
Abstract
In this cross-sectional investigation, the primary objective was to explore the correlation between the consumption of polyphenols and the likelihood of non-alcoholic fatty liver disease (NAFLD) in the adult population participating in the Hoveyzeh cohort. Data from the Hoveyzeh cohort study, part of the Persian Cohort Study, involving 10,009 adults aged 35–70, were analyzed. Exclusions were made for missing data, extreme energy intake, and liver cancer patients. Dietary habits were assessed using a food frequency questionnaire, and polyphenol intake was calculated using the Phenol Explorer database. Logistic regression analyses, adjusted for confounders, were performed to assess the relationship between polyphenol subclasses (total polyphenols, total flavonoids, phenolic acid, and lignin) and NAFLD. Among 9894 participants, those in the highest quintile of total polyphenol (OR 0.65, CI 0.5–0.84; P = 0.007), phenolic acid (OR 0.67, CI 0.52–0.86; P < 0.001), and lignin intake (OR 0.69, CI 0.52–0.87; P = 0.001) demonstrated lower odds of NAFLD compared to the lowest quintile, even after adjusting for confounding factors. However, no significant association was found between total flavonoid intake and NAFLD (OR 1.26, CI 0.96–1.67; P = 0.47). Subgroup analysis indicated a significant inverse association between total polyphenols and NAFLD in women (OR 0.64, CI 0.42–0.93; P = 0.001). Higher intake of total polyphenols, phenolic acid, and lignin was associated with reduced odds of NAFLD among adults in the Hoveyzeh cohort. This suggests that dietary patterns rich in these polyphenols may play a role in mitigating the risk of NAFLD. Further interventional and longitudinal studies are needed to validate these findings and explore potential preventive strategies involving polyphenol-rich diets.
Similar content being viewed by others

Introduction
NAFLD is a medical problem predominantly marked by the gathering of fat in the liver tissue, specifically exceeding 5% of hepatocytes1. The impact of NAFLD is reflected in its range of pathological manifestations, spanning from Simple NAFLD to steatohepatitis (Non-Alcoholic Steatohepatitis—NASH), ultimately culminating in hepatic cirrhosis and hepatocarcinoma2,3. Increased mortality is linked to the advanced phases of NAFLD. However, it is important to note that all stages of NAFLD pose a considerable risk for other chronic diseases. Its definition encompasses a state wherein the accumulation of fat in the liver tissue exceeds the typical amount and exhibits histopathological features akin to alcohol-induced liver steatosis. Notably, this condition is identified in individuals who consume minimal to no alcohol4,5,6,7.
Approximations suggest that the global incidence of NAFLD varies between 20 and 30%8. Based on Adibi et al. study, Prevalence of NAFLD among the Iranian adults was 39.3%9.Insulin resistance, obesity and metabolic syndrome are recognized as prominent risk factors linked to NAFLD10. The widespread occurrence of NAFLD diagnosis globally is closely connected to the prevalent adoption of sedentary lifestyles coupled with excessive caloric intake. Implementing changes in lifestyle, particularly achieving weight reduction, stands out as the most effective therapeutic approach for managing NAFLD. A weight loss of at least 7 to 9% is necessary to alleviate hepatic inflammation11,12,13,14. Moreover, aside from overall energy consumption, dietary composition also plays a role in influencing metabolic functions. Recent research indicates that incorporating diets rich in polyphenols may be beneficial in preventing and treating chronic conditions, such as obesity, some types of the cancer, diabetes, and other chronic diseases15,16,17,18.
Polyphenols are naturally occurring phytochemical compounds found in plant-based foods, encompassing fruits, vegetables, whole grains, and beverages such as coffee, tea, red wine, and dark chocolate6,17,19,20. Polyphenols are the predominant antioxidants present in diet, and their impacts, akin to those of vitamins, form the fundamental basis for the well-established health benefits traditionally attributed to fruits and vegetables across various diseases21,22,23. Moreover, it has been documented that these substances could influence de novo lipogenesis 21,24.
Nevertheless, there is a scarcity of experimental or epidemiological studies exploring the protective effects of these components in NAFLD. The majority of the research has concentrated on specific categories of polyphenols and flavonoids, with less emphasis on assessing the intake of polyphenol subclasses25,26. Therefore, this population bases study was aimed to investigate the relationship between the consumption of total polyphenols, total flavonoids, phenolic acid and lignin with the odds of NAFLD among the adults.
Subjects and methods
Study design and population
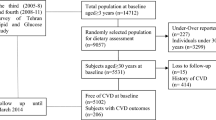
This cross-sectional investigation utilized data derived from the initial phase of the national Persian Cohort, specifically the Hoveyzeh cohort study (HCS). The HCS, conducted from May 2016 to August 2018, is a prospective study focused on non-communicable diseases within the Arab population. A total of 10,009 adults aged 35–70 participated in Hoveyzeh and Rofayyeh cities, located in the Khuzestan province of Southwest Iran. Prior to collecting data, participants were provided with a detailed explanation of the study’s objectives and methods, and subsequently informed consent was obtained from all subjects.
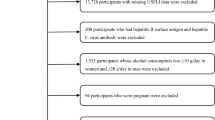
The HCS cohort study is an integral part of the Prospective Epidemiological Research Studies in Iran, known as the PERSIAN Cohort Study, and has received approval from the Ethics Committees in the Ministry of Health and Medical Education, as well as the Digestive Diseases Research Institute at Tehran University of Medical Sciences in Iran. Further information about this study has been previously published elsewhere27,28. For this study, we excluded people who had missing data, people whose daily energy intake was higher than 4500 kcal or less than 700 kcal, and also patients with liver cancer, patients who were taking hepatotoxic drugs or had followed restricted diets during the last three months (n = 115) and final analysis was done on data from 9894 adults. The research received ethical approval from the Ethics Committee of Ahvaz Jundishapur University of Medical Sciences under the reference number (IR.AJUMS.REC.1398.640).
Anthropometric measurements
Digital scales (Seca 755) were employed to measure weight with an accuracy of 100 g, while individuals wore lightweight clothing and no shoes. Height, accurate to 0.5 cm, was measured using a Seca stadiometer (Seca company, Model 206, Germany) with individuals standing in a normal alignment, shoulders relaxed, and without shoes. Body mass index (BMI) was computed by dividing weight (in kilograms) by the square of height (in meters).
Assessment of blood pressure and biochemical markers
Following a fasting period of 10 to 12 h, blood specimens were gathered from each participant. To isolate serum from the blood, the samples underwent centrifugation for 15 min at 1000 revolutions per minute and were subsequently preserved at -80 °C until analysis. Additional procedural information can be found in the preceding research28. The glucose oxidase method was employed to measure fasting blood glucose (FBG). Enzymatic kits from Pars Azmoon, Iran, were utilized to determine total cholesterol (TC), triglyceride (TG), aspartate aminotransferase (AST), alanine transaminase (ALT), and high-density lipoprotein (HDL). Systolic and diastolic blood pressure were recorded twice for each arm using Riester sphygmomanometers, separated by a 10-min interval, and the average of the two measurements was reported. The diagnosis of NAFLD was based on the patient's medical record and the reports of the individual's family physician in the patient's medical record.
Dietary assessment
A semi-quantitative food frequency questionnaire (FFQ) comprising 130 food items was employed to evaluate the typical dietary habits of individuals28. Participants were instructed to indicate the frequency of consuming each item over the past year, specifying whether it occurred daily, weekly, monthly, or annually. Trained dietitians conducted face-to-face interviews with participants to complete all questionnaires. The quantity of each food item was converted into grams per day using household measures. Subsequently, the recorded food intake in grams per day was entered into Nutritionist IV to compute the overall energy and nutrient intake.
Polyphenol evaluation
The assessment of polyphenol consumption in the diet involved the utilization of an enhanced edition of the phenol explorer database (www.phenol-explorer.eu). This database encompasses 501 polyphenols categorized into 6 classes and 31 subclasses. Additionally, it provides insights into the impact of food processing on the levels of polyphenols 29. We gathered information on the total polyphenol content, along with its primary subcategories, including flavonoids, phenolic acids, and lignans, from a selection of 80 food items. The overall polyphenol content was predominantly determined using the Folin assay. In cases where this method was not applicable, we aggregated the individual polyphenol subclasses to derive the total polyphenol content. Regarding flavonoids and phenolic acids, we computed their concentrations through chromatography following hydrolysis whenever applicable, and lignans measured using chromatography after hydrolysis. In all computations, we took into account food preparation techniques like cooking, frying, and other methods, incorporating the retention factor as documented in the "phenol explorer database." Subsequently, the quantities of polyphenols were assessed by calculating the polyphenol content in conjunction with the daily intake of each food item.
Statistical analysis
Statistical analysis was performed utilizing the Statistical Package for the Social Sciences (SPSS) software, version 21 (developed by SPSS Inc. in Chicago, IL, USA). The normality of the data was assessed using the Kolmogorov–Smirnov test and a histogram chart. Baseline characteristics and dietary intakes were presented as either mean ± standard error (SE) for quantitative variables, and as numbers and percentages for qualitative variables. The examination of continuous and categorical variables was conducted using either the Analysis of Variance (ANOVA) test or the Chi-square test across the dietary polyphenol intake. Ultimately, logistic regression analyses were conducted, and the reported outcomes included the level of significance, odds ratio (OR), and 95% confidence interval (CI). A statistical significance level was considered achieved when P < 0.05. The regression analyses were adjusted for confounding variables that could impact the association between the dietary polyphenols and NAFLD. These variables comprised age, energy intake, gender, smoking, alcohol consumption, physical activity levels, BMI, and education level.
Ethics approval and consent to participate
The study was carried out in accordance with the Declaration of Helsinki, and the research protocol received approval from the of Ahvaz Jundishapur University of Medical Sciences under the reference number (IR.AJUMS.REC.1398.640). Prior to collecting data, participants were provided with a detailed explanation of the study's objectives and methods, and subsequently informed consent was obtained from all subjects.
Results
The data obtained from 9894 adults participating in the Hoveyzeh cohort were participated in the current investigation. Table 1 summarized the demographic, anthropometric and clinical characteristics of people based on quintiles of polyphenol intake. The mean age of the of the study participants was 48.3 (0.22) years, and we found a significant difference in the age of the participants among the quintiles of dietary polyphenol intake (P < 0.001). Also, 3931 participants were male and the rest were female, and in terms of gender distribution, a significant difference was seen between the quintiles of dietary polyphenol intake (P < 0.001). In term of smoking and alcohol intake, there wasn’t any significance difference between subjects on quintiles of polyphenol intake (P = 0.13 for smoking and P = 0.204 for alcohol consumption). Moreover, we found a significant differences between participants in different quintiles of polyphenol intake in term of BMI distribution (P = 0.003), blood glucose (P < 0.001) and triglyceride (P < 0.001). NAFLD was identified in 1134 (prevalence, 14.52%) of the 9894 subjects. The findings from the investigation indicated that the prevalence of NAFLD in people who were in the upper quintile of dietary intake of polyphenols was significantly lower than in people who were in the lower quintile (254 patients vs. 312 patients; P = 0.02).
Nutrient and food consumption according to quintiles of the dietary polyphenol intake among the participants showed in Table 2. The mean energy intake of people in the highest quintile of dietary polyphenol intake was significantly higher than in the first quintile (3376.9 kcal/day vs. 2182.5 kcal/day; P < 0.001). Also, participants in the higher quantile of polyphenol intake, consumed significantly higher amounts of carbohydrate (P = 0.02), total fat (P = 0.01), PUFA (P = 0.03), fruits (P = 0.02) and vegetables (P = 0.04) and lower amounts of red meat (P = 0.03) than subjects in the lower quantile of dietary polyphenol intake. We couldn’t find any significant differences between participants in term of other macro and micronutrients (P > 0.05).
Table 3 showed the association between total and special polyphenols with risk of NAFLD. In the crude model and in term of total polyphenols, we found a significant inverse correlation between amount of dietary polyphenols intake and odds of NAFLD (OR 0.65, CI 0.5–0.84; P = 0.007). Also, after adjusting for confounding factors, in the full adjusted model, again, participants in the higher quantile of total polyphenols had a significant lower odd of NAFLD compared the reference group (OR 0.65, CI 0.5–0.84; P = 0.007). Also, in the subgroup analysis, only in women, we found a significant inverse association between total polyphenols intake and odds of NAFLD (OR 0.64, CI 0.42–0.93; P = 0.001).
In term of total flavonoids intake, people in the upper quintile of total flavonoid dietary intake compared to the first quintile were not at a lower odd of developing NAFLD and the relationship was not significant in the crude (OR 1.26, CI 0.96–1.67; P = 0.47) and full adjusted model (OR 1.35, CI 0.99–1.87; P = 0.31). Also, in the subgroup analysis, we couldn’t find significant correlation between total flavonoids intake and NAFLD in men (OR 1.11, CI 0.64–1.95; P = 0.24) and women (OR 1.24, CI 0.84–1.82; P = 0.73).
In term of dietary phenolic acid, participants in the higher quantile of dietary phenolic acid than subjects in the reference group had a significant lower odd of NAFLD in the crude (OR 0.67, CI 0.52–0.86; P < 0.001) and full adjusted model (OR 0.72, CI 0.54–0.95; P < 0.001). Also, in the subgroup analysis, high intake of phenolics could show protective effects against NAFLD only in women (OR 0.66, CI 0.46–0.89; P < 0.001).
When we evaluated the association between dietary lignans intake and odds of NAFLD, it revealed that subjects in the higher quantiles of dietary lignans intake, had lower odds of NAFLD in the crude (OR 0.69, CI 0.52–0.87; P = 0.001) and adjusted model (OR 0.78, CI 0.65–0.97; P = 0.03). However, in the subgroup analysis based on gender, we couldn’t find any significant correlations.
Discussion
The findings from the investigation indicated that participants with higher amounts of total polyphenols had a lower risk of NAFLD than subjects with lower amount of intake. Also, the results of our study showed that people who consumed a higher amount of phenolic acid and lignan through diet were less at risk of developing NAFLD than participants with low amounts of intake. However, in term of total flavonoids intake and its association with risk of NAFLD, we couldn’t find a significant correlation.
Polyphenols, widely acknowledged as water-soluble antioxidants, are present in some foods. In a case–control investigation conducted by Salehi-sahlabadi et al., encompassing 225 participants diagnosed with NAFLD and 450 control subjects, it was revealed that those in the highest tertile of total flavonoids and total phenolic acids exhibited a reduced likelihood of NAFLD in comparison to those in the lowest tertile. However, after accounting for additional confounding factors, the connection between total flavonoids and the odds of NAFLD ceased to be significant19. These results were in line with our findings. Also, similar to our findings, Sohouli et al., in a different case–control study, discovered that individuals in the top tertile of lignans consumption demonstrated a 66% lower likelihood of developing NAFLD in comparison to those in the lowest tertile. Hower, They did not identify any substantial association between the dietary intake of overall flavonoids and total phenolic acids with liver disease30. In another population-based study among the 2694 adults from the Guangzhou Nutrition and Health Study, In their research, scientists observed a gradual association between higher flavonoid intakes and a decreased likelihood of deteriorating NAFLD31. In our study, contrary to the findings of that particular study, there was no notable association observed between total flavonoid consumption and the likelihood of developing NAFLD.
A lack of physical activity plays a role in the development of NAFLD by leading to dysfunction in adipocytes and fostering insulin resistance. This insulin resistance, in turn, activates sterol regulatory element-binding protein-1(SREBP-1), resulting in the accumulation of fat within hepatocytes, along with elevated levels of pro-inflammatory cytokines and lipotoxicity. As a result, the activation of inflammation and fibrosis occurred due to mitochondrial dysfunction triggered by oxidative stress and the generation of reactive oxygen species32.Polyphenols have the potential to safeguard against NAFLD by diminishing lipid accumulation, serving as antioxidants, demonstrating anti-inflammatory properties, and enhancing insulin sensitivity33,34,35. Insulin resistance is one of the important factors in the NAFLD pathogenesis. Insulin resistance resulted from elevated levels of non-esterified fatty acids (NEFA) liberated from adipose tissues and the intermediary byproducts of hepatic lipid synthesis or breakdown36. Polyphenols have the capacity to increase the expression of the PPARγ gene or act as agonists for PPARγ. Consequently, this leads to a reduction in TNF-α and IL-6 levels while promoting an increase in adiponectin, phosphoenolpyruvate carboxykinase, fatty acid transport protein, and insulin receptor substrate-2. These effects collectively contribute to the enhancement of insulin resistance37,38,39. Moreover, polyphenols increased the expression of the PPARα gene or protein. PPARα, prominently present in the liver, oversees the transport of NEFA and activates enzymes associated with β-oxidation. This regulatory action restricts inflammation by impeding NF-κB and diminishing the expression of C-reactive protein40. It should be noticed that due to the observational nature of this study, it is not possible to confirm the cause-and-effect relationship between the consumption of polyphenols and the odds of developing NAFLD, and in our study only correlation is shown.
In the present study, we found that subjects in the higher quantiles of lignin intake had a lower odd of developing NAFLD. The primary origins of lignin consumption in our study participants were derived from various dietary sources, including wheat flour-based breads, flaxseed, legumes, garlic, almonds, olive oil, and some vegetables. These food items constitute a significant portion of a nutritious dietary pattern and are associated with a reduced risk of NAFLD41. In an interventional study, Yari et al. showed that flaxseed supplementation as a main source of lignin among the patients with NAFLD caused a significant improvement in the liver steatosis and inflammation42,43,44,45.
Based on our knowledge, the present study was the first population-based study with a big sample size that evaluated the association between total polyphenols, total flavonoids, lignin and phenolic acid with odds of NAFLD. High sample size, multi-centeredness and accurate assessment of dietary intakes were other strengths of this study. However, the present study had some limitations that should be considered. Firstly, as we mentioned, the study's observational design limits the ability to establish a cause-and-effect relationship between polyphenol consumption and the odds of developing NAFLD. The findings demonstrate correlation rather than causation. Second, the dietary intake data relied on self-reported responses obtained through an FFQ. This method may be subject to recall bias and may not accurately reflect actual dietary habits. Third, despite adjusting for several confounding variables in the regression analyses, there may still be unaccounted or residual confounding factors that could influence the observed associations. Finally, the diagnosis of NAFLD relied on medical records and reports from individual family physicians. Variability in the accuracy and consistency of these records could affect the reliability of the NAFLD diagnosis.
Conclusion
Our findings revealed that higher intake of total polyphenols, phenolic acid, and lignin was associated with lower odds of NAFLD among adults in the Hoveyzeh cohort. This observation held true even after adjusting for potential confounding factors such as age, energy intake, gender, smoking, alcohol consumption, physical activity levels, BMI, and education level. However, no significant correlation was found between total flavonoids intake and the risk of NAFLD. Future research, including interventional studies and longitudinal investigations, is warranted to further elucidate the role of polyphenols in preventing and managing NAFLD. Nevertheless, our findings underscore the potential importance of dietary patterns rich in polyphenols as a component of strategies to mitigate the risk of NAFLD and its progression to advanced stages.
Data availability
The data that support the findings of this study are available from The Hoveyzeh Cohort Study (HCS), but restrictions apply to the availability of these data, which were used under license for the current study and so are not publicly available but is available with the corresponding author upon reasonable request.
References
Neuschwander-Tetri, B. A. Non-alcoholic fatty liver disease. BMC Med. 15, 1–6 (2017).
Francque, S. M. et al. Non-alcoholic fatty liver disease: A patient guideline. JHEP Rep. 3, 100322 (2021).
Huang, T., Behary, J. & Zekry, A. Non-alcoholic fatty liver disease: A review of epidemiology, risk factors, diagnosis and management. Intern. Med. J. 50, 1038–1047 (2020).
Stefan, N. & Cusi, K. A global view of the interplay between non-alcoholic fatty liver disease and diabetes. Lancet Diabetes Endocrinol. 10, 284–296 (2022).
Tilg, H., Adolph, T. E., Dudek, M. & Knolle, P. Non-alcoholic fatty liver disease: The interplay between metabolism, microbes and immunity. Nat. Metab. 3, 1596–1607 (2021).
Morvaridzadeh, M. et al. Effect of ginger (Zingiber officinale) supplementation on oxidative stress parameters: A systematic review and meta-analysis. J. Food Biochem. 45, e13612 (2021).
Aziz, T., Khan, A. A., Tzora, A., Voidarou, C. & Skoufos, I. Dietary implications of the bidirectional relationship between the gut microflora and inflammatory diseases with special emphasis on irritable bowel disease: Current and future perspective. Nutrients 15, 2956 (2023).
Mitra, S., De, A. & Chowdhury, A. Epidemiology of non-alcoholic and alcoholic fatty liver diseases. Transl. Gastroenterol. Hepatol. 5, 13 (2020).
Adibi, A., Maleki, S., Adibi, P., Etminani, R. & Hovsepian, S. Prevalence of nonalcoholic fatty liver disease and its related metabolic risk factors in Isfahan, Iran. Adv. Biomed. Res. 6, 47 (2017).
Souza, M. R. D. A., Diniz, M. D. F. F. D. M., Medeiros-Filho, J. E. M. D. & Araújo, M. S. T. D. Metabolic syndrome and risk factors for non-alcoholic fatty liver disease. Arquivos de Gastroenterologia 49, 89–96 (2012).
Pouwels, S. et al. Non-alcoholic fatty liver disease (NAFLD): A review of pathophysiology, clinical management and effects of weight loss. BMC Endocr. Disord. 22, 1–9 (2022).
Paternostro, R. & Trauner, M. Current treatment of non-alcoholic fatty liver disease. J. Intern. Med. 292, 190–204 (2022).
Aziz, T. et al. Genome investigation and functional annotation of Lactiplantibacillus plantarum YW11 revealing streptin and ruminococcin-A as potent nutritive bacteriocins against gut symbiotic pathogens. Molecules 28, 491 (2023).
Rahimlu, M., Shab-Bidar, S. & Djafarian, K. Body mass index and all-cause mortality in chronic kidney disease: A dose–response meta-analysis of observational studies. J. Renal Nutr. 27, 225–232 (2017).
Berná, G. & Romero-Gomez, M. The role of nutrition in non-alcoholic fatty liver disease: Pathophysiology and management. Liver Int. 40, 102–108 (2020).
Keshavarz, Z. et al. Non-alcoholic fatty liver disease and dairy products consumption: Results from FASA Persian cohort study. Front. Nutr. 9, 962834 (2022).
Parsi, A., Torkashvand, M., Hajiani, E., Rahimlou, M. & Sadeghi, N. The effects of crocus sativus extract on serum lipid profile and liver enzymes in patients with non-alcoholic fatty liver disease: A randomized placebo-controlled study. Obes. Med. 17, 100165 (2020).
Mohammadifard, N. et al. The effect of ketogenic diet on shared risk factors of cardiovascular disease and cancer. Nutrients 14, 3499 (2022).
Salehi-Sahlabadi, A. et al. Dietary polyphenols and the odds of non-alcoholic fatty liver disease: A case-control study. Clin. Nutr. ESPEN 41, 429–435 (2021).
Morvaridzadeh, M. et al. Effect of soy products and isoflavones on oxidative stress parameters: A systematic review and meta-analysis of randomized controlled trials. Food Res. Int. 137, 109578. https://doi.org/10.1016/j.foodres.2020.109578 (2020).
Rahimlou, M. et al. Effects of ginger supplementation on anthropometric, glycemic and metabolic parameters in subjects with metabolic syndrome: A randomized, double-blind, placebo-controlled study. J. Diabetes Metab. Disord. 18, 119–125 (2019).
Echeverría, F., Bustamante, A., Sambra, V., Videla, L. & Valenzuela, R. Beneficial effects of dietary polyphenols in the prevention and treatment of NAFLD: Cell-signaling pathways underlying health effects. Curr. Med. Chem. 29, 299–328 (2022).
Morvaridzadeh, M. et al. Effect of soy products and isoflavones on oxidative stress parameters: A systematic review and meta-analysis of randomized controlled trials. Food Research International 137, 109578 (2020).
Rodriguez-Ramiro, I., Vauzour, D. & Minihane, A. Polyphenols and non-alcoholic fatty liver disease: Impact and mechanisms. Proc. Nutr. Soc. 75, 47–60 (2016).
Mazidi, M., Katsiki, N. & Banach, M. A higher flavonoid intake is associated with less likelihood of nonalcoholic fatty liver disease: results from a multiethnic study. J. Nutr. Biochem. 65, 66–71 (2019).
Zhao, L. et al. Protective effects of five structurally diverse flavonoid subgroups against chronic alcohol-induced hepatic damage in a mouse model. Nutrients 10, 1754 (2018).
Poustchi, H. et al. Prospective epidemiological research studies in Iran (the PERSIAN Cohort Study): Rationale, objectives, and design. Am. J. Epidemiol. 187, 647–655 (2018).
Cheraghian, B. et al. Cohort profile: The Hoveyzeh Cohort Study (HCS): A prospective population-based study on non-communicable diseases in an Arab community of Southwest Iran. Med. J. Islamic Rep. Iran 34, 141 (2020).
Rothwell, J. A. et al. Phenol-explorer 3.0: A major update of the Phenol-Explorer database to incorporate data on the effects of food processing on polyphenol content. Database 2013, bat070 (2013).
Sohouli, M. H. & Lari, A. The association between polyphenols intake and odds of non-alcoholic fatty liver disease (NAFLD) among adult population. Int. J. Nutr. Sci. 5, 118–125 (2020).
Zhong, Q.-W. et al. Higher flavonoid intake is associated with a lower progression risk of non-alcoholic fatty liver disease in adults: A prospective study. Br. J. Nutr. 125, 460–470 (2021).
Buzzetti, E., Pinzani, M. & Tsochatzis, E. A. The multiple-hit pathogenesis of non-alcoholic fatty liver disease (NAFLD). Metabolism 65, 1038–1048 (2016).
Bayram, H. M., Majoo, F. M. & Ozturkcan, A. Polyphenols in the prevention and treatment of non-alcoholic fatty liver disease: An update of preclinical and clinical studies. Clin. Nutr. ESPEN 44, 1–14 (2021).
Williamson, G. & Sheedy, K. Effects of polyphenols on insulin resistance. Nutrients 12, 3135 (2020).
Rahimlou, M. & Dehghani, A. In Molecular Mechanisms of Action of Functional Foods and Nutraceuticals for Chronic Diseases 101–120 (CRC Press, 2023).
Sakurai, Y., Kubota, N., Yamauchi, T. & Kadowaki, T. Role of insulin resistance in MAFLD. Int. J Mol. Sci. 22, 4156 (2021).
Papuc, C., Goran, G. V., Predescu, C. N., Tudoreanu, L. & Ștefan, G. Plant polyphenols mechanisms of action on insulin resistance and against the loss of pancreatic beta cells. Crit. Rev. Food Sci. Nutr. 62, 325–352 (2021).
Shahwan, M., Alhumaydhi, F., Ashraf, G. M., Hasan, P. M. & Shamsi, A. Role of polyphenols in combating Type 2 diabetes and insulin resistance. Int. J. Biol. Macromol. 206, 567–579 (2022).
Aziz, T., Hussain, N., Hameed, Z. & Lin, L. Elucidating the role of diet in maintaining gut health to reduce the risk of obesity, cardiovascular and other age-related inflammatory diseases: Recent challenges and future recommendations. Gut Microbes 16, 2297864 (2024).
Liu, S., Yu, J., Fu, M., Wang, X. & Chang, X. Regulatory effects of hawthorn polyphenols on hyperglycemic, inflammatory, insulin resistance responses, and alleviation of aortic injury in type 2 diabetic rats. Food Res. Int. 142, 110239 (2021).
Zamora-Ros, R. et al. The association between dietary flavonoid and lignan intakes and incident type 2 diabetes in European populations: The EPIC-InterAct study. Diabetes Care 36, 3961–3970 (2013).
Yari, Z. et al. Flaxseed supplementation in non-alcoholic fatty liver disease: A pilot randomized, open labeled, controlled study. Int. J. Food Sci. Nutr. 67, 461–469 (2016).
Morshedzadeh, N. et al. The effects of flaxseed supplementation on metabolic syndrome parameters, insulin resistance and inflammation in ulcerative colitis patients: An open-labeled randomized controlled trial. Phytother. Res. 35, 3781–3791 (2021).
Zahid, H. et al. Assessing the effect of walnut (Juglans regia) and olive (Olea europaea) oil against the bacterial strains found in Gut Microbiome. Progr. Nutr. 27, 1–13 (2022).
Morshedzadeh, N. et al. Association between adipokines levels with inflammatory bowel disease (IBD): Systematic reviews. Digest. Dis. Sci. 62, 3280–3286 (2017).
Funding
This work was supported by the Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran.
Author information
Authors and Affiliations
Contributions
S.A.H. conceived the study, M.R., Z.R., N.S., N.B.J., G.B., A.K. and B.C.H. collected the data. R.T., and M.R. analyzed data. S.A.H. and Z.R. interpreted the statistical analyses and M.R. wrote the first draft of the manuscript. S.A.H., G.B. and A.K. contributed to the manuscript revising and editing. All of the authors critically revised the manuscript. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Rahimlou, M., Baghdadi, G., Khodi, A. et al. Polyphenol consumption and Nonalcoholic fatty liver disease risk in adults. Sci Rep 14, 6752 (2024). https://doi.org/10.1038/s41598-024-57416-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-57416-0
Keywords
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
