
Abstract
Diabetes Mellitus (DM) is a common chronic disease and a public health challenge worldwide. The present study aimed to analyze the trend in DM incidence, mortality, and mortality-to-incidence ratio (MIR) world over 30 years. The age-standardized DM incidence and mortality rates for both genders and different countries of the world from 1990 to 2019 were extracted from the Global Burden of Disease (GBD) study and the Human Development Index (HDI) was obtained for all countries from the United Nations Development Program (UNDP) database. The mean trends for the indicators for developing countries, developed countries, and all countries were evaluated using Generalized Estimating Equations (GEE) and the spline model. The estimates showed that the global mean trend of DM incidence from 1990 to 2019 followed an upward trend with an annual increase of 3.73 cases per 100,000 people. The global mean of DM mortality followed an upward trend with an annual increase of 0.43 cases until 2005 followed by a downward trend after this year with an annual decrease of 0.14 and the global mean MIR followed a downward trend during the same period with an annual decrease of 0.001 per 100,000 people. Besides, the mean incidence of DM in developing countries followed an upward trend similar to the trend in developed countries. Additionally, the mean mortality rate due to DM in developing countries increased with a slope of 0.62 until 2005 and then decreased with a slope of 0.02, and the mean MIR trend in the developed and developing countries showed a downward trend. Thus, developed countries followed a relatively faster decrease in MIR than developing countries.The data from the present study show the increased incidence of DM has made it one of the most important health concerns in the world, and if this issue is not addressed, this disease can cause more concerns for communities in the coming years. This being so, more DM prevention and control programs need to be put into practice.
Similar content being viewed by others


Introduction
Diabetes mellitus (DM) is a global public health problem that imposes a heavy global burden on public health and is associated with socio-economic consequences1. Various studies have shown that the incidence of DM has increased in recent decades2,3. It is predicted that the number of people with DM will increase from 171 million in 2000 to 300 million by 2025 and 366 million by 20304,5,6. The World Health Organization (WHO) report on DM mortality showed that the mortality rate due to DM increased by 3% from 2000 to 20197, and DM is the leading cause of death of 1.5 million people in 20198.
DM can lead to complications in different body organs and tissues and aggravate other disorders and complications, leading to a heavy economic burden. The mean medical costs for people with DM are estimated to be 2.3 times higher than the medical costs of people without DM. The American Diabetes Association (ADA) reported that the cost of diagnosed DM in 2017 was $327.2 billion. Given the growing economic costs and the social burden that DM and its complications impose on societies9, there is a need for further research on DM in all countries.
Generally, the increasing incidence of DM in different regions is different due to several factors such as lifestyle, eating habits, access to health care, etc. Furthermore, the prevalence of obesity is increasing all over the world10 due to high-calorie diets and sedentary lifestyles. Thus, the increased prevalence of obesity along with population aging is one of the main reasons behind the increased prevalence of DM11. Another factor affecting variations in the prevalence of DM in different countries can be the development rate of the countries. According to the WHO, the prevalence of DM in low- and middle-income countries has increased at a faster rate than in high-income countries7. Moreover, IDF Diabetes Atlas (2021) reported that three out of every four adults with DM live in low and middle-income countries12. The Human Development Index (HDI) is one of the important measures of mean achievement, living conditions, and human development in different countries. Thus, it is necessary to compare developing and developed countries in terms of the prevalence of diabetics to help policymakers in controlling the process of this disease.
Most of the epidemiological studies conducted on the incidence and mortality rate of DM have used descriptive or cross-sectional designs. Furthermore, no study has yet addressed the effects of the development and geographical location on the incidence, mortality, and MIR of diabetics. For example, in recent years, several epidemiological studies have investigated the incidence and mortality of DM in different parts of the world. Jinli Liu et al. reported that the age-standardized incidence of diabetics worldwide increased from 234 in 1990 to 285 cases per 100,000 in 201713. Xiling Lin et al. also showed that the age-standardized mortality rate worldwide increased from 15.7 to 17.5 per 100,000 people from 1990 to 201714. Thus, a suitable statistical technique with a high degree of accuracy needs to be used to describe and compare this diversity in the incidence of diabetics in different regions from 1990 to 2019. To this end, using longitudinal data, the present study aimed to examine the DM incidence and mortality rates worldwide and specify the impact of development on the variations in the DM incidence and mortality rates in different regions of the world. The insights from this study can be used by international policymaking support centers active in the field of diabetics to bridge the existing gaps.
Methods
Data sources
In this study, the data on the age-standardized DM incidence and mortality rates per 100,000 people for both genders and different countries of the world from 1990 to 2019 were extracted from the Global Burden of Disease (GBD) free online database of the Institute for Health Metrics and Evaluation (IHME) of the University of Washington15. Then, the mortality-to-incidence ratio (MIR) was calculated by dividing the age-standardized mortality rate by the age-standardized incidence rate for both sexes in each year and in different countries. MIR is a measure of the burden of disease in a specific region or country. This ratio determines whether a country or region has a higher or lower mortality rate for a specific disease that is normalized to its incidence. MIR is also a simple and common method to estimate the 5-year relative survival rate of patients16,17.
Human Development Index (HDI) data were also from the United Nations Development Program (UNDP) database for each country from 1990 to 202118. Accordingly, the countries with HDI values less than 0.788 were considered developing countries, and countries with HDI values of 0.788 or higher were taken as developed countries19. Finally, 189 countries with available incidence and mortality rates and HDI data were included in the study.
Statistical analysis
In this longitudinal study, summary statistics related to DM incidence rate, mortality rate, and MIR were presented for each IHME region from 1990 to 2019. Then, the annual mean trends of the indicators were graphically shown based on the region and the development level. In the next step, the marginal modeling approach and the Generalized Estimating Equation (GEE) method were used to evaluate the longitudinal effect of development on the incidence, mortality, and MIR of DM. GEE is a population-level approach that allows researchers to obtain estimates of model parameters that are averaged over the entire population20. To examine the mean trends in DM burden indices, the marginal model was fitted separately for developed and developing countries as shown in Eq. (1):
where \({\mu }_{ij}\) is the mean indexes for country i (i = 1,2,…,189) in year j (j = 1,2,…,30), \({\beta }_{0}\) is the intercept, and \({\beta }_{1}\) is the slope of the model showing the mean annual changes in the indices. Moreover, for cases where the mean trend had a non-linear pattern, the spline model (Eq. (2)) was used:
where \({t}^{*}\) is the turning point of the mean trend graph21. All statistical procedures and model fitting were performed in SPSS-26 and STATA-17 software.
Results
A total of 189 countries were included in the study to evaluate the DM incidence, mortality, and MIR from 1990 to 2019. Figure 1 shows the trends of the DM incidence, mortality, and MIR in different regions based on the IHME data. As can be seen, all regions experienced a significant increase in the incidence of DM during the 30 years (Fig. 1a). The mortality rate for LAC was relatively stable during the period and the HI region experienced a downward trend in the mortality rate. Moreover, the CEEECA, NAME, SA, SSA, and SAEAO regions showed an upward trend in the mortality rate due to DM. However, the NAME countries had an upward trend from 1990 to 2006 and a decreasing trend in their DM mortality from 2006 to 2019. In addition, the SAEAO countries experienced a significant upward trend from 1990 to 2005, but they followed a steady trend from 2005 to 2019. Likewise, SSA displayed an increasing trend from 1990 to 2004 and followed a stable trend from 2004 to 2019 (Fig. 1b). The trend of diabetes-induced MIR for the CEEECA and SA regions was relatively stable over the period, while an upward pattern was observed in other regions (Fig. 1c).

Mean trends of DM (a) incidence, (b) mortality, and (c) MIR rates per 100,000 individuals by IHME super regions in the period 1990–2019.
Table 1 shows the descriptive statistics for DM incidence, mortality, and MIR in each IHME region and all countries studied in 5-year intervals and 2019. As shown in the table, the countries in the SAEAO region have the highest incidence and mortality rates and the countries in the SSA region have the highest MIR from 1990 to 2019. In addition, the maximum incidence and mortality rate were found in the SAEAO region in 2019, and the maximum MIR was observed in the SSA region in 1990.
Table 2 shows the descriptive statistics for DM indicators by developing and developed countries in the studied period. As can be seen, developing countries had a lower incidence rate and a higher mortality rate and MIR in the period in question.
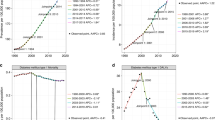
Figure 2 displays the trends of DM incidence, mortality, and MIR for developing countries, developed countries, and the whole world from 1990 to 2019. As shown in this figure, the mean incidence and MIR for developing, developed countries, and the whole world seem to follow a linear trend. Thus, the linear GEE model was used to assess the mean trends. Moreover, as the mean mortality rate for all three regions follows a non-linear pattern, the spline model (the existence of a peak in 2005) was used to investigate the DM mortality trends.

Mean trends of DM (a) incidence, (b) mortality, and (c) MIR rates per 100,000 individuals by development factor and total world countries in the period 1990–2019.
The estimated coefficients and parameters based on the GEE and spline model are presented in Table 3. The results in this table suggest that the developed countries had an intercept of about 3 per 100,000 people more than the developing countries. This means that the mean incidence rate in developed countries was about 3 per 100,000 people higher than the incidence of diabetics in developing countries in 1990. In addition, the mean incidence rates in developed and developing countries follow an upward trend, and the estimated slope of the mean incidence rates is almost the same (3.65 vs. 3.78), indicating a relatively similar increase in the mean incidence of diabetics in both developing and developing countries. Moreover, the estimated intercept for the incidence of DM in all countries was about 213.96 per 100,000 people in 1990 with a positive slope with an annual increase of 3.73 per 100,000 from 1990 to 2019 for the entire world.
The intercept for the mortality rate in developing countries was about 15 per 100,000 people more than in developed countries. The mean mortality rate from DM in developing countries increased annually until 2005 with a positive slope of 0.62 per 100,000 people and then followed a downward trend with a slope of 0.02 from 2005 to 2019. The mean trend mortality rate for developed countries was almost constant during the study period (P > 0.05). The mean mortality rate for all countries shows that the estimated intercept for the mortality rate in all countries in 1990 was about 34.40 per 100,000 people and then the annual mean mortality rate for DM increased with a positive slope of 0.43 per 100,000 people until 2005 and then followed a downward trend with a slope of 0.14 from 2005 to 2019.
Finally, the mean MIR for developing countries was about 1.8 times that of developed countries in 1990. Likewise, the estimated slope for the mean MIR in developed countries followed a downward trend and was twice that of developing countries from 1990 to 2019. Moreover, the mean global MIR decreased significantly with an annual decrease of about 0.001 units.
Discussion
The results of this study showed that the global mean incidence rate of DM followed an upward trend in both developed and developing countries from 1990 to 2019. The global mean mortality rate due to DM also followed an upward trend in developing countries until 2005, and then a downward trend, but showing no significant change in developed countries over time. The mean MIR showed a downward trend in both developed and developing countries, while developed countries had a relatively faster decrease in MIR than developing countries.
An analysis of the global incidence rate of diabetics showed that almost all countries experienced a significant upward trend from 1990 to 2019 with an annual increase of 3.73 per 100,000 people. The upward trend in the incidence of DM was consistent with some other reports around the world. For example, Lin et al. found that the incidence of DM increased globally from 1990 to 201714.
A comparison of the incidence of DM in developed and developing countries from 1990 to 2019 showed no significant difference in the increase in the incidence rate of diabetics in developed and developing countries (slope 3.65 vs. 3.78). Moreover, the descriptive analysis indicated the incidence of DM in developed countries has increased by 48.2% in these 30 years, while this increase in developing countries in the same period has been slightly higher (49.7%). According to Jinli Liu et al., the incidence of DM has increased in both developing and developed countries13.
The increased incidence of DM can typically be attributed to a higher prevalence of risky behaviors such as obesity, inactivity, and unhealthy diet. Accordingly, a systematic review study showed that lifestyle interventions such as physical activity and healthy diets can lead to a reduction in DM22. Studies have also shown that the prevalence of obesity23 and the ratio of energy received through fat has increased over time24. In addition, population aging can also be one of the reasons for the increase in the incidence of DM. Studies have confirmed that the incidence of non-communicable diseases increases with population aging25. Another factor affecting the increased incidence of DM is the improvement of DM diagnosis methods. With the improvement of DM screening techniques and improved public awareness, people's participation in screening programs has increased, leading to the detection of more diabetic cases. Furthermore, studies have indicated that the percentage of people with undiagnosed DM has decreased over time26. A study showed that the number of people who tested HbA1c increased over time. The level of public literacy has also increased in communities25. In addition to the more accurate diagnosis methods, measurement and diagnosis methods also adjusted, for example, screening criteria have changed over time and the cut-off points for DM diagnosis have decreased over time27.
An analysis of the DM mortality rate for each IHME region indicated that all regions except HI have had an increasing trend in the DM mortality rate from 1990 to 2019, as confirmed in some other reports around the world. For example, Lin et al. found that the global trend of mortality due to DM increased from 1990 to 201714. Other studies have also reported a downward trend in DM mortality in the countries in the HI region, including Canada28, Australia29, United Kingdom, and several European countries30. According to Xiling Lin et al., the mortality rate of DM in high-income countries decreased from 1990 to 201714.
The data in the present study also showed the global mean mortality rate due to DM increased by 0.43 per 100,000 people annually until 2005 following a decrease by a factor of 0.14 in each follow-up year. One of the reasons for the reduction of mortality due to DM can be the reduction of complications due to DM. Accordingly, Mohammed K Ali et al., found that hospital admissions due to diabetic complications decreased after 200531.
Our findings also suggested that the DM mortality rate in developing countries has increased by 23.9% in 30 years but decreased by 9.9% in developed countries. In a similar vein, Xiling Lin et al. compared the mortality rates due to DM between developing and developed countries and reported that the number of death due to DM increased in developing countries annually until 2005 with a positive slope of 0.62 in every 100,000 people and then followed a downward trend with a negative slope of 0.02. However, no significant change was observed in developed countries over time. The decreased mortality rate caused by DM in developing countries can be attributed to the developments in DM education, continuous monitoring of blood sugar, and widespread use of insulin and its analogs32,33. The absence of a significant change in DM mortality in developed countries can be attributed to improvements in developed countries in previous years. However, the mortality rate has followed a stable trend since then. In contrast, a study by Lin et al. and the report of the World Health Organization showed that the mortality rate due to DM has increased in the world14. A reason for such contradictory findings is that previous studies in the literature have used only descriptive statistics, while robust analytical techniques such as GEE and spline model were used in the present study to assess the linear and non-linear indicators of the DM incidence, mortality, and MIR.
In the present study, MIR was used as a surrogate index for the five-year survival rate of diabetic patients. According to our findings, MIR followed a downward trend from 0.15 in 1990 to 0.12 in 2019 with a partial slope of 0.001 (showing an mean annual decrease). Consistent with the findings of the present study, a meta-analysis study showed that the mortality proportion among DM patients in the world decreased by 43% from 1970 to 1989, by 53% from 1990 to 1999, and by 74% from 2000 to 201634. MIR is a measure of the number of patients who die after developing DM. This index can indicate the improvement of early diagnosis and better control of the disease35. A look at the MIR trend in IHME regions shows that HI countries have had the largest decrease (from 0.09 to 0.04 with a 54% decrease) in these years, while the countries in the SA region have had the lowest decrease (from 0.123 to 0.117 with a 5% decrease) in the same period. Moreover, during a 30-year follow-up, developed countries had a greater reduction in MIR of DM than developing countries. It seems that the survival rate of patients in the richest region has improved faster compared to other regions. The key reasons for this increase in survival rates are likely to be more widespread screening programs and early detection of the disease, the promotion of knowledge, attitudes, and practices of people around the world about DM prevention strategies, and improved levels of care for diabetic patients.
The significant association between HDI and MIR shows that in recent years, developed countries have focused on improving the adoption of a healthy lifestyle as well as access to health care services in the prevention or control of DM and increasing life expectancy. On the other hand, socioeconomic status is directly associated with the patient's survival. Thus, patients with higher socioeconomic status may experience more survival due to greater and better access to DM related care and services36.
The most important limitation in the present study was the unavailability of accurate and reliable data on DM incidence and mortality rates in some countries, especially in less developed areas, is a significant limitation that may affect the accuracy of the study's findings and conclusions. Therefore, future studies should focus on collecting more accurate and reliable data on DM incidence and mortality. However, the main strength of the present study was the use of longitudinal GBD data with a long follow-up period with 30 repeated measurements and the use of advanced statistical models that enabled us to obtain more accurate estimates. On the other hand, using MIR as a proxy for survival is a reliable approach to explain the differences in the age-standardized incidence and mortality rates due to DM in different geographical areas. To calculate this index, there is no need to conduct studies with long-term follow-up, which are potentially time-consuming, expensive, and prone to various biases. Moreover, to the best of our knowledge, unlike the present study, no study has evaluated the relationship between development and MIR of DM.
Conclusion
The results in the present study indicated that the increased incidence of DM is one of the most important health concerns in the world. With the extensive changes in recent years in people's lifestyles, increasing urbanization, industrialization, and population aging in developing countries, the incidence and mortality rates of diabetics are somewhat similar to developed countries. If the changes in the risk factors for DM are not taken into account, this disease can cause more concerns for communities in the coming years. This being so, countries should implement cost-effective DM prevention and control programs to increase public awareness of DM risk factors, promote active lifestyles, improve nutrition, and increase access to diagnostic and treatment services.
Data availability
The datasets generated and analysed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- DM:
-
Diabetes mellitus
- MIR:
-
Mortality-to-incidence ratio
- GBD:
-
Global burden of disease
- HDI:
-
Human development index
- UNDP:
-
United nations development program
- GEE:
-
Generalized estimating equations
- WHO:
-
World health organization
- ADA:
-
American diabetes association
- IHME:
-
Institute for health metrics and evaluation
- CEEECA:
-
Central Europe, Eastern Europe, and Central Asia
- HI:
-
High income
- LAC:
-
Latin America and Caribbean
- NAME:
-
North Africa and Middle East
- SA:
-
South Asia
- SAEAO:
-
Southeast Asia, East Asia, and Oceania
- SSA:
-
Sub-Saharan Africa
References
Patterson, C. C. et al. Trends and cyclical variation in the incidence of childhood type 1 diabetes in 26 European centres in the 25 year period 1989–2013: A multicentre prospective registration study. Diabetologia 62, 408–417 (2019).
Geiss, L. S. et al. Changes in incidence of diabetes in US adults, 1997–2003. Am. J. Prev. Med. 30, 371–377 (2006).
Patterson, C. C. et al. Trends in childhood type 1 diabetes incidence in Europe during 1989–2008: Evidence of non-uniformity over time in rates of increase. Diabetologia 55, 2142–2147 (2012).
Campbell, R. K. Type 2 diabetes: Where we are today: an overview of disease burden, current treatments, and treatment strategies. J. Am. Pharm. Assoc. 49, S3–S9 (2009).
Levitt, N. S. Diabetes in Africa: Epidemiology, management and healthcare challenges. Heart 94, 1376–1382 (2008).
Wild, S., Roglic, G., Green, A., Sicree, R. & King, H. Global prevalence of diabetes: Estimates for the year 2000 and projections for 2030. Diabetes Care 27, 1047–1053 (2004).
World Health Organization. diabetes fact sheets. https://www.who.int/news-room/fact-sheets/detail/diabetes . Accessed 5 April 2023.
Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2019. Results. Institute for Health Metrics and Evaluation., https://vizhub.healthdata.org/gbd-results/ (2020).
Association, A. D. Economic costs of diabetes in the US in 2017. Diabetes Care 41, 917–928 (2018).
Roberto, C. A. et al. Patchy progress on obesity prevention: Emerging examples, entrenched barriers, and new thinking. The Lancet 385, 2400–2409 (2015).
Mayer-Davis, E. J. & Costacou, T. Obesity and sedentary lifestyle: Modifiable risk factors for prevention of type 2 diabetes. Curr. Diab. Rep. 1, 170–176 (2001).
International Diabetes Federation. diabetes facts figures. 2021. https://idf.org/about-diabetes/facts-figures. Accessed 22 May 2023.
Liu, J. et al. Trends in the incidence of diabetes mellitus: results from the Global Burden of Disease Study 2017 and implications for diabetes mellitus prevention. BMC Public Health 20, 1–12 (2020).
Lin, X. et al. Global, regional, and national burden and trend of diabetes in 195 countries and territories: An analysis from 1990 to 2025. Sci. Rep. 10, 14790 (2020).
Global Burden of Disease (GBD). 2019. http://ghdx.healthdata.org/gbd-results-tool. Accessed 21 March 2023.
Asadzadeh Vostakolaei, F. et al. The validity of the mortality to incidence ratio as a proxy for site-specific cancer survival. Eur. J. Public Health 21, 573–577 (2011).
Choi, E. et al. Cancer mortality-to-incidence ratio as an indicator of cancer management outcomes in Organization for Economic Cooperation and Development countries. Epidemiol. Health 39 (2017).
United Nations Development Program (UNDP). https://hdr.undp.org/data-center/documentation-and-downloads. Accessed 21 March 2023.
Zhu, K.-F., Wang, Y.-M., Zhu, J.-Z., Zhou, Q.-Y. & Wang, N.-F. National prevalence of coronary heart disease and its relationship with human development index: A systematic review. Eur. J. Prev. Cardiol. 23, 530–543 (2016).
Wang, M. Generalized estimating equations in longitudinal data analysis: a review and recent developments. Adv. Stat. 2014 (2014).
Fitzmaurice, G. M., Laird, N. M. & Ware, J. H. Applied longitudinal analysis. (John Wiley & Sons, 2012).
Uusitupa, M. et al. Prevention of type 2 diabetes by lifestyle changes: A systematic review and meta-analysis. Nutrients 11, 2611 (2019).
Collaboration, N. R. F. Trends in adult body-mass index in 200 countries from 1975 to 2014: A pooled analysis of 1698 population-based measurement studies with 19.2 million participants. The lancet 387, 1377–1396 (2016).
Vadiveloo, M., Scott, M., Quatromoni, P., Jacques, P. & Parekh, N. Trends in dietary fat and high-fat food intakes from 1991 to 2008 in the Framingham Heart Study participants. Br. J. Nutr. 111, 724–734 (2014).
Thibault, V. et al. Factors that could explain the increasing prevalence of type 2 diabetes among adults in a Canadian province: A critical review and analysis. Diabetol. Metab. Syndrome 8, 1–10 (2016).
Selvin, E., Wang, D., Lee, A. K., Bergenstal, R. M. & Coresh, J. Identifying trends in undiagnosed diabetes in US adults by using a confirmatory definition: A cross-sectional study. Ann. Internal Med. 167, 769–776 (2017).
Malkani, S. & Mordes, J. P. Implications of using hemoglobin A1C for diagnosing diabetes mellitus. Am. J. Med. 124, 395–401 (2011).
Lipscombe, L. L. & Hux, J. E. Trends in diabetes prevalence, incidence, and mortality in Ontario, Canada 1995–2005: A population-based study. The Lancet 369, 750–756 (2007).
Harding, J. L., Shaw, J. E., Peeters, A., Davidson, S. & Magliano, D. J. Age-specific trends from 2000–2011 in all-cause and cause-specific mortality in type 1 and type 2 diabetes: A cohort study of more than one million people. Diabetes Care 39, 1018–1026 (2016).
Goodall, R. et al. Trends in type 2 diabetes mellitus disease burden in European Union countries between 1990 and 2019. Sci. Rep. 11, 15356 (2021).
Ali, M. K., Pearson-Stuttard, J., Selvin, E. & Gregg, E. W. Interpreting global trends in type 2 diabetes complications and mortality. Diabetologia 65, 3–13 (2022).
Jenkins, C. et al. Reducing disparities for African Americans with diabetes: Progress made by the REACH 2010 Charleston and Georgetown Diabetes Coalition. Public Health Rep. 119, 322–330 (2004).
Kirkman, M. S., Tuncer, D. & Brown, C. E. Findings from a national diabetes survey: Highlighting progress and opportunities for diabetes prevention and care. Diabetes Spect. 32, 277–283 (2019).
Chen, L. et al. A systematic review of trends in all-cause mortality among people with diabetes. Diabetologia 63, 1718–1735 (2020).
Amini, M., Zayeri, F. & Salehi, M. Trend analysis of cardiovascular disease mortality, incidence, and mortality-to-incidence ratio: Results from global burden of disease study 2017. BMC Public Health 21, 1–12 (2021).
Saydah, S. H., Imperatore, G. & Beckles, G. L. Socioeconomic status and mortality: Contribution of health care access and psychological distress among US adults with diagnosed diabetes. Diabetes Care 36, 49–55 (2013).
Acknowledgements
The authors thank the GBD and UNDP team for their free access and comprehensive database.
Author information
Authors and Affiliations
Contributions
M.B.H. contributed to the acquisition, analysis, and interpretation of data and writing the manuscript. H.M. and A.K. have contributed to the conception and design of the work and writing the manuscript. All authors have approved the final draft.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Balooch Hasankhani, M., Mirzaei, H. & Karamoozian, A. Global trend analysis of diabetes mellitus incidence, mortality, and mortality-to-incidence ratio from 1990 to 2019. Sci Rep 13, 21908 (2023). https://doi.org/10.1038/s41598-023-49249-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-49249-0
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
