
Abstract
Study design:
Systematic review.
Objectives:
To determine the different treatment modalities aimed at achieving fecal continence in spina bifida (SB) patients and their effectiveness.
Setting:
International literature.
Method:
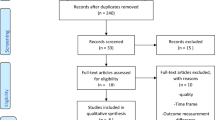
Electronic databases were searched (‘Pubmed’, ‘Web of science’, ‘CINAHL’ and ‘Cochrane’) identifying studies published since the mid-eighties and screened for relevance according to the Centre for Reviews and Dissemination procedure guidelines. A total of 37 studies were selected for inclusion.
Results:
Studies on toilet sitting, biofeedback, anal plug, retrograde colon enemas (RCE) and antegrade colon enemas were found. Fecal continence was achieved in 67% of SB patients using conservative methods (n=509). In patients using RCE (n=190) an 80% continence rate was reached. Patients following surgical treatment (n=469) reached an 81% continence rate, however, 23% needed redo surgery because of complications. Better fecal continence was associated with an improved quality of life, which was negatively influenced by the amount of time spent on bowel management.
Conclusion:
Evidence favors an individually tailored stepwise approach with surgery as a final step in case of failure of conservative measures. Continued specialized support throughout life remains important to maintain continence. Cross-over and comparative trials are needed in order to optimize treatment.
Similar content being viewed by others


Introduction
Spina bifida (SB) or meningomyelocele is a complex neuroembryological disorder resulting from a variable degree of incomplete closure of the posterior neural tube. Clinical presentation is highly variable and depends on the localization of the defect along the spinal cord and the degree of incomplete closure. These patients present with a spectrum of impairments but the primary functional deficits are lower-limb paralysis and sensory loss, bladder and bowel dysfunction and cognitive dysfunction.1
In the majority of patients the lower regions of the spine are affected, resulting in dysfunction of the distal gastrointestinal tract: rectum, anus and anal sphincter. Voluntary control of defecation requires normal rectal sensation, peristalsis and normal anal sphincter function. Two primary involuntary reflexes, the intrinsic and parasympathic reflex, located at sacral level 2–4, initiate defecation. The pudendal nerve, responsible for voluntary defecation, controls the opening and closing of the external anal sphincter. Nerve damage above the S2 level will impair both involuntary reflexes and pudendal nerve function. Loss of the involuntary reflexes perturbs rectal sensation and initiation of defecation. Damage of the pudendal nerve leads to partial or total loss of the voluntary sphincter control. Perturbation of these processes will result in bowel incontinence, which is often associated with constipation in SB patients.2, 3 Fecal incontinence in SB patients is reported to be present in 28–53%, regardless of the therapy used.4, 5, 6, 7
Fecal and urinary incontinence importantly affect quality of life (QoL) in SB patients and form a major barrier to attending school, obtaining employment and sustaining relationships. Krogh et al.4 report that 66% of SB patients older than 6 years with fecal incontinence perceive incontinence as having a negative influence on their social activities. Lie et al.8 report that 75% of SB patients with urinary incontinence regard incontinence as a stress factor.
Review question
A systematic literature review was performed regarding treatment modalities for constipation and/or fecal incontinence in SB patients and their success rate. Treatment success is defined as fecal continence that corresponds to stool losses less than once a month.
Review method
The review is performed following the guidelines of the Centre for Reviews and Dissemination procedures.9
Study selection
Inclusion criteria:
-
Original papers with full paper available
-
Written in English
-
SB patient cohort larger than 20
-
SB patients using any form of bowel management
Exclusion criteria:
-
No data on outcome of treatment for SB patients
-
Review, opinion or editorial pieces
Study identification
The following databases were used for study identification: ‘Pubmed’ and ‘Web of science’, ‘CINAHL’ and ‘Cochrane’ database. A search was performed in March 2013. The following Mesh terms were used: ‘spina bifida and bowel management’, ‘spina bifida and fecal incontinence’, ‘spina bifida and enema’ ‘myelomeningocele and bowel management’, ‘myelomeningocele and fecal incontinence’ and ‘myelomeningocele and enema’. The search covered studies published since 1986 as this was the start of important bowel management evolutions, with the introduction of retrograde colon enemas (RCE) by Shandling10 and some years later the antegrade colon enema (ACE) by Malone.11
This database search resulted in a selection of 37 papers (see flowchart).4, 5, 6, 7, 10, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43
A limitation of the review is the lack of search in gray literature as well as the absence of expert contact to attain more information on the subject.
Data extraction was performed independently by two authors to avoid selection bias in the process. From the full copies retrieved, two articles were not retained by both authors.

Results
A total of 37 studies were included in the review.4, 5, 6, 7, 10, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43
Most studies were observational studies with retrospective or prospective data on SB patient cohorts in a single or multiple center setting. Only two were randomized clinical trials on the use of electrical stimulation, of which one was double-blind controlled23 and one was patient-blinded.26 All studies had a low grade of recommendation.44
Clinical data were collected using questionnaires,6, 7, 12, 13, 14, 15, 17, 19, 23, 24, 25, 29, 30, 34, 35, 37, 43 neurogenic bowel dysfunction scales,20, 26, 45 QoL questionnaires4, 16, 21, 22, 27, 28, 31, 32, 38, 41 or child behavior checklists.4, 31 The collection methods were interviews during follow-up visits6, 15, 20, 25, 43 or telephone contacts4, 7, 12, 17, 23, 32, 38 or both.16, 31, 37, 41
The follow-up period of SB patients after starting bowel management varied from 3,15, 19, 20, 22, 23, 41, 42 over 12,12, 13, 21, 25, 31 3016, 17, 18, 27, 28, 29, 30, 34, 39 and 60 months24, 32, 33, 35, 36, 40, 43 to 120 months.38, 43
To explore different treatment modalities for bowel management in SB and their effectiveness the studies were grouped according to the treatment modality: conservative bowel management (16 studies), electrical stimulation (4 studies) and non-conservative (surgical) bowel management (17 studies).
Conservative bowel management
The studies on conservative bowel management are summarized in Table 1. From the 16 studies, 1 reported on toilet sitting, 2 on biofeedback, 1 on anal plug use, 4 on a stratified treatment strategy and 8 on RCE.
Most studies on bowel management used the above-mentioned strict continence definition (no stool loss or stool loss less than once a month).4, 6, 12, 16, 17, 18, 19, 20, 21 Some studies gave no definition7, 13, 15 or used a less-strict definition.5, 10, 14, 22 The results for fecal pseudo-continence achievement using conservative bowel management varied from 3613 to 100%.10 In order to calculate the combined continence rate, only the studies using the strict continence definition of stool losses less than once a month were used. Fecal pseudo-continence was achieved in 67% (341/509).
Looking only at the studies on RCE (n=8), fecal pseudo-continence was achieved in 80% (144/190). Two studies reported on the effect of RCE on constipation. Mattsson et al.19 reported absence of constipation when using RCE, whereas Ausili et al.20 reported 60% (36/60) constipation relief using RCE. In both studies, all SB patients suffered from constipation at the start. The irrigation fluid used was saline in 3,10, 16, 18 tap water in 417, 19, 21, 22 and one did not mention the fluid type used.20 The irrigation volumes used were sometimes fixed body weight-related quantities (20 ml kg−1)10, 16, 17 or varied between 30019 and 616 ml.21
The time spent on treatment was not often reported7, 12, 13, 14, 15, 17, 20 and if reported varied from 155, 10, 16, 21, 22 over 30 min18 to 60 min.19 Krogh et al.4 described a threefold increase in treatment time when comparing RCE with digital evacuation.
Although achieving fecal pseudo-continence is the primary treatment goal, patient satisfaction is an important secondary goal. Results on satisfaction could not be compared as all reporting studies used different questionnaires and scales. Some studies reported an improvement of satisfaction or a high satisfaction rate associated with successful bowel management.16, 17, 19, 20, 21 The study of Shoshan et al.15 described a significant reduction of daily life impairment by fecal incontinence after bowel management intervention. Finally, implementing a stepwise fecal incontinence treatment protocol improved fecal pseudo-continence and in parallel resulted in better socialization, less need for support by the caregiver and less negative emotional impact.22 However, two studies reported RCE to be ‘a daily burden’. In both studies, the time spent and the energy needed to perform RCE were perceived as a major obstacle.17, 19 Non-compliance and non-motivation could be a result of dissatisfaction with the treatment choice. King et al.12 reported a non-compliance rate of 28%.
Electrical stimulation
The studies on electrical stimulation are summarized in Table 2.
Due to different stimulation techniques and result reports, the studies are not comparable. Most studies (3/4) used the above stated definition of pseudo-continence.23, 24, 25 Only the study of Kajbafzadeh et al.26 used a less-strict pseudo-continence definition. The achieved pseudo-continence rate ranged from 5024 to 70%.25 An increased spontaneous stool frequency was reported by two studies.23, 26 Only one study reported a 73% decrease of constipation. The study of Marshall and Boston23 was the only double-blind randomized placebo-controlled trial reporting an important placebo effect (no actual data available).
Non-conservative, surgical bowel management
The studies are summarized in Table 3. During a surgical procedure, the appendix (or ileum if appendix is not available) is used to create a catheterizable stoma. Besides using the appendix or creating a stoma a cecostomy can be made laparoscopically or percutaneously. A stoma or cecostomy can be placed both right- or left-sided. In this review, mainly results on right-sided stoma were found.
Most studies (10/17) on surgical bowel management or ACE used the strict definition for fecal pseudo-continence (no stool loss or stool loss less than once a month).28, 30, 31, 32, 35, 36, 37, 38, 39, 43 Some studies (5/17) gave no definition for fecal pseudo-continence27, 29, 33, 40, 41 or a less-strict definition.42 One study evaluated incontinence with a 5-point Likert scale.34 The reports on achieving fecal pseudo-continence using non-conservative bowel management varied from 60 (only adults)43 to 94%.35, 36 Again only the studies using the above-mentioned strict definition of pseudo-continence were used to calculate the overall effectiveness of non-conservative treatment. Fecal pseudo-continence was achieved in 81% (378/469). No study reported on constipation. The washout fluid used was saline in 4,27, 32, 37, 42 tap water in another 431, 35, 36, 39 and a combination of both in 2 studies.34, 43 Five studies did not mention the type of fluid used.28, 30, 33, 40, 41 Most authors do not mention the volumes used (9/17).28, 29, 30, 33, 37, 38, 39, 40, 41 When mentioned, volumes varied between 30027 and 1500 ml (in adults).43 The time spent for treatment was not reported in nine studies.28, 29, 30, 33, 35, 36, 38, 39, 40 If reported, it varied from 3027, 37, 43 to 50 min.31, 32, 34, 41, 42, 43
Complications are an important issue in case of surgical treatment. The complication rate varied widely. It was not clear whether studies reported all complications in a comparable way. The follow-up time of the different studies is different, also leading to a different complication rate. The most frequently reported complications were stomal stenosis, wound infections and perforations. Redo surgery for complications varied from 529, 38 over 10%27, 36, 40 to an even higher rate of 30%.28, 31, 32, 42 Overall redo surgery was necessary in 23% (142/616) of patients.
Comparison of the satisfaction rate was not attempted due to the differences in questionnaires and scales used. An improved satisfaction or a high satisfaction rate when using ACE was reported in six studies.27, 28, 29, 31, 32, 38 One study described a significant improvement in anxiety, depression and bother of both caretakers and patients.41 However, most studies report a drop-out rate of 529 to 30%.38 This could be perceived as dissatisfaction of the used strategy. Lack of transition care is, as reported by one study, also an important reason for dissatisfaction. This issue was also reflected in a difference of pseudo-continence rate between children and adults as described in one study, with children achieving higher rates associated with stricter follow-up.43
Discussion
Most studies included in the review report on case series or patient cohorts without controls and therefore no conclusions are drawn regarding best mode of treatment. Further on, data were collected retrospectively in most studies and only a few used standardized questionnaires. Follow-up since starting treatment varied widely. Only two randomized trials both on electrical stimulation were identified. One was a double-blind placebo-controlled study, including, however, a very small patient group without clear end points. Therefore, stating recommendations or drawing conclusions on the different types of treatments used is tentative.
The results indicated that several treatment strategies can achieve pseudo-continence. Large colon washouts, retrograde or antegrade (surgical), however, seem to provide the best overall outcome. The RCE-treated patient group (n=190) is smaller and has a shorter follow-up period compared with the patients treated by surgery. Despite the good pseudo-continence results, most authors state that surgery remains the final step in bowel management because of the amount of complications and drop-outs associated with this treatment modality. Some also consider ACE procedures in case of urological interventions. RCE, should be considered as a first-line treatment when both patients and parents are willing to invest in fecal pseudo-continence. Rigorous follow-up and problem solving in case of treatment failure with extra attention for transition care from adolescence to adulthood is of major importance in becoming and staying fecal pseudo-continent.
For all the treatment strategies used, the balance between successful therapy and the daily time investment will influence the compliance. Several studies tried to measure the impact of both fecal incontinence and treatment issues on social life and daily burden. The wide variety in disease severity as well as the multitude of health issues involved make the QoL measurement especially difficult.
Most centers use a stepwise and individually tailored protocol in the treatment of fecal incontinence with ACE surgery as a last step. These programs are largely experience based and hardly evidence based. A common relevant definition of fecal pseudo-continence is needed to compare study results. In order to ameliorate results and gain insight into which treatment suits which patient, multicenter comparative trials will be needed in patients with comparable impairments, using standardized QoL outcome measurements. Cross-over trials are needed to compare the effect of different irrigation modalities in both RCE and ACE.
Conclusion
Irrigations both retrograde and antegrade are valuable treatment options in becoming fecal continent for SB patients. Surgery is currently used as final step in achievement of pseudo-continence. The burden of treatment can be important and should be accounted for. More research is needed to evaluate different techniques, long-term results of treatment and prediction of success or failure using clearly defined fecal pseudo-continence as a primary goal and standardized QoL evaluation as a secondary goal. Motivational support and strict follow-up of SB patients regarding fecal incontinence have an important role in the outcome.
Data archiving
There were no data to deposit.
References
Vinck A, Nijhuis-van der Sanden MW, Roeleveld NJ, Mullaart RA, Rotteveel JJ, Maassen BA . Motor profile and cognitive functioning in children with spina bifida. Eur J Paediatr Neurol 2010; 14: 86–92.
Churchill BM, Abramson RP, Wahl EF . Dysfunction of the lower urinary and distal gastrointestinal tracts in pediatric patients with known spinal cord problems. Pediatr Clin North Am 2001; 48: 1587–1630.
Zickler CF, Richardson V . Achieving continence in children with neurogenic bowel and bladder. J Pediatr Health Care 2004; 18: 276–283.
Krogh K, Lie HR, Bilenberg N, Laurberg S . Bowel function in Danish children with myelomeningocele. APMIS 2003; 109: S81–S85.
Vande Velde S, Van Biervliet S, Van Renterghem K, Van Laecke E, Hoebeke P, Van Winckel M . Achieving fecal continence in patients with spina bifida: a descriptive cohort study. J Urol 2007; 178: 2640–2644 discussion 4.
Verhoef M, Lurvink M, Barf HA, Post MW, Van Asbeck FW, Gooskens RH et al. High prevalence of incontinence among young adults with spina bifida: description, prediction and problem perception. Spinal Cord 2005; 43: 331–340.
Malone P, Wheeler R, Williams J . Continence in patients with spina bifida: long term results. Arch Dis Child 1994; 70: 107–110.
Lie HR, Lagergren J, Rasmussen F, Lagerkvist B, Hagelsteen J, Borjeson MC . Bowel and bladder control of children with myelomeningocele: a Nordic study. Dev Med Child Neurol 1991; 33: 1053–1061.
Centre for Reviews and Dissemination Systematic Reviews. CRD’s Guidance For Undertaking Reviews in Healthcare. University of York: York, North Yorkshire, UK. 2008.
Shandling B, Gilmour RF . The enema continence catheter in spina bifida patients: successful bowel management. J Pediatr Surg 1987; 22: 271–273.
Malone PS, Ransley PG, Kiely EM . Preliminary report; the antegrade continence enema. Lancet 1990; 336: 1217–1218.
King JC, Currie DM, Wright E . Bowel training in spina bifida: importance of education, patients compliance, age and anal reflexes. Arch Phys Med Rehabil 1994; 75: 243–247.
Whitehead WE, Parker L, Bosmajian L, Morrill-Corbin ED, Middaugh S, Garwood M et al. Treatment of fecal inctontinence in children with spina bifida: comparison of biofeedback and behaviour modification. Arch Phys Med Rehabil 1986; 67: 218–224.
Ponticelli A, Iacobelli BD, Silveri M, Broggi G, Rivosecchi M, De Gennaro M . Colorectal dysfunction and faecal incontinence in children with spina bifida. Br J Urol 1998; 81 (Suppl 3): 117–119.
Soshan L, Ben-Zvi D, Katz-Leurer M . Use of the anal plug in the treatment of fecal incontinence in patients with myelomeningocele. J Pediatr Nurs 2008; 23: 395–399.
Liptak GS, Revell GM . Management of bowel dysfunction in children with spinal cord disease or injury by means of the enema continence catheter. J Pediatr 1992; 120: 190–194.
Schöller-Gyüre M, Nesselaar C, van Wieringen H, van Gool JD . Treatment of defecation disorders by colonic enemas in children with spina bifida. Eur J Pediatr Surg 1996; 6 (Suppl I): 32–34.
Eire PF, Cives RV, Gago MC . Faecal incontinence in children with spina bifida: the best conservative treatment. Spinal Cord 2008; 36: 774–776.
Mattsson S, Gladh G . Tap-water enema for children with myelomeningocele and neurogenic bowel dysfunction. Acta Paediatr 2006; 95: 369–374.
Ausili E, Focarelli B, Tabacco F, Murolo D, Sigismondi M, Gasbarrini A et al. Transanal irrigation in myelomeningocele children: an alternative safe and valid approach for neurogenic constipation. Spinal cord 2010; 48: 560–565.
Pereira PL, Salvador OP, Arcas JA, Urrutia MJM, Romera RL, Monereo EJ . Transanal irrigation for the treatment of neuropathic bowel dysfunction. J Ped Urol 2010; 6: 134–138.
Choi EK, Shin SH, Yj Im, Kim MJ, Han SW . The effects of transanal irrigation as a stepwise bowel management program on the quality of life of children with spina bifida and their caregivers. Spinal Cord 2013; 51: 384–388.
Marshall DF, Boston VE . Altered bladder and bowel function following cutaneous electrical field stimulation in children with spina bifida—interim results of a randomized double-blind placebo-controlled trial. Eur J Pediatr Surg 1997; 7 (Suppl I): 41–43.
Palmer LS, Richards I, Kaplan WE . Transrectal electrostimulation therapy for neuropathic bowel dysfunction in children with myelomeningocele. J Urol 1997; 157: 1449–1452.
Han SW, Kim MJ, Kim JH, Hong CH, Kim JW, Noh JY . Intravesical electrical stimulation improves neurogenic bowel dysfunction in children with spina bifida. J Urol 2004; 171: 2648–2650.
Kajbafzadeh AM, Sharifi-Rad L, Nejat F, Kajbafzadeh M, Talaei HR . Transcutaneous interferential electrical stimulation for management of neurogenic bowel dysfunction in children with myelomeningocele. Int J Colorectal Dis 2012; 27: 453–458.
Hensle TW, Reiley EA, Chang DT . The Malone antegrade continence enema procedure in the management of patients with spina bifida. J Am Coll Surg 1998; 186: 669–674.
Shankar KR, Losty PD, Kenny SE, Booth JM, Turnock RR, Lamont GL et al. Functional results following the antegrade continence enema procedure. Br J Surg 1998; 85: 980–982.
Webb HW, Barraza MA, Stevens PS, Crump JM, Erhard M . Bowel dysfunction in spina bifida—an American experience with the ACE procedure. Eur J Pediatr Surg 1998; 8 (Suppl I): 37–38.
Curry JI, Osborne A, Malone PS . The MACE procedure: experience in the United Kingdom. J Pediatr Surg 1999; 34: 338–340.
Aksnes G, Diseth TH, Helseth A, Edwin B, Stange M, Aafos G et al. Appendicostomy for antegrade enema: effects on somatic and psychosocial functioning in children with myelomeningocele. Pediatrics 2002; 109: 484–489.
Dey R, Ferguson C, Kenny SE, Shankar KR, Coldicutt P, Baillie CT et al. After the honeymoon—medium-term outcome of antegrade continence enema procedure. J Pediatr Surg 2003; 38: 65–68.
Casale AJ, Metcalfe PD, Kaefer MA, Dussinger AM, Meldrum KK, Cain MP et al. Total continence reconstruction: a comparison to staged reconstruction of neuropathic bowel and bladder. J Urol 2006; 176: 1712–1715.
Lemelle JL, Guillemin F, Aubert D, Guys JM, Lottmann H, Lortat-Jacob S et al. A multicentre study of the management of disorders of defecation in patients with spina bifida. Neurogastroenterol Motil 2006 Feb; 18: 123–128.
Bani-Hani AH, Cain MP, King S, Rink RC . Tap water irrigation and additives to optimize success with the Malone antegrade continence enema: the Indiana university algorithm. J Urol 2008 Oct; 180: 1757–1760.
Bani-Hani AH, Cain MP, Kaefer M, Meldrum KK, King S, Johnson CS et al. The Malone antegrade continence enema: a single institutional review. J Urol 2008; 180: 1106–1110.
Wong AL, Kravarusic D, Wong SL . Impact of cecostomy and antegrade colonic enemas on management of fecal incontinence and constipation. Ten years of experience in pediatric population. J Pediatr Surg 2008; 43: 1445–1451.
Yardley IE, Pauniaho SL, Baillie CT, Turnock RR, Coldicutt P, Lamont GL et al. After the honeymoon comes divorce: long-term use of the antegrade continence enema procedure. J Pediatr Surg 2009; 44: 1274–1277.
Matsuno D, Yamazaki Y, Shiroyanagi Y, Ueda N, Suzuki M, Nishi M et al. The role of the retrograde colonic enema in children with spina bifida: is it inferior to the antegrade continence enema? Pediatr Surg Int 2010; 26: 529–533.
Bar-Yosef Y, Castellan M, Joshi D, Labbie A, Gosalbez R . Total continence reconstruction using the artificial urinary sphincter and the Malone continence enema. J Urol 2011; 185: 1444–1448.
Ok JH, Kurzrock EA . Objective measurement of quality of life changes after ACE Malone using the FICQoL survey. J Ped Urol 2011; 7: 389–393.
Siddiqui AA, Fishman SJ, Bauer SB, Nurko S . Long-term follow-up of patients after antegrade continence enema procedure. JPGN 2011; 52: 574–580.
Vande Velde S, Van Biervliet S, Van Laecke E, De Bruyne R, Verhelst H, Hoebeke P et al. Colon enemas in treatment of fecal incontinence in patients with spina bifida. J Urol 2013; 189: 300–304.
Atkins D . Grading quality of evidence and strength of recommendations. BMJ 2004; 328: 1490–1494.
Krogh K, Christensen P, Sabroe S, Laurberg S . Neurogenic bowel dysfunction score. Spinal Cord 2006; 44: 625–631.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Velde, S., Biervliet, S., Bruyne, R. et al. A systematic review on bowel management and the success rate of the various treatment modalities in spina bifida patients. Spinal Cord 51, 873–881 (2013). https://doi.org/10.1038/sc.2013.123
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2013.123
Keywords
This article is cited by
-
Outcomes of autologous bone marrow mononuclear cell administration in the treatment of neurologic sequelae in children with spina bifida
Stem Cell Research & Therapy (2023)
-
Transitioning care for adolescents with spina bifida in the US: challenges for management
Child's Nervous System (2023)
-
Reduction of transverse rectal diameter and its effect on bladder dynamics in children with spinal dysraphism
BMC Urology (2022)
-
External kinesiology tape for improvement in fecal incontinence symptom bother in women: a pilot study
International Urogynecology Journal (2022)
-
Malone Antegrade Continence Enemas vs. Cecostomy vs. Transanal Irrigation—What Is New and How Do We Counsel Our Patients?
Current Urology Reports (2019)
