
Abstract
Fibromyalgia (FM) is a multicomponent illness and despite its worldwide prevalence, a complete understanding of its aetiology and pathogenesis remains unclear. The goal of the study is to analyze the level of association between elastic properties of tissue measured by strain elastography (SEL) and pain pressure threshold (PPT) in the characteristic painful points described in patients suffering from FM. This was a cross-sectional, observational study. A sample comprised of 42 subjects with FM was recruited from a private care centre. The occiput, low cervical, trapezius, supraspinatus, paraspinous, lateral pectoral, second rib, lateral epicondyle, medial epicondyle, gluteus, greater trochanter, knee, and anterior tibial PPTs were bilaterally assessed using a standard pressure algometer and elastic properties of tissue were evaluated by SEL. Linear regression analysis showed significant associations between SEL and dominant trapezius PPT (β = 0.487, 95% CI [0.045, 0.930], p = 0.032) after adjustments for the age, body mass index, and menopause status (higher SEL and higher pain sensitivity). No significant associations between SEL and the other PPTs variables were found in women diagnosed with FM. The PPT of the dominant trapezius is associated with SEL measurements in subjects suffering from FM. More studies are required to fully explain the underlying mechanisms.
Similar content being viewed by others
Introduction
Fibromyalgia (FM) is characterized as a widespread and diffuse chronic musculoskeletal pain on the human body, accompanying in addition to other symptoms such as dysesthesia, tingling, tender points (TPs), fatigue, morning stiffness, headache, abdominal pain, sleep disturbances, anxiety, altered moods, and concentration difficulties, among others1,2,3. In the worldwide population, between 0.4 and 9.3% of people suffer from FM with an average prevalence rate of 2.7%4. The estimated prevalence of FM is 2.31% and 2.40% in the European and Spanish population respectively, with a greater probability in women compared with men (ratio 21:1). Likewise, the frequent age range of clinical manifestations is between 30 and 50 years of age4,5.
According to the American College of Rheumatology (ACR), the criteria for diagnosis of FM are: (1) generalised pain for at least 3 months, and (2) TPs on digital palpation, with a force approximately of 4 kg, for at least 11 of the 18 bilateral points6. However, in 2016, the ACR included new conditions for diagnosis of a person with FM such as widespread pain for at least 4 of 5 body regions, pain or symptoms maintained during 3 months, or high scores in the Widespread Pain Index (WPI) or Symptom Severity Scale (SSS) scale, indicating a worsening in the widespread and the intensity of pain2.
The pathophysiology and underlying mechanisms of FM remain uncertain. Scientific literature considers the phenomenon of central sensitization to be the principal key factor in the development of the FM7. However, there are other series of neurogenic, vascular, inflammatory, immunological, nutritional, and genetic factors that could explain this chronic condition syndrome3,8,9. In this sense, studies have highlighted the existence of morphological abnormalities in the diameter and density of blood capillaries, which could influence the sympathetic tone and activity and modifying the microcirculatory blood flow, skin conductance, mechanotransduction, and tensegrity of the tissues10,11. In this regard, new techniques for the quantification of FM and myofascial pain are appearing, such as magnetic resonance imaging (MRI), microanalytic techniques, infrared thermography and ultrasonography. Among them, ultrasonography is gaining popularity and its use is growing in both research and clinical settings12. Specifically, strain elastography (SEL) has the ability to quantify the elasticity of tissue13, thus offering possibilities of assessing stiffness and tissue quality, such as in TPs.
A TP is a specific localized area that can be found on a muscle, muscle–tendon junction, fat pad, or bursa region and is extremely sensitive to pressure or touch. These points are frequently linked to musculoskeletal disorders like FM14,15,16.
On the other hand, Myofascial Trigger Points (MTrPs) are described as hyperirritable tenderness points in taut bands of skeletal muscle or their corresponding fascia that cause local pain, referred pain, and a local twitch response when pressure is applied. Clinically, MTsP can be categorized as “latent” or “active”. When mechanically stimulated by palpation or dry needling, an active MTrP produces local and referred pain that the patient can feel. Latent MTrPs are asymptomatic and do not produce palpable pain14,17.
A TP, as opposed to a trigger point, should be used to describe an area when local pressure applied to a delicate area causes pain without referred pain or reproduction of pain14. It has been established that TP and MTrP can manifest in most muscles of the human body, although some locations, such as the back, face, neck, knee, calf, gluteus maximus, quadriceps, and hips, are most often affected16,17.
The elastic characteristics of soft tissues are indicative of alterations in the mechanical functions of soft tissue that occur with age and disease18. The mechanical failures that occur in tissues are associated with increases in both morbidity and mortality18. Additionally, the elastic properties of soft tissue, as well as cartilaginous tissues, are influenced or even determined by the activity of the sympathetic nervous system19. In patients with FM, a relationship between psychological factors and the elasticity of tissues has been shown20, as well as with sympathetic nervous system dysfunction21, however, little research has been carried out to study elastic properties in tender or MTrp, and the existing results are not yet conclusive. Therefore, there is a need for research to assess such painful points to better understand the relationship between tissue elasticity and pain pressure thresholds (PPT), since SEL can be employed to measure the elastic properties of soft tissue, and a decrease in elasticity indicates the progression of disease and/or the effects of unsuccessful aging21,22,23. We hypothesized that establishing a potential association between the PPT in FM and the elastic properties of soft tissue opens up the possibility of using elastic property measurements to assess treatment effectiveness, particularly when pain and other symptoms, including psychosocial factors, are linked to these properties.
Hence, the aim of the study was to analyse the level of association between SEL and PPT in the characteristic painful points described in patients suffering from FM.
Methods
Design
This was a cross-sectional, observational study. This study received ethical approval by the Ethics Committee of Human Research of the University of Granada, Spain (approval number: 1044/CEIH/2020), and was reported in line with the STROBE statement24 and conducted by the Declaration of Helsinki. All experiments were performed in accordance with relevant guidelines and regulations.
Setting
Participants were recruited in a private care centre and rehabilitation service, from January 30 (2021) to January 30 (2022). Formal meetings and trial information sheets were provided to the participants. Informed consent was obtained from all subjects and/or their legal guardian (s).
Participants
Participants were screened to determine whether they met the following inclusion and exclusion criteria:
Inclusion criteria
(i) Aged between 34 and 64 years; ii) FM diagnosis following the ACR classification2.
Exclusion criteria
(i) Presenting any inflammatory, (ii) orthopedic, (iii) or neurological disease which may affect cognitive, balance, hearing, and vision impairment in terms of the ability to answer questions.
Recruitment procedures
A physiotherapist collaborating in the project was in contact with the participants at the time of recruitment and carrying out the treatment, as well as providing them the information about the study and eligibility criteria. Those who fit in the study and remained interested in the participation signed a consent form.
Outcome measures
Pain pressure threshold (PPT)
PPT were bilaterally assessed over the 12 initial TPs considered by the ACR for FM diagnosis6, together with the anterior tibial, other characteristic painful point presented in central sensitization conditions25, with a standard pressure algometer of 1 cm2 (FPK 20; Wagner Instruments, Greenwich, CT, USA).
The TPs assessed were: (i) at the suboccipital muscle insertions, (ii) at the anterior aspects of the intertransverse spaces at low cervical C5–C7, (iii) at the midpoint of the trapezius (upper border), (iv) at the supraspinatus origins, above the scapula spine near the medial border, (v) paraspinous, at the level of the mid-scapula, 3 cm lateral to the midline, (vi) at the second costochondral junctions (second rib), (vii) at the level of the fourth rib at the anterior axillary line (lateral pectoral), (viii) 2 cm distal to the epicondyles, (ix) medial epicondyle, (x) at the distal dorsal third of the forearm, (xi) at the upper outer quadrants of buttocks in the anterior fold of gluteal muscle, (xii) greater trochanter just posterior to the trochanteric prominence and (xiii) at the medial knee fat pad, proximal, to the joint line. We have followed the measurement protocol previously described in literature26. We positioned the algometer perpendicular to the TP, to assess PPT, the pain threshold was set as the minimum pressure that caused pain. Positive evidence of a TP was considered to exist when participants reported “pain” at or below a pressure of 4 kg. The mean of three measurements at each TP was used for the analysis. The total count of positive TPs was recorded for each participant6,26,27. Pressure algometry is considered a valid and reliable method for the evaluation of pain sensitivity28.
SEL measurements
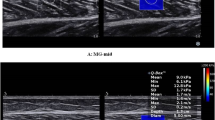
The Logiq S7 using a 15 MHz linear probe (GE Healthcare, Milwaukee, WI) was used to carry out all the measurements by an expert physiotherapist with eleven years of experience in ultrasound imaging. All participants were positioned in the same orientation used for the MTrPs) identification protocol29. All images were obtained with the transducer placed longitudinally with the muscle fibers and positioning the center of the probe over the TP of interest and the control point locations, following recommendations from reliability studies30. Then, the tissue was compressed, a software incorporated quality control evaluated the recommended compression size, being approximately 2–5 mm. The exact raw strain value (0–6; with 0 being softest and 6 being the hardest tissue) was calculated using A 5 mm circular region of the area of interest was used to calculate the exact raw strain value, as indicated by the manufacturer’s instructions and following previous studies26,27. In order to minimize intra-observer variation, a mean of the three measured areas at each was calculated. Following manufacture’s recommendations, only sequences with the highest image quality were used (Fig. 1).

Quantitative strain elastography (SEL) assessment in the upper trapezius muscle in a woman with Fibromyalgia. Different circles represent assessments of different regions of interest (ROI) from superficial to deep tissues.
Sample size
Sample size was determined using G * Power 3.1.9.7 software (Heinrich-Heine-Universität Düsseldorf, Düsseldorf, Germany). Based on results of PPT through sonoelastograhpy in patients with nonspecific lumbopelvic pain of a previous cross-sectional study31, it is necessary to include a minimum of 18 subjects with FM to obtain a power of 80% and an alpha level (α) of 0.05. The sample size was increased to 48 participants after taking into account an expected loss rate of approximately 62.5%. The final sample of the study was 42 women with FM.
Statistical analysis
The statistical analysis was conducted by SPSS Statistics Version© 24 software for Windows (IBM Corporation, Armonk, NY, USA). The data for continuous and categorical variables were expressed as mean ± standard deviation (SD) and frequency (%), respectively. The normality and distribution of the variables was performed using the Kolmogorov–Smirnov test (α-value = 0.05). To test homoscedasticity and independence of the variables, we also performed the Levene test (α-value = 0.05) and Durbin-Watson test. We used a One Sample T-test with 95% confidence interval (95% CI; α-value = 0.05) to test the demographic and clinical data. Linear regression analysis was performed to check the associations among SEL and PPTs in FM women after adjustment for age, menopause status, body mass index (BMI). The results of the linear regression analysis were shown as estimate (β) with 95% CI and p-value. We fixed the level of statistical significance at p < 0.05.
Ethics approval and consent to participate
This study has received ethical approval by the Ethics Committee of Human Research of the University of Granada, Spain (approval number: 1044/CEIH/2020). All participants signed a consent form to participate.
Results
Sociodemographic characteristics
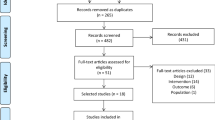
Forty-two women with FM (mean age, 52.83 ± 8.04) were recruited and met the inclusion and exclusion criteria established in this study. The sociodemographic data of women with FM are summarised in Table 1. Finally, a flow diagram of study was included (Fig. 2).

Flow diagram of participants.
Associations between strain elastography and pain pressure thresholds in women diagnosed with FM
Table 2 illustrates the associations among SEL and PPT variables in women with FM. Linear analysis regression only revealed that SEL was significantly associated with the dominant trapezius PPT (β = 0.487, 95% CI [0.045, 0.930], p = 0.032) after adjustment by age, menopause status, and BMI. There were no significant correlations between SEL and the other TPs in the women with FM.
Discussion
The aim of this study was to analyse the degree of association between the elasticity of the tissues and the level of the PPT in the characteristic TPs established for patients with FM. We hypothesized that SEL would show an increased stiffness measurement in TPs and this would be positively related to the level of the PPT. Our results showed a significant regressions association between SEL measurements and dominant trapezius PPT in patients with FM, but there were no significant regressions between SEL and the rest of the PPTs. Central sensitization is proposed as a primary key factor in the development of FM7. Given that the elastic properties of soft tissue are known to be influenced or possibly determined by the activity of the sympathetic nervous system, it is plausible that any dysfunction in the sympathetic nervous system could result in alterations in the tensegrity of the tissue. This, in turn, may significantly impact an individual’s perception of pain10,11. It is our hypothesis that if a correlation can be established between PPT and SEL in individuals with FM, it opens up the possibility of using SEL and PPT in the assessment of subjects with FM, and this theory would warrant further investigation. The fact that significant results have been found in the dominant trapezius may indicate that the presented theory only occurs in that point from the 13 TP assessed. Therefore, presenting a painful and stiff dominant trapezius may be a common characteristic and sign in those with FM, which could serve as a part of the explanatory assessment in such condition. However, this is a first research approach, and more studies are needed to corroborate our findings.
The use of SEL as a non-invasive technique to measure the mechanical properties of tissue has been increasing in recent years13,32,33. Previous studies have described using SEL in different organs, such as liver fibrosis, breast, thyroid, prostate, kidney and lymph node or low back pain13,34,35. In this regard, SEL has been used to analyse the effectiveness of different interventions such as radiofrequency27,36;radial extracorporeal shock wave therapy37, manual therapy38 and conservative physical therapy39,40 in diverse pathologies. Additionally, there is a previous study in which SEL was used to evaluate the effects of photobiomodulation on tissues in patients with FM27. SEL has also been used to perform a differential diagnosis between patients with psoriasis that suffers chronic widespread pain and patients with FM41,42,43.
To the best of our knowledge, this is the first study assessing the tissue elasticity of the TPs in female patients with FM and the relationship of these TPs to the SEL; therefore, a comparison with other studies is difficult. Muro-Culebras and Cuesta-Vargas evaluated and compared the stiffness of TPs in women with FM and in healthy subjects using sono-myography and sono-myoelastography. They observed hypoechoic areas in the ultrasound images of the upper trapezius in both groups but sono-myoelastographydid not reveal greater stiffness in these areas compared with the rest of the muscle16, which is in line with our results. Also, in this regard, a recent study by Karayol and Sibel analysed the level of association between the objectivity of visual analog scale (VAS) values and elasticity values of rhomboid major muscles using Shear Wave Elastography (SWE) in FM and healthy subjects, determining that there was no significant association between VAS scores and SWE values44. In line with our results, which show a correlation between the PPT in the trapezius muscle and SEL, the evidence suggests a higher prevalence of MTrPs in the upper quarter muscles29, with the trapezius being the most affected muscle in MTrPS40.
Recent studies have described that SEL can provide an objective and reproducible measure of the changes in elasticity in MTrPs, showing that stiff nodules vibrate with less amplitude than healthy tissue39,40,45. In this context, similarities between TPs and MTsPs have been described, since both are related to pathologies that occurs with non-inflammatory myalgia; TPs in FM and MTrPs in MPS16, and are the result of the interaction between the autonomic nervous system and anon-specific response of the central nervous system46. In this line, the study by Ge et al. in 2010 support the similarities between TPs and MTrPs, since they found that TPs sites coincide with MTrPs in people with FM47.
Since TPs can be associated with a variety of diseases such as infections, inflammation, or lesions and MTrPs are common in patients with a variety of conditions ranging from cancer, neck and shoulder disorders to spinal and musculoskeletal disorders14,17, it would be very interesting to carry out future studies that compare TPs between patients with FM and healthy subjects or that analyse and compare the characteristics of TPs/MTrPs in other pathologies.
Tissue quality is understood based on the elastic properties of connective tissue, which means proper loading capacity as well as aging. The muscle elasticity measurement indicates the stiffness of the tissue assessed. The interpretation of a “good” muscle SEL quality assessment would be one showing soft elastic characteristics rather than hard elastic characteristics. This is because of vascularity mainly and sympathetic tone. However, SEL measurements are highly evaluator-dependent and results should be interpreted with caution.
The present study shows strengths that should be highlighted. Firstly, this is the first study that analyses the relationship between the elasticity of tissue and all the PPTs in patients with FM. Secondly, all SEL measurements were carried out by an expert who has more than 10 years of experience in ultrasound and SEL. Finally, this study opens new possibilities of research in relation with soft tissue elasticity and the perception of pain.
Study limitations
The present study also has some limitations that should be recognized. Sample size is small, with FM participants only, and the design of the study is observational and cross-sectional, which means our results should be interpreted with caution. Besides, SEL measurements, although widely accepted and used, are highly dependent on the operator, which must be taken into account when interpreting our results48,49. Future studies should utilise a larger sample size and include a control group in order to corroborate our findings and extrapolate the data.
Furthermore, future studies comparing the results of SEL and PPT in TPs from patients with FM and a healthy population, as well as changes in SEL of the PPTs after a treatment program, are needed.
Conclusions
In the light of the results, there was an association between SEL measurements and dominant trapezius PPT in subjects with FM, but there was no significant association between SEL and the rest of the PPT points. Further studies to corroborate our findings and to fully explain the underlying mechanism are needed.
Data availability
The data will be available by contacting the corresponding author.
Abbreviations
- ACR:
-
American College of Rheumatology
- BMI:
-
Body mass index
- FM:
-
Fibromyalgia
- MRI:
-
Magnetic resonance imaging
- MPS:
-
Myofascial pain syndrome
- MTrPs:
-
Myofascial trigger points
- PPT:
-
Pain pressure thresholds
- SEL:
-
Strain elastography
- SWE:
-
Shear wave elastography
- SSS:
-
Symptom severity scale
- TPs:
-
Tender points
- WPI:
-
Widespread pain index
References
Bair, M. J. & Krebs, E. E. Fibromyalgia. Ann. Intern. Med. 172, ITC33–ITC48. https://doi.org/10.7326/AITC202003030 (2020).
Wolfe, F. et al. 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Semin. Arthritis Rheum. 46, 319–329. https://doi.org/10.1016/j.semarthrit.2016.08.012 (2016).
Häuser, W. et al. Fibromyalgia. Nat. Rev. Dis. Prim. 1, 15022. https://doi.org/10.1038/nrdp.2015.22 (2015).
Queiroz, L. P. Worldwide epidemiology of fibromyalgia. Curr. Pain Headache Rep. 17, 356. https://doi.org/10.1007/s11916-013-0356-5 (2013).
Cabo-Meseguer, A., Cerdá-Olmedo, G. & Trillo-Mata, J. L. Fibromyalgia: Prevalence, epidemiologic profiles and economic costs. Med. Clin. (Barc.) 149, 441–448. https://doi.org/10.1016/j.medcli.2017.06.008 (2017).
Wolfe, F. et al. The American college of rheumatology 1990 criteria for the classification of fibromyalgia. Arthritis Rheum. 33, 160–172. https://doi.org/10.1002/art.1780330203 (1990).
Chinn, S., Caldwell, W. & Gritsenko, K. Fibromyalgia pathogenesis and treatment options update. Curr. Pain Headache Rep. 20, 25. https://doi.org/10.1007/s11916-016-0556-x (2016).
Russell, I. J. & Larson, A. A. Neurophysiopathogenesis of fibromyalgia syndrome: a unified hypothesis. Rheum. Dis. Clin. N. Am. 35, 421–435. https://doi.org/10.1016/j.rdc.2009.06.005 (2009).
Peck, M. M. et al. The influence of pro-inflammatory cytokines and genetic variants in the development of fibromyalgia: A traditional review. Cureus 12, e10276. https://doi.org/10.7759/cureus.10276 (2020).
Choi, D. H. & Kim, H. S. Quantitative analysis of nailfold capillary morphology in patients with fibromyalgia. Korean J. Intern. Med. 30, 531–537. https://doi.org/10.3904/kjim.2015.30.4.531 (2015).
Morf, S. et al. Microcirculation abnormalities in patients with fibromyalgia—Measured by capillary microscopy and laser fluxmetry. Arthritis Res. Ther. 7, R209–R216. https://doi.org/10.1186/ar1459 (2005).
Basford, J. R. & An, K. N. New techniques for the quantification of fibromyalgia and myofascial pain. Curr. Pain Headache Rep. 13, 376–378. https://doi.org/10.1007/s11916-009-0061-6 (2009).
Sigrist, R. M. S., Liau, J., el Kaffas, A., Chammas, M. C. & Willmann, J. K. Ultrasound elastography: Review of techniques and clinical applications. Theranostics 7, 1303–1329. https://doi.org/10.7150/thno.18650 (2017).
Borg-Stein, J. & Stein, J. Trigger points and tender points: one and the same? Does injection treatment help?. Rheum. Dis. Clin. N. Am. 22, 305–322. https://doi.org/10.1016/s0889-857x(05)70274-x (1996).
Jahan, F., Nanji, K., Qidwai, W. & Qasim, R. Fibromyalgia syndrome: An overview of pathophysiology, diagnosis and management. Oman Med. J. 27, 192–195. https://doi.org/10.5001/omj.2012.44 (2012).
Muro-Culebras, A. & Cuesta-Vargas, A. I. Sono-myography and sono-myoelastography of the tender points of women with fibromyalgia. Ultrasound Med. Biol. 39, 1951–1957. https://doi.org/10.1016/j.ultrasmedbio.2013.05.001 (2013).
Li, L. et al. Criteria used for the diagnosis of myofascial trigger points in clinical trials on physical therapy: Updated systematic review. Clin. J. Pain 36, 955–967. https://doi.org/10.1097/AJP.0000000000000875 (2020).
Akhtar, R., Sherratt, M. J., Cruickshank, J. K. & Derby, B. Characterizing the elastic properties of tissues. Mater. Today 14, 96–105. https://doi.org/10.1016/S1369-7021(11)70059-1 (2011).
Nguyen, Q. T., Jacobsen, T. D. & Chahine, N. O. Effects of inflammation on multiscale biomechanical properties of cartilaginous cells and tissues. ACS Biomater. Sci. Eng. 3, 2644–2656. https://doi.org/10.1021/acsbiomaterials.6b00671 (2017).
Navarro-Ledesma, S., Aguilar-García, M., González-Muñoz, A., Pruimboom, L. & Aguilar-Ferrándiz, M. E. Do psychological factors influence the elastic properties of soft tissue in subjects with fibromyalgia? A cross-sectional observational study. Biomedicines 10, 3077. https://doi.org/10.3390/biomedicines10123077 (2022).
Navarro-Ledesma, S. et al. The relationship between daily physical activity, psychological factors, and vegetative symptoms in women with fibromyalgia: A cross-sectional observational study. Int. J. Environ. Res. Public Health 19, 11610. https://doi.org/10.3390/ijerph191811610 (2022).
Schleip, R. Fascial plasticity: A new neurobiological explanation—Part 1. J. Bodyw. Mov. 7, 11–19. https://doi.org/10.1016/S1360-8592(02)00067-0 (2003).
Kulshreshtha, P. & Deepak, K. K. Autonomic nervous system profile in fibromyalgia patients and its modulation by exercise: A mini review. Clin. Physiol. Funct. Imaging 33, 83–91. https://doi.org/10.1111/cpf.12000 (2013).
von Elm, E. et al. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 61, 344–349. https://doi.org/10.1016/j.jclinepi.2007.11.008 (2014).
Martín-Martín, L. et al. Association between physiological and subjective aspects of pain and disability in post-stroke patients with shoulder pain: A cross-sectional study. J. Clin. Med. 8, 1093. https://doi.org/10.3390/jcm8081093 (2019).
Navarro-Ledesma, S., Carroll, J., González-Muñoz, A., Pruimboom, L. & Burton, P. Changes in circadian variations in blood pressure, pain pressure threshold and the elasticity of tissue after a whole-body photobiomodulation treatment in patients with fibromyalgia: A tripled-blinded randomized clinical trial. Biomedicines 10, 2678. https://doi.org/10.3390/biomedicines10112678 (2022).
Navarro-Ledesma, S., Gonzalez-Muñoz, A., Carroll, J. & Burton, P. Short- and long-term effects of whole-body photobiomodulation on pain, functionality, tissue quality, central sensitisation and psychological factors in a population suffering from fibromyalgia: Protocol for a triple-blinded randomised clinical trial. Ther. Adv. Chronic Dis. 13, 204062232210780. https://doi.org/10.1177/20406223221078095 (2022).
Park, G., Kim, C. W., Park, S. B., Kim, M. J. & Jang, S. H. Reliability and usefulness of the pressure pain threshold measurement in patients with myofascial pain. Ann. Rehabil. Med. 35, 412–417. https://doi.org/10.5535/arm.2011.35.3.412 (2011).
Valera-Calero, J. A. et al. Is shear-wave elastography a clinical severity indicator of myofascial pain syndrome? An observational study. J. Clin. Med. 10, 2895. https://doi.org/10.3390/jcm10132895 (2021).
Kozinc, Ž & Šarabon, N. Shear-wave elastography for assessment of trapezius muscle stiffness: Reliability and association with low-level muscle activity. PLoS One 15, e0234359. https://doi.org/10.1371/journal.pone.0234359 (2020).
Calvo-Lobo, C. et al. Tensiomyography, sonoelastography, and mechanosensitivity differences between active, latent, and control low back myofascial trigger points: A cross-sectional study. Medicine (Baltimore) 96, e6287. https://doi.org/10.1097/MD.0000000000006287 (2017).
Navarro-Ledesma, S. & Gonzalez-Muñoz, A. Short-term effects of 448 kilohertz radiofrequency stimulation on supraspinatus tendon elasticity measured by quantitative ultrasound elastography in professional badminton players: A double- blinded randomized clinical trial. Int. J. Hyperth. 38, 421–427. https://doi.org/10.1080/02656736.2021.1896790 (2021).
Eby, S. F. et al. Validation of shear wave elastography in skeletal muscle. J. Biomech. 46, 2381–2387. https://doi.org/10.1016/j.jbiomech.2013.07.033 (2013).
Murillo, C., Falla, D., Sanderson, A., Rushton, A. & Heneghan, N. R. Shear wave elastography investigation of multifidus stiffness in individuals with low back pain. J. Electromyogr. Kinesiol. 47, 19–24. https://doi.org/10.1016/j.jelekin.2019.05.004 (2019).
Buran Çirak, Y. et al. Effect of sustained natural apophyseal glides on stiffness of lumbar stabilizer muscles in patients with nonspecific low back pain: Randomized controlled trial. J. Manip. Physiol. Ther. 44, 445–454. https://doi.org/10.1016/j.jmpt.2021.06.005 (2021).
Navarro-Ledesma, S. & Gonzalez-Muñoz, A. Mid-and long-term results using 448 kHz stimulation on the elasticity of the supraspinatus tendon measured by quantitative ultrasound elastography in badminton professionals: Prospective randomized double-blinded clinical trial with nine months of follow-up. J. Clin. Med. 11, 1664. https://doi.org/10.3390/jcm11061664 (2022).
Yoldaş, S. A. et al. Does extracorporeal shock wave therapy decrease spasticity of ankle plantar flexor muscles in patients with stroke: A randomized controlled trial. Clin. Rehabil. 35, 1442–1453. https://doi.org/10.1177/02692155211011320 (2021).
Volkan-Yazici, M. et al. Comparison of Kinesio taping and manual therapy in the treatment of patients with bruxism using shear-wave elastography: A randomised clinical trial. Int J Clin Pract. 75, e14902. https://doi.org/10.1111/ijcp.14902 (2021).
Turo, D. et al. Novel use of ultrasound elastography to quantify muscle tissue changes after dry needling of myofascial trigger points in patients with chronic myofascial pain. J. Ultrasound Med. 34, 2149–2161. https://doi.org/10.7863/ultra.14.08033 (2015).
Sancar, M., Keniş-Coşkun, Ö., Gündüz, O. H. & Kumbhare, D. Quantitative ultrasound texture feature changes with conservative treatment of the trapezius muscle in female patients with myofascial pain syndrome. Am. J. Phys. Med. Rehabil. 100, 1054–1061. https://doi.org/10.1097/PHM.0000000000001697 (2021).
Marchesoni, A. et al. Use of ultrasonography to discriminate psoriatic arthritis from fibromyalgia: A post-hoc analysis of the ULISSE study. J. Clin. Med. 11, 180. https://doi.org/10.3390/jcm11010180 (2022).
Macchioni, P. et al. Ultrasonographic and clinical assessment of peripheral enthesitis in patients with psoriatic arthritis, psoriasis, and fibromyalgia syndrome: The ULISSE study. J Rheumatol. 46, 904–911. https://doi.org/10.3899/jrheum.171411 (2019).
Marchesoni, A. et al. The problem in differentiation between psoriatic-related polyenthesitis and fibromyalgia. Rheumatology (Oxford) 57, 32–40. https://doi.org/10.1093/rheumatology/kex079 (2018).
Karayol, K. C. & Karayol, S. A. Comparison of visual analog scale and shear-wave ultrasound elastography data in fibromyalgia patients and the normal population. J. Phys. Ther. Sci. 33, 40–44. https://doi.org/10.1589/jpts.33.40 (2021).
Liang, X. N., Guo, R. J. & Li, S. New application of multimodal ultrasound imaging for identification of myofascial trigger points in the trapezius muscle. Ann. Palliat. Med. 10, 9784–9791. https://doi.org/10.21037/apm-21-2103 (2021).
Kisselev, S. B. & Moskvin, S. V. The use of laser therapy for patients with fibromyalgia: A critical literary review. J. Lasers Med. Sci. 10, 12–20. https://doi.org/10.15171/jlms.2019.02 (2019).
Ge, H. Y., Wang, Y., Danneskiold-Samsøe, B., Graven-Nielsen, T. & Arendt-Nielsen, L. The predetermined sites of examination for tender points in fibromyalgia syndrome are frequently associated with myofascial trigger points. J. Pain 11, 644–651. https://doi.org/10.1016/j.jpain.2009.10.006 (2010).
Ohrndorf, S. et al. Is musculoskeletal ultrasonography an operator-dependent method or a fast and reliably teachable diagnostic tool? Interreader agreements of three ultrasonographers with different training levels. Int. J. Rheumatol. 2010, 164518. https://doi.org/10.1155/2010/164518 (2010).
Snelling, P. J. et al. Describing the learning curve of novices for the diagnosis of paediatric distal forearm fractures using point-of-care ultrasound. Australas J. Ultrasound Med. 25, 66–73. https://doi.org/10.1002/ajum.12291 (2022).
Acknowledgements
Authors would like to thank patients with Fibromyalgia recruited in a private care practice for participating in this study.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
Study conception (S.N.L., A.G.M.), design (S.N.L., A.G.M.), acquisition of data (A.G.M.), analysis and interpretation of data (S.N.L., A.C.B.), drafting of manuscript (S.N.L., A.G.M., M.A.G., A.C.B., R.T.H.) and critical revision (S.N.L., A.G.M., M.A.G., A.C.B., R.T.H.). Authors consent for publication.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Navarro-Ledesma, S., Aguilar-García, M., González-Muñoz, A. et al. Association between elasticity of tissue and pain pressure threshold in the tender points present in subjects with fibromyalgia: a cross-sectional study. Sci Rep 13, 22003 (2023). https://doi.org/10.1038/s41598-023-49550-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-49550-y
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
