
Abstract
Study design
Hospital-based retrospective epidemiological research.
Objectives
To describe the epidemiological and demographic features of patients with traumatic cervical spinal cord injury in Chongqing, China from 2009 to 2018.
Setting
Army Military Medical University Xinqiao Hospital in Chongqing.
Methods
All patients diagnosed traumatic CSCI admitted to Xinqiao hospital from 2009 to 2018 were retrospectively reviewed. Data elements referred from the International SCI Core Data Set, included date of birth, date of injury, gender, etiology of injury, vertebral injury, associated injury, ventilatory assistance, and neurological status were collected.
Results
A total of 503 patients with TCSCI met the criteria. The mean age of patients with TCSCI was 50.3 ± 13.9 years (15–85 years), and the male-to-female ratio was 4.7:1. Fall (67.2%) was the leading cause of injury, followed by transport (22.3%). The most common neurologic level of injury (NLI) was C5, accounting for 38.2%. The number of AIS D was the largest, accounting for 42%.
Conclusions
The results indicated that TCSCI occurred most frequently in the middle age and fall was the leading cause of injury. The number of patients with TCSCI was larger in male than in female. The most common NLI occurred in C5, and AIS D had the largest numbers.
Similar content being viewed by others


Introduction
Traumatic cervical spinal cord injury (TCSCI) is a devastating and potentially life-threatening injury, which often causes severe disability and complications [1,2,3,4]. The incidence of spinal cord injury (SCI) is about 10.4–57.8 cases per million population in developed countries, and 12.7–29.7 cases per million population in developing countries [5,6,7]. 51–55% of SCIs occurred in the cervical spine [7,8,9]. China is the most populous developing country, and the number of CSCI is also large. It has led to medical and economic burden to families and the country [10]. So it is necessary to investigate the epidemiological characteristics of CSCI and to improve prevention strategies [7, 10].
Patients with TCSCI often require longer hospital stays, more medical cost and are at risk of death due to various complications [8, 11, 12]. The requirement of endotracheal intubation, tracheostomy, or mechanical ventilation is also more common in patients with TCSCI than in the thoracic or lumbar SCI [1, 13,14,15]. There have been epidemiological studies on SCI in Tianjin, Guangdong and Shanghai [12, 16, 17]. These epidemiological researches in China make the basis for undertaking the study. Chongqing has a total population of about 31,243,200 (2019), as one of the four municipalities in China. However, there are few epidemiological studies on TCSCI in Chongqing [11, 18]. We conducted a 10-year retrospective study to investigate the epidemiological profiles of TCSCI in Chongqing, which hopefully improve appropriate preventive strategies. This is the first epidemiological study on Chongqing, based on International SCI Core Data Set (version 2.0).
Methods
Participants
Xinqiao hospital is the tertiary referral centers for acute SCI in Chongqing, located in the southwest of China. Retrospective analysis was performed on 503 patients with TCSCI admitted in orthopedics department of Xinqiao hospital from January 2009 to December 2018. All procedures used in this research were approved by the Ethics Committee of the Army Military Medical University. Clinical data were screened from the medical record system according to the International Classification of Diseases (ICD-10) diagnostic code S14 [19]. Exclusion criteria were patients younger than 15 years old, cervical nerve root injury, incomplete medical record, or uncertain diagnosis of TCSCI.
Data collection
Demographic variables and epidemiological features were collected referred by International SCI Core Data Set (version 2.0) [20] as recommended by the International Spinal Cord Society (ISCoS), including date of birth, date of injury, gender, etiology of injury, vertebral injury, associated injury, ventilatory assistance, neurological level of injury (NLI), and American Spinal Injury Association (ASIA) impairment scale. The age was divided into five groups with the interval of 15 years: 15–29, 30–44, 45–59, 60–74, and 75+. Etiology of injury was categorized as sports and leisure, assault, transport, fall, and other traumatic cause. NLI was assessed by International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI) (2019 revision) [21]. ASIA impairment scale classification was divided into five grades: A, B, C, D, and E, based on sensory and motor examination on both sides of the body.
Statistical analysis
Continuous variables were recorded using mean ± standard deviation. Classification variables were converted to dichotomous variables using frequency and/or percentage records. Statistical analysis was performed using SPSS version 25.0 (SPSS, Chicago, IL) and Excel 2016(Microsoft, Redmond, WA).
Results
A total of 503 patients with TCSCI were discharged from hospital over the study period, 2010–2018. The average age at the time of injury was 50.3 ± 13.9 years (15–85 years). As shown in Fig. 1, the average age at the time of injury was relatively stable during the 10-year study, ranging from 45 to 55 years old. TCSCI usually occurred between 45 and 59 years old, accounting for 39.4%, followed by 30–44 years (132, 26.2%) and 60–74 years (120, 23.9%) (Table 1).

TCSCI usually occurred between 45–59 years old, followed by 30–44 years old.
TCSCI was most common in male (414, 82.3%), while 17.8% (89) were female. The male-to-female ratio was 4.7:1 (Table 1). As shown in Table 1, from 2009 to 2018, the number of males was generally far more than that of female, with a ratio ranging from 3:1 to 11.5:1. The occupations of patients with CSCI included industry workers (143, 28.4%), peasants (127, 25.2%), clerks (85, 16.9%), and the retired (72, 14.4%).
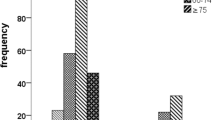
In general, fall was the leading cause of TCSCI, accounting for 67.2% (Table 1). Transport was the second leading cause of injury, accounting for 22.3%. As shown in Fig. 2, in the age group 30–44 years and 45–59 years, fall and transport were the leading cause of TCSCI, while no transport happened to those over 75 years old.

The age groups were divided into five categories and the etiology was indicated by different colors or patterns.
The number of AIS D at any level (211, 41.1%) was the largest, followed by C1–C4 AIS A–C (155, 30.8%). The distribution of ASIA grade was shown in Fig. 3A. The neurologic level of injury (NLI) in TCSCI showed a single peak distribution (Fig. 3B). NLI often occurred in the C5 segment, accounting for 38.2%, followed by C4 and C6.The number of NLI above C5 was 182, accounting for 36.2%. Among 503 TCSCI patients, 36.2% had a high cervical neurological lesion (C2–C4).

A Distribution histogram of ASIA scale in TCSCI patients. The number of AIS D was the largest. B Distribution histogram of the neurologic level of injury in TCSCI patients. Distribution histogram showed a single peak distribution, whichNLI often occurred in the C5 segment.
Among the 503 patients with TCSCI, 52.5% (264) suffered from vertebral injury, 12.5% (63) sustained associated injury as defined by ISCoS (Table 1). During hospitalization, 71 (14.1%) patients suffered respiratory failure, requiring mechanical ventilation (MV). Among them, 34 patients suffered mechanically ventilated pneumonia. There was electrolyte disturbance in 12 patients, hypoalbuminemia in 7, urinary infection in 5, and pressure injury in 2.
A univariate analysis was used to examine the differences between TCSCI patients with and without MV. Patients with AIS A (45.1% vs. 3.1%, p < 0.05) or NLI above C5 (67.6% vs. 31.9%, p < 0.05) were more likely to suffer from respiratory failure and to need MV. Age and sex had no correlation with requirement for MV (Table 2).
Discussion
There have been several research studies in different regions of China on the epidemiological features of SCI [11, 17, 18, 22, 23]. China is the largest developing country, and its rapid economic development has also brought changes in the epidemiology of SCI [12, 18]. International Spinal Cord Injury Data Sets was proposed by the ISCoS in order to gather data elements to enable worldwide SCI data and outcomes to be assessed and compared [20, 24, 25]. There are few epidemiological studies on SCI, especially TCSCI in Chongqing, China [18]. This is the first Hospital-based retrospective research standard by International SCI Core Data Set for TCSCI in Chongqing.
During the 10 years research, the average age at the time of injury has changed and shows a slight increasing trend from 48.4 years in 2009–2010 to 53.2 years in 2015–2016. TCSCI usually occurred between 45 and 59 years old in Chongqing. In Tianjin, China, the average age of TCSCI was 54 years and most injuries occurred in the 45–65-year between 2008 and 2012 [12]. The results were in accordance with our research. People in this age group bears the burden of the family and is the main force of labor in China. In previous studies, TSCI occurred mostly in male, about four times as many as in female [12, 26, 27]. In our research, the ratio was 4.7:1 in TCSCI, similar to previous conclusions. Ning [18] reported that the male/female ratio on SCI research was 4.33:1 in Chongqing from 2009 to 2013. Overall, men take on more high-risk jobs, while women take on less risky work, some of them are full-time homemakers in Chongqing.
In developed countries, transport was the leading cause of SCI, accounting for 30–50%, followed by fall [7, 28]. Zhou et al. [29] reported that in Tianjin, China, fall (55.1%), was the leading cause of SCI, followed by motor vehicle collisions (35.9%). In our research, fall (67.2%) was the leading cause of TCSCI, and transport (22.3%) was the second most common cause of injury. There are some reasons for this difference. Firstly, the number of cars per capita in developed countries is much higher than that in developing countries, and the probability of traffic accidents is correspondingly increased. Secondly, improvements in car safety, such as the use of airbags and seat belts, and harsh penalties for drunken driving, have reduced the incidence of traffic accidents [30, 31]. Thirdly, Chongqing city is mostly mountainous. The Yangtze River and Jialing River run through it, so there are many bridges and tall buildings here. The ups and downs of the terrain may increase the probability of falls [18].
According to our data, the most common NLI occurred in C5, followed by C4 and C6. Wu et al. [12] and Wang et al. [11] came to the same conclusion in a retrospective analysis of different regions. Thirty-six percent of TCSCI were above C5. As we all known, diaphragm is the most important breathing muscle, and the phrenic nerve, which supplies the movement of the diaphragm, is composed of the anterior branches of C3-5. Due to loss of diaphragm and/or intercostal muscle function, the higher and more complete the level of injury, the more serious the respiratory system will be damaged after CSCI [32, 33].
In a retrospective study, Lenehan et al. [6] and Sekhon and Fehlings [7] found that nearly half of SCI was complete (AIS A), followed by AIS D. However, in our conclusion, AIS D had the largest numbers, while AIS A was far less than AIS D. It is not difficult to find that the proportion of TCSCI caused by transport in developing countries is far lower than that in developed countries. Transport often causes complete SCI, which is more common in young people, while falls are more common in the elderly, and the injuries are mostly incomplete [7, 22, 34]. Xinqiao hospital is the tertiary referral centers for acute SCI in Chongqing. Part of severely injured patients with TCSCI do not have the opportunity to be transferred to our hospital, which may be another reason for the difference.
Nevertheless, there are several limitations in the current study. Firstly, it was a retrospective study. Epidemiological data like education level, ethnicity, length of hospital stay, data about rehab and so on were missing in the study. Secondly, this is a hospital-based descriptive research about TCSCI in Chongqing. China still needs to complete its database of SCI, compared with the well-established database in developed countries. Thirdly, because the number of deaths before hospitalization of TCSCI cannot be obtained, and part of patients refused to be treated and discharged home, this paper failed to further study of mortality.
Conclusion
This is a retrospective epidemiological study of TCSCI in Chongqing from 2009 to 2018. The results indicated that TCSCI occurred most frequently in the middle age and fall was the leading cause of injury. The number of patients with TCSCI was larger in male than in female. The most common NLI occurred in C5, and AIS D had the largest numbers. Preventive measures should be taken to reduce the occurrence of TCSCI based on the epidemiological features.
Data availability
The datasets generated during and analyzed during the current study are available from the corresponding author on reasonable request.
References
Leelapattana P, Fleming JC, Gurr KR, Bailey SI, Parry N, Bailey CS. Predicting the need for tracheostomy in patients with cervical spinal cord injury. J Trauma Acute Care Surg. 2012;73:880–4.
Beom JY, Seo HY. The need for early tracheostomy in patients with traumatic cervical cord injury. Clin Orthop Surg. 2018;10:191–6.
Yugue I, Okada S, Ueta T, Maeda T, Mori E, Kawano O, et al. Analysis of the risk factors for tracheostomy in traumatic cervical spinal cord injury. Spine. 2012;37:E1633–8.
Higashi T, Eguchi H, Wakayama Y, Sumi M, Saito T, Inaba Y. Analysis of the risk factors for tracheostomy and decannulation after traumatic cervical spinal cord injury in an aging population. Spinal Cord. 2019;57:843–9.
Perez K, Novoa AM, Santamarina-Rubio E, Narvaez Y, Arrufat V, Borrell C, et al. Incidence trends of traumatic spinal cord injury and traumatic brain injury in Spain, 2000-2009. Accid Anal Prev. 2012;46:37–44.
Lenehan B, Street J, Kwon BK, Noonan V, Zhang H, Fisher CG, et al. The epidemiology of traumatic spinal cord injury in British Columbia, Canada. Spine. 2012;37:321–9.
Sekhon LH, Fehlings MG. Epidemiology, demographics, and pathophysiology of acute spinal cord injury. Spine. 2001;26:S2–12.
Martin ND, Marks JA, Donohue J, Giordano C, Cohen MJ, Weinstein MS. The mortality inflection point for age and acute cervical spinal cord injury. J Trauma. 2011;71:380–5.
Kattail D, Furlan J, Fehlings M. Epidemiology and clinical outcomes of acute spine trauma and spinal cord injury: experience from a specialized spine trauma center in Canada in comparison with a large national registry. J Trauma. 2009;67:936–43.
Ibrahim A, Lee KY, Kanoo LL, Tan CH, Hamid MA, Hamedon NMA, et al. Epidemiology of Spinal Cord Injury in Hospital Kuala Lumpur. Spine. 2013;38:419–24.
Wang H, Xiang Q, Li C, Zhou Y. Epidemiology of traumatic cervical spinal fractures and risk factors for traumatic cervical spinal cord injury in China. J Spinal Disord Tech. 2013;26:E306–13.
Wu Q, Li YL, Ning GZ, Feng SQ, Chu TC, Li Y, et al. Epidemiology of traumatic cervical spinal cord injury in Tianjin, China. Spinal Cord. 2012;50:740–4.
Como JJ, Sutton ER, McCunn M, Dutton RP, Johnson SB, Aarabi B, et al. Characterizing the need for mechanical ventilation following cervical spinal cord injury with neurologic deficit. J Trauma. 2005;59:912–6.
Liebscher T, Niedeggen A, Estel B, Seidl RO. Airway complications in traumatic lower cervical spinal cord injury: a retrospective study. J Spinal Cord Med. 2015;38:607–14.
Yang XX, Huang ZQ, Li ZH, Ren DF, Tang JG. Risk factors and the surgery affection of respiratory complication and its mortality after acute traumatic cervical spinal cord injury. Medicine. 2017;96:e7887.
Yang R, Guo L, Huang L, Wang P, Tang Y, Ye J, et al. Epidemiological characteristics of traumatic spinal cord injury in Guangdong, China. Spine. 2017;42:E555–61.
Chang FS, Zhang Q, Sun M, Yu HJ, Hu LJ, Wu JH, et al. Epidemiological study of spinal cord injury individuals from halfway houses in Shanghai, China. J Spinal Cord Med. 2018;41:450–8.
Ning GZ, Mu ZP, Shangguan L, Tang Y, Li CQ, Zhang ZF, et al. Epidemiological features of traumatic spinal cord injury in Chongqing, China. J Spinal Cord Med. 2016;39:455–60.
Hirsch JA, Nicola G, McGinty G, Liu RW, Barr RM, Chittle MD, et al. ICD-10: history and context. AJNR Am J Neuroradiol. 2016;37:596–9.
Biering-Sorensen F, DeVivo MJ, Charlifue S, Chen Y, New PW, Noonan V, et al. International Spinal Cord Injury Core Data Set (version 2.0)-including standardization of reporting. Spinal Cord. 2017;55:759–64.
Kirshblum S, Snider B, Rupp R, Read MS, International Standards Committee of A, IscoS. Updates of the International Standards for Neurologic Classification of Spinal Cord Injury: 2015 and 2019. Phys Med Rehabil Clin N Am. 2020;31:319–30.
Feng H, Ning G, Feng S, Yu T, Zhou H. Epidemiological profile of 239 traumatic spinal cord injury cases over a period of 12 years in Tianjin, China. J Spinal Cord Med. 2011;34:388–94.
Ning G, Wu Q, Li Y, Feng S. Epidemiology of traumatic spinal cord injury in Asia: a systematic review. J Spinal Cord Med. 2012;35:229–39.
Liu N, Hu ZW, Zhou MW, Biering-Sorensen F. The practice of spinal cord injury core data collection among Chinese physicians: a survey-based study. Spinal Cord. 2015;53:658–62.
DeVivo M, Biering-Sorensen F, Charlifue S, Noonan V, Post M, Stripling T, et al. International Spinal Cord Injury Core Data Set. Spinal Cord. 2006;44:535–40.
Devivo MJ. Epidemiology of traumatic spinal cord injury: trends and future implications. Spinal Cord. 2012;50:365–72.
Halvorsen A, Pettersen AL, Nilsen SM, Halle KK, Schaanning EE, Rekand T. Epidemiology of traumatic spinal cord injury in Norway in 2012-2016: a registry-based cross-sectional study. Spinal Cord. 2019;57:331–8.
Pickett GE, Campos B, Mauricio, Keller JL, Duggal N. Epidemiology of traumatic spinal cord injury in Canada. Spine. 2006;31:799–805.
Zhou Y, Wang XB, Kan SL, Ning GZ, Li YL, Yang B, et al. Traumatic spinal cord injury in Tianjin, China: a single-center report of 354 cases. Spinal Cord. 2016;54:670–4.
Bárbara-Bataller E, Méndez-Suárez JL, Alemán-Sánchez C, Sánchez-Enríquez J, M. S-H. Change in the profile of traumatic spinal cord injury over 15 years in Spain. Scand J Trauma Resusc Emerg Med. 2018;26:27.
Smith E, Brosnan M, Comiskey C, Synnott K. Road collisions as a cause of traumatic spinal cord injury in ireland, 2001-2010. Top Spinal Cord Inj Rehabil. 2014;20:158–65.
Romero J, Vari A, Gambarrutta C, Oliviero A. Tracheostomy timing in traumatic spinal cord injury. Eur Spine J. 2009;18:1452–7.
Berney S, Bragge P, Granger C, Opdam H, Denehy L. The acute respiratory management of cervical spinal cord injury in the first 6 weeks after injury: a systematic review. Spinal Cord. 2011;49:17–29.
Smith E, Fitzpatrick P, Murtagh J, Lyons F, Morris S, Synnott K. Epidemiology of traumatic spinal cord injury in Ireland, 2010-2015. Neuroepidemiology. 2018;51:19–24.
Author information
Authors and Affiliations
Contributions
DS: This author helped to analyze and interpret the data, draft, and revise the paper. ZZ: This author helped to design the study, draft, and revise the paper, and approve the final paper.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Sun, D., Zhang, Z. Epidemiological characteristics of traumatic cervical spinal cord injury in Chongqing, China, from 2009 to 2018. Spinal Cord Ser Cases 7, 70 (2021). https://doi.org/10.1038/s41394-021-00434-1
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41394-021-00434-1
