
Abstract
Study design:
Autopsy cases of isolated spinal neurosarcoidosis are extremely rare or none.
Objectives:
To report an autopsy case of isolated spinal neurosarcoidosis without the involvement of other organs.
Summary of Background data:
A few reports of isolated spinal neurosarcoidosis are present, but no autopsy cases of isolated spinal neurosarcoidosis are present in the English literature.
Setting:
Japan.
Methods:
An autopsy case of isolated spinal neurosarcoidosis was examined pathologically.
Results:
A 54-year-old woman was admitted to our hospital because of leg numbness and muscle weakness. Imaging modalities showed an irregular contour and a mass-like lesion in the spinal cord. No biopsies were performed. Clinical diagnoses were suspected sarcoidosis and malignant lymphoma. The patient was treated by steroids and anti-cancer drugs, but she suddenly died of unknown cause. An autopsy revealed fibrosis and non-caseating granulomata in the spinal cord. No acid-fast bacteria or fungi were recognized by special stains. A PCR revealed no acid-fast bacteria including tuberculosis. Other organs including the brain and lung showed no sarcoidosis lesions. A pathological diagnosis of isolated spinal neurosarcoidosis was made. Other pathological diagnoses were systemic congestion, lung emphysema, food impaction in the upper esophagus and larynx, cardiac hypertrophy and marked dilation of the colon. The cause of death was thought to be respiratory failure.
Conclusion:
We have reported a very rare autopsy case of isolated spinal neurosarcoidosis, with an emphasis on pathological findings.
Similar content being viewed by others


Introduction
Sarcoidosis is a multisystem granulomatous disease of unknown pathogenesis. Neurosarcoidosis occurs in 5–10% of patients with sarcoidosis.1, 2, 3 Neurosarcoidosis occurs preferentially in the brain.1, 2, 3 Spinal neurosarcoidosis is relatively rare compared with brain neurosarcoidosis.1, 2, 3 In addition, isolated spinal neurosarcoidosis sparing other organs is very rare.4, 5, 6 Furthermore, autopsy cases of isolated spinal sarcoidosis are extremely rare or none. The author herein reports an autopsy case of isolated spinal neurosarcoidosis with an emphasis on pathological findings.
Case report
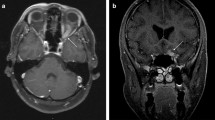
A 54-year-old woman was admitted to our hospital because of leg numbness and muscle weakness. A blood laboratory test revealed no significant changes. Her angiotensin-converting enzyme level was within the normal range. A systemic positron emission tomography scan showed dense signals in the spinal cord as well as in the body. Imaging modalities including magnetic resonance imaging showed an irregular contour of the spinal cord and perispinal tumor-like shadows (Figure 1). A tentative diagnosis of neurosarcoidosis was made, and the patient was treated by steroids. Further imaging modalities showed a mass-like lesion in the cervical spinal cord (Figure 1); the lesion was suspected to be malignant lymphoma and the patient was treated by chemotherapy. However, no biopsies were performed. During the scrutiny of lymphoma and sarcoidosis, the patient died suddenly of unknown cause. An autopsy was performed.

MRI of the spinal cord. The perispinal cord areas show a marked tumor-like shadow. It is particularly prominent in the cervical spine and medulla oblongata.
The autopsy revealed irregular patch-like thickenings of the leptomeninges of the entire spinal cord (Figure 2a). A mass-like lesion measuring 22 × 20 × 18 mm3 was recognized in the cervical spine (Figure 2b). The cut surface of the lesion showed thickened leptomeningeal lesions (Figure 2c). The entire spiral cord was examined histologically. The mass-like lesion and patch-like lesions were fibrosis with mild lymphocytic infiltrations (Figures 3a and b). Non-caseating epithelioid granulomata with Langhans giant cells were scattered (Figure 3c). The granulomata were also recognized in the medulla of the spinal cord. The perispinal nerves were entrapped in the fibrosis (Figure 3d). Special stains including Ziehl-Neelsen, Grocott and Gram revealed no acid-fast bacteria, fungi and Gram-positive bacteria. PCR for acid-fast bacteria including tuberculosis showed negative results. The sarcoid lesions were not present in other organs including the brain and lung. No malignant lymphoma was recognized. Therefore, isolated spinal neurosarcoidosis was diagnosed. Other pathological diagnoses were systemic congestion, lung emphysema, food impaction in the upper esophagus and larynx, cardiac hypertrophy, and marked dilation of colon. The case of death was thought to be acute respiratory failure due to food impaction.

Macroscopic findings of isolated spinal neurosarcoidosis. (a) The spinal cord shows white, slightly elevated patch-like lesions. (b) A mass-like formation (arrow) is recognized in the cervical spinal cord. (c) The cut surface shows leptomeningeal and spinal thickening.

Microscopic findings of isolated spinal neurosarcoidosis. (a) The leptomeninges of the spinal cord (upper) show marked fibrosis (lower). Hematoxylin–eosin (HE), × 20 (b) The fibrosis is accompanied by mild lymphocytic infiltration. The left upper part is the spinal cord. HE, × 100 (c) Non-caseating granuloma (center) with Langhans giant cells (upper left) are scattered. HE, × 200. (d) Nerves (center) are entrapped in the fibrosis. HE, × 200.
Discussion
The presence of non-caseating granuloma is essential for the diagnosis of sarcoidosis. In addition, other granuloma-forming diseases such as tuberculosis and fungal diseases should be excluded in making the diagnosis of sarcoidosis. In the present study, non-caseating granulomata were present in the spinal cord, and no stainable bacteria and fungi were identified. In addition, the PCR technique revealed no acid-fast bacteria including tuberculosis. Thus, the diagnosis of sarcoidosis is confirmative in the present case.
In general, sarcoidosis affects lungs and lymph nodes. Neurosarcoidosis is recognized in 5–10% of cases of systemic sarcoidosis.1, 2, 3 Neurosarcoidosis without the involvement of other organs is very rare.1, 2, 3 The present case was isolated spinal neurosarcoidosis, which is an extremely rare condition.4, 5, 6 In addition, autopsy cases of such spinal isolated neurosarcoidosis were extremely rare or none.
In neurosarcoidosis, mass formations are occasionally recognized clinically.6 In the present case also, a mass-like lesion was noted in the cervical spine, and clinically was suspected to be malignant lymphoma. In neurosarcoidosis, biopsies were occasionally difficult because of the lesional locations, as in the present case.
In the present study, the spinal lesions showed extensive fibrosis with mild lymphocytic infiltrations. These appearances are considered to be influenced by steroids and anti-cancer chemotherapy. It is highly possible that numerous non-caseating granulomata were present before the chemotherapy, which diminished the granulomata and led to fibrosis.
In summary, wehave reported a very rare autopsy case of isolated spinal neurosarcoidosis with an emphasis on pathological findings.
References
Lower EE, Weiss KL . Neurosarcoidosis. Clin Chest Med 2008; 29: 475–492.
Hoitsma E, Fabrer CG, Drent M, Sharma OP . Neurosarcoidosis: a clinical dilemma. Lancet Neurol 2004; 3: 397–407.
Vinas FC, Rengachary S . Diagnosis and management of neurosarcoidosis. J Clin Neurosci 2001; 8: 505–513.
Randeva HS, Davidson R, Chamoun V, Bouloux PM . Isolated neurosarcoidosis-a diagnostic emigma: case report and discussion. Endcrine 2002; 17: 241–247.
Schaller B, Kruschat T, Schmidt H, Bruck W, Buchfelder M, Ludwig HC . Intradural, extramedullary spinal sarcoidosis: report of a case and review of the literature. Spine J 2006; 6: 204–210.
Veras L, Utz JP, Houser OW . Sarcoidosis presenting as a central nervus system mass lesion. Chest 1997; 111: 518–521.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Terada, T., Shigeno, K., Hori, M. et al. Isolated spinal neurosarcoidosis: an autopsy case. Spinal Cord 48, 776–778 (2010). https://doi.org/10.1038/sc.2010.18
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2010.18
Keywords
This article is cited by
-
Benign myelitis as a first presentation of systemic sarcoidosis: importance of early diagnosis and treatment
Acta Neurologica Belgica (2013)
