
Abstract
Study design
Cross-sectional, retrospective survey.
Objective
To find the factors influencing the return to work status (RTW) in persons with spinal cord injury (SCI).
Setting
Tertiary care university teaching hospital, India.
Methods
A total of 109 community-dwelling persons with SCI who had been previously rehabilitated and were residing within a 100 km radius from our rehabilitation center were recruited. The return to work status in addition to the demographic, injury, work, environment, physical, and psychosocial characteristics were self-reported via interview.
Results
The return to work rate was 82%. The odds of a return to work post injury was 93 times higher for persons who reported high self-motivation when compared to persons who reported low self-motivation (OR = 93.6, 95% CI 10.5–836.6). The odds of a return to work were nine times higher for persons who reported adequate social support from the family and in the community when compared to those who reported inadequate social support (OR = 8.9, 95% CI 10.5–52.6). Other factors significantly associated with return to work status include younger age at injury, being single, lower level of lesion, vocational training, independence in self-care, and accessibility and mobility to all places.
Conclusion
Motivation and social support are critical to successful return to work following SCI. Comprehensive multidisciplinary rehabilitation, which targets vocational goals, improvements in individual functioning and mobility, and community access are important for successful employment outcomes.
Similar content being viewed by others

Introduction
Improvement in quality of life, community integration, and return to work (RTW) are important for persons with spinal cord injury (SCI) [1]. A person’s RTW status is one of the key indicators of successful rehabilitation and the pinnacle of community reintegration [2]. It has a significant influence on various factors such as life satisfaction, psychological change after injury, change of family and social relationships [3, 4], and existence [1].
RTW rates published in the previous literature for SCI range from 21 to 78.6% [1, 3,4,5,6,7,8,9,10,11,12]. The participants’ characteristics, data collection methods, definition of employment used, and the duration of injury are the factors attributed to a wide range in rates [13]. The facilitators for RTW reported are younger age [1, 3, 5], male gender [10, 11], higher education [3, 4, 6, 7], married [3, 6], less severe injury [5, 9, 10], independent in personal care and mobility [1, 3, 4, 6, 7, 9], and vocational training [3]. The lack of adequate transportation facilities, apprehensions about benefits or financial needs, employer preferences, and access to proper rehabilitation facilities are the barriers for returning to work [13].
In India, there are 1.5 million persons with SCI, among which a majority are male (82%) and aged 16–30 years [8]. RTW opportunities for persons with SCI in India, among the organized sectors where the work structure is more fixed and consistent, and the employees get a secured work, are very limited. We have observed that there are more opportunities among the unorganized sectors such as self-employment, home-based work, sheltered workshops, and job training centers. However, there is limited literature on the employment status and opportunities for persons with SCI in India.
Our center has been providing rehabilitation services at a national level for persons with SCI for the last 60 years in a university hospital setting in a small South Indian city. Our program includes a 3-month inpatient training for the patient and their caregivers, and we structure and tailor the program according to the needs of our patients. We examined the RTW outcomes, and its correlates, among our sample of rehabilitated South Indian persons with SCI.
Methods
Participants
We considered community-dwelling persons with SCI who had completed 12 weeks of inpatient rehabilitation, living within a 100-km radius from our center, a minimum of 1-year post injury, over 18 years old and who attended our annual follow-up program. We excluded patients with associated comorbidities like psychiatric and neurologic conditions. The International Standards for Neurological Classification of Spinal Cord Injury were used to classify the participants’ level and completeness of injury [14].
Study design and setting
The study involved a cross-sectional sample of participants recruited from our rehabilitation center, which is part of a tertiary care university teaching hospital in a small South Indian city from November 2015 to February 2016. The rehabilitation center has a defined geographical area of 100 km radius for regular follow-up activities. Among the patients who live in this follow-up area, 70% live in rural communities with roads and houses that are inaccessible to wheelchairs. There are very few employment opportunities available for persons with disability. Moreover, the economic benefits provided by the government in the community are very less.
Intervention at the rehabilitation center
SCI rehabilitation is an 8–12 week residential, postacute rehabilitation program that starts after the injured person is stable with at least one family member staying with the patient throughout this time. The approximate cost of our inpatient program, excluding food and medicines, is around $900 and is often self-paid because no government or insurance facility is available for rehabilitation in our country. Our program also offers a 6-month residential vocational training program post inpatient rehabilitation to support and empower persons with SCI from rural backgrounds. The training follows and emphasizes a self-employment model to develop small-scale businesses which are home based, as there are no adequate government policies and statutes for employment of persons with disabilities in our country. The program offers tailoring as a primary vocational training and embroidery, toy making, and greeting cards making as add-on training along with a life skills course. We reported the detailed description of the intervention provided at our center in our previous publication [15].
Sample size
We recruited participants using a convenience sampling method. The formula used to calculate the sample size was n = Z21−α/2p (1 − p)/d2. We took a proportion of 37% RTW rate with a precision of 10% and a desired confidence interval at 95% for calculating sample size [16]. The minimum sample required to do our study was 90.
Variables
Dependent variable
RTW: defined as being employed or self-employed, either full-time or part-time (excluding students and homemakers).
Independent variables
Current age; education; marital status; level and severity of the injury was according to American Spinal Injury Association Impairment Scale; vocational training; independence in activities of daily living (ADL), transport, and access to all places; and self-motivation, family support, and social support.
Outcome measure
“Occupational therapists undertook the one-to-one interviews” using the self-reported data form. We designed the data form based on the previous literature to enable data collection. Most of the questions were closed-ended. Few of the questions were open-ended concerning their psychosocial characteristics like motivating factors and the social support to allow greater understanding. The examples of open-ended questions included: “what were the motivating factors to RTW?” and “what was the social support you had?”
The data form comprised the following sections: (i) demographic characteristics including current age, age at the time of injury, age at the time of first vocation post injury, gender, educational status, and marital status; (ii) injury characteristics such as duration of illness, level, and severity of the injury; (iii) details on the work status before and after the onset of SCI that included the work, time spent on work, vocational training, and barriers; (iv) details on environmental characteristics such as the location of residence and architectural barriers at the home and work; (v) details on physical and mobility characteristics that included information related to independence in self-care and mobility, type of mobility aid used, and the mode of transportation; (vi) psychosocial characteristics including family and social support; and (vii) financial characteristics including information such as the number of earning members in the family and annual income and expenditure details.
The final version of the data form consisted of 29 items, which we derived after administering it to five patients and was reviewed by a panel of experts in SCI. We provided options under each item and requested the participants to choose the best option that suited them. They could also provide additional information to clarify their answers (see Supplementary File for data form).
Data analysis
We analyzed the data using SPSS for Windows (version 18.0). We presented the categorical variables such as age, education, marital status, level of injury, the severity of the injury, vocational training, ADL, transport independence, access to all places, self-motivation, family support, and social support as frequencies and percentages. Chi-square tests were used to measure the association between the proportion of patients who returned to work and demographic, injury, work, environment, physical, and psychosocial characteristics. We performed the adjusted analysis for all variables using multivariate regression analysis. The data on financial characteristics were not included for analysis since it was not sufficiently reliable.
Results
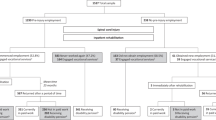
We invited 400 persons with SCI to the annual follow-up program, who lived within a 100 km radius from our center. Of the 140 people with SCI who attended the annual follow-up program, 109 consented to participate. Participants’ demographic, injury, work, physical, mobility, and psychosocial characteristics are presented in Table 1.
Out of 109 participants, 89 (82%) had returned to work. Overall, 65 (73%) of these adopted their own home-based business. Participants of less than 40 years of age and who were single, lower level of SCI had better RTW status. All 23 (100%) participants who received post injury vocational training returned to work when compared to those who did not receive vocational training. Participants who reported independence in ADL, transport, and access to all places showed a better RTW status when compared to those who reported dependence on all these variables. On comparing the RTW status based on the psychosocial factors, we found significant differences in self-motivation and social support (Table 1).
Table 2 shows the results of multiple logistic regression analysis, testing the prediction for the RTW status. The variables included age at injury, marital status, level of injury, ADL independence, transport independence, access of all places, self-motivation, and social support. Self-motivation and social support were found to influence the RTW status. Persons with self-motivation had 93 times more chances for returning to work when compared to those who do not have self-motivation. Results also showed that when compared to those with less social support, participants with greater social support had nine times more chances for returning to work.
Discussion
We investigated the RTW status and its predictive factors in South Indian persons with SCI who completed inpatient rehabilitation in our center. Our study showed a high (82%) RTW rate when compared to the rates published in the previous literature [1, 3,4,5,6,7,8,9,10,11,12].
We could attribute one of the primary reasons for the high RTW rate in our study to the economic necessity among our participants. A major portion of our participants consisted of males (94%) who were the sole breadwinners of the family prior to the injury and lived in a rural area (79%). A majority of them engaged in a daily wage labor. Therefore, there is a great need for a person with SCI to RTW, so they can also contribute to the family’s income to some extent [15]. This is analogous to the findings of a study done in Malaysia [1].
Despite the percentage of persons returning to work being 82%, the work they engage post injury was not providing sufficient earnings for them. Many of them did not return to their previous work because of various limitations, both personal and environmental, and also the lack of adequate government programs and policies in our country for persons with disabilities. Therefore, 73% of them adopted their own business.
The most important predictive factors for RTW in our population derived from logistic regression analyses were self-motivation and social support. This is concordant with previous results, which stated that focusing on various psychosocial factors like an internal locus of control and motivation to work plays an important role in the RTW process. Individuals who had an employment were more likely to have strong social support than the unemployed [6, 17]. These results highlighted the importance of incorporating strategies to improve motivation and to provide social support systems for better reintegration into work for persons with SCI, regardless of their personal, social, and injury characteristics.
The other factors that were found to improve the chance of RTW were similar to the findings in the previous literature such as a younger age group [1, 3, 5], lower level of injury [7, 9, 18], vocational training [3], independence in ADL [8, 16] and transportation [4, 17], and those who had access to all places [19].
Limitations
Our study included only a quarter of the patients with SCI residing within the follow-up area. This underrepresentation was due to the fact that the patients were conveniently selected only from our annual follow-up program. The patients who did not participate possibly had greater physical, social, and/or economic problems, thus introducing a bias in the results of the RTW rate. The participants might have had better independence, transport options, and social support. This could have led to an overestimate of RTW rates in our study. A larger and more random sample might have yielded different results.
Another limitation of the study was that the validity of the psychosocial data could be challenged as it was largely subjective and self-reported.
The third limitation is that the socioeconomic status could not be calculated for our participants, which is reported to be a prognostic factor associated with positive RTW outcomes [20].
The results of our study should be interpreted cautiously because the participants were chosen from our regular follow-up area and will not be representative of all persons with SCI in India, as there are limited rehabilitation and vocational training centers for persons with SCI in India.
Conclusion
One of the ultimate rehabilitation goals to achieve successful reintegration into the community is to return people to profitable and secure work [5]. Our study showed the relationship of various predictive factors and the likelihood of the person with SCI returning to work. An RTW rate of 82% was found among the participants, although we recognized that this was a selective group which was able to attend the follow-up event. Significant predictors of RTW were found to be good self-motivation and the presence of good social support. The other possible predictors which influence RTW were being younger at the age at the time of injury, being single, a lower level of lesion, having had vocational training, a higher degree of independence in self-care, transport, and access to all places. The results suggest that a comprehensive rehabilitation and vocational program, which emphasizes RTW as the ultimate goal, can improve employment status post injury.
Data availability
The data generated/analyzed during the current study are available from the corresponding author on reasonable request.
References
Ramakrishnan K, Chung TY, Hasnan N, Abdullah SJF. Return to work after spinal cord injury in Malaysia. Spinal Cord. 2011;49:812–6.
Meade MA, Lewis A, Jackson MN, Hess DW. Race, employment, and spinal cord injury. Arch Phys Med Rehabil. 2004;85:1782–92.
Jang Y, Wang Y-H, Wang J-D. Return to work after spinal cord injury in Taiwan: the contribution of functional independence. Arch Phys Med Rehabil. 2005;86:681–6.
Krause JS, Terza JV. Injury and demographic factors predictive of disparities in earnings after spinal cord injury. Arch Phys Med Rehabil. 2006;87:1318–26.
Krause JS, Kewman D, DeVivo MJ, Maynard F, Coker J, Roach MJ, et al. Employment after spinal cord injury: an analysis of cases from the Model Spinal Cord Injury Systems. Arch Phys Med Rehabil. 1999;80:1492–500.
Hess DW, Ripley DL, McKinley WO, Tewksbury M. Predictors for return to work after spinal cord injury: a 3-year multicenter analysis. Arch Phys Med Rehabil. 2000;81:359–63.
Lin M-R, Hwang H-F, Yu W-Y, Chen C-Y. A prospective study of factors influencing return to work after traumatic spinal cord injury in Taiwan. Arch Phys Med Rehabil. 2009;90:1716–22.
Gupta N, Solomon J, Raja K. Employment after paraplegia in India: a postal survey. Spinal Cord. 2011;49:806–11.
Krause JS, Terza JV, Erten M, Focht KL, Dismuke CE. Prediction of post-injury employment and percentage of time worked after spinal cord injury. Arch Phys Med Rehabil. 2012;93:373–5.
Kang E-N, Shin H-I, Kim H-R. Factors that influence employment after spinal cord injury in South Korea. Ann Rehabil Med. 2014;38:38–45.
Reinhardt JD, Post MWM, Fekete C, Trezzini B, Brinkhof MWG. SwiSCI Study Group. Labor market integration of people with disabilities: results from the Swiss Spinal Cord Injury Cohort Study. PLoS ONE. 2016;11:e0166955.
Trezzini B, Schwegler U, Reinhardt JD. Work and wellbeing-related consequences of different return-to-work pathways of persons with spinal cord injury living in Switzerland. Spinal Cord. 2018;56:1166–75.
Ottomanelli L, Lind L. Review of critical factors related to employment after spinal cord injury: implications for research and vocational services. J Spinal Cord Med. 2009;32:503–31.
Kirshblum SC, Burns SP, Biering-Sorensen F, Donovan W, Graves DE, Jha A, et al. International Standards for Neurological Classification of Spinal Cord Injury (revised 2011). J Spinal Cord Med. 2011;34:535–46.
Samuelkamaleshkumar S, Radhika S, Cherian B, Elango A, Winrose W, Suhany BT, et al. Community reintegration in rehabilitated South Indian persons with spinal cord injury. Arch Phys Med Rehabil. 2010;91:1117–21.
Tomassen PC, Post MW, van Asbeck FW. Return to work after spinal cord injury. Spinal Cord. 2000;38:51–5.
Lidal IB, Huynh TK, Biering-Sørensen F. Return to work following spinal cord injury: a review. Disabil Rehabil. 2007;29:1341–75.
Wood-Dauphinée S, Exner G, Bostanci B, Exner G, Glass C, Jochheim K-A, et al. Quality of life in patients with spinal cord injury–basic issues, assessment, and recommendations. Restor Neurol Neurosci. 2002;20:135–49.
Krause JS, Sternberg M, Maides J, Lottes S. Employment after spinal cord injury: differences related to geographic region, gender, and race. Arch Phys Med Rehabil. 1998;79:615–24.
Etuknwa A, Daniels K, Eib C. Sustainable return to work: a systematic review focusing on personal and social factors. J Occup Rehabil. 2019;29:679–700.
Acknowledgements
The authors would like to thank Dr. Debbie Skeil for her insightful suggestions, careful reading, and English editing of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors were salaried by the Department of Physical Medicine and Rehabilitation, Christian Medical College, Vellore. The authors declare that there is no conflict of interest.
Ethics approval
The Institutional Review Board (IRB) and the ethics committee (IRB minute no: 8193) approved the research proposal. The authors certify that they followed all applicable institutional and governmental regulations concerning the ethical use of identifiable data during this research.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Blessyolive, J., Samuelkamaleshkumar, S., Annpatriciacatherine, S. et al. Return to work status in rehabilitated South Indian persons with spinal cord injury: a cross-sectional survey. Spinal Cord Ser Cases 7, 32 (2021). https://doi.org/10.1038/s41394-021-00398-2
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41394-021-00398-2
