
Abstract
Study design:
A repeated measures, non-randomised controlled trial.
Objective:
To examine the effectiveness of individualised cognitive behaviour therapy (CBT) on the psychological adjustment of patients undergoing rehabilitation for newly acquired spinal cord injury.
Setting:
South Australian Spinal Cord Injury Service, Hampstead Rehabilitation Centre, South Australia, Australia.
Methods:
Eleven participants received individual CBT as part of their spinal rehabilitation. Self-reported levels of depression, anxiety and stress were assessed before the intervention, at week 12 of rehabilitation and at 3 months post-discharge, using the depression, anxiety and stress scales (DASS-21). Functional independence was also assessed, using the Functional Independence Measure (FIM). Responses were compared with 13 participants, closely matched on demographic and injury variables, who received standard psychological care (that is, assessment and monitoring only).
Results:
Depression scores for treatment participants showed a significant time effect, with worsening symptoms reported at three-month follow-up, after CBT was discontinued. In contrast, the DASS-21 scores of standard care participants remained at subclinical levels throughout the study. Clinical improvements in symptoms of anxiety and stress were also reported by the treatment group as inpatient therapy progressed.
Conclusion:
Targeted, individualised psychological treatment contributed to short-term, meaningful improvements in emotional outcomes for individuals reporting psychological morbidity after recent spinal injury. The results also highlight the need for ongoing access to specialised, psychological services post-discharge. Replication of these results with a larger sample is required before definitive conclusions can be drawn.
Similar content being viewed by others

Introduction
The psychological impact of spinal cord injury (SCI) is significant, with 30% of patients showing clinical levels of anxiety and/or depression during rehabilitation1 and after returning to community living.2 Research suggests that specialist psychological interventions have a role in managing these emotional outcomes.3, 4
Research also indicates that the provision of psychotherapy in spinal rehabilitation is constrained by a number of factors, including workforce issues, with limited staff resources often only allowing for a consultative service instead of comprehensive psychological assessment and intervention,5 and service delivery models that emphasise time-limited therapy.6, 7 Although group-based programmes using cognitive-behavioural therapy (CBT) have been advocated as a time-efficient inpatient therapy model,3, 4 their effectiveness is influenced by group homogeneity, with regard to patient characteristics.8 There is also evidence that patients prefer individual counselling when discussing emotive issues.9 This suggests that group CBT should augment, rather than replace, individual therapy.
In light of these issues, we undertook a small-scale study to evaluate the discipline-specific contribution of psychology to rehabilitation outcomes in patients with newly acquired SCI. This was achieved by comparing self-reports of patients who received psychological intervention with those of matched peers who required less intensive psychological support. It was expected that individual-based CBT, similar to previous group trials, would be of therapeutic benefit. However, it was not known whether any such benefit would be maintained after being discharged from an inpatient setting and in the absence of continued CBT.
Materials and methods
Participants
Participants were adults (⩾18 years) with English comprehension (at least primary school level education), who were undergoing rehabilitation at the Spinal Injuries Unit of Hampstead Rehabilitation Centre. Only individuals with a newly acquired injury, no pre-morbid psychiatric illness (such as substance abuse or psychosis diagnosed in the last 12 months) and no significant cognitive deficits sufficient to interfere with therapy participation, as determined by medical report, were included. Participants were recruited on a prospective basis over an 18-month period.
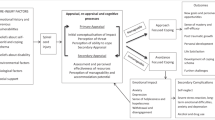
Details of participant selection and group allocation are provided in Figure 1. The final sample of 11 treatment and 13 standard care participants met the minimum required to achieve a large effect size of 0.80 for a two-tailed test with 90% power at a 0.05 significance level.10

Flow chart of participation.
Measures
A standard measure, the functional independence measure (FIM),11 was used to assess disability severity. The FIM was carried out on a person's admission and discharge date, with ratings determined by a team of allied health, nursing and medical staff. The FIM consists of 18 items that address motor and cognitive aspects of function. Items are scored on a 7-point scale that ranges from 1 (total assistance) to 7 (complete independence), with total scores ranging from 18 to 126. Higher scores indicate a lower severity of disability. The FIM shows good evidence of reliability and validity and is routinely used in spinal rehabilitation.12
The depression, anxiety and stress scales (DASS-21)13 were administered on an individual's admission to the Unit. This 21-item questionnaire, derived from the original 42-item DASS, consists of three subscales designed to measure the emotional states of depression, anxiety and stress. Each subscale contains seven items scored on a 4-point scale that ranges from 0 (‘Did not apply to me at all’) to 3 (‘Applied to me very much’). Subscale scores are summed and multiplied by two to allow comparison with normative values. The subscale scores can also be added to produce a composite measure of distress, with a score range from 0 to 126. Higher scores are indicative of higher levels of depression, anxiety and stress. The DASS-21 has been shown to be a sensitive indicator of mood in people with SCI.14
Procedures
Written informed consent was sought to access FIM and DASS-21 scores before psychological intervention (Time 1) and to re-administer at two additional time intervals: at week 12 (Time 2) of an individual's rehabilitation program or on discharge, if earlier (average Time 2 interval=11.3 weeks, s.d.=2.1), and at three months post-discharge (Time 3; DASS-21 only). The standard care group was tested at the same time intervals.
A clinical psychologist (DSD) was responsible for study recruitment. Although a detection bias is added by having one investigator allocate participants and deliver the intervention, this was unavoidable as the study was based in a single clinical setting that employed only one psychologist. Importantly, this clinician was not involved in assessing outcomes, with the FIM determined by other professionals and the DASS-21 based on self-report, thereby minimising any potential bias.
Participants were drawn from consecutive admissions to the Spinal Injuries Unit. Study eligibility was determined during the patient's routine screen with the psychologist. This assessment, which involved clinical interview and baseline measurement (including the DASS-21), determined the treatment decision. Those who reported elevated levels of distress (that is, DASS-21 scores in the moderate-to-severe range) were offered individual CBT. This subgroup was targeted for intervention as research suggests that individuals with clinically significant levels of distress are at risk of poor, long-term emotional outcomes and are a priority for psychological treatment.2, 3 In comparison, patients who reported DASS-21 scores in the subclinical range, and who met the same inclusion criteria, were assigned to the standard care group. These participants were also screened to match the treatment group on age, sex and injury. Participants in the standard care group continued to be monitored by the Unit's medical team and could withdraw from the study if their psychological treatment needs increased. Individuals who declined study participation or were ineligible were still offered individual CBT during their rehabilitation.
Treatment
Therapy followed a cognitive behaviour model that has shown efficacy in SCI groups.3, 4 The CBT was delivered by the Unit's clinical psychologist (DSD) and provided in addition to physical therapies. Therapy was guided by patients' psychological problems and treatment response but was also affected by physical rehabilitation schedule conflicts. On average, treatment participants received 11 CBT sessions (s.d.=4.5; range from 7 to 22 sessions). This involved fortnightly consultations of 30–60 min duration with the psychologist. There was a positive relationship between length of rehabilitation stay and amount of psychotherapy received (rs=0.44, P=0.031), with longer admissions allowing more opportunity for intervention. Owing to limited staffing, CBT was only offered to patients in the rehabilitation setting, with psychology services not readily available in the acute or community settings.
The key treatment goals were: to build individuals' confidence regarding the benefits of receiving CBT, education about the emotional impact of SCI, relieve symptoms of stress and the development of coping skills (including problem-solving strategies, behavioural activation and cognitive appraisal skills). In addition, peer professionals were available to all participants to provide mentoring. Peers are thought to have a critical role in spinal rehabilitation, with peer involvement contributing to improved emotional outcomes including self-esteem and social support.15 Psychiatric evaluation was also required for five treatment participants who reported severe distress. Low-dose amitriptyline was prescribed to these participants, as well as to five participants in the standard care group, for night-time sedation and to manage neuropathic pain.
Data analysis
Median and interquartile ranges were used to examine variability in group DASS-21 scores. Median, rather than mean, scores were reviewed because the data were not normally distributed. Given that the treatment and standard care groups had differing prognoses, with more severely distressed persons allocated to CBT, the two groups were evaluated separately. As the data did not meet the stringent requirements of parametric techniques, non-parametric statistics were used. The Friedman's analysis of variance and Wilcoxon's matched-pairs signed ranks test were considered the most appropriate statistical methods to determine the effectiveness of CBT.
Significant within-group differences would have been difficult to achieve due to the small sample size, even with clinically meaningful improvements in mood due to treatment.16 Therefore, treatment efficacy was also evaluated using Cohen's d effect sizes, based on the formula provided by Morris and DeShon.17 As a guideline, Cohen's d values of 0.2, 0.5 and 0.8 equate to small, medium and large group differences, respectively.18 The direction of effect was standardised so that a positive effect indicated that CBT was beneficial to outcome and a negative effect indicated an undesirable outcome.
Statement of ethics
All applicable institutional and governmental regulations concerning the ethical use of human volunteers were followed during the course of this research.
Results
Sample comparability
The final sample of 24 participants was found to be comparable to those who either declined to participate or withdrew before study commencement (n=6) in terms of gender (83 male vs 67%, Fisher's Exact test=0.57; Cramer's V=0.17; P>0.05) and injury type (58% with paraplegia vs 67%, Fisher's Exact test=1.00; Cramer's V=0.07; P>0.05). Although these groups did not differ significantly in age (U=49.00, Z=1.19, P>0.05, Cohen's d=0.66), the moderate effect size indicates that the final sample was older (on average, 13.6 years older).
The sample demographics were also compared to the Unit's admission statistics to determine whether these results were likely to be generalisable to the larger group of SCI patients. There were no significant group differences in age (t(80)=0.16; P>0.05; d=0.04), gender (83% male vs 67%; χ2(1)=2.18; P>0.05) or injury severity (58% with paraplegia vs 57%; χ2(1)=0.10; P>0.05), suggesting that the study sample was representative of the broader group of patients admitted to the Unit.
Participants
The study sample was almost exclusively male (83%; Table 1) and all participants were Caucasian. The largest percentage had completed high school (63%), followed by tertiary qualifications (25%). Most were employed (63%) and a higher percentage of individuals were single (58%) at the time of their injury.
In terms of their injury details (Table 1), the treatment and standard care groups did not differ significantly on injury type or lesion severity. Both traumatically acquired injuries (for example, falls, motor vehicle accidents) and non-traumatic injuries (for example, spinal abscess) occurred.
Functional rehabilitation outcomes
There were no significant differences between the treatment and standard care groups in terms of their length of hospital or rehabilitation stay (Table 1). Although there was a trend for those in the treatment group to have had longer acute admissions (by approximately 33 days), this difference was not significant. Functional rehabilitation outcomes were also similar for the groups (see Table 1), with no significant differences in mean total FIM scores on admission or at discharge. Moreover, the associated effect sizes were small (dadmission=0.27, ddischarge=0.19). Total FIM scores did not correlate significantly with total DASS-21 scores at admission (rs=0.04; P>0.05) or discharge (rs=−0.03; P>0.05), suggesting that functional state and mood were not strongly related.
The employment rate post-injury was low, with only two participants returning to work after being discharged. This figure may have been a reflection of either the older age range of participants, with 33% (n=8) having retired before their injury, or of their ongoing rehabilitation needs, with 54% (n=13) continuing to receive outpatient physical therapy at final follow-up.
Depression, anxiety and stress outcomes
Table 2 summarises the median scores on the DASS-21 for the sample at each of the three time points. As expected, the treatment group reported significantly higher subscale and total DASS-21 scores at each time point, and greater variability in these scores, as evident in the large interquartile ranges.
The results of the Friedman analyses of variance (Table 2) demonstrated significant differences in the depression scores for treatment participants across time, but no differences in their DASS-21 total scores or associated anxiety and stress subscale scores. The DASS-21 scores for the standard care group did not change significantly over time (see Table 2).
Post-hoc analyses for the treatment group (Table 3) showed a decline in the levels of depression from baseline to week 12 of treatment, although this equated to only a very small effect (d=0.08). In contrast, there was a significant increase in depressive symptomatology at three-month follow-up (d=−0.68). Similarly, total DASS-21 scores and subscale scores for anxiety and stress, declined from baseline to week 12 and were associated with moderate, positive effect sizes (total DASS-21 d: 0.38, anxiety d: 0.50; stress d: 0.48). At three-month follow-up, treatment participants reported a significant increase in levels of general distress and anxiety.
The clinical impact of these findings is highlighted by additionally examining individual ‘caseness’. Of the six treatment participants who reported clinical anxiety at baseline, two reported a reduction in symptom severity (that is, from extremely severe to the moderate or mild range) and two reported a complete resolution of symptoms. Similarly, all three treatment participants who initially reported moderate to severe stress symptoms subsequently reported only mild levels of stress at week 12. In terms of depressive symptoms, two of four treatment participants reported symptom improvement at week 12 and this clinical change was significant (χ2(1)=6.67; P=0.048). The three-month follow-up data are particularly revealing. Post-discharge, when there was no access to continued psychological support, 78% (n=7) of the treatment participants met the criteria for caseness on one or more DASS-21 subscales compared with 10% (n=1) of the standard care group. A χ2 analysis showed that this percentage change was significant (χ2(1)=8.93; P=0.005).
Discussion
This small-scale study examined the impact of individual CBT in an inpatient SCI rehabilitation setting when compared with less intensive psychological support. Not surprisingly, there was large within-group variability in the levels of psychological distress reported by treatment participants. The study results also highlight the variable impact of CBT on a subgroup of individuals reporting severe symptoms of depression, anxiety and stress at baseline.
Depression scores improved with CBT and then significantly declined, post-intervention, in the treatment group. There were associated improvements in DASS-21 caseness for this group. In comparison, there was no significant time effect on the DASS-21 for participants receiving standard care. To an extent, these results mirror previous research on the effectiveness of CBT after SCI. The finding that distress levels of treatment participants were severe at the commencement of rehabilitation reinforces the need for psychological intervention in the acute stages of SCI management.1 With self-reported distress levels increasing post-discharge, the continued mental health needs of this patient group are also evident.1, 19
These results need to be interpreted in light of the methodological difficulties. Power analyses (Table 3) indicate that the study was underpowered. As such, small treatment effects, which were more achievable, would have been difficult to detect.10, 18 Replication of the study with a larger sample is therefore essential. The timing of assessments may have also affected the results. Some treatment participants had not completed their inpatient rehabilitation and, subsequently, their CBT program at the week-12 assessment. Higher treatment gains may have been observed if outcome was assessed immediately post-intervention.
Another limitation relates to the highly selected sample. Participants in the standard care group reported different levels of psychological distress at baseline, reducing the equivalence of the two groups. However, building the patient triage process into the CBT package also acknowledged the practical aspects of delivering a service in a clinical setting with limited staff resources.6
This preliminary study highlights the difficulties encountered in clinical trials, in terms of methodology and availability of participants. The CBT was dependent on limited staff resources, which impacted on therapy frequency and duration. This may, therefore, not have been the optimal treatment for the severity of problems reported. Although the efficacy of CBT was reinforced by accessing peer role models and liaison psychiatry, improvements in the service strategy could include a stepped-care service model,20 with psychological intervention commencing in the acute setting and including access to specialised outpatient services to prevent psychological relapse.
Conflict of interest
The authors declare no conflict of interest.
References
Craig AR, Tran Y, Middleton J . Psychological morbidity and spinal cord injury: a systematic review. Spinal Cord 2009; 47: 108–114.
Pollard C, Kennedy P . A longitudinal analysis of emotional impact, coping strategies and post-traumatic psychological growth following spinal cord injury. Br J Health Psychol 2007; 12: 347–362.
Craig AR, Hancock K, Dickson H, Chang E . Long-term psychological outcomes in spinal cord injured persons: results of a controlled trial using cognitive behaviour therapy. Arch Phys Med Rehabil 1997; 78: 33–38.
Kennedy P, Duff J, Evans M, Beedie A . Coping effectiveness training reduces depression and anxiety following traumatic spinal cord injury. Br J Clin Psychol 2003; 42: 41–52.
Burton C, Murphy G, Smith-Tappe G . Workforce Survey of Psychologists in the Rehabilitation Sector—Victoria. The Australian Psychological Society Ltd: Melbourne, 2005.
Schwartz SM, Shanmugham K, Trask PC, Townsend CO . Conducting psychological research in medical settings: Challenges, limitations and recommendations for effectiveness research. Prof Psychol Res Pr 2004; 35: 500–508.
Schutz LE, Rivers KO, Ratusnik DL . The role of external validity in evidence-based practice for rehabilitation. Rehabil Psychol 2008; 53: 294–302.
Huebner RA . Group Procedures. In: Chan F, Berven NL, Thomas KR (eds.). Counseling theories and techniques for rehabilitation health professionals. Springer Publishing Company: New York, 2004, pp 244–263.
Schoenberg M, Shiloh S . Hospitalised patients' views on in-ward psychological counselling. Patient Educ Couns 2002; 48: 123–129.
Kraemer HC, Thiemann S . How Many Subjects? Statistical Power Analysis in Research. Sage Publications: Newbury Park, 1991.
Hamilton BB, Granger CV, Sherwin FS, Zeilezny M, Tashman JS . Uniform national data system for medical rehabilitation. In: Fuhrer MJ (ed). Rehabilitation outcomes: Analysis and measurement. Paul H. Brookes Publishing Company: Baltimore, MD, 1987, pp 137–147.
Dawson J, Shamley D, Jamous MA . A structured review of outcome measures used for the assessment of rehabilitation interventions for spinal cord injury. Spinal Cord 2008; 46: 768–780.
Lovibond SH, Lovibond PF . Manual for the Depression Anxiety Stress Scales, 2nd ed Psychology Foundation of Australia: Sydney, 1995.
Mitchell MC, Burns NR, Dorstyn DS . Screening for depression and anxiety in spinal cord injury with DASS-21. Spinal Cord 2008; 46: 547–551.
Middleton J, Craig AR . Psychological challenges in treating persons with spinal cord injury. In: Craig AR, Tran Y (eds). Psychological Dynamics Associated with Spinal Cord Injury Rehabilitation: New Directions and Best Evidence. Nova Science Publishers: New York, 2008, pp 1–47.
Zakzanis KK . Statistics to tell the truth, the whole truth, and nothing but the truth: formulae, illustrative numerical examples, and heuristic interpretation of effect size analyses for neuropsychological researchers. Arch Clin Neuropsychol 2001; 16: 653–667.
Morris SB, DeShon RP . Combining effect size estimates in meta-analysis with repeated measures and independent-groups designs. Psychol Methods 2002; 7: 105–125.
Cohen J . A power primer. Psychol Bull 1992; 112: 155–159.
Migliorini C, Tonge B, Taleporos G . Spinal cord injury and mental health. Aust NZJ Psychiatry 2008; 42: 309–314.
O'Donnell ML, Bryant RA, Creamer M, Carty J . Mental health following traumatic injury: Toward a health system model of early psychological intervention. Clin Psychol Rev 2008; 28: 387–406.
Acknowledgements
We thank the patients and staff at Hampstead Rehabilitation Centre for their cooperation. We also thank Prof Tonge and Dr Taleporos, Monash University, for their contribution to the study's design.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Dorstyn, D., Mathias, J. & Denson, L. Psychological intervention during spinal rehabilitation: a preliminary study. Spinal Cord 48, 756–761 (2010). https://doi.org/10.1038/sc.2009.161
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2009.161
Keywords
This article is cited by
-
Regaining A Sense Of Me: a single case study of SCI adjustment, applying the appraisal model and coping effectiveness training
Spinal Cord Series and Cases (2021)
-
Depressive mood in adults with spinal cord injury as they transition from an inpatient to a community setting: secondary analyses from a clinical trial
Spinal Cord (2017)
-
Do spinal cord-injured individuals with stronger sense of coherence use different psychological defense styles?
Spinal Cord (2016)
-
Psychosocial issues in spinal cord injury: a review
Spinal Cord (2012)
