
Abstract
The COVID-19 pandemic has impacted individuals differently, and there's been a growing body of evidence pointing to neurological complications caused by the virus. However, our understanding of the range of neurological issues linked to SARS-CoV-2 infection in children is limited. This systematic review and meta-analysis aimed to assess the abnormal neuroimaging findings in pediatric COVID-19 patients, shedding light on this crucial aspect of the disease's impact on children. We conducted an extensive search in the PubMed, Medline, and ScienceDirect databases for observational studies reporting neuroimaging findings of the brain and spinal cord in children with COVID-19 between December 1, 2019, and October 30, 2021. Grey literature sources, including medRxiv and Google Scholar, were also explored. Pooled proportions of abnormal neuroimaging findings, categorized into neurovascular findings, ADEM-like lesions, encephalitic pattern, myelitis, transient splenial lesions, and other anomalies, were calculated using a random-effects model. Between-study heterogeneity was assessed using the χ2 statistic for pooled proportions and the inconsistency index I2. The Quality of the studies was evaluated using the NIH Quality Assessment Tool and the adapted Newcastle–Ottawa Scale. Our search yielded 9,605 articles, with 96 studies (involving 327 pediatric patients) included in the qualitative analysis. Of these, five reports (encompassing 111 patients) underwent quantitative analysis. The pooled proportion of pediatric COVID-19 patients with neurological symptoms and exhibiting abnormal neuroimaging findings was 43.74%. These findings were further categorized into neurovascular findings (8.22%), ADEM-like lesions (7.69%), encephalitic pattern (13.95%), myelitis (4.60%), transient splenial lesions (16.26%), and other abnormalities (12.03%). Insignificant between-study heterogeneity was observed in all categories, and our analysis did not reveal significant publication bias. In conclusion, a substantial proportion of pediatric COVID-19 patients with neurological symptoms have abnormal neuroimaging findings, underscoring the need for vigilant monitoring of neurological complications in this vulnerable population. Standardized reporting and long-term follow-up studies are essential to fully understand the implications of these findings. Collaborative research efforts will deepen our understanding of COVID-19's neurological dimensions in children and enhance clinical care for this population.
Similar content being viewed by others

Introduction
The coronavirus disease 2019 (COVID-19) pandemic, stemming from the highly pathogenic severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), emerged in December 2019 and swiftly evolved into a global crisis, affecting millions of individuals worldwide. With over 600 million confirmed cases and more than 6 million confirmed deaths as of March 20231,2, the pandemic has underscored the urgent need for a comprehensive understanding of its multifaceted impacts on human health.
Initially characterized by predominantly respiratory symptoms, COVID-19's complex clinical presentation has expanded to encompass a diverse array of manifestations. While the elderly with coexisting health conditions bore the brunt of severe outcomes, the pediatric population experienced comparatively mild disease courses, with some children remaining asymptomatic altogether3. However, as the pandemic progressed, the constellation of symptoms associated with COVID-19 extended beyond respiratory involvement, increasingly encompassing neurological manifestations4.
The neurological facet of COVID-19 has garnered significant attention due to its potential implications for both acute clinical care and long-term health outcomes. Although non-specific neurological symptoms such as headache, anosmia, dysgeusia, dizziness, disturbed consciousness, and paresthesia have been reported, a growing number of adult COVID-19 patients have exhibited distinct neurological conditions, including acute cerebrovascular disease, encephalitis, seizure, Guillain-Barré syndrome (GBS), and Miller Fisher syndrome (MFS)5,6,7. The surge in published literature has documented substantial incidences of abnormal neuroimaging findings in adults with COVID-19, adding complexity to the spectrum of the disease's presentation.
In the pediatric population, the scenario is equally intricate. An immune-mediated syndrome known as pediatric multisystem inflammatory syndrome, emerging during the latent phase of COVID-19, has been documented, with some children experiencing neurological symptoms accompanied by alterations in brain imaging8. The range of neuroimaging findings in children with COVID-19 encompasses cytotoxic lesions of the corpus callosum (CLOCCs), idiopathic intracranial hypertension (IIH), arterial ischemic stroke (AIS), hemorrhagic posterior reversible encephalopathy syndrome (PRES), and acute disseminated encephalomyelitis (ADEM)9,10,11,12,13. Notably, the burgeoning literature on COVID-19-related neuroimaging findings in children has largely consisted of case reports and series, which, while informative, possess limitations in providing comprehensive evidence-based incidence data.
Addressing this research gap, the current study embarks on a systematic review and meta-analysis to collate the diverse radiological findings reported in the evolving corpus of literature on children with COVID-19. By employing rigorous methodology, this study aims to synthesize data from various observational study designs. Ultimately, our objective is to derive a comprehensive and pooled estimate of the incidence of neuroimaging abnormalities in this pediatric population. This endeavor not only contributes to enhancing our understanding of the neurological aspects of COVID-19 in children but also provides vital evidence for radiologists and clinicians faced with interpreting neuroimaging findings in the context of COVID-19.
Methods
This systematic review and meta-analysis were conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines14.
Literature search
A comprehensive search was executed in PubMed, Medline, and ScienceDirect databases to identify studies published between December 1, 2019, and October 30, 2021. For PubMed and Medline, the search utilized MeSH terms and keywords in the title/abstract field: (Coronavirus disease OR Novel coronavirus OR 2019-nCoV OR SARS-CoV-2 OR Covid-19 OR Severe Acute Respiratory Syndrome Coronavirus 2) AND (Brain OR Central nervous system OR CNS OR spinal cord OR peripheral nervous system OR PNS OR neurological) AND (CT OR computed tomography OR MRI OR magnetic resonance imaging OR neuroimaging OR imaging OR neuroradiology OR radiology) AND (Children OR child OR pediatric OR "child, preschool"[MeSH Terms] OR "Adolescent"[MeSH Terms]). This search was conducted on April 16, 2022.
In ScienceDirect, due to limitations in allowed Boolean terms, three separate searches were conducted for relevant imaging-related keywords and COVID-19, with the final results merged. This search was performed on April 17, 2022. The following keywords, with the title/abstract/keywords field and a filter restricting results to 2019/2020/2021, were used: (CT OR computed tomography OR MRI OR magnetic resonance imaging OR imaging OR neuroimaging OR radiology) AND (Child OR pediatric), (Coronavirus disease OR Novel coronavirus OR 2019-nCoV OR SARS-CoV-2 OR Covid-19 OR Severe Acute Respiratory Syndrome Coronavirus 2) AND (child OR pediatric), (Brain OR Central nervous system OR CNS OR spinal cord OR peripheral nervous system OR PNS OR neurological) AND (child OR pediatric).
Additional sources were identified by reviewing reference lists of relevant articles. Grey literature was explored through platforms like medRxiv using the following keywords in full text, abstract, or title: "Coronavirus disease" AND neurological AND imaging AND Children, with a filter for 2019 to 2021. Google Scholar was also used with the same keywords as PubMed and Medline, and filters set for anywhere in the article and 2019 to 2021. Manual searches of related articles were also conducted. These websites were accessed on 4/1/2023, 2/2/2023, and 28/2/2023, respectively. The literature search was conducted by a single reviewer. The author was not blinded to authors, institutions, or journals during study selection or data extraction. Literature management was facilitated using EndNote version X915.
Inclusion and exclusion criteria
Included in this study were investigations of imaging findings of the brain and spinal cord in children with COVID-19. The following inclusion criteria were applied: (1) Population: Children (age ≤ 18) diagnosed with COVID-19. (2) Study design: All observational studies (case-series, case reports, cross-sectional, case–control, and cohort studies) were eligible. (3) Studies conducted between December 2019 and October 2021. (4) Outcomes: Imaging findings of the brain and spinal cord in COVID-19 patients with neurological symptoms. Only imaging findings at presentation were considered, excluding findings after treatment or follow-up.
Exclusion criteria were as follows: (1) Reviews, editorials, and letters. (2) Articles not written in English. (3) Non-human studies. A single reviewer reviewed the literature.
Data extraction
Data from selected articles were extracted into standardized formats, encompassing: (a) Study characteristics: First author's name and year of publication, country of origin, study design, sample size, article quality; (b) Patient demographic and clinical details: age, sex, imaging modality and specifications, number of neuroradiologist reviewers and their experience, reported neurological symptoms, frequency and proportion of positive neuroimaging findings, specific neuroimaging findings, pre-existing medical conditions. Data extraction was performed by one reviewer and validated for accuracy.
Quality assessment
Quality assessment of included studies was conducted by one reviewer at the study level. The NIH quality assessment tool for case reports and case series and the adapted Newcastle–Ottawa Scale for other designs were utilized for quality evaluation16,17.
Synthesis methods
The synthesis of results in this systematic review employed a narrative and quantitative approach to address the research questions. Case reports, case studies, case–control, and cross-sectional studies underwent a narrative synthesis, which entailed summarizing their findings to identify diverse radiological observations. Meanwhile, cohort studies with sample sizes greater than 10 underwent quantitative synthesis, utilizing meta-analysis techniques to estimate the incidence of neuroimaging abnormalities in the pediatric population. The primary outcomes of this meta-analysis were pooled proportion estimates of abnormal neuroimaging findings, categorized as neurovascular findings (arterial or venous stroke), ADEM-like lesions (autoimmune), encephalitic pattern (Acute Hemorrhagic Necrotizing Encephalitis), myelitis (Longitudinally Extensive Transverse Myelitis), transient splenial lesions (RESLES, MERS), and others (PRES, neuritis, brain edema, etc.).
For meta-analytic pooling of data, the random-effects model with variance stabilization was used, employing the Freeman-Tukey double arc-sine transformation18. Pooled proportions with 95% confidence intervals were derived using the Der Simonian-Laird random-effects model19. Between-study heterogeneity was assessed using χ2 statistics for pooled estimates (P < 0.05 indicating significant heterogeneity) and the Higgin's inconsistency index (I2), where I2 values of 0–40%, 30–60%, 50–90%, and 75–100% indicated insignificant, moderate, substantial, and considerable heterogeneity, respectively20. Publication bias was evaluated through Funnel plots, the Beggar's test, and Egger's tests21. All statistical analyses were performed using R22. A P-value of < 0.05 was considered statistically significant.
Results
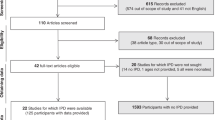
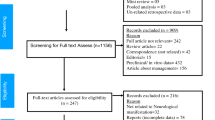
A flowchart representing the publication selection process is presented in Fig. 1. The initial literature search yielded 9605 articles. After removing duplicates, 8208 articles were subjected to eligibility screening. Among these, 7907 were excluded based on the assessment of their titles and abstracts, and 32 reports were not accessible. The full texts of the remaining 269 articles were comprehensively reviewed; 227 articles were further excluded due to various reasons such as lack of brain and spine imaging, lack of neurological symptoms, partial overlap with patient cohorts, inclusion of adult populations, insufficient details, and absence of Covid-19 infection. In cases of overlapping cohorts, preference was given to the study with more relevant information about abnormal findings. An additional 252 studies were identified through other methods (reference lists, Google Scholar, medRxiv), out of which 240 were thoroughly reviewed for eligibility. Among these, 186 were excluded due to similar reasons as mentioned before. In total, 96 articles, involving a cumulative 327 patients, were included in the qualitative review. Within the 96 articles, 5 reports encompassing 111 patients were considered for quantitative analyses23,24,25,26,27,28,29.

Flow diagram depicting the study eligibility criteria.
The characteristics of the 96 included studies are summarized in Table 1 and Supplementary Tables S1, S2 and S3. Among these, 75 were categorized as case reports or case series, while 21 were classified as cross-sectional, case–control, or cohort studies. Within the latter group, 17 studies were retrospective, 3 were prospective, and one exhibited both retrospective and prospective elements. The selected studies originated from diverse countries, including China, Turkey, Iran, Argentina, Bangladesh, Brazil, Chile, France, India, Ireland, Italy, Kosovo, Saudi Arabia, Mexico, Peru, Republic of Macedonia, Spain, Switzerland, the UK, and the USA. One study was a multinational collaboration involving France, the UK, the USA, Brazil, Argentina, India, Peru, and Saudi Arabia. Among the included studies, 49 employed MR as the sole neuroimaging modality, 10 utilized CT exclusively, and 35 employed various modalities like MR, CT, US, and OCT. Two studies did not report the modalities used30,31.
Table 2 and Supplementary Table S4 provide detailed information about the neuroimaging findings in children with COVID-19. Supplementary Table S4 contains detailed information on neuroimaging findings in case reports and case series studies, while Table 2 provides detailed information on neuroimaging findings in other types of observational studies. For cross-sectional and case–control studies with low sample sizes, only descriptive analysis was performed. In contrast, meta-analysis was conducted for cohort studies with a sample size greater than 10.
In the pool of included studies, 43.74% (95% CI 17.55 to 71.77%) of the children exhibited abnormal neuroimaging findings. Please refer to Supplementary Table S5 for detailed information. The pooled incidence of neurovascular findings was 8.22% (95% CI 2.57 to 16.00%; I2 = 0.00%). The pooled incidence of ADEM-like lesions was 7.69% (95% CI 1.89 to 16.13%; I2 = 0.00%). The pooled incidence of encephalitic pattern was 13.95% (95% CI 0.86 to 36.15%; I2 = 73.32%). The pooled incidence of myelitis was 4.60% (95% CI 0.33 to 11.87%; I2 = 0.00%). The pooled incidence of transient splenial lesions was 16.26% (95% CI 6.93 to 28.02%; I2 = 36.19%). The pooled incidence of other abnormalities was 12.03% (95% CI 4.75 to 21.48%; I2 = 34.50%) (Table 3 and Fig. 2).

Forest plots of pooled proportions. Forest plots of pooled proportions of (a) Abnormal neuroimaging findings, (b) Neurovascular findings, (c) ADEM-like lesions, (d) Encephalitic pattern, (e) Myelitis, (f) Transient splenial lesions, and (g) Other events in children with COVID-19.
All included studies exhibited no significant publication bias in funnel plots (indicating symmetric distribution of studies), Beggar’s test (P = 0.4833), and Egger’s tests (P = 0.3369) (P > 0.05) (Fig. 3). All included studies had insignificant between-study heterogeneities (P > 0.05) (Table 3).

Funnel plots of pooled proportions. Funnel plots of pooled proportions of (a) & (b) Abnormal neuroimaging findings in children with COVID-19.
The quality assessment, utilizing the NIH quality assessment tool for case report and case series studies, and the Newcastle–Ottawa Scale (NOS) for other study designs, indicated an overall fair quality, categorized as good, fair, or poor on the quality scale (Fig. 4).

The quality assessment of included studies. Proportion of studies with poor, fair, or good quality categorized by study type.
Discussion
The emergence of the COVID-19 pandemic caused by the novel coronavirus, SARS-CoV-2, has evolved into a global health crisis. Initially focused on respiratory symptoms, it's now clear that COVID-19 presents a complex clinical picture affecting various organ systems32,33. Neurological manifestations have gained attention for their potential impact on both immediate clinical care and long-term health outcomes34,35. This systematic review and meta-analysis aimed to provide a comprehensive assessment of the abnormal neuroimaging findings in children with COVID-19.
Our findings reveal that a substantial proportion of pediatric COVID-19 patients with neurological symptoms exhibit abnormal neuroimaging findings, with 43.74% of children in the included studies demonstrating such abnormalities. These findings underscore the importance of considering neurological complications in the management of pediatric COVID-19 cases.
In a systematic review conducted by Choi et al. an extensive exploration was undertaken to comprehensively assess the spectrum of COVID-19-related neurological manifestations and associated abnormal neuroimaging findings in adults. Their meta-analysis unveiled that 42.6% of adult patients exhibited abnormal neuroimaging findings, as observed through brain CT or MRI36. With acute to subacute infarcts were the most common (24.0%), followed by cerebral micro hemorrhages (6.9%), acute spontaneous intracerebral hemorrhages (5.4%), and encephalitis/encephalopathy (3.3%)36. It is important to note that their investigation exclusively centered on specific COVID-19-related neuroimaging findings in the adult population and specifically considered MRI and CT as the imaging modalities of interest, although acknowledging that alternate modalities such as OCT, and TCD are also utilized.
In contrast, our study takes a unique approach, focusing exclusively on the pediatric group of COVID-19 patients, which is an area with limited research. Additionally, we aimed to cover a wide range of neuroimaging findings using diverse range of methods commonly used in pediatric cases. This broader scope is in response to the frequent use of various imaging techniques in pediatric clinical settings, extending the depth of our investigation.
In terms of specific neuroimaging abnormalities, our analysis categorized them into neurovascular findings, ADEM-like lesions, encephalitic pattern, myelitis, transient splenial lesions, and other findings. Neurovascular findings, encompassing findings like arterial or venous stroke, exhibited a pooled incidence of 8.22%. ADEM-like lesions showed a pooled incidence of 7.69%. Encephalitic pattern, including findings like Acute Hemorrhagic Necrotizing Encephalitis, showed a pooled incidence of 13.95%. Myelitis had a pooled incidence of 4.60%. Transient splenial lesions, encompassing findings like RESLES and MERS, exhibited a pooled incidence of 16.26%. Other abnormalities, such as PRES, neuritis, and brain edema, had a pooled incidence of 12.03%. These findings emphasize the diversity of neurological involvement in pediatric COVID-19 cases, spanning from inflammatory processes to vascular events.
In a recent systematic review led by Falsaperla et al. in 2023, undertook an exhaustive examination of COVID-19-related neurological manifestations in the pediatric population. Although this study primarily emphasized clinical symptoms, it did not include a meta-analytic assessment. Nevertheless, their conclusions align closely with our own findings, albeit with distinct categorization. Their results highlighted that encephalitis represented the most frequent diagnosis, accounting for 20.83% of cases, followed by seizures (10.42%), GBS (10.42%), cerebrovascular involvement (10.42%), ADEM (8.33%), and encephalopathy (8.33%). Additionally, a fraction of cases exhibited neurological signs secondary to central nervous system lesions (4.17%), and peripheral neuropathy (4.17%)37.
The cellular and molecular basis of SARS-CoV-2's ability to affect the nervous system is not fully understood. In light of this, several theoretical mechanisms have been posited to shed light on the acute and postacute neurological manifestations associated with COVID-19. Firstly, one hypothesis proposes that SARS-CoV-2 exhibits an affinity for infecting olfactory neurons, subsequently spreading through axons and across the synapse, thereby causing central nervous system infection38. Secondly, considering the viral-induced depletion of ACE-2, there is a perturbation in the renin-angiotensin system equilibrium. Consequently, a prothrombotic state may ensue, impairing both large vessel and microvascular blood flow. This vascular dysfunction heightens the risk of thrombotic and hemorrhagic stroke following SARS-CoV-2 infection39. Thirdly, perhaps the most pivotal mechanism at play is immune dysregulation, culminating in autoimmunity and hyperinflammatory responses. The aberrant immune response is recognized as a central contributor to neurological involvement in COVID-19 cases40. Lastly, the cytokine storm and systemic hyperinflammatory responses incited by the virus present an additional avenue through which neurological manifestations may occur. Elevated pro-inflammatory cytokine levels can disrupt normal neuronal function, impede neurotransmitter systems, and induce neuronal damage41,42. Understanding the mechanisms responsible for the neurological manifestations of COVID-19 is crucial for the development of potential therapeutic interventions. These mechanisms can operate independently or in concert within individual patients, giving rise to a range of clinical and neuroimaging presentations that, while varied, often exhibit overlapping features. This underscores the significance of investigating these mechanisms in our pursuit of effective treatments43.
The observed incidence of neurological abnormalities in pediatric COVID-19 patients raises several important clinical and research implications. First, it highlights the necessity for a high index of suspicion for neurological complications in children with COVID-19, especially those presenting with neurological symptoms. Timely neuroimaging assessments and consultations with pediatric neurologists may be essential for early diagnosis and appropriate management.
Second, the findings of this study emphasize the importance of continued research into the long-term consequences of COVID-19 in children. Even in cases where acute neurological symptoms resolve, it remains to be seen whether these children may be at risk of long-term cognitive or neurological sequelae. Longitudinal studies are needed to assess the evolution of these abnormalities and their potential impact on a child's development and quality of life.
To the best of our knowledge, this study represents the first systematic review and meta-analysis of neuroimaging findings in pediatric SARS-CoV-2 cases. Nonetheless, it is important to acknowledge several limitations of this study. Firstly, some of the studies included in our analysis exhibited substantial heterogeneity, attributed to variations in study designs, patient cohorts, and imaging protocols. This inherent diversity, though mitigated through statistical methods, somewhat limits the generalizability of our findings. Secondly, the potential presence of publication bias, although not overtly evident in our assessments, cannot be entirely dismissed. Thirdly, the relatively limited number of studies constrained our ability to conduct more detailed subgroup analyses and explore specific aspects comprehensively. Moreover, in this study, our research commenced on December 1, 2019. It is essential to acknowledge a limitation related to the evolving nature of information about COVID-19 during that early period. Detailed and comprehensive information about COVID-19, including its clinical manifestations and neurological implications, may not have been readily available at the beginning of our study. As a result, some aspects of our analysis may be based on limited data and evolving knowledge in the early stages of the pandemic. Furthermore, establishing a causal relationship between COVID-19 infection and the observed neuroimaging abnormalities remains an ongoing area of investigation. These abnormalities may be influenced by systematic confounding factors such as comorbidities, mechanical ventilation, and the complex pharmacological regimens administered for respiratory distress with hypoxia. These limitations underscore the necessity for future prospective studies that consider comorbidities and conduct more intricate analyses to affirm the potential association between COVID-19 and neuroimaging findings.
Conclusion
In conclusion, this systematic review and meta-analysis highlight the incidence of abnormal neuroimaging findings in children with COVID-19. The findings underscore the importance of vigilance for neurological complications in pediatric COVID-19 cases, as well as the need for standardized reporting and long-term follow-up to better understand the implications of these abnormalities. Further research and collaboration are essential to deepen our understanding of the neurological aspects of COVID-19 in children and to improve clinical care for this vulnerable population.
Data availability
All data generated or analyzed during this study are included in this published article (and its Supplementary Information files).
References
COVID-19 Map: Johns Hopkins Coronavirus Resource Center. https://coronavirus.jhu.edu/map.html (Accessed 19 August 2023).
Zhu, N. et al. A novel coronavirus from patients with pneumonia in China, 2019. N. Engl. J. Med. 382, 727–733. https://doi.org/10.1056/NEJMoa2001017 (2020).
Parri, N., Lenge, M. & Buonsenso, D. Children with Covid-19 in pediatric emergency departments in Italy. N. Engl. J. Med. 383, 187–190. https://doi.org/10.1056/NEJMc2007617 (2020).
Niazkar, H. R., Zibaee, B., Nasimi, A. & Bahri, N. The neurological manifestations of COVID-19: A review article. Neurol. Sci. Off. J. Ital. Neurol. Soc. Ital. Soc. Clin. Neurophysiol. 41, 1667–1671. https://doi.org/10.1007/s10072-020-04486-3 (2020).
Asadi-Pooya, A. A. & Simani, L. Central nervous system manifestations of COVID-19: A systematic review. J. Neurol. Sci. 413, 116832. https://doi.org/10.1016/j.jns.2020.116832 (2020).
Gutiérrez-Ortiz, C. et al. Miller Fisher syndrome and polyneuritis cranialis in COVID-19. Neurology 95, e601–e605. https://doi.org/10.1212/wnl.0000000000009619 (2020).
Toscano, G. et al. Guillain-Barré syndrome associated with SARS-CoV-2. N. Engl. J. Med. 382, 2574–2576. https://doi.org/10.1056/NEJMc2009191 (2020).
Abdel-Mannan, O. et al. Neurologic and radiographic findings associated with COVID-19 infection in children. JAMA Neurol. 77, 1440–1445. https://doi.org/10.1001/jamaneurol.2020.2687 (2020).
Aksu Uzunhan, T. et al. Cytotoxic lesions of the corpus callosum in children: Etiology, clinical and radiological features, and prognosis. Brain Dev. 43, 919–930. https://doi.org/10.1016/j.braindev.2021.05.001 (2021).
Al Haboob, A. A. Miller Fischer and posterior reversible encephalopathy syndromes post COVID-19 infection. Neurosciences (Riyadh, Saudi Arabia) 26, 295–299. https://doi.org/10.17712/nsj.2021.3.20210002 (2021).
Aljomah, L. et al. Pediatrics COVID-19 and neurological manifestations: Single tertiary centre experience. eNeurologicalSci 24, 100355. https://doi.org/10.1016/j.ensci.2021.100355 (2021).
Appavu, B. et al. Arteritis and large vessel occlusive strokes in children after COVID-19 infection. Pediatrics https://doi.org/10.1542/peds.2020-023440 (2021).
de Miranda Henriques-Souza, A. M. et al. Acute disseminated encephalomyelitis in a COVID-19 pediatric patient. Neuroradiology 63, 141–145. https://doi.org/10.1007/s00234-020-02571-0 (2021).
Page, M. J. et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 372, n71. https://doi.org/10.1136/bmj.n71 (2021).
EndNote v. EndNote X9 (Clarivate, 2013).
Quality Assessment Tool for Case Series studies. National Heart, Lung, and Blood Institute. https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools
Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 25, 603–605. https://doi.org/10.1007/s10654-010-9491-z (2010).
Lin, L. & Xu, C. Arcsine-based transformations for meta-analysis of proportions: Pros, cons, and alternatives. Health Sci. Rep. 3, e178. https://doi.org/10.1002/hsr2.178 (2020).
DerSimonian, R. & Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 7, 177–188. https://doi.org/10.1016/0197-2456(86)90046-2 (1986).
Higgins, J. P., Thompson, S. G., Deeks, J. J. & Altman, D. G. Measuring inconsistency in meta-analyses. BMJ 327, 557–560. https://doi.org/10.1136/bmj.327.7414.557 (2003).
Egger, M., Davey Smith, G., Schneider, M. & Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 315, 629–634. https://doi.org/10.1136/bmj.315.7109.629 (1997).
R: A Language and Environment for Statistical Computing (R Foundation for Statistical Computing, 2023).
Caro-Domínguez, P. et al. Imaging findings of multisystem inflammatory syndrome in children associated with COVID-19. Pediatr. Radiol. 51, 1608–1620. https://doi.org/10.1007/s00247-021-05065-0 (2021).
Coronado Munoz, A. et al. High incidence of stroke and mortality in pediatric critical care patients with COVID-19 in Peru. Pediatr. Res. 91, 1730–1734. https://doi.org/10.1038/s41390-021-01547-x (2022).
Lindan, C. E. et al. Neuroimaging manifestations in children with SARS-CoV-2 infection: A multinational, multicentre collaborative study. Lancet Child Adolesc. Health 5, 167–177. https://doi.org/10.1016/s2352-4642(20)30362-x (2021).
Orman, G. et al. Neuroimaging offers low yield in children positive for SARS-CoV-2. AJNR Am. J. Neuroradiol. 42, 951–954. https://doi.org/10.3174/ajnr.A7022 (2021).
Palabiyik, F. et al. Imaging of multisystem inflammatory disease in children (MIS-C) associated with COVID-19. Acad. Radiol. 28, 1200–1208. https://doi.org/10.1016/j.acra.2021.05.030 (2021).
Penner, J. et al. 6-month multidisciplinary follow-up and outcomes of patients with paediatric inflammatory multisystem syndrome (PIMS-TS) at a UK tertiary paediatric hospital: A retrospective cohort study. Lancet Child Adolesc. Health 5, 473–482. https://doi.org/10.1016/S2352-4642(21)00138-3 (2021).
Ray, S. T. J. et al. Neurological manifestations of SARS-CoV-2 infection in hospitalised children and adolescents in the UK: A prospective national cohort study. Lancet Child Adolesc. Health 5, 631–641. https://doi.org/10.1016/S2352-4642(21)00193-0 (2021).
Balagurunathan, M., Natarajan, T., Karthikeyan, J. & Palanisamy, V. Clinical spectrum and short-term outcomes of multisystem inflammatory syndrome in children in a south Indian hospital. Clin. Exp. Paediatr. 64, 531–537. https://doi.org/10.3345/cep.2021.00374 (2021).
de Oliveira, M. R., Lucena, A. R. V. P., Higino, T. M. M. & Ventura, C. V. Oculomotor nerve palsy in an asymptomatic child with COVID-19. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 25, 169–170. https://doi.org/10.1016/j.jaapos.2021.02.001 (2021).
Li, X. et al. Differences in clinical features and laboratory results between adults and children with SARS-CoV-2 infection. BioMed. Res. Int. 2020, 6342598. https://doi.org/10.1155/2020/6342598 (2020).
Russo, T. et al. Gastrointestinal manifestations, clinical characteristics and outcomes of COVID-19 in adult and pediatric patients. SOJ Microbiol. Infect. Dis. 8, 1–14 (2021).
Frontera, J. A. et al. A prospective study of long-term outcomes among hospitalized COVID-19 patients with and without neurological complications. J. Neurol. Sci. 426, 117486. https://doi.org/10.1016/j.jns.2021.117486 (2021).
Paterson, R. W. et al. The emerging spectrum of COVID-19 neurology: Clinical, radiological and laboratory findings. Brain J. Neurol. 143, 3104–3120. https://doi.org/10.1093/brain/awaa240 (2020).
Choi, Y. & Lee, M. K. Neuroimaging findings of brain MRI and CT in patients with COVID-19: A systematic review and meta-analysis. Eur. J. Radiol. 133, 109393. https://doi.org/10.1016/j.ejrad.2020.109393 (2020).
Falsaperla, R., Gulisano, C., Portale, L., Maccarrone, A. & Ruggieri, M. A critical appraisal of neurological evidence on paediatric COVID-19 patients. A systematic literature review. Heliyon 9, e15630. https://doi.org/10.1016/j.heliyon.2023.e15630 (2023).
Meinhardt, J. et al. Olfactory transmucosal SARS-CoV-2 invasion as a port of central nervous system entry in individuals with COVID-19. Nat. Neurosci. 24, 168–175. https://doi.org/10.1038/s41593-020-00758-5 (2021).
Schober, M. E., Pavia, A. T. & Bohnsack, J. F. Neurologic manifestations of COVID-19 in children: Emerging pathophysiologic insights. Pediatr. Crit. Care Med. 22, 655–661 (2021).
Schober, M. E., Robertson, C. L., Wainwright, M. S., Roa, J. D. & Fink, E. L. COVID-19 and the pediatric nervous system: Global collaboration to meet a global need. Neurocrit. Care 35, 283–290. https://doi.org/10.1007/s12028-021-01269-2 (2021).
Boldrini, M., Canoll, P. D. & Klein, R. S. How COVID-19 affects the brain. JAMA Psychiatry 78, 682–683. https://doi.org/10.1001/jamapsychiatry.2021.0500 (2021).
Huang, C. et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 395, 497–506. https://doi.org/10.1016/S0140-6736(20)30183-5 (2020).
Garg, R. K. Spectrum of neurological manifestations in Covid-19: A review. Neurol. India 68, 560–572. https://doi.org/10.4103/0028-3886.289000 (2020).
Author information
Authors and Affiliations
Contributions
G.H.S. and R.E.M. contributed to this work as co-first authors. L.A.A. contributed to this work as co-second author. G.H.S. wrote the manuscript. R.E.M. assessed and reviewed the manuscript throughout the whole process of writing it down. L.A.A. mainly contributed to the analysis and results sections.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Safadieh, G.H., El Majzoub, R. & Abou Abbas, L. Neuroimaging findings in children with COVID-19 infection: a systematic review and meta-analysis. Sci Rep 14, 4790 (2024). https://doi.org/10.1038/s41598-024-55597-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-55597-2
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
