
Abstract
Study design:
Retrospective, longitudinal analysis of motor recovery data from individuals with cervical (C4–C7) sensorimotor complete spinal cord injury (SCI) according to the International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI).
Objectives:
To analyze the extent and patterns of spontaneous motor recovery over the first year after traumatic cervical sensorimotor complete SCI.
Methods:
Datasets from the European multicenter study about SCI (EMSCI) and the Sygen randomized clinical trial were examined for conversion of American Spinal Injury Association (ASIA) Impairment Scale (AIS) grade, change in upper extremity motor score (UEMS) or motor level, as well as relationships between these measures.
Results:
There were no overall differences between the EMSCI and Sygen datasets in motor recovery patterns. After 1 year, up to 70% of subjects spontaneously recovered at least one motor level, but only 30% recovered two or more motor levels, with lesser values at intermediate time points. AIS grade conversion did not significantly influence motor level changes. At 1 year, the average spontaneous improvement in bilateral UEMS was 10–11 motor points. There was only moderate relationship between a change in UEMS and a change in cervical motor level (r2=0.30, P<0.05). Regardless of initial cervical motor level, most individuals recover a similar number of motor points or motor levels.
Conclusion:
Careful tracking of cervical motor recovery outcomes may provide the necessary sensitivity and accuracy to reliably detect a subtle, but meaningful treatment effect after sensorimotor complete cervical SCI. The distribution of the UEMS change may be more important functionally than the total UEMS recovered.
Similar content being viewed by others


Introduction
The International Campaign for Cures of spinal cord injury Paralysis (ICCP) recently provided support to a panel tasked with reviewing past spinal cord injury (SCI) clinical studies and making recommendations on the conduct of future trials. To date, four integrated SCI guidelines papers have been published addressing: spontaneous neurological recovery,1 clinical trial outcome measures,2 inclusion/exclusion and ethical criteria3 and clinical trial design.4
The selection of appropriate participants and the use of sensitive outcomes to track changing sensorimotor function are important considerations for the design of clinical trials capable of measuring a statistically and functionally meaningful treatment effect after SCI. The American Spinal Injury Association (ASIA) Impairment Scale (AIS), which forms part of the International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI), has been widely used for diagnosis and prognosis of SCI, and represents a toolbox of validated outcomes for use in forthcoming clinical trials (for review, see Furlan et al.5).
With additional support of the Spinal Cord Outcomes Partnership Endeavour (SCOPE), the present analysis focused on changes in spontaneous motor activity during the first year after sensorimotor complete (AIS-A) cervical (C4–C7) SCI. In collaboration with members of the European multicenter study for SCI (EMSCI), the original data from the Sygen multicenter trial6, 7, 8 was re-analyzed in conjunction with the more recent data from the EMSCI study (http://www.emsci.org). The purpose of this retrospective analysis of the Sygen and EMSCI databases was to build on the existing knowledge of spontaneous recovery after SCI1, 9, 10, 11, 12, 13, 14 by examining: (1) the extent of AIS grade conversions, (2) recovery of upper extremity motor score (UEMS), (3) changes in cervical motor level and (4) the degree of association between these measures. This data provides an opportunity for a more in-depth evaluation of changes in UEMS and/or motor level as effective clinical end points in early phase SCI studies.
Methods
Using the Sygen and EMSCI databases, a retrospective analysis was undertaken of AIS grade, UEMS and motor level during spontaneous recovery after sensorimotor complete cervical (C4–C7) SCI, according to the revised 2002 ISNCSCI assessment guidelines.15 Briefly, AIS grade and motor scores from the key muscles for the upper extremities (C5–T1) were determined at baseline (within 1-week after SCI) and for all subsequent AIS examinations performed over the first year after SCI. As the original analysis of the Sygen data, there have been revisions to the ISNCSCI assessment for determining AIS grade and motor level. To facilitate comparisons with the more recent EMSCI data, the original data from the Sygen study were re-scored. For a definition of motor level and examples of how changes in cervical motor score impacts motor level determination during recovery, see Table 1.
Original sources of data
European multicenter study about spinal cord injury (EMSCI)
Individuals in this ongoing prospective study (started 2001; current enrollment =1890), have sustained a traumatic SCI and are being recruited from 18 European centers for the observation of neurological (that is, AIS examination) and functional (for example, ambulation) outcomes during the first year after SCI, while receiving current standards of clinical care. Participants undergo an initial examination during the very acute period (∼1 week) after SCI, with follow-up assessments targeted at 4, 12, 24 and 48 weeks after SCI. Other findings from this database have been previously published.9, 16, 17, 18, 19, 20, 21 The mean (±s.d.) timing of initial and follow-up AIS examinations of the EMSCI individuals included in this study was 0.6±0.4, 4.4± 0.8, 12.0±1.1, 24.0±1.3 and 50.1±6.8 weeks after injury.
Sygen
The Sygen database (initial enrollment=797, followed=760) comprises traumatic SCI individuals enrolled between 1992 and 1997 in a randomized, double-blind, multicenter study to examine the therapeutic benefits of monosialotetrahexosylganglioside therapy.6, 8 To measure primary efficacy, the proportion of individuals recovering two modified Benzel grades (that is, ‘marked recovery’) in the monosialotetrahexosylganglioside treatment groups (low and high dose) was compared with the placebo control group. Initial assessments were conducted within 72 h of SCI to a clinical end point of 26 weeks after SCI. Interim and follow-up AIS examinations were performed at 4, 8, 16 and 52 weeks after SCI. The overall findings of this study were no significant differences in ‘marked recovery’ in either of the monosialotetrahexosylgangliosid treatment groups at 26 or 52 weeks when compared with the placebo control group.
Statistical analysis
Inclusion criteria
All individuals in the Sygen and EMSCI databases with sensorimotor complete (AIS-A) SCI and a motor level of C4–C7 at the baseline assessment (∼1 week from SCI) were included in the present analysis. C4 motor level SCI was determined based on the normal preservation of sensory function on the C4 dermatome. Individuals with an initial motor level of C8 or T1 were not included a priori as recovery of multiple motor levels within the upper extremities could not be tracked. As the recovery of UEMS and motor level were not primary end points in the Sygen study, a preliminary statistical analysis (described below) was performed to assess possible differences between treatment groups and the placebo control. No significant differences in the recovery of UEMS or the proportion of individuals (C5–C7) changing motor levels from baseline to any of the follow-up time points was observed in the treatment groups compared with the placebo control group (P<0.05).
Statistical procedures
For each initial motor level of SCI (C4, C5, C6 and C7), the statistical analysis of AIS grade, motor level (right and left side) and UEMS (right, left and sum of both sides) was performed separately for each database. An analysis of UEMS and motor level changes was also performed for the combined group of C5–C7 SCI patients; once again for each database and from baseline to different time points over the first year after SCI. As there is no key muscle delineating the C4 spinal segment, it is difficult to reliably track deterioration from an initial C4 motor level. Thus, these individuals were analyzed separately for changes in motor level and UEMS changes. However, individuals with an initial C4 motor level SCI were included in the combined analysis of motor level and AIS grade conversion from baseline (see Tables 2 and 3). All statistical analyses were conducted in SPSS (SPSS, Inc., Chicago, IL, USA, v. 16) and R (R foundation for Statistical Computing, v. 2.10.1, www.r-project.org).
Comparisons between and within databases were performed on the proportion of individuals converting an AIS grade or changing motor levels at 4 weeks (EMSCI and Sygen), 8 (Sygen) and 12 weeks (EMSCI), 12 (EMSCI) and 16 weeks (Sygen), 24 (EMSCI) and 26 weeks (Sygen), and 50 weeks (EMSCI and 52 (Sygen) after cervical SCI (χ2-test). The distribution of UEMS at baseline and at follow-up time points was examined for each initial cervical motor level of SCI. The normality of the UEMS distribution appeared to some extent dependent on the initial motor level of SCI and/or the time point examined. First, UEMS at early-time points (<12 weeks) was less normally distributed than at later assessment times. Second, initial C4 and C7 motor levels of SCI were also less normally distributed than baseline C5 and C6 motor levels of SCI.
Linear mixed effects models account for fixed and random subject effects by describing both the behavior of the entire sample related to a specific ‘fixed’ variable (for example, time) and those ‘random’ subject variables (for example, total UEMS), specifically associated with an individual.22 In the present study, linear mixed effects models were used to analyze repeated measures of UEMS within each database and to compare spontaneous UEMS recovery (that is, rate) between databases. In both statistical analyses, the main effect on UEMS (time) was modeled separately for each initial motor level (C4–C7). Random subject effects were modeled with repeated measure correlated variables (that is, diagonal repeated measures covariance structure). To compare spontaneous recovery between databases, UEMS was modeled with the natural-log of time. This process transforms an exponential (that is, motor recovery after SCI) to a linear function, thereby facilitating linear modeling. The slopes and intercepts of linear UEMS recovery were then compared between the same initial motor levels across databases. The slopes of UEMS recovery were further analyzed within databases, between different initial levels of cervical SCI. To account for the ordinal ranking and the non-normal distribution of manual muscle testing, UEMS changes over the first year after SCI were further examined with non-parametric statistics (between databases, Mann–Whitney U; within databases, Friedman test and post hoc Wilcoxon signed rank sum test).
The effect of initial motor level, AIS grade conversion and motor level changes on UEMS recovery at 1 year after SCI were examined by stepwise linear regression using combined datasets and combined cervical motor levels (C5–C7). Furthermore, the effect of AIS grade conversion on motor level changes was examined by ordinal regression (logit link function). Alpha (α) was set at 0.05, and all multiple pairwise comparisons were Bonferroni corrected (including multiple comparisons of time within each database for the analysis of initial motor level within a database).
Results
Subject demographics and SCI characteristics
Although the ratio of males to females was similar in both databases (Sygen, M=79.5%; EMSCI, M=78.8%), EMSCI individuals were older (43.7±18.7 years) at the time of injury compared with individuals in the Sygen database (31.2±12.5 years). The total number of individuals from both databases with cervical AIS-A SCI (C4–C8) at baseline was 426. The number of individuals for each initial cervical motor level, at each assessment time point, is shown in Table 4.
AIS grade conversion
The proportion of individuals converting from sensorimotor complete cervical SCI (C4–C7, AIS-A) to incomplete SCI (⩾AIS-B) was generally similar between databases, and was only significantly different for the 8- (Sygen) and 12-week (EMSCI) comparisons (χ2=8.34, P=0.003, see Table 2). In addition, at 16 weeks after SCI (Sygen database only) the proportion of individuals spontaneously converted from complete to incomplete SCI difference between initial motor levels of SCI (χ2=15.24, P=0.002). At this time point, 58.8% of (10 of 17) individuals with a C7 motor level SCI had converted to an incomplete AIS impairment grade, in contrast to 15.2% of C4, 23.1% of C5 and 28.6% of C6 motor levels.
Motor level recovery
The initial cervical motor level (C5–C7) indicated no preference for the right side or left side of the cord and was symmetrical in 79.6 and 76.1% of individuals in the EMSCI and Sygen databases, respectively. The proportion of AIS-A individuals with C5–C7 SCI deteriorating one or more motor levels (⩽−1), having a stable motor level (0) or recovering motor levels (+1 or ⩾+2) on the right side is shown in Figure 1.

Proportion of individuals with an initial C5–C7 motor level (right side) spontaneously deteriorating, remaining stable or gaining motor levels from baseline to different time points over the first year after cervical AIS-A SCI. The percentage of individuals in each category of motor level change or stability at one year after SCI is displayed on the right. ((a) Sygen; (b) EMSCI).
As a function of the initial cervical motor level of SCI, the proportion of individuals remaining stable or spontaneously changing motor levels is shown in Table 3. Only in the Sygen database, and only at 4 (χ2=46.25, P<0.001) and 8 weeks (χ2=32.97, P<0.001) after cervical SCI, was the proportion of individuals changing motor levels dependent on the initial motor level. This significant difference was transient and not present at later time points. The proportion of individuals with an initial C4 motor level who subsequently changed motor levels was not significantly different between databases at any time point after SCI.
UEMS
Based on the slopes and intercepts of the linear mixed models, there were no significant differences between databases in UEMS recovery for the same initial cervical motor level (right side motor level; see Supplementary Table 1 for model parameters). In neither database nor for all comparable recovery times was there a significant difference in the rate of UEMS recovery (slope of the linear model) based on the initial cervical motor level of SCI (all comparisons, P>0.05). Only the UEMS recovery (combined C5-C7) between 1 and 12 weeks (EMSCI) was significantly greater than 1 and 8 weeks time span for the Sygen study (Mann–Whitney U, P=0.003). Similarly, UEMS recovery was greater between 1 and 12 weeks in the EMSCI database when compared with 1 and 8 weeks in the Sygen database for individuals with C4 motor level SCI (Mann–Whitney U, P<0.01).
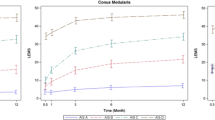
For each cervical motor level (C4, C5, C6 and C7), UEMS significantly increased from initial baseline to 1 year after SCI (P<0.001, Table 4 and Figure 2). In both databases, all pairwise comparisons of UEMS (C5–C7) from baseline to later time points (Table 5) were significant at each successive time point up to 26 weeks (P<0.05). However, only in the Sygen database did UEMS significantly increase between 26 and 52 weeks after SCI (P<0.001). Using non-parametric statistics the findings were similar; UEMS significantly recovered from 1 week after SCI to ∼1 year in both databases for all motor levels of SCI (Friedman's test, P<0.01). For combined cervical motor levels (C5–C7) in both databases, UEMS significantly increased at each successive time point up to 1 year after SCI (Wilcoxon rank, P<0.01).

UEMS during spontaneous recovery in the EMSCI and Sygen databases. (a–d), initial motor level of C4, C5, C6 and C7, respectively. (Error bars=95% confidence intervals).
Relationship between outcomes: AIS grade, UEMS and motor levels
The motor score and motor level determination were completed independently for each side of the cervical spinal cord. Unilateral values from only the same side of the cord were used to investigate relationships between UEMS and motor level. First, the initial cervical motor level was not a significant factor in UEMS recovery (P=0.237), and thus was automatically excluded by the stepwise regression model. Second, the UEMS change from baseline to ∼1 year after SCI was associated with a motor level change (P<0.001; Figure 3a). However, the relationship was only moderate (r2=0.30). Including AIS conversion in the stepwise regression model only improved r2 to 0.33 (P=0.006; Figure 3b). According to ordinal regression analysis, the initial cervical motor level (C5–C7, P>0.08) or AIS grade conversion (P=0.321) were not significant predictors of motor level changes.

UEMS change from baseline (∼1 week) to ∼1 year after SCI (EMSCI, 50 weeks; Sygen, 52 weeks) as a function of (a) motor level changes (right side) and (b) AIS grade conversion during this same time period (bilateral). (Combined databases and cervical motor levels, C5–C7).
Discussion
The purpose of this study was to examine the extent of spontaneous motor recovery in the upper extremities of individuals after traumatic sensorimotor complete (AIS-A) cervical SCI. Similar to previous reports,10 the majority of C4–C7 AIS-A individuals regained at least one motor level in the injured cervical cord within 1 year after SCI (Sygen=73.2%, EMSCI=57.6%). Of these individuals, a smaller proportion (∼30%) recovered two or more motor levels (Figure 1), which is a novel finding that was confirmed in both datasets. In all cases, the percentage recovering one or two motor levels was lower at intermediate time points that may be more relevant to the clinical end point for early phase acute SCI trials (for example, 18% for two motor levels at 16 weeks, Figure 1, Table 3). Although relatively rare in both databases (combined total, n=11, 4.6%), motor level deterioration was more prevalent after C6 or C7 SCI, but only at early intermediate time points (4–8 weeks).
The spontaneous recovery of UEMS at 1 year after cervical sensorimotor complete SCI (∼10–11 motor points bilaterally, Table 4) was similar to previously reported estimates of total motor score change.1, 2, 7, 12, 14 Interestingly, an individual with an initial C7 motor level SCI spontaneously recovers a similar number of motor points as an individual with an initial C5 motor level, despite having a smaller number of available cervical segments to recover motor function, and the reported lower inter-rater reliability for assessing caudal cervical myotomes (C8 and T1).23 Collectively, this suggests that spontaneous UEMS recovery: (1) occurs predominantly within the initial cervical motor level segment and/or within two spinal segments caudal to the initial motor level, and (2) is sufficiently robust to longitudinally track changes across all cervical myotomes (C5-T1), regardless of differences in psychometric properties.
In the present study, the typical recovery pattern was a rapid increase in motor scores from 1 week to 6 months, followed by a slower rate of change from 6 months to 1 year. This is similar to previous reports tracking motor recovery after sensorimotor complete cervical SCI.1, 2, 9, 10, 14 Nevertheless, it was notable that even a small increase in UEMS (∼2 points, Table 5) from 6 months to 1 year was accompanied by a marked increase in the proportion of individuals recovering additional motor levels.
The greatest proportion of spontaneous AIS grade conversions was evident at early time points (12 and 16 weeks, EMSCI and Sygen, respectively) when compared with the time course for UEMS and motor level changes. By 12 months after sensorimotor complete SCI, similar rates of AIS impairment grade conversion (20–30%, Table 2) were reported as in previous analyses of the EMSCI and Sygen databases.7, 17 The relatively large percentage (∼59%) of Sygen subjects with an initial C7 motor level SCI that undergo a conversion from AIS-A to incomplete SCI (⩾AIS-B) may be an effect due to the relatively small C7 sample size (at baseline, n=17). This large conversion from an AIS-A grade was not evident when there was a larger sample size (for example, initial motor level of C5 or C6, Table 4).
In general, the assessment of AIS grade conversion from sensorimotor complete (AIS-A) to an incomplete status (⩾AIS-B) is dependent on a number of variables, including: experience of the examiner, patient self-reports (for example, accurate sensory perception), measurement procedures (for example, anal sensory and/or motor assessment) and SCI comorbidities (for example, brain injury), all of which can collectively influence the accurate classification of SCI severity during the acute phase.24 Electrophysiological outcomes (for example, evoked potentials) and other novel strategies, such as biomarkers of SCI that correlate with injury severity,25 may help to accurately confirm the completeness of SCI, but these procedures are technically demanding.
In the present study, AIS grade conversion was only weakly related to an increase in UEMS at 1 year after SCI and not accompanied by greater motor level recovery (Figure 3b). This moderate relationship was likely the result of most individuals converting from cervical AIS-A to AIS-B (anal sensory recovery) or to a ‘limited’ AIS-C classification (anal motor recovery only).2, 17 It was not the intention of this paper to undertake a detailed analysis of changes in lower body motor recovery as they relate to specific AIS impairment grades. Nevertheless, our present study parallels previous findings, which found AIS grade conversion was not directly associated with an increase in the ‘number of muscles graded 3 or more’ (that is, a functional muscle score) in upper and/or lower extremities.17 Collectively, this suggests that the return of S4–S5 sensation (minimal criterion for incomplete AIS-B SCI) and the recovery of motor activity within individual spinal segments may not be mediated by the same underlying neural mechanisms.
A correlation between changes in UEMS with a change in motor level (that is, −1, 0, 1 and 2; Figure 3a) was not a surprising observation, given that cervical motor level is a function of the motor score in the upper extremities. However, a change in motor level cannot be reliably predicted by a change in the number of motor points (Figure 3a). The distribution of the UEMS may be more important functionally than the total UEMS recovered, including the pattern of recovery in preserved myotomes within the zone of partial preservation, which can influence motor level recovery (Kramer et al., unpublished observations).
Comparison of databases: EMSCI and sygen
As reported previously,1 using preliminary data from the EMSCI database, the similarities in motor changes between the EMSCI and Sygen studies indicates upper extremity motor outcomes are reproducible measures of spontaneous recovery after cervical sensorimotor complete SCI (AIS-A). At the intermediate time points of 8, 12 and 16 weeks after SCI, the differences in the proportion of individuals changing motor levels or converting AIS grade is most likely a function of the disparate examination times (the 12 week EMSCI data being intermediate between the Sygen data at 8 and 16 weeks, Table 3). This suggestion is supported by the similar data obtained from both databases at congruent assessment time points (for example, 4 weeks, 24/26 weeks and 50/52 weeks). The overall similarities are apparent even though EMSCI has less rigorous inclusion/exclusion criteria, including: age, surgery, variability in the time of assessments and more subjects dropping out at later assessment times (24 and 50 weeks after SCI, Table 4). Therefore, although the EMSCI protocol differs from the strict criteria of a randomized controlled trial (RCT), such as the Sygen trial, the similar patterns of motor recovery after cervical AIS-A SCI would appear to underscore the reliability of the recovery patterns and overcome any data collection differences.
Given the ∼10-year difference in the data collected by the two databases, it may seem disappointing that greater spontaneous recovery was not observed within the EMSCI database. Although more intensive surgical and rehabilitation efforts have been implemented in the interim, there has been little success in improving the neurological recovery after cervical AIS-A SCI. As the current viewpoint is that recent treatment advances have facilitated better recovery after incomplete SCI, further analysis should be undertaken to determine if upper and lower extremity motor recovery patterns following AIS-B–D cervical SCI are different between databases.
Implications for clinical trials
A fundamental question regarding clinical trials is which outcome measure will provide a sensitive and reliable end point for accurately measuring safety, as well as detecting a subtle treatment effect. However, it is difficult to develop optimal clinical trial protocols and clinical end points for a disorder, like SCI, that has yet to validate a treatment with a clear clinical benefit. Furthermore, as many neuroprotective and regenerative therapeutic studies will recruit individuals during the acute or sub-acute stage of SCI, the safety and efficacy of a therapeutic must be shown during a period of spontaneous neurological change. Therefore, achievable clinical end points can only be established if the natural history of neurological outcomes over the first year after SCI is known.
For therapies applied locally to the site of spinal injury, detecting proximal changes in adjacent spinal segments may be more sensitive than measuring an aggregate neurological change (that is, AIS grade conversion), especially for early phase clinical trials. AIS grade conversion is acceptable as a clinical end point, but only when the treatment effect is expected to be large.26 After cervical AIS-A SCI, our analysis indicates that change in AIS impairment grade is not accompanied by a consistent or predictable improvement in UEMS or motor level. The use of motor score subscales, that is, UEMS, has been suggested to improve the relationship of motor scores with functional outcomes.14 Thus, for individuals with sensorimotor complete cervical SCI, an improvement in UEMS or motor level may more readily detect a subtle therapeutic effect and could more accurately identify a meaningful clinically important difference (for example, improvement in hand function). The current data suggest that most of the increase in UEMS occurs within two spinal levels caudal to the initial motor level. Thus, for sensorimotor complete cervical SCI, UEMS may be an acceptable outcome measure for early phase trials (Table 4). In addition, a significant increase in the number of individuals exhibiting unchanged or deteriorating motor function could also be used as an indicator of an adverse neurological response to a therapeutic intervention (Figure 1).
Individuals with complete thoracic level injuries are often suggested as initial participants for early phase SCI studies, as any deleterious intervention is less likely to compromise functional capacity.18 As thoracic motor change is not measured by the ISNCSCI, the determination of a therapeutic gain or loss is difficult and is limited to a change in thoracic sensory dermatomes. Further analysis of thoracic AIS-A subjects from both EMSCI and Sygen databases is being undertaken to address these questions (Zariffa et al. unpublished observations).
For a treatment to be validated in later phase clinical trials (that is, pivotal phase III) an outcome measure must be directly related to an improved functional capacity. Although UEMS is related to the independent capacity for activities of daily living,27 motor level improvement is a more direct index of enhanced activities of daily living.18, 28 For example, an increase in nonfunctional muscle strength (motor score of 1–2) across a large number of key muscles (representing specific cord segments) would not be as beneficial as an increase in functional muscle strength (motor score ⩾3) across a smaller number of contiguous cervical cord segments. The recovery of at least one motor level after sensorimotor complete cervical SCI is so frequent that detecting a statistically significant difference between a treatment and control group would require a very large study population (see below). A better metric (with more reasonable sample sizes) might rely on the percentage of individuals showing an increase of two or more motor levels in response to a therapeutic intervention.
Sample size calculations
We have used the present data to generate illustrative sample calculations of the number of participants that would have to be enrolled to a clinical study using UEMS or change in motor levels as clinical end points. Sample size calculations can be accomplished using a myriad of different formulae. Briefly, we used tests of equality for a two-sample, parallel-designed study; including a test of proportions29 and comparison of means.30 Sample sizes were calculated for individuals with C5–C7 SCI, based on the recovery of either mean UEMS or two motor levels from baseline to ∼1 year after SCI (50 and 52 weeks, EMSCI and Sygen, respectively). We used 80% power (β=0.2) for detecting a clinically meaningful difference and α=0.05. The numbers of subjects required to be enrolled in the treatment and control groups (equal allocation) for varying treatment effect sizes are shown in Figure 4. Nevertheless, there are a number of factors that can influence power calculations, including the heterogeneity of the study population and the size of the postulated treatment effect.3 The disparity between the number of subjects required to demonstrate a significant effect using motor score compared with motor levels may be, in part, be explained by the demand for motor level changes to have functional improvement of motor points (⩾3/5) over contiguous spinal segments (described above).

Example of sample size calculations to demonstrate a significant change in either UEMS (a) or recovery of two motor levels (b) from baseline to ∼1 year after SCI (β=0.2, α=0.05, equal allocation of subjects to treatment and control groups). Note: effect size based on the mean spontaneous UEMS increase or two motor level improvement ∼1 year after SCI in combined databases and cervical motor levels (C5–C7).
Study limitations
As with many retrospective analyses, the accuracy of the data from each subject cannot be verified, but the relatively large sample size of the datasets overcomes much of the possible variability. Given the standard of care after SCI (for example, surgery and timing of surgery, as well as rehabilitation training) may influence outcomes, including spontaneous neurological recovery, it is possible that non-uniform treatment can also influence the data. However, the Sygen study was completed in a rigorous manner, using an RCT protocol that limited confounding variables, but still had similar motor outcomes as the EMSCI database for cervical sensorimotor complete SCI. Future studies should be specifically designed to address these questions.
Conclusion
Over the entire course of a clinical trial program, complete validation of a therapeutic as safe and beneficial is likely to require a comprehensive ‘toolbox’ of outcome measures, including: electrophysiological, neurological, neuroimaging, autonomic, pain, functional outcome and quality of life tools.2 Many proposed therapeutic interventions are likely to involve the local infusion of a drug or transplantation of cells at or near the site of SCI. It is reasonable to suggest that the principal activities of these types of treatments, however modest, will be most readily apparent in spinal segments adjacent to the administered therapeutic agent and facilitating an endogenous neural substrate of repair or recovery. Thus, in early phase studies, careful tracking of motor scores in the upper limbs may provide the necessary sensitivity and accuracy to reliably detect a subtle, but statistically significant treatment effect after cervical SCI. Nevertheless, the distribution of the UEMS may be more important than the total UEMS recovered and therefore, the derivation of motor levels, from motor scores, might provide a surrogate clinical end point that is linked to functional capacity and predict a clinically meaningful important difference in a pivotal phase III trial.31
References
Fawcett JW, Curt A, Steeves JD, Coleman WP, Tuszynski MH, Lammertse D et al. Guidelines for the conduct of clinical trials for spinal cord injury as developed by the ICCP panel: spontaneous recovery after spinal cord injury and statistical power needed for therapeutic clinical trials. Spinal Cord 2007; 45: 190–205.
Steeves JD, Lammertse D, Curt A, Fawcett JW, Tuszynski MH, Ditunno JF et al. Guidelines for the conduct of clinical trials for spinal cord injury (SCI) as developed by the ICCP panel: clinical trial outcome measures. Spinal Cord 2007; 45: 206–221.
Tuszynski MH, Steeves JD, Fawcett JW, Lammertse D, Kalichman M, Rask C et al. Guidelines for the conduct of clinical trials for spinal cord injury as developed by the ICCP panel: clinical trial inclusion/exclusion criteria and ethics. Spinal Cord 2007; 45: 222–231.
Lammertse D, Tuszynski MH, Steeves JD, Curt A, Fawcett JW, Rask C et al. Guidelines for the conduct of clinical trials for spinal cord injury as developed by the ICCP panel: clinical trial design. Spinal Cord 2007; 45: 232–242.
Furlan JC, Fehlings MG, Tator CH, Davis AM . Motor and sensory assessment of patients in clinical trials for pharmacological therapy of acute spinal cord injury: psychometric properties of the ASIA Standards. J Neurotrauma 2008; 25: 1273–1301.
Geisler FH, Coleman WP, Grieco G, Poonian D . The Sygen multicenter acute spinal cord injury study. Spine (Phila Pa 1976) 2001; 26 (24 Suppl): S87–S98.
Geisler FH, Coleman WP, Grieco G, Poonian D . Measurements and recovery patterns in a multicenter study of acute spinal cord injury. Spine (Phila Pa 1976) 2001; 26 (24 Suppl): S68–S86.
Geisler FH, Coleman WP, Grieco G, Poonian D . Recruitment and early treatment in a multicenter study of acute spinal cord injury. Spine (Phila Pa 1976) 2001; 26 (24 Suppl): S58–S67.
Curt A, van Hedel HJ, Klaus D, Dietz V . Recovery from a spinal cord injury: significance of compensation, neural plasticity, and repair. J Neurotrauma 2008; 25: 677–685.
Ditunno Jr JF, Cohen ME, Hauck WW, Jackson AB, Sipski ML . Recovery of upper-extremity strength in complete and incomplete tetraplegia: a multicenter study. Arch Phys Med Rehabil 2000; 81: 389–393.
Mange KC, Ditunno Jr JF, Herbison GJ, Jaweed MM . Recovery of strength at the zone of injury in motor complete and motor incomplete cervical spinal cord injured patients. Arch Phys Med Rehabil 1990; 71: 562–565.
Waters RL, Adkins RH, Yakura JS, Sie I . Motor and sensory recovery following complete tetraplegia. Arch Phys Med Rehabil 1993; 74: 242–247.
Waters RL, Adkins RH, Yakura JS, Sie I . Motor and sensory recovery following incomplete tetraplegia. Arch Phys Med Rehabil 1994; 75: 306–311.
Marino RJ, Ditunno Jr JF, Donovan WH, Maynard Jr F . Neurological recovery after traumatic spinal cord injury: data from the Model Spinal Cord Injury Systems. Arch Phys Med Rehabil 1999; 80: 1391–1396.
American Spinal Injury Association. Reference Manual of the International Standards for Neurological Classification of Spinal Cord Injury. American Spinal Injury Association: Chicago, IL, 2003 (www.asia-spinalinjury.org).
Jakob W, Wirz M, van Hedel HJ, Dietz V . Difficulty of elderly SCI subjects to translate motor recovery—‘body function’—into daily living activities. J Neurotrauma 2009; 26: 2037–2044.
Spiess MR, Muller RM, Rupp R, Schuld C, van Hedel HJ . Conversion in ASIA impairment scale during the first year after traumatic spinal cord injury. J Neurotrauma 2009; 26: 2027–2036.
van Hedel HJ, Curt A . Fighting for each segment: estimating the clinical value of cervical and thoracic segments in SCI. J Neurotrauma 2006; 23: 1621–1631.
van Hedel HJ, EMSCI Study Group. Gait speed in relation to categories of functional ambulation after spinal cord injury. Neurorehabil Neural Repair 2009; 23: 343–350.
van Hedel HJ, Dietz V . Walking during daily life can be validly and responsively assessed in subjects with a spinal cord injury. Neurorehabil Neural Repair 2009; 23: 117–124.
Wirth B, van Hedel HJ, Kometer B, Dietz V, Curt A . Changes in activity after a complete spinal cord injury as measured by the Spinal Cord Independence Measure II (SCIM II). Neurorehabil Neural Repair 2008; 22: 279–287.
Pinheiro JC, Bates DM . Linear Mixed Effects Models. Mixed Effects Models in S and S-Plus. Springer Verlag: New York, 2000.
Savic G, Bergstrom EM, Frankel HL, Jamous MA, Jones PW . Inter-rater reliability of motor and sensory examinations performed according to American Spinal Injury Association standards. Spinal Cord 2007; 45: 444–451.
Burns AS, Lee BS, Ditunno Jr JF, Tessler A . Patient selection for clinical trials: the reliability of the early spinal cord injury examination. J Neurotrauma 2003; 20: 477–482.
Kwon BK, Stammers AM, Belanger LM, Bernardo A, Chan D, Bishop et al. Cerebrospinal fluid inflammatory cytokines and biomarkers of injury severity in acute human spinal cord injury. J Neurotrauma 2010; 27: 669–682.
Blight AR, Tuszynski MH . Clinical trials in spinal cord injury. J Neurotrauma 2006; 23: 586.
Rudhe C, van Hedel HJ . Upper extremity function in persons with tetraplegia: relationships between strength, capacity, and the spinal cord independence measure. Neurorehabil Neural Repair 2009; 23: 413.
Bromley I . Functional Independence. Tetraplegia and Paraplegia: A guide for physiotherapists, 6th edn. Elsevier: Philadelphia, PA, USA, 2006, p 397.
Shao J, Wang H, Chow SC . Large Sample Tests for Proportions. Sample Size Calculations in Clinical Research, Second ed. edited by S. C. Chow Chapman and Hall, Boca Raton, FL, 2008, pp 83–115.
Shao J, Wang H, Chow SC . Comparing Means. Sample Size Calculations in Clinical Research, Second ed. edited by S. C. Chow Chapman and Hall, Boca Raton, FL, 2008, pp 49–81.
Ditunno JF . Outcome measures: evolution in clinical trials of neurological/functional recovery in spinal cord injury. Spinal Cord 2010; 48: 674–684.
Acknowledgements
The support of ICCP (http://www.campaignforcure.org) and SCOPE (http://www.scopesci.org) is gratefully acknowledged. We are grateful for the constructive suggestions of José Zariffa. John Kramer is a doctoral trainee of the Canadian Institute of Health Research and Michael Smith Foundation for Health Research. EMSCI is supported by the International Foundation for Research in Paraplegia, Zürich, Switzerland (IFP, Zurich).
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Supplementary information
Rights and permissions
About this article
Cite this article
Steeves, J., Kramer, J., Fawcett, J. et al. Extent of spontaneous motor recovery after traumatic cervical sensorimotor complete spinal cord injury. Spinal Cord 49, 257–265 (2011). https://doi.org/10.1038/sc.2010.99
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2010.99
Keywords
This article is cited by
-
Pharmacological management of acute spinal cord injury: a longitudinal multi-cohort observational study
Scientific Reports (2023)
-
Segmental motor recovery after cervical spinal cord injury relates to density and integrity of corticospinal tract projections
Nature Communications (2023)
-
Clinical translation of stem cell therapy for spinal cord injury still premature: results from a single-arm meta-analysis based on 62 clinical trials
BMC Medicine (2022)
-
Spontaneous Motor Recovery after Cervical Spinal Cord Injury: Issues for Nerve Transfer Surgery Decision Making
Spinal Cord (2022)
-
A taxonomy for consistent handling of conditions not related to the spinal cord injury (SCI) in the International Standards for Neurological Classification of SCI (ISNCSCI)
Spinal Cord (2022)
