
Abstract
Study design:
Retrospective longitudinal study of short- and long-term urinary complications in chronic spinal cord injury (SCI) patients managed at the Midlands Centre for Spinal Injuries (MCSI).
Setting:
MCSI, Oswestry, UK.
Method:
A total of 185 SCI patients were admitted to the MCSI between 1984 and 1989. Only 119 patients who met the following criteria were included: traumatic SCI, Frankel grade A–D, admission within 6 weeks post injury, regular annual follow-up or alternate year at MCSI, follow-up longer than 8 years. Follow-up ranged between 8 and 21 years with a mean of 17.7 (s.d.=1.98). The method of bladder drainage varied from the time of injury. Drainage was by indwelling urethral catheterisation (IndUC) before admission to the MCSI. Within 24 h of admission, assisted clean intermittent catheterisation (ACIC) by the nursing staff was commenced. This was followed by clean intermittent self catheterisation (CISC) once the patient was mobilised in the wheel chair and trained in the procedure. When detrusor reflex activity develops, patients with good hand function were given a choice between CISC and reflex voiding (RV). Patients with poor hand function are given the choice between RV, suprapubic catheters or ACIC during hospitalisation and after discharge. Only a minority of these patients choose ACIC following discharge. RV was supplemented occasionally by sphincterotomy. There were 99 males and 20 females (5:1). The age at the time of injury was 16–63 years with a mean of 29 (s.d.=12). Instead of a single method, a pattern of bladder management was analysed in the context of three continuous phases: Phase1 preadmission to MCSI. Phase2 during first hospitalisation at MCSI. Phase3 post discharge. In each phase, the patients were divided into those with and without complications. The complications were analysed in relation to the management and other relevant factors.
Results:
The total complication rate at all stages was 62%. Complications of the upper urinary tract accounted for 22.6%. These results compared favourably with published material.
Conclusion:
The sequential system of supervised bladder management commencing with brief IndUC followed by IntC and/or RV remains effective in keeping the complication rate relatively low in SCI patients, who undergo regular surveillance and timely intervention.
Sponsorship:
The project was supported by SPIRIT, a charitable not for profit trust that supports teaching, training, clinical research and dissemination of knowledge about all aspects of spinal paralysis in the UK.
Similar content being viewed by others
Introduction
Intermittent catheterisation has, since the late 1940s, helped improve our knowledge of the bladder and reduce the incidence of urinary complications in spinal cord injury (SCI).1, 2, 3 Bladder management in patients of this study consisted of: indwelling urethral catheterisation (IndUC) before admission to the Midlands Centre for Spinal Injuries (MCSI), assisted intermittent catheterisation (ACIC) by the nursing staff within 24 h of admission to the MCSI and subsequently, Clean intermittent self catheterisation (CISC) by the patient once he/she becomes skilled, confident and safe to carry out the procedure. Once reflex activity of the detrusor develops, the patient is offered informed choice between CISC and reflex voiding (RV). The quality of hand function, detrusor and sphincter function, age, psycho-social, vocational, environmental and financial circumstances usually influence patients’ choice. All patients are offered lifelong follow-up every 1 or 2 years by the MCSI. Patients with active or overactive detrusor and functional bladder outlet obstruction are given a choice between intermittent catheterisation with detrusor suppression, bladder outlet surgery with RV or suprapubic catheterisation, when necessary.4, 5, 6
The development of urodynamic studies in the 1950s to its standardisation in the 1980s have immensely expanded our knowledge about the function of the bladder and its sphincter.7, 8, 9, 10 This has led to a diversity of methods of management aimed at tackling specific abnormal function or problems of the bladder and its sphincter. They include sacral anterior root stimulation, urethral stenting, botulinum-A toxin injection, neuromodulation, artificial sphincter, and so on.11, 12, 13, 14 These new methods have changed the landscape of bladder management. Controversy however exists concerning the safety of RV.
Considering the shortage of comprehensive long-term outcome studies with various methods of management and the controversy over RV, it seems appropriate to conduct such a study within a specialised centre with a unified pattern of bladder management.
Materials and methods
This is a retrospective study of patients admitted to the MCSI, Robert Jones and Agnes Hunt Orthopaedic Hospital, Oswestry, UK.
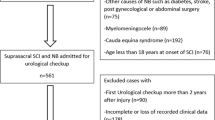
One hundred and fifty one consecutive patients who met the following criteria were included.
-
1
Traumatic SCI.
-
2
Frankel grade A–D.
-
3
Admission to MCSI between 1984 and 1989.
-
4
Admission within 6 weeks post injury.
-
5
Regular annual or alternate year follow-up at the MCSI.
-
6
Follow-up longer than 8 years after first discharge.
Another 34 patients who did not meet these criteria were excluded.
The medical records, imaging, neurological diagnoses and laboratory tests were comprehensively reviewed independently by the three coauthors.
There were 99 males and 20 females (5:1). The age at the time of injury was 16–63 years with a mean of 29 (s.d.±12). The causes of injury are presented in Figure 1. The majority of patients were admitted within 3 days of injury and the great majority within one week (Figure 2). The neurological impairment at the time of the first discharge is used for analysis due to the long-term nature of the study.

Causes of injury.

Time lag from injury to admission.
There were 69 paraplegic and 50 tetraplegic patients. Two of the paraplegic patients had a S3 sacral lesion. The number is too small to warrant a special group. Both developed only minor urinary tract infection (UTI). When patients of this study were admitted, the ASIA/ISCOS Classification had not yet been developed, hence the Frankel scale was used. The Frankel scale was A in 63 patients, B in 8, C in 14 and D in 34.
Routine clinical assessment, urine analyses, ultrasound scans or intra venous urograms (IVU) were carried out every one or two years in all patients. Patients had free phone access and were encouraged to contact the MCSI if they developed any problems, including urological problems. Annual or alternate year cystoscopies were regularly performed in patients with suprapubic or indwelling catheters. Urodynamic studies were carried out in patients with urinary tract symptoms and when urological investigations revealed abnormality/ies. Urodynamic studies were done in 94 (79%) patients. In all, 25 patients (21%) did not have urodynamic studies. Of these, 17 were Frankel D and with minor bladder problems. The other 8 patients were Frankel A, B or C. Four of them had minor UTI while the others had no complications.
The bladder management was divided into three phases.
-
Phase 1: before admission to the MCSI.
-
Phase 2: during hospitalisation at the MCSI.
-
Phase 3: after discharge from the MCSI.
The rationale of such division is the following.
The methods of bladder management and their efficacy depended on: the stage of development of the neurological lesion, a number of personal non-medical circumstances as well as the compliance of the referring hospital and/or the patient with expert medical advice.
All patients used more than one method of management at different times particularly towards old age.15 Considering that previous method/s could affect the outcome,16 it would seem reasonable to analyse a pattern of methods of management in the context of the stage of the lesion and the available expertise rather than analysing a single method in isolation.
The complications explored were urinary tract infection, pyelonephritis, upper tract dilatation, vesical calculi, upper tract calculi, urethral damage, non-functioning kidney with global atrophy and epididymo-orchitis. A diagnosis of urinary tract infection was established when the patient had fever, high WBC in the urine (>10 ml−1) and culture of urine with 105 colony-forming units per ml while no other source of infection could be located.17 Culture alone may not be decisive if it is negative while other criteria of the diagnosis are all met because there could be false-negative culture.17 Patients with negative culture while other criteria of diagnosis of an infection are met and other sources of infections are excluded are counted in this study as having UTI.
In the three previously described phases of management, all patients are grouped into those with and those without complications. The number and rate of complications are analysed in relation to the methods of bladder management.
Gender, age at injury, age at admission, mean age from injury to last follow-up, delay in admission, length of stay in the MCSI, level of lesion (tetraplegia or paraplegia) and Frankel scale are also analysed in association with complications.
Of the 119 patients, 2 Frankel D patients had no problems of micturition and felt that they did not need to attend further follow-up after 4 years of injury but were reported to be unimpaired urologically for a number of years later. Of the remaining 117 patients, follow-up from injury to last follow-up ranged 8–21 years with a mean of 17.7 (s.d.=1.98).
The statistical method used for comparing proportions was χ2, while that for comparing mean between groups with and without complications was Mann–Whitney U test.
Results
Phase 1 (before admission to the MCSI)
In all, 100 of the 119 patients were admitted to the MCSI within one week of injury and the remaining 19 patients within 6 weeks. All patients were initially managed with IndUC. In all, 38 patients (32%) did not have their method of urine drainage documented immediately before admission to the MCSI. Of the remaining 81 patients, 56 (69%) had IndUC, 22 (27%) had ACIC, and in 3 other patients, RV and/or bladder expression were used before admission to MCSI. One patient with a C4 Frankel A injury and an initial IndUC had a sphincterotomy before admission in order to achieve RV. Immediately before admission, only two (0.18%) male patients were suspected of having UTI. They were admitted 15 and 38 days post injury, respectively. The number is too small to warrant any statistical analysis.
Phase 2 (during hospitalisation in the MCSI)
Soon after admission to the MCSI, the indwelling catheter is removed and drainage is achieved initially by ACIC carried out by the nursing staff. Once convenient, confident and safe, patients with good hand function (paraplegic and some patients with C8 tetraplegia) carry out CISC. Female patients with poor hand function usually choose suprapubic or indwelling urethral catheter drainage. Informed patient's choice of RV is respected following education of the patient about the potential complications of unsupervised RV and the importance of regular medical surveillance and vigilant reporting of urinary problems and/or symptoms of autonomic dysreflexia. Anticholinergics were administered to patients with detrusor overactivity. Alpha blockers were administered to patients with marked bladder outlet obstruction. Both anticholinergics and alpha blockers were administered to patients with detrusor sphincter dyssynergia and symtoms of autonomic dysreflexia. Bladder outlet surgery was considered with full informed consent of the patient if the medication failed and RV remained the preferred method of drainage by the patient.
Throughout phase 2 period of observation, 45 patients (38%) had complications, 74 patients (62%) had no complications. The complications are listed in Table 1. UTI stands out as the most common complication either alone or in combination with other complications. Eight patients (10%) had upper urinary tract complications. Fifty-nine male and fifteen female patients had no complications in phase 2 of the study.
Tables 2 and 3 reveal the bladder management in each of the group without and with complications, respectively. In both groups, the overwhelming method of bladder management was four-hourly intermittent catheterisation. Therefore, factors other than intermittent catheterisation may have contributed to the difference between those with and those without complications.
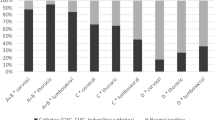
When we looked at the level of injury, it was noted that paraplegic patients on clean intermittent catheterisation (CIC) had a lower complication rate than tetraplegic patients on CIC (Figure 3); however, the difference was not statistically significant (χ2 P>0.05).

The breakdown of number of paraplegic and tetraplegic patients in patients with and without complications during phase 2 (stay in MCSI).
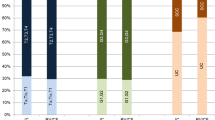
We looked at the density of the neural injury. Figure 4 reveals the distribution of Frankel scales. Of 45 patients with complications, 37 (82.2%) belonged to A, B and C. Of the 74 patients without complications, 48 (65.8%) belonged to A, B and C. The difference is statistically significant (χ2 P<0.05).

Breakdown of number of patients of Frankel grades in patients with and without complication during phase 2 stay in the MCSI.
The length of hospital stay of patients without complications is 41–391 days with a mean of 148 (s.d.=73), while that with complications is 30–422 days with a mean of 205 (s.d.=78). The difference is not statistically significant.
The length of hospital stay was longer in patients with Frankel A, B and C than in the Frankel D patients. This was 30–422 days with a mean of 183 days (s.d.=77) in Frankel A, B and C patients compared with 41–391 days with a mean of 136 (s.d.=79) in the Frankel D group. The difference is not significant.
The length of hospital stay for the paraplegic patient ranged between 41–422 days with a mean of 139 days (s.d.=72), while for the tetraplegic it was 30–360 with a mean of 212 (s.d.=72). The difference is highly significant (P<0.01).
Phase 3 (after discharge from MCSI to last follow-up)
During this period, seventy-three patients (61%) had complications. The complications are listed in Table 4. The overwhelming complication was UTI. Nineteen patients (16%) had upper urinary tract (UUT) problems. Forty-six (39%) patients had no complications. Of those with complications, 59 were male and 14 female. Of those without complications, 39 were male and 7 female. There is no significance between genders.
The breakdown of patients with tetraplegia and paraplegia is shown in Figure 5. This indicates that paraplegics have a higher proportion in the group without complications but the difference is not statistically significant (P>0.05).

The breakdown of number of paraplegic and tetraplegic patients in patients with and without complications during phase 3 after discharge from MCSI.
When the density of lesion is considered as seen in Figure 6, the ratio of Frankel A+B+C to D in the non-complication group was 19:27, while in the complication group the ratio was 66:7. The difference is statistically highly significant (P<0.001).

Breakdown of number of patients of Frankel grades in patients with and without complication phase 3 after discharge from MCSI
Table 5 lists the methods of urine drainage. Twenty-four patients enjoyed near normal micturition without the need of any further intervention. They all belonged to Frankel D. Only three of them had mild UTI.
Of the 10 patients who continued to use IndUC, 6 were tetraplegic and 4 were paraplegic.
RV dominated in both groups. If the 24 patients with Frankel D who did not need intervention were excluded for fair comparison, of the remaining 95 patients, 20 of the 25 patients (80%) in the non-complication group used RV with or without bladder expression. In the complication group, 42 of the 70 patients (60%) used RV with or without bladder expression.
Summary of complications of all phases
The overall complications of all three phases are summarised and compared with a similar report published recently in Table 6 and Table 7. 16 In our series, the eight patients with urethral problems had long period of catheterisation, either indwelling or intermittent.
In all three phases, 13 of 16 females and 65 of 103 males had complications. Upper tract complications were seen in 2 females and 15 males, respectively. There is no statistically significant difference between genders.
The age at the time of injury of patients without complication was 16–63 with a mean of 31 (s.d.=12.8). The age at the time of injury of patients with complications was 15–60 with a mean of 29 (s.d.=11.4). The age at the last follow-up of patients without complication was 33–80 with a mean of 48 (s.d.=13). The age at the last follow-up of patients with complications was 31–80 with a mean of 47 (s.d.=11.6). There is almost no difference between the two groups at the time of injury and last follow-up.
Discussion
Due to the relative short time between injury and admission to the MCSI, the incidence of urinary complications before admission to the MCSI is minimal and does not lend itself to detailed analysis. This report focuses on the period of admission to the MCSI and posts discharge up to a minimum of 8 years follow-up studying complications and their relation with bladder management, neurological level and density of the neural damage.
In our study, the incidence of complications does not seem to be related to age or gender.
During hospitalisation in the MCSI, the preferred methods of bladder management in the overwhelming majority are ACIC followed by CISC when the patient is capable of doing so. We therefore tried to look into other possible factors associated with complications. We found that the higher the level of lesion and the more dense the neurological injury, the higher is the incidence of complications. Both high level and high density of injury were associated with statistically significant higher incidence of complications. This suggests that both the level and the density of the injury are significant determinant factors in the development of complications. The stay in the hospital is unsurprisingly significantly longer in the group with urinary tract complications who usually have more severe injuries.
The incidence of complication rose from 38% during their stay in the MCSI to 62% in the post-discharge period of the study. This is not surprising, as following discharge, the more chronic the lesion, the older the patient becomes and the less attention the patient receives in the community, the more he/she is likely to develop complications. The relatively high proportion of RV used in both groups with and without complications suggests that, with annual or alternate year regular urological surveillance and easy access to the Spinal Injury Centre, when symptoms arise, these methods could be made safe. In the group without complications, the proportion of patients with RV was higher than in the group with other methods of bladder drainage. This by no means suggests that RV carries less risk. Our regular and frequent surveillance of the urinary system and open telephone access to the service has enabled us to spot early symptoms and signs of increased risk to the upper and lower urinary tract such as frequent UTIs, bladder calculi, autonomic dysreflexia, excess spasticity, detrusor overactivity, ureteric reflux and potential upper tract involvement in time to review the management of the patient. It could be argued that alternative methods of bladder drainage can carry similar risks if left unsupervised.
The incidence of complications of UUT also increased from 6.7 to 16% in phase 3. This could be due to natural progression of the urological condition, different methods of bladder management in the community and/or lack of compliance of the patient. In both groups with and without complications, the main method of drainage used was RV with or without Crede manoeuvre. Again, during this period the only difference between those with and without complications is the density of the spinal cord lesion. Patients in Frankel scales A+B+C with more dense lesions are statistically significantly more numerous in the group with complications than the group without complications.
In a recent report of Weld and Dmochowski (W&D),16 the overall number of patients with complications was 294 out of 316 (93%) compared with 74 out of 119 (62%) in our series. In the W&D report, various UUT complications were observed 83 times in 316 patients. It must be appreciated that W&D classify pyelonephritis and upper tract calculi as two separate groups of UUT complications. These are also separate from the major group of UUT abnormalities, which probably include only hydronephrosis and reflux. When the same patient suffered more than one UUT complication, it was counted more than once. This method of counting inevitably led to some double or even triple counting when one patient had more than one UUT complication. Hence, its rate cannot be accurately compared with our low rate of 14% (17 out of 119 patients). However, when the UUT complications are looked into individually, in every UUT complication, our rate is much lower. Hence, it can be said that the overall rate of UUT complications is lower in our series than that of W&D.
W&D reported that 93% of their patients developed clinical lower urinary tract infection symptoms while the incidence of UTI in our series was 61%. W&D however do not define the presentations of UTI and hence the difficulty in accurately comparing the incidence of UTI between the two series. It is noteworthy that, UTI is the commonest reported of all complications of SCI in all series.18, 19 It is also worth mentioning that the series of W&D had a large proportion of sacral lesions, 47 out of 316 patients (15%), whereas in our group sacral lesions constituted only 1.7%. The density of the neurological deficit of W&D's series was not described. The article only classified the neurological deficit as complete or incomplete. It is not clear in W&D's series if there was a predominance of Frankel B & C incomplete and proportionately less Frankel D incomplete patients or not. If that had been the case, according to our findings this would have been expected to be associated with a higher incidence of complications. In other words, it is difficult to make accurate comparisons between the two series because of the lack of important information.
The sharp contrast of sphincterotomy performed in 34 patients (28.5%) in this series compared with 0% in the report of W&D and other communications suggest that there has been a trend for the past decade or so to perform the procedure much less frequently or not at all.16, 20 We believe that damage of the upper urinary tract is potentially an even more dangerous condition if the patient chooses RV when bladder overactivity with detrusor sphincter dyssynergia is not properly dealt with. Like others, we believe sphincterotomy still has an important role to have in the neurogenic bladder management.21, 22, 23 Furthermore, sphincterotomy may have contributed to the relatively low complication rate in this study. Occasional profuse bleeding during the procedure, damage to the branch of the pudendal nerve and the need for repeated operations may have contributed to the reluctance of performing sphincterotomy. These problems can be resolved with improvement of technique, appropriate equipment, improved skills and with accumulation of experience.23
Suprapubic catheterisation was used in five patients (4.2%) in our group compared with eight (2.5%) in the report by W&D. Suprapubic drainage remains an option for bladder drainage in the female tetraplegic patient and in selected cases.24, 25 In another recent report from New Zealand, of the entire SCI population of 1018, 149 (14.6%) patients had suprapubic drainage for long-term bladder management.26 In these 149 patients, upper tract calculi were detected in 14 (9.4%) during a 6-year follow-up. This follow-up is short: 6 years compared with ours of 19.1 years. This could explain the overall complication rate of 51% in their series being lower than 65% in ours, as well as the lower incidence of UTI that was 27% in their series compared with ours (44%). Despite our longer follow-up period, we have much fewer upper tract calculi (that is, of 2/151 patients) compared with the New Zealand study (14/149 patients).
No patients required surgical nephrectomy in our series. This compares 12 patients with nephrectomy (3.8%) patients in the report of W&D, where one patient had nephrectomy due to additional trauma rather than progressive urological problems of SCI. In our series, there was one case of global atrophy of a non-functioning kidney as a result of hydronephrosis and Staghorn kidney calculus. Although no surgery was carried out, this could be considered as self-nephrectomy.
If properly managed and supervised, RV in our experience remains a safe and practical option of management following recovery from spinal shock and return of bladder reflexes. Dahlberg et al.27 also found that RV was associated with fewer UTIs than CISC. RV in the community is also safe provided patients are regularly and frequently followed up and monitored urologically by specialists familiar with the problems of patients with SCI. It is also important that patients and carers are well educated in the potential problems and presentations of problems associated with RV, especially, those of autonomic dysreflexia. As well as regular and frequent monitoring and patient education, the MCSI provides a hotline for patients to consult with the specialists whenever problems arise. It could be argued that whatever is the type of drainage of the bladder these conditions should apply.
In our experience, the type of neurogenic bladder is not the only factor that determines the choice of bladder drainage. The level of injury, quality of hand function, age, environmental, vocational, psychological, social and sometimes financial factors influence the choice of management for a particular patient, as well as the compliance by the patient. We feel it is therefore important that the patient is made aware of all available methods of management and the advantages and disadvantages of each in order for him/her to make an informed choice of the method that suits him/her best and will comply with. Whatever the method of management of the neurogenic bladder, regular and frequent urological surveillance by clinicians familiar with all the urological as well as the non-urological problems of the SCI patient is essential for good outcomes and the prevention and/or early diagnosis and treatment of complications.
Conclusion
An indwelling or a suprapubic catheter for a few days before admission to a SCI Centre remains a practical and effective method of initial bladder drainage, if ACIC or CISC cannot be safely commenced in the referring hospital. Considering expert urological surveillance and a system of early intervention are essential for minimising the rate of morbidity and urological complications irrespective of the method of drainage; the patient can be given a choice between both CISC and RV to take into account personal capability, lifestyle, vocation and environmental circumstances and quality of life as long as the patient is aware and agreeable to undergo lifelong surveillance to protect renal functions. Our study suggests that, besides the method of bladder drainage and the adequacy of management of the urinary system, both the level and density of the neurological damage are likely to be factors in the development of complications of the urinary tract at least during the acute and subacute phases of SCI, while in the chronic phase the more dense the neurological lesion, the higher the risk of complications. Further studies will be required to confirm this.
References
Guttman L . Initial treatment of traumatic paraplegia. Proc Roy Soc Med 1954; 47: 1103–1109.
Guttman L, Frankel H . Chapter 9: the value of intermittent catheterisation in the early management of traumatic paraplegia and tetraplegia. Paraplegia 1966; 4: 63–84.
Dik P, Ypma F, Gool JD . Chapter 9: History of the use of catheters in spinal cord lesions. In: Dik P (ed.) Urological Treatment and Follow-up of Patients with Spinal Dysraphism. Dissertation of Universiteit: Utrecht, 2004.
O’Flynn JD . Early and late management of the neuropathic bladder in spinal cord injury patients. J Urol 1978; 120: 726.
Golji H . Urethral sphincterotomy for chronic spinal cord injury. J Urol 1980; 123: 204.
Cook JB, Smith PH . Percutaeneous suprapubic cystotomy after spinal cord injury. Br J Urol 1976; 48: 119.
Boyce WH, Corey EL, Vest SA, French CR . The correlation of electromyographic records with neurogenic dysfunction of the human urinary bladder. J Urol 1953; 70: 605–614.
Adramson AS, Roussan MS, Oronzio G . Method of evaluation of function of neurogenic bladder. JAMA 1966; 195: 554.
Bradley WE, Timm GW, Scott FB . Cystometry: III. Cystometers Urol 1975; 5: 843.
Abrams P, Blaivas JG, Stanton SL, Andersen JT, Fowler CJ, Gerstenberg T et al. Sixth report on the standardisation of terminology of lower urinary tract function. Procedures related to neurophysiological investigations: electromyography, nerve conduction studies, reflex latencies, evoked potentials and sensory testing. The International Continence Society Committee on Standardisation of Terminology, New York, May 1985. Scand J Urol Nephrol 1986; 20: 161–164.
Brindley GS, Polkey CE, Rushton DN . Sacral anterior root stimulator for bladder control in paraplegia. Paraplegia 1982; 20: 365.
Shaw PJR, Milroy EJ, Timoney AG, el Din A, Mitchell N . Permanent external striated sphincter stents in patients with spinal injuries. Brit J Urol 1990; 66: 297–302.
Schurch B, Stöhrer M, Kramer G, Schmid DM, Gaul G, Hauri D . Botulinum-A Toxin for treating detrusor hyperreflexia in spinal cord injured patients: a new alternative to anticholinergic drugs? Preliminary results. J Urol 2000; 164: 692–697.
Kirkham APS, Knight SL, Craggs MD, Casey AT, Shah PJ . Neuromodulation through sacral nerve roots 2 to 4 with a Finetech-Brindley sacral posterior and anterior root stimulator. Spinal Cord 2002; 40: 272–281.
Drake MJ, Cortina-Borja M, Savic G, Charlifue SW, Gardner BP . Prospective evaluation of urological effects of aging in chronic spinal cord injury by method of bladder management. Neuourol Urodynam 2005; 24: 111–116.
Weld KJ, Dmochowski RR . Effect of bladder management on urological complications in spinal cord injured patients. J Urol 2000; 163: 678–772.
Tomson C (2003). Section 20, Chapter 12, Urinary tract infection. In: Warrell DA et al. (eds). Oxford Textbook of Medicine, 4th edn. vol. 3. Oxford University Press, pp 240–433.
Ruutu M, Lehtonen T . Urinary tract complications in spinal cord injured patients. Ann Chir Gynaecol 1984; 73: 325.
Penders J, Huylenbroeck AA, Everaert K, Van Laere M, Verschraegen GL . Urinary infections in patients with spinal cord injury. Spinal Cord 2003; 41: 549–552.
Hansen RB, Biering-Sorenson F, Kristensen JK . Bladder emptying over a period of 10–45 years after a traumatic spinal cord injury. Spinal Cord 2004; 42: 631.
Perkash I . Laser sphincterotomy and ablation of the prostate using a sapphire chisel contact tip firing neodymium:YAG laser. J Urol 1994; 152: 2020.
Vapnek JM, Couillard DR, Stone AR . Is sphincterotomy the best management of the spinal cord injured bladder? J Urol 1994; 151: 961.
Fontaine E, Hajri M, Rhein F, Fakacs C, Le Mouel MA, Beurton D . Reappraisal of endoscopic sphincterotomy for post-traumatic neurogenic bladder: a prospective study. J Urol 1996; 155: 277–280.
McDiarmad SA, Arnold EP, Palmer NB, Anthony A . Management of spinal cord injured patients by indwelling suprapubic catheterisation. J Urol 1995; 154: 492–494.
Guy P, Grundy D (2002) Chapter 7, Urological management. In: Grundy D, Swain A (eds). ABC of Spinal Cord Injury 4th edn. BNJ Publishing Group: London, 33–40.
Sugimura T, Arnold E, English S, Moore J . Chronic suprapubic catheterisation in the management of patients with spinal cord injuries: analysis of upper and lower urinary tract complications. BJU Int 2008; 101: 1396–1400.
Dahlberg A, Perttilä I, Wuokko E, Ala-Opas M . Bladder management in persons with spinal cord lesion. Spinal Cord 2004; 42: 694–698.
Acknowledgements
The authors would like to thank the staff of the MCSI, in particular Mrs H Edwards and her administrative team, Mr A Osman and Mr J Chowdry, consultant surgeons in spinal injury; the consultants and members of staff of the radiology department, in particular Professor I McCall, Dr V Pullicino and Dr D Tyrrell, the body of staff and management of the RJ&AH Orthopaedic Hospital NHS Trust.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
This work is licensed under the Creative Commons Attribution-NonCommercial-No Derivative Works 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/3.0/
About this article
Cite this article
El-Masri(y), W., Chong, T., Kyriakider, A. et al. Long-term follow-up study of outcomes of bladder management in spinal cord injury patients under the care of The Midlands Centre for Spinal Injuries in Oswestry. Spinal Cord 50, 14–21 (2012). https://doi.org/10.1038/sc.2011.78
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2011.78
Keywords
This article is cited by
-
Bladder management in individuals with spinal cord injury or disease during and after primary rehabilitation: a retrospective cohort study
World Journal of Urology (2022)
-
Long-term bladder and bowel management after spinal cord injury: a 20-year longitudinal study
Spinal Cord (2018)
-
Bladder management in individuals with chronic neurogenic lower urinary tract dysfunction
Spinal Cord (2016)
-
Who decides? A qualitative study on the decisional roles of patients, their caregivers and doctors on the method of bladder drainage after spinal cord injury
Spinal Cord (2015)
-
Complications, secondary interventions and long term morbidity after en bloc sacrectomy
European Spine Journal (2015)
