
Abstract
Study Design:
Systematic literature review.
Objective:
The primary aim of this study was to evaluate interventions aimed at improving employment outcomes for individuals with spinal cord injuries (SCI).
Methods:
An electronic search of Medline/PubMed, EMBASE, Cochrane database, CINAHL, PsycINFO, Social Science Abstracts and Social Work Abstract databases was performed on 31 December 2013. To be included in the review, studies needed to investigate interventions among individuals with SCI where employment was an outcome. Exclusion criteria include (i) reviews, (ii) studies not published in English and (iii) non-peer reviewed publications.
Results:
Fourteen studies met the inclusion criteria, two were randomized controlled trials. The strongest evidence finds that supported employment can improve employment outcomes among individuals with SCI. The use of service dogs has also been shown to improve employment outcomes. The remaining 12 studies are observational and predominantly focus on vocational rehabilitation programs.
Conclusion:
There is a dearth of high-quality intervention research that targets employment outcomes in individuals with SCI. Consequently, conclusions are mostly based on evidence from observational studies. Vocational rehabilitation programs are the primary focus of this evidence, but conclusions may be confounded, as individuals may be self-selecting for these programs. Additional randomized trials on employment interventions are needed to overcome these limitations. Studies should aim to identify which components of these programs have the greatest influence on employment outcomes.
Similar content being viewed by others

Background
The International Classification of Functioning, Disability and Health (ICF) of the World Health Organization defines employment as ‘engaging in all aspects of work, as an occupation, trade, profession or other form of employment, for payment or where payment is not provided, as an employee, full or part time, or self-employed.’1 Gainful employment helps individuals achieve economic self-sufficiency, and is considered a source of personal growth,2 adjustment to disability,3 social integration, life satisfaction, and is associated with improved health and well-being.4, 5 As a result, employment is one of the most important psychosocial topics for individuals with spinal cord injuries (SCI).6
Research indicates high variability in employment rates after SCI as a result of differences in study design, sample characteristics such as the age, duration of injury, work experience prior to injury and differences in the definition of the concept of ‘employment’ itself.7 Nevertheless, systematic reviews indicate that approximately 35% of individuals with SCI are employed post injury.8, 9 Though it is not surprising that a catastrophic event such as a SCI would present an employment challenge, a considerable number of unemployed individuals have a desire to work, and judge themselves as able to do so.10
An individual’s employment status is the result of a complex interaction between personal, environmental and injury-related factors. A recent systematic review identified 32 factors associated with employment outcomes in individuals with SCI (Trenaman et al., submitted). The authors of that review categorized factors based on the World Health Organization’s International Classification of Functioning and Disability (ICF)1 which includes the domains of activity and participation, personal, environmental, body structures and function, and health condition. In addition, factors were subcategorized based on their modifiability, which is important because it ultimately determines how this information is used to improve employment outcomes in this population. Non-modifiable factors such as age, sex, race/ethnicity and severity of injury can help identify and focus resources on individuals who will face the greatest challenge in gaining employment. On the other hand, modifiable factors serve as the foundation for interventions, and can provide guidance for individuals developing programs where the primary (or secondary) goals are to improve employment outcomes for individuals with SCI.
The objectives of this review are to systematically evaluate the interventions that have been associated with employment outcomes in individuals with SCI, to contrast the findings against known modifiable and non-modifiable factors from the literature, and to identify factors that have been understudied to date as a means of informing future research in this area.
Methods
Eligibility criteria
To be included in the review, studies needed to (i) investigate interventions among individuals with SCI where employment was a primary or secondary outcome and (ii) have a sample comprised of individuals at least 18 years of age with a SCI, or have provided results specific to individuals with a SCI if a heterogeneous sample was used. Exclusion criteria include (i) reviews, (ii) studies not published in English and (ii) non-peer reviewed publications.
Information sources
Medline/PubMed, EMBASE, CINAHL, PsycINFO, Cochrane Database, Social Science Abstracts and Social Work Abstract databases were searched. No limits were applied on publication date.
Search strategy
The electronic search was undertaken on 31 December 2013. The following search terms were used:
(employment OR supported employment OR unemployment OR employment status OR employability OR employment disabled OR gainful employment OR self-employment OR part time employment OR temporary employment OR employee assistance OR employee assistance program OR vocation OR vocation assistance OR vocational rehabilitation OR vocational education OR work resumption OR workplace OR return to work OR work force OR labor force OR career assistance OR career OR job) AND (spinal cord injury OR paraplegia OR tetraplegia OR quadriplegia)
All publications were then entered into an electronic reference manager (RefWorks) where duplicates were removed. Additional papers were identified through hand-searching the reference list of included papers.
Study selection process
Review at the title level was undertaken independently by two reviewers, with relevant studies reviewed at the abstract and full-text level (LT, WCM). The authors identified papers for inclusion with full agreement (i.e., no discrepancies needed to be resolved through discussion).
Data collection process
Dataset was extracted by one reviewer (LT).
Data Items
For each study, the author(s), year of publication, country, study design, sample size, population, intervention and employment outcome were compiled.
Results
Study selection
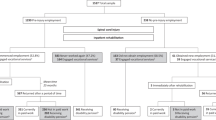
Fourteen studies met the inclusion criteria (see Figure 1). Studies were published between 1982 and 2012, with the majority from the United States (n=9). The remaining studies were from Taiwan (n=2), Australia (n=1), Canada (n=1) and India (n=1). There were two randomized trials and 12 observational studies. Table 1 summarizes the included studies. Most studies focused on vocational rehabilitation, with others on targeted social support, community integration, assistive technology, functional independence and psychological functioning (see Table 1).

PRISMA diagram of systematic review process.
One randomized controlled trial evaluated the use of trained service dogs for individuals with severe ambulatory disabilities, with employment as one of the main outcome measures.11 There were 48 participants, of whom 22 had SCI, randomized to the experimental group (service dog at 1 month) or to the control group (service dog at 13 months). At 12 months, 14 of 24 individuals in the experimental group were employed part-time, compared with 0 of 24 in the control group. At 24 months, where the experimental group had a service dog for the entire period and the control group for just 12 months, 23 of 24 individuals in the experimental group, and 17 of 24 in the control group were employed part-time. Notably, traditional vocational rehabilitation services were not part of the intervention.
The second randomized controlled trial evaluated a supported employment (SE) intervention in veterans with SCI.12 This trial included an intervention site with a group that received SE, a control group which received treatment as usual along with a control group at another site. It was found that individuals receiving SE were 2.5 times more likely to obtain competitive employment than individuals who received treatment as usual at the same site, and 11.4 times more likely than those in the control group at the other site. Intention to treat analysis revealed that individuals in the SE group earned significantly more per week than the treatment as usual-observational site group, but not the treatment as usual-intervention site group.
Observational analyses of vocational rehabilitation interventions have found that education, on-the-job training, job search assistance, job placement assistance, on-the-job support, maintenance services, assistive technology and ‘other services’ were correlated with gaining employment.13 Marini et al.14 evaluated components of vocational rehabilitation services in over 10 000 individuals and found that job placement assistance, on-the-job training, assistive technology and job finding services were significantly associated with a competitive employment. Jellineck and Harvey15 compared state vocational rehabilitation services to on-site professional counselors for vocational rehabilitation, and found that 4 individuals with SCI who used state vocational services were employed 3 years post discharge, compared with 15 in the group who had access to on-site counselors. Inge et al.16 followed three individuals and tailored vocational rehabilitation their needs; intervention intensity ranged from minor to intensive, and all three were able to gain employment.
King et al.17 evaluated an enhanced case management intervention, which included support while individuals returned to the community. After 1 year, 17% of individuals had returned to work (approximately equal to the rate from the National Spinal Cord Injury Statistical Center) while 32% had begun educational training (compared with 15%). Wang et al.18 evaluated a multi-faceted program, which aimed to improve psychosocial and physical functioning, while also including vocational training. The analysis was completed just as the 6-month intervention was finishing; no one in the intervention group was employed or attending school, whereas 20% (11 out of 55) in the control group were employed and one was attending school. Jang et al.19 performed an observational analysis of individuals who received vocational rehabilitation services compared with those who did not. They found that 50% of employed individuals had received vocational rehabilitation compared with 28% of unemployed individuals.
Hansen et al.20 investigated a program in India that focused on physical conditioning, vocational training and work placements, and found that 50% (23 out of 46) individuals had gained employment. A pilot study in Australia evaluated a program, which featured lifestyle support packages that aim to improve activities of daily living. No statistically significant difference in labor market participation was observed between individuals who had received support compared with those who had not. Phillips et al.21 evaluated a telerehabilitation intervention that focused on skin care, nutrition, bowel and bladder routines, psychosocial issues and equipment needs, and was delivered via video in one intervention group, audio in another, while the control group received usual care. Being in one of the two intervention groups trended toward a longer time until return to productive activities such as school, work or home-making though it was not significant (P=0.083). Lastly, Shem et al.22 evaluated a peer mentorship intervention and found that among those in the study, 7 (24%) participants returned to school, 2 (6.9%) participants returned to work and 1 (3.4%) participant returned to school part-time.
Discussion
In this systematic review, we have synthesized intervention studies from the SCI literature that have evaluated employment as an outcome. We found a profound lack of high-quality studies evaluating the influence of interventions on employment outcomes following SCI, despite the known importance of employment among individuals with SCI. Two randomized controlled trials have been completed, one involving social support with a guide dog and the other offering an enhanced supportive employment program, and both improved employment outcomes. The observational studies we reviewed provide additional evidence that supports targeting vocational rehabilitation and social support.
The majority of studies included in this review focused on vocational rehabilitation, which has the primary objective of improving employment outcomes. As identified in a review of factors associated with employment outcomes, vocational rehabilitation interventions have been identified as key in enabling return to work following SCI (Trenaman et al., submitted).8 If improving employment outcomes is the primary goal, vocational rehabilitation is the logical intervention to facilitate return to work.
The strongest evidence comes from a randomized trial of a SE intervention compared with conventional vocational rehabilitation. SE integrates members of the vocational rehabilitation team into the care continuum, allowing them to access and discuss care with other team members.23 It also promotes a more personalized experience, with support built around the preferences of the individual. Individuals receiving SE were 2.5 times more likely to gain employment than those receiving usual care at the site offering the intervention, and 11.4 times more likely than those receiving usual care at a site that did not.12 Study authors noted that at the site offering the SE intervention, there was an elevated awareness and attention to vocational issues, and that this translated into increased use of conventional vocational rehabilitation services among the control group. This highlights the positive impact that established vocational rehabilitation programs can have if they are adequately promoted and utilized, in addition to added benefit from greater integration and personalization of services.
The only other randomized trial found improved employment outcomes following the use of service dogs. Though this study adds evidence to how employment outcomes can be modified, the considerable cost and time associated with training and maintenance might preclude program planners from implementing a service dog program.
A previous systematic review identified education as the modifiable factor that was associated with the greatest increase in odds of employment (Trenaman et al., submitted). Four of the included studies focused on education as an outcome (in addition to employment).15, 17, 21, 22 Phillips et al.21 used a broader outcome definition called ‘productive activities’ that included both employment and education, whereas others investigated education on its own. Given that education may be an intermediate step to obtaining employment, it is a justifiable end point of studies investigating employment outcomes and may provide a better overall view of the employment prospects for those with SCI.
Many of the studies in our review either did not include a control group or failed to adequately specify the employment rate for comparison with those in the intervention group. In these cases, it is difficult, if not impossible, to determine the proportion of individuals returning to work that is directly attributable to the intervention. One study attempted to overcome this by comparing the rate of employment (and return to education) with figures from the National Spinal Cord Injury Statistical Center.17 Future studies should make a concerted effort to ensure that employment outcomes are adequately reported so evidence-based conclusions on effective return-to-work strategies can be drawn. Timing is also an important consideration when evaluating interventions. One study performed the analysis immediately after the individuals completed a vocation rehabilitation program; this meant that no information can be obtained whether or not those in the intervention group were employed or pursued education.18 Performing the evaluation at 6 months, 1 year (or even longer) post intervention would have allowed for a better understanding of how the intervention influenced employment outcomes from a temporal or change in status perspective.
Interventions that are targeted toward several modifiable factors may ensure a higher likelihood of returning to employment. Our review provides evidence that interventions have often targeted a number of factors. Whereas vocational rehabilitation is often cited as a single ‘factor’ (Trenaman et al., submitted), it actually represents a host of activities and processes, including on-the-job training, job search and placement assistance, and on-the-job support.13 For instance, Inge et al.16 targeted vocational rehabilitation in addition to assistive technology and Wang et al.18 targeted both psychological functioning and functional independence.
Policy differences in social benefits, such as financing, food, lodging or transportation, have been shown to be important predictors of employment outcomes for individuals with SCI.7 These benefits may act as disincentives to return to work if they are withheld when the individual earns above a certain threshold. Thus, the policy context is critical to understanding and developing interventions in this area. Guaranteed benefits regardless of employment income may overcome this barrier to employment; studies comparing regions with different public policies could help determine how policies can best meet the needs of individuals with SCI and society more broadly.
Limitations
Our search terms did not capture non-English publications, or those not indexed in the databases that we searched, but we are convinced that our search strategy was reasonably comprehensive. We were also unable to perform an assessment of quality of publications given the heterogeneity in the methodology and factors investigated.
Conclusions
Despite their disability, many individuals with SCI possess the potential and desire to remain or become productive members of society while deriving the positive psychosocial benefits of employment at the same time. People with SCI may benefit from employment interventions; however, there is a dearth of high-quality research related to interventions that specifically target employment outcomes in individuals with SCI. Consequently, conclusions are mostly based on evidence from observational studies making it difficult to determine causality. For instance, did vocational rehabilitation improve employment outcomes, or did individuals more interested in gaining employment participate in vocational rehabilitation? There is a critical need for high-level evidence studies that address employment in SCI. The best evidence of ‘actionable’ interventions in SCI is from SE. Though only one randomized trial of SE has been completed in SCI, SE has been successful for individuals with other health conditions.24 Future research should focus on identifying innovative interventions, and, given the multifaceted nature of employment programs, the components of the interventions that have the greatest effect on employment outcomes must also be investigated.
DATA ARCHIVING
There were no data to deposit.
References
World Health Organization. International Classification of Functioning, Disability and Health. World Health Organization: Geneva, Switzerland. 2001.
Ville I, Ravaud JF . Work values: a comparison of non-disabled persons with persons with paraplegia. Disabil Rehabil 1998; 20: 127–137.
Krause JS . Employment after spinal cord injury. Arch Phys Med Rehabil 1992; 73: 163–169.
Vogel LC, Klaas SJ, Lubicky JP, Anderson CJ . Long-term outcomes and life satisfaction of adults who had paediatric spinal cord injuries. Arch Phys Med Rehabil 1998; 79: 1496–1503.
Murphy GC, Athanasou JA . The effect of umemployment on mental health. J Occup Organi Psychol 1999; 72: 83–99.
Guttmann L . The place of our spinal paraplegic fellowman in society. Rehabilitation 1959, 15–27.
Ottomanelli L, Lind L . Review of critical factors related to employment after spinal cord injury: implications for research and vocational services. J Spinal Cord Med 2009; 32: 503–531.
Lidal IB, Huynh TK, Biering-Sorensen F . Return to work following spinal cord injury: a review. Disabil Rehabil 2007; 29: 1341–1375.
Ottomanelli L, Sippel JL, Cipher DJ et al. Factors associated with employment among veterans with spinal cord injury. J Vocat Rehabil 2011; 34: 141–150.
Tomassen PC, Post MW, van Asbeck FW . Return to work after spinal cord injury. Spinal Cord 2000; 38: 51–55.
Allen K, Blascovich J . The value of service dogs for people with severe ambulatory disabilities. A randomized controlled trial. JAMA 1996; 275: 1001–1006.
Ottomanelli L, Goetz LL, Suris A, McGeough C, Sinnott PL, Toscano R et al. Effectiveness of supported employment for veterans with spinal cord injury: results from a randomized multisite study. Arch Phys Med Rehabil 2012; 93: 740–747.
Arango-Lasprilla JC, Cardoso E, Wilson LM, Romero MG, Chan F, Sung C . Vocational rehabilitation service patterns and employment outcomes for Hispanics with spinal cord injuries. Rehab Res Pol Educ 2011; 35: 149–162.
Marini I, Lee GK, Chan F, Chapin MH, Romero MG . Vocational rehabilitation service patterns related to successful competitive employments outcomes of persons with spinal cord injury. J Vocat Rehabil 2008; 28: 1–13.
Jellinek HM, Harvey RF . Vocational/educational services in a medical rehabilitation facility: outcomes in spinal cord and brain injured patients. Arch Phys Med Rehabil 1982; 63: 87–88.
Inge KJ, Wehman P, Strobel W, Powell D, Todd J . Supported employment and assistive technology for persons with spinal cord injury: Three illustrations of successful work supports. J Vocat Rehabil 1998; 10: 141–152.
King T, Emery R, Warren S, Landis T . A collaborative approach to returning clients to work during the first year after spinal cord injury. Top Spinal Cord Inj Rehabil 2004; 9: p33.
Wang RY, Yang YR, Yen LL, Lieu FK . Functional ability, perceived exertion and employment of the individuals with spinal cord lesion in Taiwan. Spinal Cord 2002; 40: 69–76.
Jang Y, Wang YH, Wang JD . Return to work after spinal cord injury in Taiwan: the contribution of functional independence. Arch Phys Med Rehabil 2005; 86: 681–686.
Hansen Holm C, Mahmud I, Bhuiyan AJ . Vocational reintegration of people with spinal cord lesion in Bangladesh – An observational study based on a vocational training project at CRP. Asia Pac Disabil Rehabil J 2007; 18: 63–75.
Phillips VL, Hunsaker AE, Florence CS . Return to work and productive activities following a spinal cord injury: the role of income and insurance. Spinal Cord 2012; 50: 623–626.
Shem K, Medel R, Wright J, Kolakowsky-Hayner SA, Duong T . Return to work and school: a model mentoring program for youth and young adults with spinal cord injury. Spinal Cord 2011; 49: 544–548.
Ottomanelli L, Goetz L, McGeough C, Suris A, Sippel J, Sinnott P et al. Methods of a multisite randomized clinical trial of supported employment among veterans with spinal cord injury. J Rehab Res Dev 2009; 26: 919–930.
Dijkers M . Rebuttal to Ottomanelli et al. Methods of a multisite randomized clinical trial of supported employment among veterans with spinal cord injury. J Rehabil Res Dev 2009; 46: 919–930.
Jongbloed L, Backman C, Forwell SJ, Carpenter C . Employment after spinal cord injury: the impact of government policies in Canada. Work 2007; 29: 145–154.
Rowell D, Connelly L . Labor market outcomes for people with a spinal cord injury. Econ Hum Biol 2010; 8: 223–232.
Acknowledgements
We would like to recognize the contribution of Luc Noreau, Erik von Elm and Amira Tawashy to past iterations of the systematic review that informed this publication, in addition to Brodie Sakakibara and Janice Eng who provided valuable feedback on the manuscript.
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Competing interests
Logan Trenaman has previously worked for a company that received funding from the Rick Hansen Institute. Dr William C Miller and Reuben Escorpizo declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Trenaman, L., Miller, W., Escorpizo, R. et al. Interventions for improving employment outcomes among individuals with spinal cord injury: A systematic review. Spinal Cord 52, 788–794 (2014). https://doi.org/10.1038/sc.2014.149
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2014.149
This article is cited by
-
Employment status, hours working, and gainful earnings after spinal cord injury: relationship with pain, prescription medications for pain, and nonprescription opioid use
Spinal Cord (2020)
-
The Impact of Vocational Interventions on Vocational Outcomes, Quality of Life, and Community Integration in Adults with Childhood Onset Disabilities: A Systematic Review
Journal of Occupational Rehabilitation (2020)
-
Employment After Spinal Cord Injury
Current Physical Medicine and Rehabilitation Reports (2020)
-
Work and SCI: a pilot randomized controlled study of an online resource for job-seekers with spinal cord dysfunction
Spinal Cord (2019)
-
The meaning of work after spinal cord injury: a scoping review
Spinal Cord (2018)
