
Abstract
In this study, we aimed to separately evaluate the relationship between waist circumference and the incidence of hyperuricemia in men and women in the general Japanese population. We performed a population-based longitudinal study using data from the annual health examination of residents of Iki City, Japan. A total of 5567 participants without hyperuricemia at baseline were included in the analysis. The men and women were placed into groups according to the tertile of waist circumference. The outcome was incident hyperuricemia (uric acid > 416 µmol/L [7.0 mg/dL]). The relationship between waist circumference and the incidence of hyperuricemia was investigated using Cox proportional hazards models. During the follow-up period, hyperuricemia developed in 697 people (551 men and 146 women). The incidence (per 1000 person-years) of hyperuricemia increased with increasing waist circumference in the men (34.9 for tertile 1, 49.9 for tertile 2 and 63.3 for tertile 3; Ptrend < 0.001) and women (5.5 for tertile 1, 6.3 for tertile 2 and 11.9 for tertile 3; Ptrend < 0.001). Significant associations were identified after adjustment for potential confounders (men: Ptrend < 0.001; women: Ptrend = 0.014). In conclusion, both men and women with larger waist circumferences were at higher risks of subsequent hyperuricemia.
Similar content being viewed by others
Introduction
Hyperuricemia is a substantial risk factor for gouty arthritis owing to urate deposition and ureteral stones1. In recent years, hyperuricemia has also been reported to be associated with higher risks of chronic kidney disease (CKD), cardiovascular disease and all-cause mortality2. The prevention of hyperuricemia and subsequent gout, ureteral stones, CKD, cardiovascular disease and death requires an approach based on the latest information regarding the risk factors.
The links of fat distribution with subsequent gout and urinary tract stone disease has been recognised since the 1950s3. In addition to overall obesity, abdominal obesity has been reported to be strongly associated with metabolic disorders and greater risks of various diseases4,5,6. Although the body mass index (BMI) is commonly used in clinical practice, it cannot distinguish fat mass from lean mass and does not provide information regarding fat distribution. Current evidence regarding the relationship between obesity and hyperuricemia is derived mainly from observational studies in which BMI was used; Therefore, the link between abdominal obesity (which closely correlates with waist circumference7,8) and uric acid metabolism has not been well characterised. Two previous cross-sectional studies have shown significant associations between waist circumference and hyperuricemia in both men and women9,10. In addition, a longitudinal study of 2,895 middle-aged Chinese people showed an association between large waist circumference (≥ 95 cm in men and ≥ 85 cm in women) and a high incidence of hyperuricemia, although the dose-dependency and sex predisposition of the relationship were not evaluated11. Therefore, there is uncertainty surrounding the longitudinal, dose-dependent, and sex-specific relationships between waist circumference and the incidence of hyperuricemia, particularly in Japanese people.
In the present study, we aimed to clarify the relationships between waist circumference and the subsequent development of hyperuricemia in men and women in the general Japanese population.
Results
The participants were placed into sex-specific groups according to their waist circumference: tertile 1 (≤ 81.0 cm), tertile 2 (81.1–88.0 cm) and tertile 3 (> 88.0 cm) for men; and tertile 1 (≤ 78.0 cm), tertile 2 (78.1–86.5 cm) and tertile 3 (> 86.5 cm) for women.
Tables 1 and 2 present the baseline characteristics of the participants, according to tertile of waist circumference, for men (Table 1) and women (Table 2). Both men and women with larger waist circumferences were more likely to have hypertension, diabetes and dyslipidaemia.
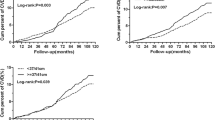
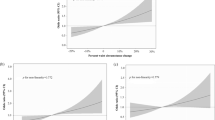
During follow-up (mean 5.4 years), 697 people (551 men and 146 women) developed hyperuricemia. Table 3 shows the risk of hyperuricemia in each group of men and women. The incidence of hyperuricemia (per 1000 person-years) was higher in men with larger waist circumferences: 34.9 for tertile 1, 49.9 for tertile 2 and 63.3 for tertile 3 (Ptrend < 0.001). This relationship was also significant after adjustment for age, hypertension, diabetes, dyslipidaemia, CKD, current smoking, current alcohol consumption and exercise status: the multivariable-adjusted hazard ratios were 1.25 (95% confidence interval [95% CI] 0.99–1.57) for tertile 2 and 1.49 (95% CI 1.18–1.89) for tertile 3, compared with tertile 1 (Ptrend < 0.001). Among men, mediation analysis revealed significant pure indirect effects of hypertension (P = 0.007) but similar results were obtained from sensitivity analysis excluding hypertension from covariates: the multivariable-adjusted hazard ratios were 1.31 (95% CI 1.04–1.65) for tertile 2 and 1.62 (95% CI 1.29–2.04) for tertile 3, compared with tertile 1 (Ptrend < 0.001). There were no significant mediation effects of other confounding factors. Similar results were also obtained for women, the incidences (per 1,000 person-years) were 5.5 for tertile 1, 6.3 for tertile 2 and 11.9 for tertile 3 (Ptrend < 0.001); and the adjusted hazard ratios were 0.93 (95% CI 0.56–1.54) for tertile 2 and 1.67 (95% CI 1.05–2.66) for tertile 3, compared with tertile 1 (Ptrend = 0.014). Among women, there were no significant mediation effects of confounding factors. There were no clear differences in the multivariable-adjusted associations between the tertile groups of waist circumference and the incidence of hyperuricemia in men and women (P = 0.136 for the interaction).
Tables 4 and 5 show the multivariable-adjusted hazard ratios associated with waist circumference for the incidence of hyperuricemia in subgroups of men (Table 4) and women (Table 5). Closer associations between waist circumference and the incidence of hyperuricemia were obtained for men aged ≥ 65 years (hazard ratio 2.19, 95% CI 1.46–3.29 for tertile 3 vs. tertile 1) than for men aged < 65 years (hazard ratio 1.26, 95% CI 0.93–1.69, P = 0.015 for the interaction). There were no other significant differences in the relationships of waist circumference with hyperuricemia in subgroups defined by hypertension, diabetes, dyslipidaemia, CKD, smoking habits, alcohol consumption or exercise status for the men or the women (interactions all P > 0.1).
Discussion
In the present observational study of the general Japanese population, waist circumference was shown to be associated with subsequent hyperuricemia in both men and women. These associations remained significant after adjustment for the effects of the potential confounders age, hypertension, diabetes, dyslipidaemia, CKD, smoking, daily alcohol consumption and exercise status. There were no clear differences in the relationships of waist circumference with hyperuricemia in the subgroups, although there was a closer association for men aged ≥ 65 years.
In most previous studies, the relationship between obesity and hyperuricemia was investigated using BMI12,13,14,15. A cross-sectional study of 5591 Korean adults showed significant associations between waist circumference and hyperuricemia in both men and women9. A cross-sectional study of 33,498 Japanese people also showed significant increments in the prevalence of hyperuricemia with increases in waist circumference in both men and women10. There have been few longitudinal studies, but a cohort study of 2895 middle-aged Chinese adults showed that the odds ratio of hyperuricemia for the highest quartile of waist circumference was 2.2 times higher than that for the lowest quartile11. To the best of our knowledge, the present study is the first longitudinal study of the general Japanese population to confirm the findings of previous studies, and has revealed clear associations between waist circumference and the incidence of hyperuricemia in both men and women in Japan.
In the subgroup analysis performed in the present study, a closer association was identified between waist circumference and the incidence of hyperuricemia in men aged ≥ 65 years than in those aged < 65 years (P = 0.015 for the interaction). Although this might have been a chance finding, the interaction might be attributable to the higher risk of hyperuricemia that is present in older individuals16,17. Further investigation of the role of the interaction between age and abdominal obesity with respect to the development of hyperuricemia is required.
The pathophysiological mechanisms underlying the association between obesity and the development of hyperuricemia are complex and not fully understood. One possible mechanism is that insulin resistance and the subsequent hyperinsulinemia, which are closely associated with central obesity, have effects on the proximal tubules, increasing the reabsorption of sodium-bound uric acid18,19,20. Another is that the expansion of adipose tissue depots and the development of central obesity result in hyperuricemia through excessive uric acid production21, because adipose tissue expresses xanthine oxidoreductase (XOR), and therefore generates uric acid22,23. The association between waist circumference and hyperuricemia might also be mediated by lifestyle-related diseases, such as high blood pressure, impaired glucose tolerance and dyslipidaemia10.
Although the present study was a large-scale longitudinal study of the general Japanese population, it had several limitations. First, because it was a retrospective study, the results of the analysis may have been affected by selection bias. Second, we recruited people who attended health examinations, and therefore they were probably more likely to be aware of healthy lifestyle habits than those who did not attend such examinations. Third, the exact date of onset of hyperuricemia could not be determined, because it was diagnosed at annual physical examinations. Fourth, information regarding the use of urate-lowering medications was not available. Finally, the findings were based on a single measurement of waist circumference, which may not have accurately reflected the status of the participant. However, a random misclassification of this nature would tend to underestimate the magnitude of trends, and therefore the actual association might be closer than that identified in the present study.
Methods
Research design and participants
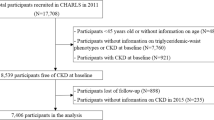
The ISSA-CKD (Iki City Epidemiological Study of Atherosclerosis and Chronic Kidney Disease) study is a retrospective study of the residents of Iki City, Japan. The details of this study have been provided previously24,25,26,27,28. Iki City has approximately 26,000 residents and is on an island in the northern part of Nagasaki Prefecture. A total of 8024 residents (≥ 30 years old) who underwent an annual health examination in Iki City at least once between 2008 and 2019 were eligible for inclusion in the present study. After excluding 1,902 people for whom less than a year of follow-up data were available, 544 who had hyperuricemia at baseline, and 11 with missing waist circumference data, 5567 residents (2331 men and 3236 women) remained for inclusion in the analysis. An opt-out approach was used to obtain the informed consent of the participants and the study was approved by the Fukuoka University Medical Ethics Review Board (No.2017M010). The study was conducted in accordance with the principles of the Declaration of Helsinki and the Ethical Principles for Medical Research and Ethical Guidelines for Medical and Biological Research Involving Human Subjects of the Japanese government.
Data collection
At each health check, each participant’s waist circumference was measured in the standing position during standard expiration, at the umbilical level, as per the guidelines of Japan’s Ministry of Health, Labour and Welfare, by trained medical staff. The participants were placed into sex-specific groups according to tertile of waist circumference, because of the heterogeneous distribution of waist circumference in men and women.
BMI (kg/m2) was calculated as body mass (kg)/height (m)2, and a BMI ≥ 25 kg/m2 was regarded as indicating obesity29. After at least 5 min of rest in the sitting position, each participant’s blood pressure (BP) was measured twice using mercury, anaeroid or automated sphygmomanometers with appropriate-sized cuffs placed on their right upper arm. The mean of two BP values was used in the present analysis. A BP of ≥ 140/90 mmHg or the use of BP-lowering medication was regarded as indicating hypertension.
A standard questionnaire was used to obtain information regarding the participants’ smoking habits, alcohol consumption, and exercise status at baseline. Participants were classified as current smokers (regular smokers for ≥ 6 months) or not. Alcohol consumption was classified into whether or not the participant reported current daily drinking. Exercise status was classified as regular exercise (≥ 30 min per day at least twice weekly) or no regular exercise.
Fasting or non-fasting samples of blood and urine were obtained from each participant. The serum uric acid concentration was measured using an enzymatic method. High-performance liquid chromatography was used to measure glycated haemoglobin (HbA1c) levels (National Glycohemoglobin Standardization Program value). An enzymatic method was used to measure plasma glucose concentration. HbA1c ≥ 6.5%, fasting blood glucose ≥ 7.0 mmol/L, non-fasting blood glucose ≥ 11.1 mmol/L or the use of glucose-lowering therapies was regarded as indicating the presence of diabetes. The serum triglyceride, high-density lipoprotein (HDL)-cholesterol and low-density lipoprotein (LDL)-cholesterol concentrations were measured using enzymatic methods. An LDL cholesterol ≥ 3.62 mmol/l, HDL cholesterol < 1.03 mmol/l, triglycerides ≥ 1.69 mmol/l or the use of lipid-lowering medication was regarded as indicating dyslipidaemia. An enzymatic method was used to measure the serum creatinine concentration. The estimated glomerular filtration rate (eGFR) was calculated as follows: eGFR (mL/min/1.73 m2) = 194 × serum creatinine (mg/dL)−1.094 × age−0.287 (× 0.739 if female)30. Urinary protein concentration was assessed using a dipstick, and proteinuria was defined as a score of (1 +) or higher. eGFR < 60 mL/min/1.73 m2 and/or proteinuria was regarded as indicating the presence of CKD.
Definition of the outcome
The outcome was the incidence of hyperuricemia (uric acid concentration > 7.0 mg/dL [416 µmol/L])1 during follow-up.
Statistical analysis
SAS version 9.4 (Cary, NC, USA) was used for all the statistical analyses. Tertile groups of waist circumference were defined separately for men and women using the “Rank” procedure of SAS. Continuous data are presented as the mean ± SD, and trends across the tertile groups were evaluated using a simple regression model. Categorical data are presented as frequencies and percentages, and trends across the tertile groups were evaluated using a logistic regression model. The person-year approach was used to estimate incidences of hyperuricemia in the sample as a whole and in the tertile groups. The relationship between waist circumference and the incidence of hyperuricemia was evaluated using Cox proportional hazards models. Mediation analysis was performed according to a method described by Discacciati et al.31.
The effects of waist circumference on the incidence of hyperuricemia were compared between subgroups defined according to age; the presence or absence of hypertension, diabetes, dyslipidaemia, and CKD; smoking habits; alcohol consumption habits; and exercise habits by adding interaction terms to the statistical models. All the tests were two-tailed. P < 0.05 was considered to represent statistical significance.
Conclusion
In the present longitudinal study of the general Japanese population, people with higher waist circumference were found to be at a higher risk of subsequent hyperuricemia, whether men or women. These results suggest that lifestyle interventions for individuals with abdominal obesity could prevent the development of hyperuricemia.
Data availability
The datasets generated and analysed within the current study are not publicly available as they are the property of Iki City, Nagasaki, Japan. Their publication would be in violation of the Act on the Protection of Personal Information of the Japanese government but are available from the corresponding author on reasonable request.
References
Hisatome, I. et al. Japanese Society of Gout and Uric and Nucleic Acids 2019 guidelines for management of hyperuricemia and gout 3rd edition. Gout. Uric. Nucl. Acids. 44, 111–140 (2020).
Dehlin, M., Jacobsson, L. & Roddy, E. Global epidemiology of gout: Prevalence, incidence, treatment patterns and risk factors. Nat. Rev. Rheumatol. 16, 380–390 (2020).
Vague, J. The degree of masculine differentiation of obesities: A factor determining predisposition to diabetes, atherosclerosis, gout, and uric calculous disease. Am. J. Clin. Nutr. 4, 20–34 (1956).
Song, X. et al. Comparison of various surrogate obesity indicators as predictors of cardiovascular mortality in four European populations. Eur. J. Clin. Nutr. 67, 1298–1302 (2013).
Cerhan, J. R. et al. A pooled analysis of waist circumference and mortality in 650,000 adults. Mayo. Clin. Proc. 89, 335–345 (2014).
Miyawaki, T. et al. Contribution of visceral fat accumulation to the risk factors for atherosclerosis in non-obese Japanese. Intern. Med. 43, 1138–1144 (2004).
Neeland, I. J. et al. Visceral and ectopic fat, atherosclerosis, and cardiometabolic disease: A position statement. Lancet Diabetes Endocrinol. 7, 715–725 (2019).
Zeng, Q. et al. CT-derived abdominal adiposity: Distributions and better predictive ability than BMI in a nationwide study of 59,429 adults in China. Metabolism 115, 154456 (2021).
Kim, I. Y. et al. Women with metabolic syndrome and general obesity are at a higher risk for significant hyperuricemia compared to men. J. Clin. Med. 8, 837 (2019).
Miyagami, T. et al. The waist circumference-adjusted associations between hyperuricemia and other lifestyle-related diseases. Diabetol. Metab. Syndr. 9, 11 (2017).
Zhou, Z., Li, K., Li, X., Luan, R. & Zhou, R. Independent and joint associations of body mass index, waist circumference, waist-height ratio and their changes with risks of hyperuricemia in middle-aged and older Chinese individuals: a population-based nationwide cohort study. Nutr. Metab. 18, 62 (2021).
Ashley, F. W. Jr. & Kannel, W. B. Relation of weight change to changes in atherogenic traits: The Framingham Study. J. Chronic. Dis. 27, 103–114 (1974).
Kuwabara, M. et al. Different risk for hypertension, diabetes, dyslipidemia, and hyperuricemia according to level of body mass index in Japanese and American subjects. Nutrients 10, 1011 (2018).
Choi, H. K. et al. Population impact attributable to modifiable risk factors for hyperuricemia. Arthritis. Rheumatol. 72, 157–165 (2020).
Nakanishi, N., Tatara, K., Nakamura, K. & Suzuki, K. Risk factors for the incidence of hyperuricaemia: A 6-year longitudinal study of middle-aged Japanese men. Int. J. Epidemiol. 28, 888–893 (1999).
Zhu, Y., Pandya, B. J. & Choi, H. K. Prevalence of gout and hyperuricemia in the US general population: The National Health and Nutrition Examination Survey 2007–2008. Arthritis Rheum. 63, 3136–3141 (2011).
Song, P. et al. Prevalence and correlates of hyperuricemia in middle-aged and older adults in China. Sci. Rep. 8, 4314 (2018).
Cappuccio, F. P., Strazzullo, P., Farinaro, E. & Trevisan, M. Uric acid metabolism and tubular sodium handling: Results from a population-based study. JAMA. 270, 354–359 (1993).
Quiñones Galvan, A. et al. Effect of insulin on uric acid excretion in humans. Am. J. Physiol. 268, E1–E5 (1995).
Maaten, J. T. et al. Renal handling of urate and sodium during acute physiological hyperinsulinaemia in healthy subjects. Clin. Sci. 92, 51–58 (1997).
Matsuura, F. et al. Effect of visceral fat accumulation on uric acid metabolism in male obese subjects: Visceral fat obesity is linked more closely to overproduction of uric acid than subcutaneous fat obesity. Metabolism 47, 929–933 (1998).
Tsushima, Y. et al. Uric acid secretion from adipose tissue and its increase in obesity. J. Biol. Chem. 288, 27138–27149 (2013).
Nagao, H. et al. Hypoxanthine secretion from human adipose tissue and its increase in hypoxia. Obesity 26, 1168–1178 (2018).
Maeda, T. et al. Usefulness of the blood pressure classification in the new 2017 ACC/AHA hypertension guidelines for the prediction of new-onset chronic kidney disease. J. Hum. Hypertens. 33, 873–878 (2019).
Kawazoe, M. et al. Effect of chronic kidney disease on the association between hyperuricemia and new-onset hypertension in the general Japanese population: ISSA-CKD study. J. Clin. Hypertens. 23, 2071–2077 (2021).
Abe, M. et al. Comparison of body mass index and waist circumference in the prediction of diabetes: A retrospective longitudinal study. Diabetes Ther. 12, 2663–2676 (2021).
Funakoshi, S. et al. Eating before bed and new-onset hypertension in a Japanese population: The Iki city epidemiological study of atherosclerosis and chronic kidney disease. Hypertens. Res. 44, 1662–1667 (2021).
Tada, K. et al. Association between serum uric acid and new onset and progression of chronic kidney disease in a Japanese general population: Iki epidemiological study of atherosclerosis and chronic kidney disease. Clin. Exp. Nephrol. 25, 751–759 (2021).
Yuji, M. The examination committee of criteria for ‘obesity disease’ in Japan, Japan society for the study of obesity. Circ. J. 66, 987–992 (2002).
Matsuo, S. et al. Revised equations for estimated GFR from serum creatinine in Japan. Am. J. Kidney. Dis. 53, 982–992 (2009).
Discacciati, A., Bellavia, A., Lee, J. J., Mazumdar, M. & Valeri, L. Med4way: A Stata command to investigate mediating and interactive mechanisms using the four-way effect decomposition. Int. J. Epidemiol. 48, 15–20 (2019).
Acknowledgements
We sincerely appreciate residents and the local government of the Iki City, Nagasaki, Japan.
We thank Mark Cleasby, PhD from Edanz (https://jp.edanz.com/ac) for editing a draft of this manuscript.
Author information
Authors and Affiliations
Contributions
Conceptualization, H.A. and K.K.; data curation, H.A.; formal analysis, T.M. and H.A.; investigation, T.U., C.N., Kaori M., Kazuyo I., A.M., S.F., M.A., A.S., M.K., C.Y., Koji T., Kazuhiro T., Kenji I., T.Y., S.M., D.K., Kosuke M. and K.K.; methodology, H.A.; project administration, H.A.; software, H.A.; supervision, H.A.; Writing–original draft., K.K. and H.A.; Writing–review and editing, Kosuke M., D.K., S.M., T.Y., Koji T., Kazuhiro T., Kenji I., M.A., A.S., M.K., C.Y. and K.K. All authors were informed about each step of manuscript processing including the submission, revision, revision reminder, etc.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kawano, K., Ueno, T., Maeda, T. et al. Relationship between abdominal circumference and the incidence of hyperuricemia in the general Japanese population. Sci Rep 14, 4573 (2024). https://doi.org/10.1038/s41598-024-55008-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-55008-6
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
