
Abstract
Study design:
Representative community cross-sectional self-report survey of adults with spinal cord injury (SCI).
Objectives:
To establish semantic translation and validation of the Swedish scales—the Spinal Cord Lesion Coping Strategies Questionnaire and the Spinal Cord Lesion Emotional Wellbeing Questionnaire.
Setting:
Adults on the Victorian traumatic SCI register and attendees of the nontraumatic outpatient clinic were invited to participate.
Methods:
Instruments were forward and backward translated to establish semantic equivalence. Principle components analyses were undertaken. Correlation and logistic regression analyses were conducted to demonstrate validity of the instruments using both positive (high quality of life) and negative (depression and anxiety) psychological outcomes.
Results:
The final sample consisted of 443 adults with SCI living in the community. Both instruments demonstrated acceptable psychometric properties. Univariate correlation analyses showed most of the new scale components displayed medium to large relationships in the expected direction with the psychological outcomes and the other subscales. Health status and helplessness were significant predictors of both the positive and negative psychological outcomes in the logistic regression analyses. Acceptance was significantly related to the positive outcome only. Female and incomplete tetraplegia categories were significantly and positively related to depression only.
Conclusion:
Notwithstanding a few issues with some of the subscales, the results support the usefulness of these easy to use instruments and point to ways for further development of the scales.
Similar content being viewed by others


Introduction
Compelling arguments have established the need for reliable standardized condition-specific instruments to assess the coping efforts made by persons with a spinal cord injury (SCI).1, 2
The Spinal Cord Lesion Coping Strategies Questionnaire (SCL CSQ) provides a succinct indication of condition-specific (that is, SCI) coping mechanisms of acceptance, fighting spirit and social reliance employed by respondents; acceptance measures the extent of revaluation of life values, fighting spirit measures efforts to behave independently and social reliance measures the tendency towards dependent behaviour. Due to the recency of development, there has been limited use of the scale; however, the scale has displayed satisfactory properties with different samples sourced within the same catchment area.1, 2, 3, 4, 5
The Spinal Cord Lesion Emotional Wellbeing Questionnaire (SCL EWQ) provides a succinct indication of the emotional consequences to the SCI, evaluating the positive emotional outcome of personal growth and the negative outcomes of helplessness and intrusion; personal growth determines the current positive change in attitude stemming from the life crisis (that is, SCI), helplessness determines the level of perplexity, out of control and low self esteem currently felt and intrusion determines the level of bitterness and brooding. There has been less use of the SCL EWQ.2, 6, 7 The scale seems promising, but has not been validated with any standardized scales measuring psychopathology to date.
Both scales were developed in Sweden and had undergone only the first stage of appropriate forward/backward translation procedures before publication. There were two aims of this study. The first was to complete translation procedures to establish semantic equivalence for their use on Australian populations with SCI and so comprises the first part of the project. The other was to validate the efficacy of the translated instruments using both positive (high subjective QoL) and negative (depression and anxiety) mental health outcomes and so comprises the second part of the project.
Method: Part 1 establishing semantic equivalence of the two scales
Part 1 (a) Completion of the forward/backward translation process
The items of both SCL CSQ and SCL EWQ were assessed for face validity with special consideration of the vernacular of Australian English while still retaining the essence of each factor. After consensus was reached between the original authors and the Australian research group, structured cognitive debriefing interviews to discuss the new scales were conducted with nine people with SCI who were residents in supported housing (eight with traumatic SCI 5 male; time since injury: 3 years to more than 37 years). The new Australian coping strategies and emotional consequences scales are SCL CSQ v1 Australia and SCL EWQ v1 Australia, and these are included in Appendix A.
Part 1 (b) Factor analysis of the translated scales using principle components analyses
Participants
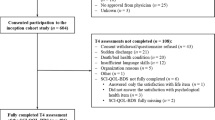
The sample consisted of 443 adults with sudden-onset SCI who were 18 years and older and 6 months or more post injury; 14% (n=62) with non-traumatic aetiology. Two recruitment sites were used: the outpatient register of the only hospital with the dedicated traumatic SCI unit that also treats some nontraumatic SCI (Austin Hospital, Victoria, Australia), and the outpatient clinic of the only other hospital in Melbourne with a dedicated SCI rehabilitation unit that focuses on treating nontraumatic SCI (Caulfield General Medical Centre, Victoria, Australia). Participants could complete the survey on the web, by telephone or on hard copy.
Analyses
The SCL CSQ v1 Australia and the SCL EWQ v1 Australia were subjected to confirmatory principal components analyses (PCA) to confirm the presence of three factors per scale.
Results: Part 1(b) establishing semantic equivalence of the two scales
The factor analyses confirmed the three factor-structure of the original Swedish version for both scales: SCL CSQ v1 Australia (coping strategies scale) and SCL EWQ v1 Australia (emotional consequences scale).
Inspection of the correlation matrix revealed the presence of many coefficients of 0.3 and above confirming suitability for factor analyses for both scales. The Kaiser—Meyer–Oklin value was 0.815 for the coping strategies scale and 0.894 for the emotional consequences scale, exceeding the recommended value of 0.6;8, 9 and the Bartlett's test of sphericity10 reached statistical significance (P<0.001) for both scales, supporting the factorability of the correlation matrix of each scale. PCA confirmed the presence of three components in each scale. Varimax rotation revealed that each component consisted of a number of strong loadings and all variables loaded substantially on only one component in both scales.
The three-component solution explained a total of 59.86% of the variance in the coping strategies scale (Table 1). The results support the use of the acceptance, social reliance and personal growth items as originally found by Elfström et al.2 with the exception of item 7—I refuse to let the injury rule my life. This item was originally included within the fighting spirit factor and its face validity seems to support this contention. However in the PCA, the item clearly loads on the acceptance factor. In the current study this item was included in the acceptance subscale. The Cronbach-α coefficient for the overall scale was 0.745; the Cronbach-α coefficients for each domain were acceptance=0.804, fighting spirit=0.636 and social reliance=0.789. None of the variables had a skewness or kurtosis exceeding ±1 with the exception of fighting spirit which was marginally outside at 1.022.
The three-component solution explained a total of 61.63% of the variance in the emotional consequences scale (Table 2). The results of the PCA support the use of the helplessness, intrusion and personal growth items as separate scales, as originally found by Elfström et al.2 The Cronbach-α coefficient for the overall scale was 0.792; the Cronbach-α coefficients for each domain were helplessness=0.864, intrusion=0.831 and personal growth=0.465. Examination of the α-if-item-deleted option for personal growth did not reveal any mechanism for improvement and though the α-level was considerably lower than that for the other domains, it still fell within acceptable levels.11, 12 None of the variables had a skewness or kurtosis exceeding ±1.
Method: Part 2 validate the efficacy of the translated instruments
The relationship between the coping strategies scale, the emotional consequences scale, high subjective QoL, depression and anxiety outcomes.
Instruments
The survey consisted of demographic and injury related items and the standardized instruments of SCL CSQ v1 Australia and SCL EWQ v1 Australia, the subjective QoL Satisfaction subscale from the Comprehensive Quality of Life for Adults, version 5 (COMQoL-A5)13 and the Depression, Anxiety, and Stress Scale—short version (DASS-21).14
The positive outcome was overall subjective QoL which was the mean of the seven subjective QoL domains13—material, health, productivity, intimacy, safety, place in the community and emotional wellbeing. This score was then converted into a percentage of scale maximum score (%SM; formula as per Cummins,13 p28) and then dichotomized into 0=subjective QoL below 70 %SM (or low subjective QoL) and 1=subjective QoL 70 %SM and above (or high subjective QoL).
The negative mental health outcomes of the presence of depression and anxiety were computed from the scores of the depression and anxiety subscales from DASS-21.14 These scores were dichotomized into 0=non-clinical range and 1=clinical range, using the published thresholds.14
The independent variable health consisted of a 1–10 score where higher scores indicated better health and it was derived from two questions. One question asked about the frequency of visits to the doctors over the previous 3 months. The other question asked for the names of medications taken daily. Each question was scored on 1–5 scale and then summed.
Both the coping strategies and emotional consequences scales follow the original 1–4 scoring pattern. Higher scores confirm a higher affirmation of the domain. If some scores were missing then the recommended half score was used.
Analyses
Mean and s.d. established the parameters of the coping strategies and emotional consequences scales. Correlation analyses established the strength of the relationships between the new scales and both the positive and negative outcomes. Identical logistic regression analyses, which examined the relationship between both of the scales and each psychological outcome while keeping demographic and injury-related characteristics constant, were used due to the expected positive skewing of the outcome results. Psuedo-R2 statistics (Cox and Snell R2 and the Nagelkerke R2) indicate the amount of variance explained by the independent variables within each model.
Results: Part 2 validate the efficacy of the translated instruments
Characteristics of the cohort
This final cohort consisted of 443 individuals with SCI living in the community, male n=345 (78%). The mean age of respondents was 51.78 years (range 18–86 years). The mean time since injury was 19.20 years (range 1–66 years). The proportion of the cohort with incomplete paraplegia was 33.6% (n=149), complete paraplegia 30.7% (n=136), incomplete tetraplegia 25.3% (n=112) and complete tetraplegia 10.2% (n=45). Most were in a relationship (married/defacto/living with partner; n=260, 58.7%), some had been in a relationship (divorced/widowed/separated; n=68, 15.3%) and the rest were single (n=114, 25.7%).
The mean and s.d. of the scores for the new subscales were acceptance M=3.028 (s.d.=0.594), social reliance M=2.689 (s.d.=0.698), fighting spirit M=3.242 (s.d.=0.4312),helplessness M=2.117 (s.d.=0.633), intrusion M=2.102 (s.d.=0.802) and personal growth M=2.563 (s.d.=0.530).
Univariate correlation analyses (Spearman's ρ) showed many of the subscales displayed medium to large relationships in the expected direction with the psychological outcomes and the other subscales (Table 3). Social Reliance seemed the least useful with only small to no relationships with the other factors.
The logistic regression analyses revealed few statistically significant independent variables (see Table 4). Health and the emotional consequences subscale Helplessness were significantly related to each outcome. Better health increased the likelihood of high subjective QoL by 20% (OR=1.195 (95% CI: 1.054–1.356)), and decreased the likelihood of depression by 20% (OR=0.831 (95% CI: 0.718–0.962)) and anxiety by 28% (OR=0.763 (95% CI: 0.691–0.888)). Higher helplessness increased the likelihood of depression by more than 15 times (OR=15.328 (95% CI: 6.663–35.264)) and anxiety by five times (OR=5.149 (95% CI: 2.745–9.661)). Each unit decrease in helplessness increased the likelihood of high subjective QoL by more than eight times (OR=0.116 (95% CI: 0.057–0.238)).
There were two independent variables that were significantly associated with one outcome only. Acceptance was significantly associated with high subjective QoL (OR=3.428 (95% CI: 1.789–6.569)). Level of injury was significantly associated with depression. Those with incomplete tetraplegia were four times more likely to experience depression (OR=4.001 (95% CI: 1.367–11.712)). Pseudo-R2 statistics suggest the models explained around 40–55% of the variance in depression, around 21–30% in anxiety and around 33–44% in high subjective QoL (Table 5).
Discussion
The emotional consequences and coping strategies scales had not been used in Australian English language studies previously. Both the scales displayed satisfactory psychometric properties. Factors from both scales displayed strong associations with both mental health and subjective QoL outcomes in the univariate analyses.
Helplessness, a subscale of the emotional consequences scale, was one of two independent variables to substantially impact on each mental health outcome while keeping other coping, demographic and injury-related variables constant. Helplessness was originally conceived to be a consequence of the interaction of stress and coping based on the transactional theory of stress.2 Previously, helplessness was regarded as strongly related with social reliance and acceptance, in positive and negative directions, respectively.2 However, this was not the case in this study.
The significant positive association of helplessness with poor mental health outcomes is consistent with the limited previous research where helplessness was conceived as a coping style.15 This is the first study to consider the role of helplessness on affirmative (high subjective QoL) and pessimistic (depression and anxiety) outcomes simultaneously. The significant negative association of helplessness with high subjective wellbeing underscores the importance of this construct within this vulnerable population. Health was the only other independent variable to substantially impact on each outcome despite it being only an indirect measure of health. The significance and direction of Health with each mental health outcome is consistent with previous research that used various manifestations of health.16, 17, 18
There were three independent variables, which were associated with one outcome only. Acceptance was associated with high subjective QoL but not with poor mental health outcomes. This has important implications for adaptation to SCI theory as well as rehabilitation practices. The lack of acceptance does not mean clinically significant depression or anxiety but may perhaps signal extra vulnerability. Future research is needed to further tease this out.
Gender was significantly associated with depression only. The increased likelihood of depression in females was not surprising, given the significant association well established in general population psychology19 and previous research into depression after SCI.20 The level of injury was also significantly associated with depression only and contrasts with previous research.20, 21 Those with incomplete tetraplegia had a stronger association with depression compared to the other levels of SCI. There are a couple pointers why this may be so. Qualitative responses from some with incomplete tetraplegia (from the survey but not reported here) spoke of not fitting in with the general population even though they looked the same, that is, hidden disability. They also spoke of not fitting in with the population with SCI because they didn't look like them either. These comments were included in their reports of how they felt about themselves and also when giving an account of the actions of both the general population and their own families towards themselves. Both the quantitative and qualitative results focus the attention towards the interaction of the individual with the psychosocial environment as a significant mediator of mental health and are in accord with the conceptual biopsychosocial model of disability.
An alternative explanation also comprises a limitation of the study. The crude partitioning of the level of SCI variable could have introduced potential confounding by the inclusion of dissimilar levels of capabilities within each grouping. The study was a self-report survey and two respondents were unsure to which group they belonged. Medical records were not available to confirm their level of SCI. Further research within the Australian context will hopefully shed light on this conundrum.
There were some subscales that were less useful, particularly in the logistic regression models, such as social reliance and personal growth. Generally, the more items within the subscales, the more productive the results were. It is difficult to capture complex concepts with only a few items. Adding further items to the subscales may better capture these constructs and improve the psychometric properties of these subscales. In this study, an item that was originally a part of fighting spirit, clearly loaded on acceptance. Fighting spirit and social reliance have also posed problems in the UK English and German language versions of the coping strategies scale. Those problems were thought to have resulted from translation inaccuracies since cognitive debriefing interviews were not performed to check that the translations captured what they intended to.22 However cognitive debriefing interviews were conducted in this study, so perhaps cultural issues are also impacting on these constructs. There were comparatively large s.d. in the subscales in the logistic regression analyses. Expanding the 1–4 response scores of the new scales may help to fine tune the results.
Notwithstanding these issues, these new scales provided strong predictors of each mental health outcome. The results of this study support the usefulness of these easy to use scales and point to ways to further develop these new scales.
References
Elfström ML, Kreuter M, Lars-Olof P, Sullivan M . General and condition-specific measures of coping strategies in persons with spinal cord lesions. Psychol Health Med 2005; 10: 231–242.
Elfström ML, Ryden A, Kreuter M, Persson L, Sullivan M . Linkages between coping and psychological outcome in the spinal cord lesioned: development of SCL-related measures. Spinal Cord 2002; 40: 23–29.
Elfstrom M, Ryden A, Kreuter M, Taft C, Sullivan M . Relations between coping strategies and health-related quality of life in patients with spinal cord lesion. J Rehabil Med 2005; 37: 9–16.
Elfström ML, Kreuter M . Relationships between locus of control, coping strategies and emotional well-being in persons with spinal cord lesion. J Clin Psychol Med Settings 2006; 13: 89–100.
Elfström ML, Kreuter M, Rydén A, Persson L-O, Sullivan M . Effects of coping on psychological outcome when controlling for background variables: a study of traumatically spinal cord lesioned persons. Spinal Cord 2002; 40: 408–415.
Elfström ML, Kreuter M . Relationships between locus of control, coping strategies and emotional well-being in persons with spinal cord lesion. J Clin Psychol Med Settings 2006; 13: 93–104.
Elfström ML, Kreuter M, Ryden A, Persson L-O, Sullivan M . Effects of coping on psychological outcome when controlling for background variables: a study of traumatically spinal cord lesioned persons. Spinal Cord 2002; 40: 408.
Kaiser H . A second generation little jiffy. Psychometrika 1970; 35: 401–415.
Kaiser H . An index of factorial simplicity. Psychometrika 1974; 39: 31–36.
Bartlett MS . A note on the multiplying factors for various chi square approximations. J R Stat Soc 1954; 16 (Series B): 296–298.
Boyle GJ . Does item homogeneity indicate internal consistency or item redundancy in psychometric scales? Pers Individ Differ 1991; 12: 291–294.
Cortina JM . What is coefficient alpha? An examination of theory and applications. J Appl Psychol 1993; 78: 98–104.
Cummins RA . Comprehensive Quality of Life Scale—Adult (ComQol-A5), 5th edn. Deakin University: Melbourne, 1997.
Lovibond SH, Lovibond PF . Manual for the Depression Anxiety Stress Scales, 2nd edn. The Psychology Foundation of Australia Inc.: Sydney, Australia, 1995.
Shnek ZM, Foley FW, LaRocca NG, Gordon WA, DeLuca J, Schwartzman HG et al. Helplessness, self-efficacy, cognitive distortions, and depression in multiple sclerosis and spinal cord injury. Ann Behav Med 1997; 19: 287–294.
Boekamp JR, Overholser JC, Schubert DSP . Depression following a spinal cord injury. Int J Psychiatry Med 1996; 26: 329–349.
Budh CN, Osteraker A-L . Life satisfaction in individuals with a spinal cord injury and pain. Clin Rehabil 2007; 21: 89–96.
Scivoletto G, Petrelli A, Di Lucente L, Castellano V . Psychological investigation of spinal cord injury patients. Spinal Cord 1997; 35: 516–520.
Andrews G, Hall W, Teesson M, Henderson S . The Mental Health of Australians. Canberra: Mental Health Branch, Commonwealth Department of Health and Aged Care, 1999.
Krause JS, Kemp B, Coker J . Depression after spinal cord injury: relation to gender, ethnicity, aging, and socioeconomic indicators. Arch Phys Med Rehabil 2000; 81: 1099–1109.
Bombardier CH, Richards JS, Krause JS, Tulsky D, Tate DG . Symptoms of major depression in people with spinal cord injury: implications for screening. Arch Phys Med Rehabil 2004; 85: 1749–1756.
Elfström ML, Kennedy P, Lude P, Taylor N . Condition-related coping strategies in persons with spinal cord lesion: a cross-national validation of the Spinal Cord Lesion-related Coping Strategies Questionnaire in four community samples. Spinal Cord 2007; 45: 420–428.
Acknowledgements
We acknowledge the support of the Monash University Postgraduate Publishing Award and the Robert Rose Foundation PhD scholarship to CEM.
Author information
Authors and Affiliations
Corresponding author
Appendix A
Appendix A
SCL CSQ v 1.0 Australia.
-
1
My disability has become just a part of me now (acceptance)
-
2
I have learnt to appreciate other things in my life since my injury (acceptance)
-
3
It is important for me to have goals that I can try to achieve (fighting spirit)
-
4
I have to trust that other people will help me (social reliance)
-
5
I try to make the best of life despite my injury (fighting spirit)
-
6
What I have lost physically has been made-up in so many other ways (acceptance)
-
7
I refuse to let the injury rule my life (acceptance)
-
8
I would feel helpless without the support from others (social reliance)
-
9
I depend on others' ability to help me (social reliance)
-
10
I try to manage on my own (fighting spirit)
-
11
I have accepted my injury (acceptance)
-
12
I look out for new ways to make life easier (fighting spirit)
SCL EWQ v 1.0 Australia.
-
1
I have become more humble since my injury (personal growth)
-
2
I don't seem to have any direction anymore (helplessness)
-
3
I often wonder just why I was injured (intrusion)
-
4
I don't seem to have any control over my life (helplessness)
-
5
No-one seems to understand my situation (helplessness)
-
6
I have matured since my injury (personal growth)
-
7
I will probably never get over feeling bitter and resentful that I was injured (intrusion)
-
8
Sometimes I feel ashamed of my injury (helplessness)
-
9
I feel of less worth to people who are not injured (helplessness)
-
10
I worry about my future since my injury (helplessness)
-
11
My disability feels like an undeserved punishment (intrusion)
-
12
Since the injury, I feel better about myself (personal growth)
Rights and permissions
About this article
Cite this article
Migliorini, C., Elfström, M. & Tonge, B. Translation and Australian validation of the spinal cord lesion-related coping strategies and emotional wellbeing questionnaires. Spinal Cord 46, 690–695 (2008). https://doi.org/10.1038/sc.2008.22
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2008.22
Keywords
This article is cited by
-
The associations of acceptance with quality of life and mental health following spinal cord injury: a systematic review
Spinal Cord (2020)
-
A randomised control trial of an Internet-based cognitive behaviour treatment for mood disorder in adults with chronic spinal cord injury
Spinal Cord (2016)
-
Reliability and validity of the Turkish version of spinal cord lesion-related coping strategies
Spinal Cord (2014)
-
Quality of life in adults with spinal cord injury living in the community
Spinal Cord (2011)
