in daily life1 and an increased risk of respiratory failure2 that can be severe and life threatening. These impairments, which require intensive care,3 are strongly associated with morbidity and mortality.1, 4, 5 CSCI constitutes a great clinical challenge for patients, as well as their families and rehabilitation team—the treatment and management of which is extremely expensive.3, 4, 6
As CSCI results in life-long severe disability, it is crucial to identify its clinical characteristics in order to improve prevention and treatment strategies. The present study aimed to determine the demographic and clinical characteristics of CSCI patients admitted to the Turkish Armed Forces (TAF) Rehabilitation Center and to provide a contribution to the guidance for the implementation of preventive measures.
Materials and methods
The study protocol was approved by the Gülhane Military Medical Academy Ethics Committee. The medical records of all patients with SCI admitted to the TAF Rehabilitation Center, Ankara, Turkey, during a 5-year period (2009–2013) were reviewed. TAF Rehabilitation Center is the leading institution offering primary comprehensive rehabilitation for patients with SCI in Turkey.
Demographic and clinical data for each patient with CSCI, including age at the time of injury, gender, etiology, degree and level of neurological impairment, associated injuries, surgical stabilization of the cervical spine and length of rehabilitation stay (LOS), were analysed.
Causes of injury were grouped as motor vehicle accident (MVA) that included pedestrians hit by a vehicle, falls, that included both simple falls (from ground level) and falls from a height, gunshot injury, violence, fall of weight, diving and sports injuries. The extent of injury was classified based on the ASIA-ISCoS International Standard of Neurological Classification of Spinal Cord Injury.7 Patients were divided into two groups based on the neurologic level of injury: high (C1–4) tetraplegia and low (C5–C8) tetraplegia. They were also divided into six age groups based on age at the time of injury, as follows: 0–15, 16–30, 31–45, 46–60, 61–75 and ⩾76 years.
Statistical analysis was performed using SPSS v.15.0 for Windows (SPSS Inc., Chicago, IL, USA). Continuous variables are presented as mean±s.d. and range (min.–max.), and categorical variables are shown as frequency and percentage. Descriptive statistics were used to analyze the demographic characteristics. Categorical variables were analyzed using the χ2 test. The normality of the distribution of numeric variables was examined using the Kolmogorov–Smirnov test. Differences between groups were determined via the Mann–Whitney U-test for two groups and the Kruskal–Wallis for ⩾3 groups because of the non-normal distribution of data. Multiple linear regression analysis was used to identify independent predictors of LOS. The level of statistical significance was set at P<0.05.
Results
In all, 804 patients with traumatic SCI admitted during the 5-year study period (January 2009–December 2013) were identified, of which 562 (69.9%) were paraplegic and 242 (30.1%) had a CSCI (C1–C8). These last were included in the study. Among the CSCI patients, 80.6% were male and 19.4% were female (male:female ratio is 4.15:1).
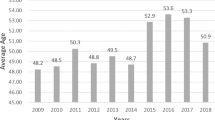
The mean age at the time of injury was 32.58±14.71 years (range: 4–79 years). The mean age of the male patients (31.94±13.98 years) was lower than that of the female patients (35.26±17.28 years); however, the difference was not significant (P=0.281). As shown in Figure 1, most of the patients were aged 16–30 years (n=117, 48.3%) at the time of injury, followed by the group of 31–45 years (n=70, 28.9%). There was a significant difference in the age group between the sexes (P=0.029); however, the mean age was similar in both groups (P=0.281) (Table 1).

Age distribution of patients with cervical spinal cord injury.
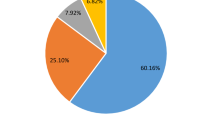
The most common cause of CSCI was MVA (49.2%), followed by falls (21.5%) and diving accidents (18.2%). In all the age groups, except the ⩾76-year group, MVA was the predominant cause of injury. A significant difference in etiology was observed among the age groups (P<0.001). The majority of falls were falls from a height (76.9%). Simple fall-related CSCI was more common in those aged ⩾46 years at the time of injury (83.3%). The rate of falls among male and female patients was roughly equal. Diving accident-related CSCIs were most common (79.5%) in the 16- to 30-year group and in male patients (95.5%).
There was a significant difference in CSCI etiology between the male and female patients (P=0.004). Distribution of CSCI patient characteristics according to etiology is shown in Table 2.
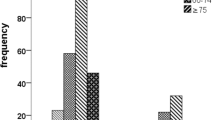
The level of CSCI exhibited bimodal distribution, with a peak at C4 (35.1%), and a second smaller peak at C5 (27.7%) (Figure 2). In terms of the severity of injury, 109 (45%) patients had complete tetraplegia, and 133 (55%) had incomplete tetraplegia. When compared with low CSCI patients, high CSCI patients were more likely to have complete lesion (54.3 versus 39.2%, P=0.022) (Table 3). The most common etiology in cases of complete lesion was MVA (44%), followed by diving accident (21.1%), and fall from a height (19.3%).

Injury level distribution of patients with cervical spinal cord injury.
Complete injury was most common in the 16- to 30-year group. Complete injury was more common than incomplete injury in patients with C4 CSCI (Table 4). There were no any differences in the level or severity of injury based on etiology (P>0.05).
Of all the patients, 16 (6.6%) had ⩾1 upper or lower extremity fractures, 11 (4.5%) had a thoracic injury, 7 (3.1%) had a head injury including skull fracture, intracranial hemorrhage and brain contusion, 1 (0.4%) had an amputation and 2 (0.8%) had other injuries (aortic injury and splenic rupture).
Surgical stabilization of the spine was performed in most of the patients (83.5%). Such treatment was adopted at the highest in diving accident (95.5%), with no statistical difference between low and high CSCIs.
The mean LOS was 66.78±52.65 days. The only variable that strongly predicted longer LOS via multiple linear regression analysis was high CSCI (P=0.008) (Table 5).
Discussion
To the best of our knowledge, the present study is one of the largest on patients with CSCI and is the first to focus on these unique patients in Turkey. We think that the present findings may provide a comprehensive picture of Turkish CSCI patients because the TAF Rehabilitation Center treats SCI patients from all regions of Turkey.
The proportion of tetraplegia
In earlier studies CSCIs have been reported to represent a wide range of percentage among the total SCIs. In our study, they accounted for 30.1% of the total SCI, and this percentage is lower than that reported in developed countries (41.6–75%).3, 8, 9, 10, 11 Such low percentage is similar to that reported in earlier studies performed in Turkey and other developing countries (4.8–47.2%).8, 12, 13, 14, 15 It has been reported that the incidence of tetraplegia increases with age, being more frequent in individuals aged ⩾60.3, 9, 10, 16 The geriatric age group (aged ⩾65 years) currently accounts for only 7.7% of the total population in Turkey (http://www.tuik.gov.tr/). The TAF Rehabilitation Center does not admit CSCI patients with serious pressure sores or respiratory failure, including patients with tracheostomy or ventilator dependence. The low percentage of CSCI patients in the present study might have been associated both with the TAF Rehabilitation Center admission policy and the relatively small elderly population in Turkey.
Age
Traumatic SCI has been previously reported to have a bimodal distribution, with a peak age-specific incidence involving young adults, and a second smaller peak in the older population.10, 11 In the present study the mean age at the time of CSCI was similar to that reported by Frielingsdorf and Dunn4 (34.6 years). Our findings show that fewer children and old individuals had CSCI compared with other age groups. Pickett et al.11 and Fredø et al.17 reported that the incidence of patients aged >60 years with CSCI was 26.5% and 54.5%, respectively, which are much higher than that observed in the present study (6.2%).
Gender distribution
Previous studies reported that males have a much higher risk of traumatic SCI than females.4, 8, 9, 12, 13 In the present study CSCI in males was almost four times higher than in females, which is consistent with other studies conducted in Turkey.12, 13 Across all age groups, the male:female ratio was the lowest in the 0- to 15-year group (1.2:1) and in patients aged 60 years (1.5:1); conversely, the 16- to 30-year group had the highest male:female ratio (5.9:1). For all causes of injury male patients outnumbered female patients, and the male:female ratios were as follows: diving accident: 21:1; falls: 4.2:1; MVA: 2.4:1.
Etiology
MVA and falls combined have been reported to be most frequent etiology in CSCI,4, 5, 11 as it was observed in the present study, in which the most frequent etiology was MVA (49.2%). Although MVA-related CSCI was more common in males than in females (70.6% versus 29.4%), they represent the most frequent cause of injury involving female individuals (74.5% versus 43.1%). We think that these findings are related to Turkey’s sociocultural structure. Most of the females are housewives or they are employed in relatively less dangerous jobs and their participation in high-risk activities is lower than those of men. Therefore, females are less prone to non-MVA-related SCI. Falls were the second most frequent etiology of CSCI in the present study (21.5%), and falls from a height predominated (77%). Patients with fall-related injuries tended to be older.10, 17 Simple fall-related CSCI accounted for 5% of all cases, a relatively low percentage that was consistent with the number of patients aged 60 years.
The third most common cause of CSCI was diving into shallow water, which is not surprising in consideration of Turkey’s extensive shoreline. Thompson et al.18 reported that diving-related CSCI accounted for only 3.1% of all causes of injury, but that diving accidents was associated the highest risk of CSCI. An earlier study performed at the TAF Rehabilitation Center indicated that diving-related CSCI accounted for 13.8% of all CSCI cases between 2000 and 2007,14 which is lower than the 18.2% observed in the present study that was conducted between 2010 and 2013, showing an increase in the incidence of diving accident-related CSCI. This indicates to us that there is a lack of diving safety educational programming.
Level and severity of injury
The majority of the CSCI patients in the present study sustained low CSCI; however, the low/high CSCI ratio (1.57:1) was lower than that reported by Lenehan et al.10 and Gur et al.15 (3.33:1 and 3.93:1, respectively). The most common neurological level in the present study was C4 (35.1%), followed by C5 (27.7%), which is in contrast to earlier findings that reported C5 and C6 to be the most common neurological levels.4, 12, 13, 14, 15, 16 The most common cause of C4 injury in the present study was MVA (47%), followed by diving accident (17.6%), and C4 injury was the most common injury associated with diving accidents (34%). The higher rate of C4 injury observed in the present study might be attributable to the higher incidence of MVA- and diving accident-related injuries collected in our study.
Incomplete CSCIs have been reported to occur more often than complete CSCI.6, 10, 17 Our finding was in line with these studies. It has also been reported that the percentage of incomplete CSCI is increasing, compared with complete CSCI.6 With regards to the mechanisms of injury in our study, complete lesions were most commonly caused by MVAs; however, gunshot wounds were associated with the highest rate of complete injury (76.9%), followed by falls from a height (52.5%) and diving accidents (52.3%). The findings indicate that these three causes were responsible for 40% of all CSCIs.
Surgical spine stabilization
Only a small part (6.5%) of the CSCI patients were treated conservatively. Frielingsdorf and Dunn4 reported that 70% of the patients underwent surgical stabilization. Lenehan et al.10 reported that the proportion of traumatic SCI patients treated surgically increased from 61.8% in 1995 to 86.4% in 2004, and that the percentage of patients treated conservatively increases with age, which is consistent with our findings, as the surgical stabilization rate was lower in the CSCI patients aged >60 years (66.7%) than in those aged <60.
Associated injuries
In the present study, only 37 (15.3%) patients presented with associated injuries, of which fracture of the upper or lower extremities predominated, which is in agreement with Frielingsdorf and Dunn’s findings.4 Head injuries are associated with an increased risk of cervical spine injury;5, 19 however, they occurred in a small percentage in this study.
Length of rehabilitation stay
Pickett et al.11 reported that LOS was strongly associated with both the level and severity of SCI. In the present study multiple linear regression analysis showed that only high CSCI increased LOS, accounting ~2 weeks longer than those with low CSCI. A longer LOS can be expected in complete lesions. However, LOS for incomplete lesions was not significantly different from the complete lesions. These are often the patients who appear to have significant recovery over longer periods of rehabilitation.
The limitations of this study are mainly represented by its retrospective design that cause missing of data, and by the inclusion of only patients admitted to an inpatient rehabilitation center. Another limitation to consider is the TAF Rehabilitation Center admission criteria for patients with CSCI (mentioned earlier).
Conclusion
On the basis of the present findings, the number of CSCI patients varied by age at the time of injury; most were aged 16–45 years and their number progressively decreased with age. A male predominance among the patients was observed and MVA was the most frequent cause of injury. The use of helmet for motorcyclists and seat belt should be encouraged in the society. The lectures on prevention of injury to groups such as school children should be commonly performed to elicit public awareness. Diving accidents are associated with a high rate of CSCI, and based on the present findings diving safety educational programming is essential for reducing the incidence of diving-related CSCI in Turkey. Lastly, we think that more studies on SCI need to focus on CSCI, which is one of the most devastating chronic disorder.
Data Archiving
There were no data to deposit.
References
Snoek GJ, IJzerman MJ, Hermens HJ, Maxwell D, Biering-Sorensen F . Survey of the needs of patients with spinal cord injury: impact and priority for improvement in hand function in tetraplegics. Spinal Cord 2004; 42: 526–532.
Branco BC, Plurad D, Green DJ, Inaba K, Lam L, Cestero R et al. Incidence and clinical predictors for tracheostomy after cervical spinal cord injury: a National Trauma Databank review. J Trauma 2011; 70: 111–115.
Wyndaele M, Wyndaele JJ . Incidence, prevalence and epidemiology of spinal cord injury: what learns a worldwide literature survey? Spinal Cord 2006; 44: 523–529.
Fielingsdorf K, Dunn RN . Cervical spine injury outcome—a review of 101 cases treated in a tertiary referral unit. S Afr Med J 2007; 97: 203–207.
Clayton JL, Harris MB, Weintraub SL, Marr AB, Timmer J, Stuke LE et al. Risk factors for cervical spine injury. Injury 2012; 43: 431–435.
Spinal cord injury facts and figures at a glance. J Spinal Cord Med 2013; 36: 715–716.
Chiu WT, Lin HC, Lam C, Chu SF, Chiang YH, Tsai SH . Review paper: epidemiology of traumatic spinal cord injury: comparisons between developed and developing countries. Asia Pac J Public Health 2010; 22: 9–18.
Sabre L, Hagen EM, Rekand T, Asser T, Kõrv J . Traumatic spinal cord injury in two European countries: why the differences? Eur J Neurol 2013; 20: 293–299.
Lenehan B, Street J, Kwon BK, Noonan V, Zhang H, Fisher CG et al. The epidemiology of traumatic spinal cord injury in British Columbia, Canada. Spine (Phila Pa 1976) 2012; 37: 321–329.
Pickett GE, Campos-Benitez M, Keller JL, Duggal N . Epidemiology of traumatic spinal cord injury in Canada. Spine (Phila Pa 1976) 2006; 31: 799–805.
Karacan I, Koyuncu H, Pekel O, Sümbüloglu G, Kirnap M, Dursun H et al. Traumatic spinal cord injuries in Turkey: a nation-wide epidemiological study. Spinal Cord 2000; 38: 697–701.
Karamehmetoğlu SS, Nas K, Karacan I, Sarac AJ, Koyuncu H, Ataoğlu S et al. Traumatic spinal cord injuries in southeast Turkey: an epidemiological study. Spinal Cord 1997; 35: 531–533.
Tuğcu I, Tok F, Yılmaz B, Göktepe AS, Alaca R, Yazıcıoğlu K et al. Epidemiologic data of the patients with spinal cord injury: seven years' experience of a single center. Ulus Travma Acil Cerrahi Derg 2011; 17: 533–538.
Gur A, Kemaloglu MS, Cevik R, Sarac AJ, Nas K, Kapukaya A et al. Characteristics of traumatic spinal cord injuries in south-eastern Anatolia, Turkey: a comparative approach to 10 years' experience. Int J Rehabil Res 2005; 28: 57–62.
Feng HY, Ning GZ, Feng SQ, Yu TQ, Zhou HX . Epidemiological profile of 239 traumatic spinal cord injury cases over a period of 12 years in Tianjin, China. J Spinal Cord Med 2011; 34: 388–394.
Fredø HL, Rizvi SA, Lied B, Rønning P, Helseth E . The epidemiology of traumatic cervical spine fractures: a prospective population study from Norway. Scand J Trauma Resusc Emerg Med 2012; 20: 85.
Thompson WL, Stiell IG, Clement CM, Brison RJ, Canadian C-Spine Rule Study Group. Association of injury mechanism with the risk of cervical spine fractures. CJEM 2009; 11: 14–22.
Leucht P, Fischer K, Muhr G, Mueller EJ . Epidemiology of traumatic spine fractures. Injury 2009; 40: 166–172.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Disclaimer
There are no funding or grants or equipment provided for the project from any source, financial benefits to the authors and it is not published in any form of presentation previously.
Rights and permissions
About this article

Cite this article
Güzelküçük, Ü., Kesikburun, S., Demir, Y. et al. Demographic and clinical characteristics of patients with traumatic cervical spinal cord injury: a Turkish hospital-based study. Spinal Cord 53, 441–445 (2015). https://doi.org/10.1038/sc.2014.211
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2014.211
This article is cited by
-
Epidemiological characteristics of spinal cord injury in Northwest China: a single hospital-based study
Journal of Orthopaedic Surgery and Research (2020)
-
Transportation mode and timing of spinal cord decompression and stabilization in patients with traumatic spinal cord injury in Iran
Spinal Cord (2019)
-
Prevention of diving-induced spinal cord injuries—preliminary results of the first Romanian mass media prophylactic educational intervention
Spinal Cord Series and Cases (2017)
-
Spinal cord and spine trauma in a large teaching hospital in Ghana
Spinal Cord (2016)
