
Abstract
Study design:
A randomized, double-blind, placebo-controlled, crossover, multicenter trial. A 1-week baseline period was followed by two treatment periods of 5 weeks duration with levetiracetam increased from 500 mg b.i.d. to a maximum of 1500 mg b.i.d. separated by a 1-week washout period.
Objectives:
The objective of the study was primarily to evaluate the efficacy of the anticonvulsant levetiracetam in patients with spinal cord injury (SCI) at- and below-level pain and secondarily to evaluate the effect on spasm severity.
Setting:
Outpatients at two spinal cord units and a pain center.
Methods:
Patients were allowed to continue their usual pain treatment at a constant dose. The primary outcome measure was the change in median daily pain score (on a 0–10 point numeric rating scale) from 1-week baseline period to the last week of each treatment period. Secondary outcome measures included pain relief of at- and below-level pain, allodynia, spasms and spasticity.
Results:
A total of 36 patients with SCI at- and or below-level pain were enrolled. Of these, 24 patients completed the trial. We found no effect of levetiracetam on the primary (P=0.46) or any of the secondary outcome measures. Only two patients continued levetiracetam treatment following the trial, and one patient was still in levetiracetam treatment at the 6-month follow-up. Levetiracetam was generally well tolerated with no serious adverse events.
Conclusions:
Levetiracetam does not relieve neuropathic pain or spasm severity following spinal cord injury.
Similar content being viewed by others

Introduction
Chronic neuropathic pain is a significant problem following spinal cord injury (SCI). Approximately 40–50% of patients with SCI suffer from neuropathic pain, which often has a substantial impact on their quality of life.1, 2, 3, 4, 5, 6 The anticonvulsants pregabalin and gabapentin and the tricyclic antidepressant amitriptyline have been shown to relieve neuropathic pain in some patients with SCI,7, 8, 9, 10 but many patients fail to achieve relief and continue to suffer from pain despite treatment attempts.11, 12 Neuropathic pain felt below the level of injury, referred to as below-level pain, is a central pain likely to have different mechanisms than neuropathic pain felt at the level of injury.13
Levetiracetam, the S-enantiomer of α-ethyl-2-oxo-1-pyrrolidine acetamide, is a novel antiepileptic drug indicated as monotherapy in the treatment of partial onset seizures with or without secondary generalization in patients with newly diagnosed epilepsy and as adjunctive therapy in the treatment of myoclonic seizures and primary generalized tonic-clonic seizures. Levetiracetam binds to a synaptic vesicle protein SV2A in the brain and spinal cord and is thought to act by inhibiting presynaptic neurotransmitter release.14, 15, 16 In animal models of peripheral neuropathic pain, levetiracetam has been shown to induce antinociceptive effects.17, 18, 19 In experimental human pain models, levetiracetam increased pain tolerance thresholds but had no effect on temporal pain summation.20 An open-label study and case reports suggest efficacy of levetiracetam in postherpetic neuralgia,21 painful polyneuropathy,22 neoplastic plexopathies23 and central neuropathic pain and spasms in multiple sclerosis.24 Levetiracetam has a favorable adverse effect profile with no known clinically relevant pharmacokinetic interactions.25
The present study examined the efficacy of levetiracetam in neuropathic pain following SCI in a randomized, double-blind, placebo-controlled trial and furthermore evaluated its effect on spasms and spasticity. Parts of the article has been presented in abstract form previously.26
Methods
Patients
Patients were recruited from December 2005 to March 2008 from the two spinal cord units in Denmark and the pain clinic at Aarhus University Hospital. The study was approved by the local ethical committees (no. 2005-0135), the Danish Data Protection Agency, Copenhagen, Denmark (no. 2005-41-5546) and the Danish Medicines Agency, Copenhagen, Denmark (no. 2612-2919). The study was registered in the European Clinical Database (EudraCT no. 2005-003171-21) and in the database ClinicalTrials.gov. The study was carried out in accordance with the International Conference on Harmonization Good Clinical Practice (GCP) guidelines and monitored by the GCP unit of the University of Aarhus, and all patients gave informed written consent. Patients aged ⩾18 years with at- and/or below-level neuropathic pain for at least 3 months due to trauma or disease of the spinal cord or cauda equina with a median pain intensity ⩾4 on a 0–10 point numeric rating scale (NRS) during a 1-week baseline period were eligible for the study. Neuropathic pain was defined as chronic pain in an area of sensory abnormality corresponding to the spinal cord or nerve root lesion, and the pain should have no primary relation to movement, inflammation or other local tissue damage. Below-level pain was defined as neuropathic pain present more than three dermatomes below the neurological level and at-level pain as pain located within the dermatome at and three dermatomes below the neurological level.27 Patients were excluded for any of the following reasons: known concomitant cerebral damage, pregnancy or lactation, alcohol or substance abuse, hypersensitivity to levetiracetam or pyrrolidine derivates, epilepsy, psychiatric disease, depression, severe liver disease or impaired renal function. Patients taking antidepressants were slowly tapered off during a prestudy period of at least 1 week before the baseline period. Concomitant treatment with spasmolytics (baclofen and tizanidine), gabapentin, pregabalin, opioids and simple analgesics (nonsteroid anti-inflammatory drugs, paracetamol or acetylsalicylic acid) for pain was allowed in a constant and unchanged dose during the trial.
Study design
The study was designed as a randomized, double-blind, placebo-controlled, crossover, multicenter trial. The study was carried out at the Danish Pain Research Center, University of Aarhus, the Spinal Cord Unit, Viborg Hospital, and the Clinic for Spinal Cord Injuries, the Neuroscience Centre, Rigshospitalet, Denmark. At the baseline visit, a medical history and a full neurological and physical examination were obtained. Pain patients completed the Danish version of the McGill pain questionnaire.28, 29 Spinal lesions were classified according to the International Standards for Neurological Classification of Spinal Cord Injury.30 A 1-week baseline period was followed by two 5-week treatment periods with levetiracetam or identical placebo tablets, separated by a 1-week washout period. Tablets containing 500 mg were administered as two divided doses. The dose was gradually increased from 500 mg × 2 in the first week to 1000 mg × 2 in the second week and 1500 mg × 2 in weeks 3–5. Patients were permitted to reduce the final dose to 2000 or 2500 mg daily if they experienced unacceptable adverse events, but the final dose had to be at least 2000 mg and continued for at least 2 weeks to complete the trial. In this case, the last observation carried forward was used. Three further visits were scheduled: at the end of the baseline week and at the end of each treatment period. Drug compliance was monitored by counting unused tablets. After the end of the trial, the patients were offered to start levetiracetam treatment and all patients were sent a small questionnaire for 6-month follow-up. The questionnaire was returned to a research nurse, who was not involved in the study, and sent to the primary investigator after completion of the enrollment. Paracetamol up to 6 tablets of 500 mg daily was used as escape medication.
Assignment to treatment sequence was randomized by a computer-generated randomization list with a block size of 4 and a consecutive allocation of patients as they entered the study in each of the three centers. A pharmacist in the hospital pharmacy who did not participate in conduct of the trial generated the randomization plan. The three investigators were provided with sealed code envelopes, one for each patient, containing information on the treatment given, and the envelopes were returned unopened to the monitor after study termination.
Outcome measures
Patients were asked to rate their pain in the morning by indicating the number that best described their pain on average in the last 24 h from 0 (no pain) to 10 (worst imaginable pain) and sleep interference from 0 (no interference) to 10 (worst imaginable interference) using a pain diary. The predefined primary outcome measure was the change in median daily pain score from the baseline week to the last week of treatment. The predefined secondary outcome measures were the following: (1) pain relief for overall, at-level and below-level pain (complete, good, moderate, slight, none or worse); (2) number of patients with 33% pain relief; (3) sleep interference; (4) use of escape medication; (5) change in specific pain symptoms evaluated using the Neuropathic Pain Symptom Inventory;31 (6) effect on evoked pain: brush-evoked allodynia (pain) or dysesthesia (unpleasantness), cold allodynia or dysesthesia (evoked by a thermal roll of 20 °C and an acetone droplet) and pinprick hyperalgesia (evoked by bending a von Frey hair no. 5.88, bending force 75.9 g per 745 mN, Semmes-Weinstein monofilaments; Stoelting, Wood Dale, IL, USA) measured on the NRS (0–10); (7) patient global impression of change; (8) comparison of number of responders in the group with and without allodynia and (9) spasm intensity and severity assessed by the patient using the NRS (0–10) and the Penn Spasm Frequency Scale,32 and spasticity assessed by the investigator using the modified Ashworth scale over knee joints.33 The baseline physical examination was carried out by one of five experienced physicians who also (in addition to one study nurse) performed the evaluations of pain outcome measures, which were carried out using the same equipment and standardized instructions to the patients. All personnel involved were trained by the same investigator (NBF)
Other measurements
Adverse events were assessed using open-ended questions at each visit, and blindness was assessed by asking the patients and treating researchers which treatment sequence they believed they received and the reason for this.
Statistics
Differences in baseline data between the study population and withdrawn patients were tested using t-test or Fisher's exact test. Analyses were made on patients who achieved at least 2000 mg per day levetiracetam or the corresponding placebo for at least 2 weeks in each period (study population) and with a compliance of tablet counts of at least 70%. For the pain intensity scoring in the pain diary, the last observation carried forward method was used to account for early discontinuation; other missing data were not replaced. A responder was defined as a patient with a 33% pain reduction (from median daily pain during the baseline week to the median daily pain during the last week of treatment). Differences in treatment effect between patients with or without concomitant pain treatment was evaluated with Mann–Whitney U-test. Differences between treatments were evaluated by Kock's adaptation of the Wilcoxon signed-rank test and the Mainland–Gart test for dichotomized data. All P-values given are two tailed. P<0.05 was considered statistically significant. Considering a between-treatment group difference in pain score of at least 1.5 on the 0–10 NRS as clinically relevant and a standard deviation of 2.5,34 30 patients were expected to be sufficient to obtain a statistical power greater than 90% (α=0.05). With a sample size of 24, the power of the study was 85% to detect a 1.5-point difference.
Results
Patients
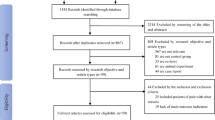
A total of 38 patients were screened and 36 randomized in the study. Of these, 2 patients dropped out before randomization because they could not be tapered out of escitalopram and amitriptyline treatment, respectively. Also, 12 patients dropped out after randomization (Figure 1) and 24 patients achieved at least 2000 mg per day for at least 2 weeks without major protocol violation, and these comprise our study population. The study population includes one patient who took morphine and codeine for a short time in the middle of the placebo period as the patient underwent hemorrhoidectomy. Clinical characteristics of the patients are summarized in Table 1. The withdrawn patients and the study population did not differ in these characteristics, but there was a tendency that withdrawn patients were more often treated with concomitant pain medications (11/12 versus 14/24, P=0.059, Fisher's exact test). In the study population, 15 patients had evoked pain, 7 patients at-level, 3 below-level and 5 both at- and below-level pain. Of 12 withdrawn patients, 8 had evoked pain. The most common pain descriptors chosen from the McGill pain questionnaire among the 24 patients completing the trial were pricking/boring (18 patients), shooting (15), tingling (14) and burning (11), whereas grueling (13), agonizing (11), annoying (10) and blinding (10) were the most common affective descriptors.

Study flow diagram.
Of the study population, four patients discontinued treatment early; three patients completed only 4 weeks of levetiracetam treatment and one patient completed 4 weeks of placebo treatment (P=1.0, Mainland–Gart test). During levetiracetam treatment, 21 patients reached the maximum dosage and 3 patients received 2000 mg per day, whereas 23 patients received the maximum dose during placebo treatment (P=1.0, Mainland–Gart test).
Compliance
The mean compliance by tablet count was 97.7% (s.d. 7.2) in the levetiracetam period and 97.9% (s.d. 4.4) in the placebo period.
Primary outcome measure
There was no difference in the median pain intensity during levetiracetam and placebo treatment (P=0.46, Kock's adaptation of the Wilcoxon signed-rank test) (Table 2, Figure 2).

Pain intensity scores at baseline (gray box) and each week during levetiracetam (diagonal lines) and placebo treatment (white boxes). Boxes represent medians with 25th and 75th percentiles; error bars, 10th and 90th percentiles.
Secondary outcome measures
Levetiracetam did not significantly change any of the secondary end-points (Table 2, Figure 3). Of 20 patients, 3 during levetiracetam and 1 during placebo reported at least moderate pain relief of their below-level pain whereas these figures were 2 during levetiracetam and 1 during placebo of 13 patients with at-level pain. One patient in each treatment phase obtained 50% pain relief whereas three in levetiracetam and four in placebo treatment obtained 33% pain relief (responders, nonsignificant differences). Two of the three responders to levetiracetam also reported pain relief, but neither wished to continue treatment due to side effects, although one later tried levetiracetam in a lower dose without success. Of the three responders, two had evoked pain, one with slight mechanical and cold allodynia, which was not consistently relieved by levetiracetam, and one with acetone-evoked dysesthesia, which was completely relieved by levetiracetam. Two patients wished to start levetiracetam treatment following the end of the study: one of these because of pain relief and slight side effects in one period, which turned out to be the placebo period. The other patient felt an increase in pain following termination of the study drug (levetiracetam) in period one, although no pain relief was reported at visit 3. The first patient still reported pain relief from levetiracetam after 6 months, whereas the second patient terminated treatment after 2 months due to tiredness. There was no difference in pain reduction during levetiracetam treatment between patients treated with concomitant pain medication (n=14) and patients without concomitant pain medication (n=10) (P=0.55, Mann–Whitney U-test) or between patients treated with gabapentin and/or pregabalin (n=9) and patients without gabapentin/pregabalin treatment (n=15) (P=0.95, Mann–Whitney U-test).

Patient global impression of change. Number of patients reporting a lot, some, slight, no change or worsening.
Adverse events
Seven patients were withdrawn because of side effects during levetiracetam treatment and two during placebo treatment (P=0.21, Mainland–Gart test). The adverse events causing patients to withdraw from the study during levetiracetam treatment were incoordination (4), dizziness (3), somnolence (3), constipation/nausea (3), confusion (1) and rash (1). Adverse events and the number of patients reporting adverse events and moderate to severe adverse events tended to be more common during levetiracetam than placebo treatment, but this was not statistically significant (P>0.075, Mainland–Gart test) (Table 3).
Assessment of blindness
Ten patients (42%) correctly identified the treatment sequence, one identified the wrong sequence and thirteen were unable to suggest a specific sequence (54%). The researchers correctly identified the treatment sequence in eight patients and identified the wrong sequence in one. Among the 10 patients who identified the right sequence, the reason for choosing that was pain relief in 2 patients, adverse events in 6 and both pain relief and adverse events in 1.
Withdrawn patients
Twelve patients were withdrawn from the study, of these ten were exposed to levetiracetam. Only one patient exposed to levetiracetam reported pain relief but dropped out due to side effects.
Discussion
This randomized, placebo-controlled, crossover trial of the new anticonvulsant drug levetiracetam found no effect on neuropathic pain following SCI. There was also no effect on evoked pain and spasms.
Although we did not reach the predefined 30 completed patients, the study had an adequate sample size to give an 85% power to detect a change in pain score of 1.5 point on the NRS (0–10). There was no tendency toward treatment effect, and the study is unlikely to have overlooked a clinically relevant pain-relieving effect. The power calculation was carried out for the primary outcome measure and the study may have been underpowered for other measures, including evoked pain and spasms, that were not present in all patients. There was however no tendency toward improvement in any of the secondary outcome measures. 42% identified the correct treatment sequence but this unblinding did not result in better treatment response. The results are in line with a recently published randomized controlled trial, which found no effect of levetiracetam on the postmastectomy pain syndrome.35 Most patients reached the 3000 mg per day dose, which is the maximum recommended dose in epilepsy, but we cannot exclude that 5 weeks are too short a period to test if there is a long-term effect of levetiracetam. Levetiracetam was given as add-on to other pain treatment in 58% of the patients. There is therefore a risk that the study includes patients who are refractory to further treatment effect. However, patients with and without concomitant pain treatment had the same pain reduction during levetiracetam treatment. In addition, although not systematically recorded, the patients were likely to have tried other medications without effect in tolerable doses before entering this trial, which increases the risk of including patients refractory to treatment.
The reason for the lack of efficacy with levetiracetam is unknown. In animal models, levetiracetam has been shown to induce antihyperalgesic effects in the chronic constriction injury model17 and streptozocin-induced diabetic rats.17, 18, 19 It is possible that the pharmacological action of levetiracetam does not interfere with central pain mechanisms. This is in accordance with the experimental study finding no effect of levetiracetam on temporal pain summation.20 However, the lack of efficacy on the postmastectomy syndrome35 suggests lack of interference with mechanisms underlying peripheral postsurgical neuropathic pain as well. It is possible that the pharmacological action of levetiracetam is not involved in neuropathic pain mechanisms and that interference with the SV2A, in levetiracetam doses used in humans, will have no impact on neuropathic pain. However, if levetiracetam is effective in painful diabetic neuropathy, which has not been studied, it would suggest differences in underlying pain mechanisms between these various neuropathic pain states. A possible limitation of this study is the heterogeneity of the group, which included patients with both at- and below-level pain.
The high number of patients with concomitant medication may also increase the risk of additive side effect, which is supported by the tendency toward more withdrawals among patients with concomitant pain treatment. The study had a remarkably low placebo effect. In general, crossover studies have lower placebo responses than parallel group trials.36 Interestingly, previous studies in SCI pain have found low8 or no9, 34 overall placebo response, but the reason for this is unknown.
Central nervous system-related side effects are common with most anticonvulsants, although the newer generation anticonvulsants, such as levetiracetam, generally have better safety profiles and more favorable pharmacokinetic profiles than older generation anticonvulsants. There was a tendency toward higher incidences of somnolence, dizziness and incoordination as well as withdrawal due to side effects during levetiracetam treatment than during placebo treatment although there were no statistically significant differences in this relatively small study. We also saw a tendency toward more patients reporting worsening on the patient global impression of change scale during the levetiracetam than the placebo period. This study suggests that levetiracetam may be poor tolerated in a subgroup of patients.
In conclusion, levetiracetam in doses titrated up to 3000 mg had no analgesic or other benefit in patients with neuropathic pain following SCI.
References
Siddall PJ, McClelland JM, Rutkowski SB, Cousins MJ . A longitudinal study of the prevalence and characteristics of pain in the first 5 years following spinal cord injury. Pain 2003; 103: 249–257.
Werhagen L, Budh CN, Hultling C, Molander C . Neuropathic pain after traumatic spinal cord injury—relations to gender, spinal level, completeness, and age at the time of injury. Spinal Cord 2004; 42: 665–673.
Budh CN, Lund I, Ertzgaard P, Holtz A, Hultling C, Levi R et al. Pain in a Swedish spinal cord injury population. Clin Rehabil 2003; 17: 685–690.
Putzke JD, Richards JS, Hicken BL, DeVivo MJ . Interference due to pain following spinal cord injury: important predictors and impact on quality of life. Pain 2002; 100: 231–242.
Widerstrom-Noga EG, Felipe-Cuervo E, Yezierski RP . Chronic pain after spinal injury: interference with sleep and daily activities. Arch Phys Med Rehabil 2001; 82: 1571–1577.
Budh CN, Osteraker AL . Life satisfaction in individuals with a spinal cord injury and pain. Clin Rehabil 2007; 21: 89–96.
Levendoglu F, Ogun CO, Ozerbil O, Ogun TC, Ugurlu H . Gabapentin is a first line drug for the treatment of neuropathic pain in spinal cord injury. Spine 2004; 29: 743–751.
Siddall PJ, Cousins MJ, Otte A, Griesing T, Chambers R, Murphy TK . Pregabalin in central neuropathic pain associated with spinal cord injury: a placebo-controlled trial. Neurology 2006; 67: 1792–1800.
Vranken JH, Dijkgraaf MG, Kruis RM, van der Vegt MH, Hollmann MW, Heesen M . Pregabalin in patients with central neuropathic pain: a randomized, double-blind, placebo-controlled trial of a flexible-dose regimen. Pain 2007; 136: 150–157.
Rintala DH, Holmes SA, Courtade D, Fiess RN, Tastard LV, Loubser PG . Comparison of the effectiveness of amitriptyline and gabapentin on chronic neuropathic pain in persons with spinal cord injury. Arch Phys Med Rehabil 2007; 88: 1547–1560.
Widerstrom-Noga EG, Turk DC . Types and effectiveness of treatments used by people with chronic pain associated with spinal cord injuries: influence of pain and psychosocial characteristics. Spinal Cord 2003; 41: 600–609.
Norrbrink BC, Lundeberg T . Use of analgesic drugs in individuals with spinal cord injury. J Rehabil Med 2005; 37: 87–94.
Vierck CJ, Siddall P, Yezierski RP . Pain following spinal cord injury: animal studies and mechanistic studies. Pain 2000; 89: 1–5.
Lynch BA, Lambeng N, Nocka K, Kensel-Hammes P, Bajjalieh SM, Matagne A et al. The synaptic vesicle protein SV2A is the binding site for the antiepileptic drug levetiracetam. Proc Natl Acad Sci USA 2004; 101: 9861–9866.
Lambeng N, Gillard M, Vertongen P, Fuks B, Chatelain P . Characterization of [(3)H]ucb 30889 binding to synaptic vesicle protein 2A in the rat spinal cord. Eur J Pharmacol 2005; 520: 70–76.
Yang XF, Weisenfeld A, Rothman SM . Prolonged exposure to levetiracetam reveals a presynaptic effect on neurotransmission. Epilepsia 2007; 48: 1861–1869.
Ardid D, Lamberty Y, Alloui A, Coudore-Civiale MA, Klitgaard H, Eschalier A . Antihyperalgesic effect of levetiracetam in neuropathic pain models in rats. Eur J Pharmacol 2003; 473: 27–33.
Beyreuther B, Callizot N, Stohr T . Antinociceptive efficacy of lacosamide in a rat model for painful diabetic neuropathy. Eur J Pharmacol 2006; 539: 64–70.
Ozcan M, Ayar A, Canpolat S, Kutlu S . Antinociceptive efficacy of levetiracetam in a mice model for painful diabetic neuropathy. Acta Anaesthesiol Scand 2008; 52: 926–930.
Enggaard TP, Klitgaard NA, Sindrup SH . Specific effect of levetiracetam in experimental human pain models. Eur J Pain 2006; 10: 193–198.
Rowbotham MC, Manville NS, Ren J . Pilot tolerability and effectiveness study of levetiracetam for postherpetic neuralgia. Neurology 2003; 61: 866–867.
Price MJ . Levetiracetam in the treatment of neuropathic pain: three case studies. Clin J Pain 2004; 20: 33–36.
Dunteman ED . Levetiracetam as an adjunctive analgesic in neoplastic plexopathies: case series and commentary. J Pain Palliat Care Pharmacother 2005; 19: 35–43.
Hawker K, Frohman E, Racke M . Levetiracetam for phasic spasticity in multiple sclerosis. Arch Neurol 2003; 60: 1772–1774.
Patsalos N . Pharmacokinetic profile of levetiracetam: toward ideal characteristics. Pharmacol Ther 2000; 85: 77–85.
Finnerup NB, Grydehøj J, Johannesen IL, Bing J, Biering-Sørensen F, Sindrup SH et al. Levetiracetam in chronic neuropathic pain following spinal cord injury pain: a randomised controlled trial. International Association for the Study of Pain. 12th World Congress of Pain, Glasgow, August 16-22 2009 (abstract).
Widerstrom-Noga E, Biering-Sorensen F, Bryce T, Cardenas DD, Finnerup NB, Jensen MP et al. The international spinal cord injury pain basic data set. Spinal Cord 2008; 16: 818–823.
Melzack R . The McGill pain questionnaire: major properties and scoring methods. Pain 1975; 1: 277–299.
Drewes AM, Helweg-Larsen S, Petersen P, Brennum J, Andreasen A, Poulsen LH et al. McGill pain questionnaire translated into Danish: experimental and clinical findings. Clin J Pain 1993; 9: 80–87.
Marino RJ, Barros T, Biering-Sorensen F, Burns SP, Donovan WH, Graves DE et al. International standards for neurological classification of spinal cord injury. J Spinal Cord Med 2003; 26(Suppl 1): S50–S56.
Bouhassira D, Attal N, Fermanian J, Alchaar H, Gautron M, Masquelier E et al. Development and validation of the neuropathic pain symptom inventory. Pain 2004; 108: 248–257.
Penn RD, Savoy SM, Corcos D, Latash M, Gottlieb G, Parke B et al. Intrathecal baclofen for severe spinal spasticity. N Engl J Med 1989; 320: 1517–1521.
Bohannon RW, Smith MB . Interrater reliability of a modified Ashworth scale of muscle spasticity. Phys Ther 1987; 67: 206–207.
Finnerup NB, Sindrup SH, Bach FW, Johannesen IL, Jensen TS . Lamotrigine in spinal cord injury pain: a randomized controlled trial. Pain 2002; 96: 375–383.
Vilholm OJ, Cold S, Rasmussen L, Sindrup SH . Effect of levetiracetam on the postmastectomy pain syndrome. Eur J Neurol 2008; 15: 851–857.
Katz J, Finnerup NB, Dworkin RH . Clinical trial outcome in neuropathic pain. Relationship to study characteristics. Neurology 2007; 70: 263–272.
Acknowledgements
We thank Anne Grethe Rasmussen for her assistance with the data collection. This study was financially supported by UCB Pharma, the Danish Medical Research Council (no. 22040561) and Ludvig and Sara Elsass Foundation.
Author information
Authors and Affiliations
Corresponding author
Additional information
Trial registration: ClinicalTrials.gov NCT00252954.
Rights and permissions
About this article
Cite this article
Finnerup, N., Grydehøj, J., Bing, J. et al. Levetiracetam in spinal cord injury pain: a randomized controlled trial. Spinal Cord 47, 861–867 (2009). https://doi.org/10.1038/sc.2009.55
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2009.55
Keywords
This article is cited by
-
Pharmacologic therapies of pain in patients with spinal cord injury: a systematic review
Spinal Cord Series and Cases (2022)
-
Efficacy and safety of different drug treatments in patients with spinal-cord injury-related neuropathic pain: a network meta-analysis
Spinal Cord (2022)
-
Central Neuropathic Pain Syndromes: Current and Emerging Pharmacological Strategies
CNS Drugs (2022)
-
The CanPain SCI clinical practice guidelines for rehabilitation management of neuropathic pain after spinal cord injury: 2021 update
Spinal Cord (2022)
-
Evaluation and Management of SCI-Associated Pain
Current Pain and Headache Reports (2016)
