
Abstract
The process of creating virtual models of dentomaxillofacial structures through three-dimensional segmentation is a crucial component of most digital dental workflows. This process is typically performed using manual or semi-automated approaches, which can be time-consuming and subject to observer bias. The aim of this study was to train and assess the performance of a convolutional neural network (CNN)-based online cloud platform for automated segmentation of maxillary impacted canine on CBCT image. A total of 100 CBCT images with maxillary canine impactions were randomly allocated into two groups: a training set (n = 50) and a testing set (n = 50). The training set was used to train the CNN model and the testing set was employed to evaluate the model performance. Both tasks were performed on an online cloud-based platform, ‘Virtual patient creator’ (Relu, Leuven, Belgium). The performance was assessed using voxel- and surface-based comparison between automated and semi-automated ground truth segmentations. In addition, the time required for segmentation was also calculated. The automated tool showed high performance for segmenting impacted canines with a dice similarity coefficient of 0.99 ± 0.02. Moreover, it was 24 times faster than semi-automated approach. The proposed CNN model achieved fast, consistent, and precise segmentation of maxillary impacted canines.
Similar content being viewed by others


Introduction
The maxillary canine is the second most frequently impacted tooth, characterized by the failure of a canine to emerge through the gingiva and assume its correct position following the anticipated eruption time. This is due to the fact that it is often the last tooth to erupt and has a long pathway from its developmental position deep within the maxilla to its final location in the oral cavity1. Maxillary canine impaction occurs in approximately 2% of the population (range from 1.7 to 4.7%), with a higher prevalence in females than males2. Several etiological factors might contribute to its impaction, including genetic factors, lack of space, tooth root developmental abnormalities, trauma or injury and presence of oral pathological lesions3,4.
The proper positioning of maxillary canine in the dental arch is critical for functional occlusion5 and aesthetics1,6. A delayed diagnosis or lack of treatment can result in complications such as midline shift, tooth displacement, arch length defect, ankylosis, follicular cyst development, internal tooth resorption, pain, caries, and recurrent infection7. Hence, early detection and intervention are crucial. The diagnosis of canine impaction and determination of the appropriate treatment plan necessitates the utilization of radiographic imaging in conjunction with patient history and clinical examination. In this context, cone beam computed tomography (CBCT) is the most optimal radiographic imaging tool due to its ability to accurately determine the tooth’s three-dimensional (3D) position and assess its relationship with the neighboring teeth and other neighboring anatomical structures. This enables clinicians to accurately assess potential treatment options and plan the most effective course of action8,9,10,11.
Recently, the field of oral healthcare has witnessed a shift towards the utilization of digital workflows for diagnostic and treatment planning purposes. These workflows have addressed the shortcomings of conventional methods by offering enhanced precision, time-efficiency, and improved patient care12,13. The implementation of such workflows has facilitated patient-specific virtual planning, orthodontic treatment simulation, treatment progress monitoring, and 3D printing of orthodontic appliances14,15,16. This could prove particularly advantageous for complex treatment procedures such as those involving impacted canines.
In digital dental workflows involving impacted canines, CBCT image segmentation is a crucial initial step for creating an accurate 3D model of the tooth for either diagnosis, planning or outcome assessment. Any error at this stage can adversely affect the final result17. Both manual and semi-automated segmentation (SS) have been applied as clinical standards for creating virtual impacted canine models, where manual segmentation is time-consuming and operator dependent18,19. Meanwhile, SS relies on threshold selection and often requires manual adjustments, which also makes it prone to human error20,21. Recent application of deep convolutional neural networks (CNNs) has demonstrated improved performance over conventional segmentation methods for modeling of the dentomaxillofacial region, with promising results for automated segmentation (AS) of teeth, upper airway, inferior alveolar nerve canal, mandible, and maxillary sinus on CBCT images22,23,24,25,26,27,28,29,30. However, there is a lack of evidence regarding the application of CNNs for the AS of impacted canines.
Therefore, the aim of the present study was to train and assess the performance of a CNN-based tool for AS of maxillary impacted canine on CBCT images.
Material and methods
This retrospective study was conducted in compliance with the World Medical Association Declaration of Helsinki on medical research. Ethical approval was obtained from the Ethical Review Board of the University Hospitals Leuven (reference number: B322201525552).
Dataset
A total of 200 CBCT scans (46 males and 54 females; age range: 8–54 years) having uni- or bilateral maxillary impacted canine cases were collected during the period 2015–2022, from the radiological database of UZ Leuven Hospital, Leuven, Belgium. Inclusion criteria consisted of previously clinically and radiologically diagnosed unilateral/bilateral, horizontal/oblique/vertical and complete/partial maxillary canine impactions. Teeth with both complete and partially formed roots were included. The majority of cases in these datasets had orthodontic brackets. Exclusion criteria involved scans with motion artifacts and poor image quality, where margins of canine could not be optimally delineated. The CBCT images were obtained utilizing two devices, NewTom VGi Evo (Cefla, Imola, Italy) and 3D Accuitomo 170 (J Morita, Kyoto, Japan) with variable scanning parameters of 90–110 kV, a voxel size between 0.125 and 0.300 mm3 and a field of view between 8 × 8 and 24 × 19 cm.
All images were exported in Digital Imaging and Communications in Medicine (DICOM) format. Thereafter, the DICOM datasets were uploaded to a CNN-based online cloud platform known as the ‘Virtual patient creator’ (Relu, Leuven, Belgium), to assess if the tool would be able to segment impacted canines, as it had been previously trained for permanent erupted teeth segmentation24,28. Based on the visual assessment by two observers (A.S, B.E), 100 images from the total dataset of 200 images could not be segmented automatically by the platform. Hence, these failed cases were randomly divided into two subsets, training set (n = 50), to train and better fit the CNN model for impacted canines using semi-automatically segmented ground truth data; and testing set (n = 50), to test the model performance for AS compared to the ground truth data. Figure 1 illustrates the data distribution for training and testing subsets.
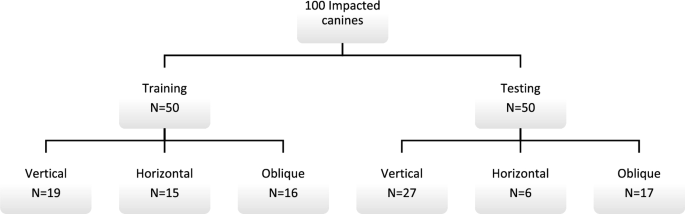
Dataset used for training and validation.
Data labelling
The ground truth for the training and testing sets was obtained through SS of impacted canines on the online platform using cloud tools such as the contour tool and smart brush function26. The contour tool interpolates the interslice region between selected contours, while the smart brush function groups voxels based on their intensities. The operator adjusted the segmentation until satisfied with the result, and all contours were verified in axial, coronal, and sagittal planes. The segmentation was performed by one observer (A.S) and subsequently reassessed by two additional observers (NM & RJ) with 10 and 25 years of experience, respectively. The canines were then exported as standard tessellation language (STL) files for further processing in the CNN pipeline.
AI architecture
The training of the CNN model involved the utilization of two 3D U-Net architectures (Fig. 2), each comprising four encoding and three decoding blocks. The architecture included two convolutional layers with a kernel size of 3 × 3 × 3, ReLU activation function, and group normalization with eight feature maps. Max pooling with a kernel size of 2 × 2 × 2 and strides of two was applied to reduce the resolution by a factor of two across all dimensions25,27.
Binary classifier training (0 or 1) was performed on both networks. All scans were resampled to a uniform voxel size. To circumvent GPU memory limitations, the entire scan was down-sampled to a fixed size. A low-resolution segmentation was achieved using the first 3D U-Net to propose 3D patches. The segments corresponding to the impacted canines were only extracted. A second 3D U-Net was employed to segment and fuse the relevant patches, which were subsequently used to construct a full-resolution segmentation map. The binary image was binarized, retaining only the largest connected component, and a marching cubes algorithm was applied. The resulting mesh was smoothed to generate a 3D model. The optimization of the model parameters was performed using a deep learning model optimization technique known as ADAM31, with an initial learning rate set to 1.25e4. During the training process, random spatial augmentations such as rotation, scaling, and elastic deformation were applied.

3D U-net architecture32.
Model testing and consistency of refined segmentations
The performance of the CNN model was evaluated using a testing set and compared to the ground truth obtained through SS performed by observer B.E. The images were uploaded to the online tool and the resulting AS was downloaded in STL file format. Moreover, a visual evaluation of the segmented testing set was performed by two observers (A.S, B.E) to determine if any refinements were necessary (Fig. 3). If required, these refinements were implemented using the brush function on the online tool to add or remove voxels from the selection. The refined segmentation was also downloaded in STL file format. The intra- and inter-observer repeatability of refined segmentations was confirmed by both observers performing the refinements twice at a two-week interval.

Automated segmentation of maxillary impacted canine and other dentomaxillofacial structures (maxillary bone, maxillary sinus and erupted teeth) on virtual patient creator platform (creator.relu.eu, Relu BV, Version October 2022).
CNN performance evaluation
The CNN model’s performance was evaluated based on time duration and voxel- and surface-based metrics.
Time analysis
The duration of testing set segmentation with the SS approach was recorded using a digital stopwatch, starting from the import of CBCT data until the generation of the canine model. On the other hand, the online platform automatically provided the time needed to obtain the final segmentation map.
Performance metrics
The performance of the CNN model was assessed by utilizing confusion matrix for voxel-wise comparison of SS ground truth and AS maps according to the following metrics: Dice similarity coefficient (DSC), Intersection over union (IoU) and 95% Hausdorff Distance (HD). In addition, the surface-based analysis involved importing superimposed STL files of SS and AS to 3-matic software (Materialise NV, Leuven, Belgium), followed by automated part comparison analysis to calculate the root mean square (RMS) difference between both segmented models.
Statistical analysis
Data were analyzed using GraphPad Prism, Version 9.0. (GraphPad Software, La Jolla, CA). A paired sample t-test was used to compare the time between SS and AS. The performance metrics were represented by mean and standard deviation values. An IoU score of < 0.5 or HD value of > 0.2 mm would indicate towards poor performance. Inter-class correlation coefficient (r) was applied to assess intra- and inter-observer consistency of the refined segmentations. A p value of less than 0.05 was considered significant.
Informed consent
Since data were evaluated retrospectively, pseudonymously and were solely obtained for treatment purposes, a requirement of informed consent was waived by the Ethical Review Board of the University Hospitals Leuven (reference number: B322201525552).
Results
Upon visual inspection of the testing dataset, it was determined that 20% (n = 10) of the cases required minor refinements. The mean values for intra-observer consistency of refinements were 92% for IOU and 96% for DSC. Inter-observer consistency yielded IOU and DSC values of 87% and 93%, respectively (Table 1). Intra-observer repeatability was determined to be 0.992, while inter-observer repeatability was 0.986.
The CNN model required an average of 21 s to perform the AS of impacted canines, while the SS took 582 s. This indicates that the CNN model was approximately 24 times faster than the SS method, with a statistically significant difference of (p < 0.0001) (Fig. 4).

Time comparison between automated and semi-automated segmentation.
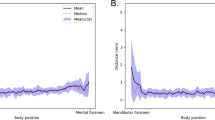
The performance metrics of AS demonstrated high values of IoU (0.99 ± 0.04) and DSC (0.99 ± 0.02) when compared to SS. A mean HD value of 0.01 ± 0.03 mm was detected with RMS difference of 0.05 ± 0.25 mm between SS and AS (Table 2 and Fig. 5), hence indicating towards almost a perfect overlap between semi- and fully-automated segmented canine surfaces.

Comparison of automated and semi-automated maxillary impacted canine segmentation. (A) three-dimensional surface model. (B) axial view. (C) sagittal view. Green color corresponds to no difference between automated and semi-automated segmentation surfaces, red color corresponds to overestimation of automated segmentation and blue color corresponds to underestimation of automated segmentation.
Discussion
A precise 3D segmentation of impacted canine is essential mainly for digital orthodontic treatment planning workflows33,34,35. Despite being a challenging and time-consuming task through manual and semi-automated approaches, CNN-based automation has the ability to produce highly accurate 3D virtual models in a time-efficient manner22,24,28. Hence, the goal of this study was to introduce and assess the performance of a CNN model for the segmentation of maxillary impacted canines. In this study, we utilized a pre-existing cloud-based platform that had been previously trained to segment multiple dentomaxillofacial structures (permanent teeth, maxillary sinus, inferior alveolar nerve, and jaw bones) and apply automated CBCT-intraoral scan registration. The performance of the model was comparable to that of SS performed by clinical experts. It is noteworthy that the model showed 100% consistency without the issue of human variability, where it was able to produce identical results when segmenting the same case multiple times. Moreover, only minor refinements were required which confirmed high similarity between AS and SS.
The presented CNN model was able to automatically segment impacted canines in 21 s, which was 24 times faster than the SS approach. Hence, demonstrating the benefits of incorporating automation into the digital workflow to increase clinical efficiency. A comparison with existing studies regarding time-efficiency was challenging due to a lack of reported time data. Time is a crucial factor in clinical dentistry and is integral to an optimal digital workflow, hence it should be reported in such studies incorporating artificial intelligence (AI) based solutions.
Limited research has been conducted on the application of deep learning-based CNNs for either classification or segmentation of impacted teeth. Specifically, no studies have focused on impacted canine segmentation on CBCT images. Hence, comparison with existing evidence was deemed difficult. Kuwada et al.36 evaluated the performance of three CNN systems (DetectNet, VGG-16, AlexNet) for detecting and classifying maxillary impacted supernumerary teeth on panoramic images. They found that DetectNet had the highest detection performance with a recall and precision of 1. Celik et al.37 proposed a deep learning-based tool for detecting impacted mandibular third molars. They compared a two-stage technique (Faster RCNN with ResNet50, AlexNet, and VGG16 as backbones) with a one-stage technique (YOLOv3) and found that YOLOv3 had the highest detection efficacy with an average precision of 0.96. Imak et al.38 used ResMIBCU-Net to segment impacted teeth (including impacted canines) on panoramic images and achieved an accuracy of 99.82%. Orhan et al.39 evaluated the diagnostic performance of a U-Net CNN model for detecting impacted third molar teeth on CBCT images and showed an accuracy of 86.2%. Meanwhile, the findings of the present suggested a high scoring of 0.99 based on both DSC and IoU. It is noteworthy that the use of accuracy as an evaluation metric for 3D AS tasks can result in misleading conclusions due to the inclusion of true negatives in the calculation. This phenomenon, known as the accuracy paradox, can result in a high accuracy value despite poor model performance40. This is particularly evident in imbalanced datasets where the over-representation of one class can lead to an overestimation of accuracy. Alternative evaluation metrics, such as, DSC, 95% HD and IoU should provide a more optimal representation of model performance.
The study’s main strength was its ability to accurately and rapidly segment impacted canines with various angulations (horizontal, oblique, vertical) on CBCT images. The inclusion of scans from two CBCT devices with different acquisition parameters and metal artifacts from brackets could enhance the tool’s practicality and robustness. Moreover, the segmentation and refinements could be performed on an easily accessible online platform without the need for third-party software, making it more convenient for clinical use.
The study also had certain limitations. Firstly, the training was limited to only maxillary impacted canines without inclusion of any other impactions. Secondly, the online tool only provided the segmentation map as an outcome without any additional tools for dimensional and morphometric measurements. Thirdly, the CNN training was based on two CBCT devices. Further studies are warranted to train the model based on the datasets from multiple CBCT devices with different scanning parameters and qualities, as well as images acquired from different institutions, for justifying its applicability for regular clinical tasks.
Conclusion
The proposed CNN model facilitated a rapid, consistent, and precise segmentation of maxillary impacted canines on CBCT images, which might aid in diagnosis and the planning of orthodontic and oral surgical interventions. The integration of impacted canine segmentation into the online tool could be considered as a significant leap towards achieving a fully AI assisted virtual workflow for planning, surgical guide designing, and follow-up assessment for various dentomaxillofacial procedures.
Data availability
The data analyzed during the current study available from the corresponding author on reasonable request.
References
Cruz, R. M. Orthodontic traction of impacted canines: Concepts and clinical application. Dental Press J. Orthod. 24, 74–87. https://doi.org/10.1590/2177-6709.24.1.074-087.bbo (2019).
Lövgren, M. L., Dahl, O., Uribe, P., Ransjö, M. & Westerlund, A. Prevalence of impacted maxillary canines: An epidemiological study in a region with systematically implemented interceptive treatment. Eur. J. Orthod. 41, 454–459. https://doi.org/10.1093/ejo/cjz056 (2019).
Alberto, P. L. Surgical exposure of impacted teeth. Oral Maxillofac. Surg. Clin. N. Am. 32, 561–570. https://doi.org/10.1016/j.coms.2020.07.008 (2020).
Anic-Milosevic, S., Varga, S., Mestrovic, S., Lapter-Varga, M. & Slaj, M. Dental and occlusal features in patients with palatally displaced maxillary canines. Eur. J. Orthod. 31, 367–373. https://doi.org/10.1093/ejo/cjp014 (2009).
Mageet, A. O. Classification of skeletal and dental malocclusion: Revisited. Stomatol. Edu J. 3, 205–211. https://doi.org/10.25241/stomaeduj.2016.3(3-4).art.11 (2016).
Schwefer, N., Freitag-Wolf, S., Meyer, G. & Kern, M. Investigation of the esthetic perception of different canine parameters. Clin. Oral Investig. 26, 6973–6983. https://doi.org/10.1007/s00784-022-04651-2 (2022).
Grisar, K. et al. Interventions for impacted maxillary canines: A systematic review of the relationship between initial canine position and treatment outcome. Orthod. Craniofac. Res. 24, 180–193. https://doi.org/10.1111/ocr.12423 (2021).
Arriola-Guillen, L. E., Aliaga-Del Castillo, A., Ruiz-Mora, G. A., Rodriguez-Cardenas, Y. A. & Dias-Da Silveira, H. L. Influence of maxillary canine impaction characteristics and factors associated with orthodontic treatment on the duration of active orthodontic traction. Am. J. Orthod. Dentofac. Orthop. 156, 391–400. https://doi.org/10.1016/j.ajodo.2018.10.018 (2019).
Friedlander-Barenboim, S. et al. Patterns of cone-beam computed tomography (CBCT) utilization by various dental specialties: A 4-year retrospective analysis from a dental and maxillofacial specialty center. Healthcare https://doi.org/10.3390/healthcare9081042 (2021).
Jacobs, R., Salmon, B., Codari, M., Hassan, B. & Bornstein, M. M. Cone beam computed tomography in implant dentistry: Recommendations for clinical use. BMC Oral Health 18, 88. https://doi.org/10.1186/s12903-018-0523-5 (2018).
Oenning, A. C. et al. Cone-beam CT in paediatric dentistry: DIMITRA project position statement. Pediatr. Radiol. 48, 308–316. https://doi.org/10.1007/s00247-017-4012-9 (2018).
Lin, Y.-M. The Digitization of Business in China: Exploring the Transformation from Manufacturing to a Digital Service Hub 199–217 (Springer, 2018).
Shujaat, S., Bornstein, M. M., Price, J. B. & Jacobs, R. Integration of imaging modalities in digital dental workflows: Possibilities, limitations, and potential future developments. Dentomaxillofac. Radiol. 50, 20210268–20210268. https://doi.org/10.1259/dmfr.20210268 (2021).
Brown, M. W. et al. Effectiveness and efficiency of a CAD/CAM orthodontic bracket system. Am. J. Orthod. Dentofac. Orthop. 148, 1067–1074. https://doi.org/10.1016/j.ajodo.2015.07.029 (2015).
Camardella, L. T., Rothier, E. K., Vilella, O. V., Ongkosuwito, E. M. & Breuning, K. H. Virtual setup: Application in orthodontic practice. J. Orofac. Orthop. 77, 409–419. https://doi.org/10.1007/s00056-016-0048-y (2016).
Christensen, L. R. Digital workflows in contemporary orthodontics. APOS Trends Orthod. 7, 12–18 (2017).
Starmans, M. P. A. et al. Handbook of Medical Image Computing and Computer Assisted Intervention 429–456 (Academic Press, 2020).
Heye, T. et al. Reproducibility of dynamic contrast-enhanced MR imaging. Part II. Comparison of Intra- and Interobserver variability with manual region of interest placement versus semiautomatic lesion segmentation and histogram analysis. Radiology 266, 812–821. https://doi.org/10.1148/radiol.12120255 (2013).
Parmar, C. et al. Robust Radiomics feature quantification using semiautomatic volumetric segmentation. PLoS ONE 9, e102107. https://doi.org/10.1371/journal.pone.0102107 (2014).
Liu, Q. et al. Vol. 12966 LNCS 606–614 (2021).
Renard, F., Guedria, S., Palma, N. D. & Vuillerme, N. Variability and reproducibility in deep learning for medical image segmentation. Sci. Rep. 10, 13724–13724. https://doi.org/10.1038/s41598-020-69920-0 (2020).
Fontenele, R. C. et al. Influence of dental fillings and tooth type on the performance of a novel artificial intelligence-driven tool for automatic tooth segmentation on CBCT images: A validation study. J. Dent. 119, 104069. https://doi.org/10.1016/j.jdent.2022.104069 (2022).
Lahoud, P. et al. Development and validation of a novel artificial intelligence driven tool for accurate mandibular canal segmentation on CBCT. J. Dent. 116, 103891–103891. https://doi.org/10.1016/j.jdent.2021.103891 (2022).
Lahoud, P. et al. Artificial intelligence for fast and accurate 3-dimensional tooth segmentation on cone-beam computed tomography. J. Endod. 47, 827–835. https://doi.org/10.1016/j.joen.2020.12.020 (2021).
Morgan, N. et al. Convolutional neural network for automatic maxillary sinus segmentation on cone-beam computed tomographic images. Sci. Rep. 12, 7523. https://doi.org/10.1038/s41598-022-11483-3 (2022).
Nogueira-Reis, F. et al. Three-dimensional maxillary virtual patient creation by convolutional neural network-based segmentation on cone-beam computed tomography images. Clin. Oral Investig. 27, 1133–1141. https://doi.org/10.1007/s00784-022-04708-2 (2023).
Preda, F. et al. Deep convolutional neural network-based automated segmentation of the maxillofacial complex from cone-beam computed tomography: A validation study. J. Dent. 124, 104238. https://doi.org/10.1016/j.jdent.2022.104238 (2022).
Shaheen, E. et al. A novel deep learning system for multi-class tooth segmentation and classification on cone beam computed tomography. A validation study. J. Dent. 115, 103865–103865. https://doi.org/10.1016/j.jdent.2021.103865 (2021).
Shujaat, S. et al. Automatic segmentation of the pharyngeal airway space with convolutional neural network. J. Dent. 111, 103705. https://doi.org/10.1016/j.jdent.2021.103705 (2021).
Verhelst, P.-J. et al. Layered deep learning for automatic mandibular segmentation in cone-beam computed tomography. J. Dent. 114, 103786. https://doi.org/10.1016/j.jdent.2021.103786 (2021).
Kingma, D. P. & Ba, J. Adam: A method for stochastic optimization. CoRR abs/1412.6980 (2015).
Çiçek, Ö., Abdulkadir, A., Lienkamp, S. S., Brox, T. & Ronneberger, O. Medical Image Computing and Computer-Assisted Intervention—MICCAI 2016 424–432 (Springer, 2016).
Li, B. et al. Randomized clinical trial of the accuracy of patient-specific implants versus CAD/CAM splints in orthognathic surgery. Plast. Reconstr. Surg. 148, 1101–1110. https://doi.org/10.1097/PRS.0000000000008427 (2021).
Palomo, J. M., El, H., Stefanovic, N. & Bazina, M. in Craniofacial 3D Imaging, 113–139 (2019).
Plooij, J. M. et al. Digital three-dimensional image fusion processes for planning and evaluating orthodontics and orthognathic surgery: A systematic review. Int. J. Oral Maxillofac. Surg. 40, 341–352. https://doi.org/10.1016/j.ijom.2010.10.013 (2011).
Kuwada, C. et al. Deep learning systems for detecting and classifying the presence of impacted supernumerary teeth in the maxillary incisor region on panoramic radiographs. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 130, 464–469. https://doi.org/10.1016/j.oooo.2020.04.813 (2020).
Celik, M. E. Deep learning based detection tool for impacted mandibular third molar teeth. Diagnostics. https://doi.org/10.3390/diagnostics12040942 (2022).
Imak, A., Çelebi, A., Polat, O., Türkoğlu, M. & Şengür, A. ResMIBCU-Net: An encoder-decoder network with residual blocks, modified inverted residual block, and bi-directional ConvLSTM for impacted tooth segmentation in panoramic X-ray images. Oral. Radiol. https://doi.org/10.1007/s11282-023-00677-8 (2023).
Orhan, K. et al. Evaluation of artificial intelligence for detecting impacted third molars on cone-beam computed tomography scans. J. Stomatol. Oral Maxillofac. Surg. 122, 333–337. https://doi.org/10.1016/j.jormas.2020.12.006 (2021).
Valverde-Albacete, F. J. & Peláez-Moreno, C. 100% classification accuracy considered harmful: The normalized information transfer factor explains the accuracy paradox. PLoS ONE 9, e84217. https://doi.org/10.1371/journal.pone.0084217 (2014).
Funding
Open access funding provided by Karolinska Institute.
Author information
Authors and Affiliations
Contributions
A.S. and R.J. conceptualized and designed the study. E.B. collected and curated the dataset. A.S. and B.E. performed the manual/refined segmentations and clinically evaluated the automated segmentations. S.A. performed the statistical analysis. N.M. and S.S. participated in writing the manuscript. All authors reviewed the manuscript. I.C. and R.J. provided resources and supervised the project.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Swaity, A., Elgarba, B.M., Morgan, N. et al. Deep learning driven segmentation of maxillary impacted canine on cone beam computed tomography images. Sci Rep 14, 369 (2024). https://doi.org/10.1038/s41598-023-49613-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-49613-0
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
