
Abstract
Erectile dysfunction (ED) is a pervasive problem among men, often shrouded in silence and stigma. This manuscript analysed the National Health and Morbidity Survey 2019 data to identify the prevalence of moderate to severe ED among men aged 18 and above in Malaysia and describe its associated factors. Self-administered questionnaire on ED utilised a locally validated International Index of Erectile Function. Variables on sociodemographics, risky lifestyles and comorbidities were obtained via an interviewer-administered questionnaire. The prevalence was determined using complex sampling analysis, and logistic regression was used to determine the associated factors of ED. A sample of 2403 men aged ≥ 18 participated, with a moderate to severe ED prevalence was 31.6% (95% CI 28.8, 34.6). The mean (± SD) of the total score of IIEF-5 for overall respondents was 18.16 (± 4.13). Multiple logistic regression analysis revealed a significant association between moderate to severe ED among men aged 60 years and above, single or divorcee, men without formal, primary, and secondary education, non-government employees, unemployed, and retiree, as well as physically inactive men. Focused public health interventions are necessary to improve education in sexual health, increase health promotion programs, and promote healthy ageing across the population.
Similar content being viewed by others

Introduction
The World Health Organization defines sexual health as “fundamental to the physical or emotional health and well-being of individuals, couples, and families and their social or economic development1.” Erectile dysfunction (ED) is a common problem among men worldwide and is one of the burdens of sexual health-related issues. ED is defined as “the consistent or recurrent inability to attain and maintain a penile erection sufficient for sexual intercourse2.” The prevalence of ED is expected to increase globally, with estimated range of 3–76.5%3. By 2025, 322 million men are expected to be affected by ED worldwide, up from 152 million men in 19954.
Penile erection is a physiological response of neurovascular events integrated with an endocrine and psychological process. It involves smooth muscle relaxation, sinusoidal engorgement with arterial blood, and venous outflow occlusion. Disruption of any of these processes leads to erectile problems. Psychogenic, organic (i.e., neurogenic, hormonal, arterial, cavernosal, or drug-induced), or mixed psychogenic and organic are the three types of ED5. The latter was the common type observed in a patient with ED.
The importance of ED as a public health issue has grown exponentially. The prevalence of ED was high among men with underlying medical problems and risky lifestyles, including cardiovascular disease (CVD), hypertension, dyslipidemia, obesity, and smoking6. ED itself costs a financial burden to the healthcare system, let alone its complication7. A prescribing pattern and cost analysis study in England reported that the rate of primary care prescriptions increased two-fold between 2009 and 2019, owing primarily to more men being screened or seeking ED help8. ED shares similar underlying pathophysiology with CVD and mounting evidence that ED substantially raises CVD risk9. Early detection of CVD for men with ED as a secondary prevention technique was cost-effective for the healthcare system10. Additionally, ED had a detrimental effect on patients' psychosocial well-being and the quality of life of their couples11.
Robust epidemiological data clarifying sociodemographic, health-related correlates, and risky lifestyle are undoubtedly essential for a comprehensive understanding of ED. When the modifiable risk factors are identified, effective service delivery, resource allocation and preventive strategies could be established. Therefore, the ED module was included in the National Health and Morbidity Survey (NHMS) 2019: Non-Communicable Diseases. This study aimed to establish the prevalence of moderate to severe ED in Malaysian men aged 18 and above and its associated factors.
Methods
Sampling design and sample size
This study was part of the National Health and Morbidity Survey (NHMS) 2019: Non-Communicable Diseases, a nationwide community-based survey conducted in Malaysia in 2019. The NHMS implemented as a cross-sectional study with a two-stage stratified random sampling design to ensure nationally representative data12. The primary stratum was in all 13 states and three federal territories in Malaysia, while the secondary stratum was in the locality, urban or rural, within the states. Sample selection consists of two stages, by which the primary sampling unit (PSU) for enumeration blocks (EBs) selection and the secondary sampling unit (SSU) for living quarters (LQs) within the EBs. In this survey, a total of 475 EBs were randomly selected, with 362 EBs from urban areas and 113 EBs from rural areas. Twelve LQs were chosen randomly within the selected EBs. All individuals residing for at least two weeks in the LQs before data collection were eligible to participate in this survey.
For the ED module, the sample size was calculated based on a 6.4% estimated prevalence of ED13, design effect of 2.0, and precision of 0.025, which resulted in 2,266 optimum sample sizes. The survey's methodology and sampling design is described in detail in the NHMS 2019 official report12. The selection of eligible respondents for the ED module was based on the screening question ‘Are you 18 years and above and sexually active?’ If the response is yes, self-administered ED module would be given to the respondents.
Measures
Sociodemographic characteristics
Sociodemographic characteristics (age, residing location, ethnicity, marital status, education, occupation, household income, and household income category) were collected using a structured questionnaire, similar with the previous NHMS 12. The Malaysian government had divided household income into three categories, namely Top 20% (T20), with a monthly income above RM10,970; Middle 40% (M40) with income ranging from RM4851 to RM10970; and lastly Bottom 40% (B40) with earnings of RM4,850 a month or less14.
ED risk factors
ED risk factors include diabetes mellitus, hypertension, hypercholesterolemia, physical activity, body weight status, smoking and alcohol habits. Non-communicable diseases (diabetes mellitus, hypertension, or hypercholesterolemia) variables were defined as respondents who reported having these illnesses (self-reported) and raised blood glucose, blood pressure, or cholesterol during clinical assessments amongst those not known to have these conditions. Clinical assessments and biochemical tests were conducted by trained nurses for fasting or random blood glucose, cholesterol level, blood pressure and anthropometric measurements.
ED
Self-administered questionnaire on validated 5-item English and Malay versions of the International Index of Erectile Function (IIEF-5) was distributed to the eligible respondents (sexually active males 18 years old and above). Each item in the IIEF-5 assesses a different domain of erectile function, i.e., erection confidence, erection firmness, maintenance frequency, maintenance ability, and intercourse satisfaction. For each item, respondents could assign a score from 1 to 5, with a higher score indicating better function. Total scores on this scale ranged from five to 25, and is classified as normal (score 22–25), mild ED (score 17–21), moderate ED (score 8–16), and severe ED (score 5–7)15. Since both moderate and severe ED are more likely to require clinical treatment than mild ED, they were combined and highlighted for this paper16,17.
Data collection
A training workshop for field supervisors, data collectors, and nurses was conducted prior to the data collection. The primary objectives of the training were to familiarize the data collection teams with the questionnaires, to develop interpersonal skills, and to appreciate the need for good teamwork. Data collection was initiated from July 2019 to October 2019, covered all states and federal territories in Malaysia. Data were sent to the Institute for Public Health for quality control and database management.
Statistical analysis
Data analysis was calculated using a complex sample module in IBM Statistical Package for Social Sciences (SPSS) for Windows version 21.0 (IBM Corp., Armonk, NY, USA). A weighting factor was applied, considering the design weight and non-response, and post-stratification adjustment was done for age, sex, and ethnicity. The detailed calculation for the weighting factor was stated in the NHMS 2019 report12. Complex sample analysis was done to illustrate the mean of IIEF-5 score within the respective domains and determine the prevalence of moderate to severe ED by sociodemographic characteristics. Factors associated with moderate to severe ED were determined at both univariate and multivariable levels by using simple logistic regression and multiple logistic regression, respectively. The outcome was a binary variable coded as “0” for normal and mild ED and “1” for moderate to severe ED. Variable selection was made using the backward stepwise logistic regression method. From the simple logistic regression analysis, factors with p value < 0.25 were included for further analysis. The final model was presented with adjusted odd ratio (AOR), beta coefficient (b), and P value, with a level of significance at P value less than 0.05. Multicollinearity and two-way interaction term were checked. Hosmer–Lemeshow test, classification table, and the receiver operating characteristic (ROC) curve were done to check for model fitness.
Ethics approval
All respondents were given a bilingual (Malay and English) consent form that detailed the survey's purpose and methodology. All procedures were approved and granted ethical approval by the Medical Research and Ethics Committee of the Ministry of Health Malaysia. This study was registered with the National Medical Research Register (NMRR) as NMRR-18-3085-44207. The survey was conducted according to the Declaration of Helsinki and the Ministry of Health Malaysia guidelines and regulations to ensure that the ethical was abide during the data collection.
Results
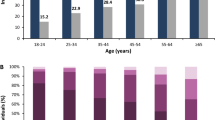
A total of 3,207 adult males were eligible for the ED module, and 2403 of them completed all the questionnaires provided, making the response rate of this study 73.5%. Table 1 shows the sociodemographic characteristics of sexually active men aged 18 and above. Figure 1 shows the mean scores according to IIEF-5 domains. Overall, the total mean score of the IIEF-5 was 18.16 ± 4.13. By domains, erection firmness shows the lowest mean score, followed by maintenance frequency and erection confidence (Fig. 1).

Descriptive mean score of IIEF-5.
Our study revealed that 31.6% of sexually active men 18 years and above reported having moderate to severe ED. The moderate to severe ED prevalence was high among rural dwellers, men aged 60 years and above, single or divorcees, people with primary education, unemployment, retiree, and people in the lowest household income category (Table 2).
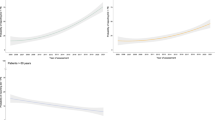
The association between moderate to severe ED and sociodemographic factors, medical conditions, and other risk factors were summarised in Table 3. Men aged 60 years and above were strongly associated with moderate to severe ED with AOR of 3.04 (95% CI 2.27, 4.10). Single or divorcees also showed higher odds with AOR of 2.88 (95% CI 2.10, 3.96) than married men. By educational status, no formal education, primary and secondary education were significantly associated with moderate to severe ED with AOR 3.04 (95% CI 1.52, 6.05), 2.30(95% CI 1.69, 3.12) and 1.81(95% CI 1.43, 2.28), respectively. Private employees, self-employed, those who were not working, unpaid workers, homemakers, students, or retirees were also associated with moderate to severe ED. Finally, physically inactive men were significantly associated with moderate to severe ED with AOR of 1.50 (95% CI 1.19, 1.89).
Discussion
From the IIEF-5 descriptive review, the total mean score was 18.16 (SD ± 4.1), comparable to the Turkish study with a mean score of 18.20 (SD ± 6.2)18. This was lower than another study done in Vienna which they found the average score was 21.3 (SD ± 4.9)19. A longitudinal study by Imai et al. reported that the mean score of ED decreased by year and rapidly declined in the older age group20. This may indicate that the prevalence of moderate to severe ED was higher in elderly than younger group. Based on our findings, moderate to severe ED prevalence was 31.6% (CI 28.8, 34.6). According to the Massachusetts Male Aging Study (MMAS), 34.8% of men aged 40–70 had moderate to severe ED21. A study done by Nicolosi et al. found that, the age-adjusted prevalence of moderate to severe ED was 17% in Italy, 15% in Brazil and 34% in Japan. Local studies reported that moderate to severe ED prevalence in Malaysia ranged from 40.8 to 46%22,23. These differences in prevalence may reflect actual demographic differences and cultural differences in the perceptions and attitudes toward ED, as the aforementioned studies were conducted among urban residents aged 40 years and older.
The high ED prevalence among older age groups was anticipated, as seen in various studies6,24,25,26. However, it was not usually expected in younger age groups. In our findings, the high prevalence of moderate to severe ED among 18–30 years old is worth discussing, even though it is not statistically significant compared to those in the 31–59 years group. The pattern of the exceptionally high prevalence of ED among young men had been observed in various studies, especially those studies using the IIEF as ED measurement tools26,27. The comparatively high prevalence of ED among young men may be explained by psychological variables such as inexperience with sexuality, performance anxiety, and life pressures. A cohort study among sexually active young adult men revealed that a history of depression, antidepressants usage, and anxiety leads to higher odds of having moderate to severe ED28. A recent study found an increased occurrence of ED in men under the age of 40, and this pattern is likely underrated due to younger populations' under-reporting29. Although ED in young adult men was believed to be due to psychogenic factors, there were increased amounts of data regarding ED as a proxy of cardiovascular, diabetes and overall men’s health30. A careful and comprehensive general health assessment of patients complaining of ED should be carried out, regardless of patient’s age.
From the multiple logistic regression analysis, men aged 60 years and above were three times more likely to have moderate to severe ED than the 31–59 years group. Advanced age has been considered the main unmodifiable risk factor for ED, with signs and symptoms most typically occurring in men over the age of 6531,32. The ageing process can affect all the components in our body (nerves, arteries, veins, muscles, and hormones), including those needed in erection function29. ED is often believed to be a regular part of the ageing process. However, this assumption may not be entirely accurate as ED is not just a natural result of ageing where to be accepted alongside other aging-related disorders. For the elderly, ED may occur due to specific illnesses or adverse treatment for certain diseases31. Ageing is unavoidable; however, maintaining good health and controlling chronic illness will help to mitigate potential health-related problems.
From our study, single or divorcee men were found to be associated significantly with moderate to severe ED, which was also observed in a number of studies28,33. Single respondents, especially teenagers and young adults, may lack experience and knowledge regarding their sexual abilities. A previous study reported that lack of sexual knowledge and anxiety are common contributing factors to ED29. A study done in Thailand found that married men rate their sexual abilities better than single, separated, divorced, and widowed males34. Unstable relationships, stress, depression, and emotional issues can be related to sexual problems and ED35. Based on NHMS 2019, single men and divorcees reported having a higher prevalence of depression than married men12. This finding corresponds to our results with the higher prevalence of moderate to severe ED among single and divorcee men than in the married group. Early sexual education and relationship counselling can be beneficial in preventing ED and encourage people to recognize their health, well-being, and dignity while developing respectful social and sexual relationships.
There was an inverse relationship between education and presence of moderate to severe ED. Similar findings were observed from various studies where low educational status was associated with ED27,35. The current study clearly showed the odd ratio reduced by education level. This association possibly explains that educated people have more knowledge and self-awareness regarding their sexual abilities and, hence, take preventive measures or treatment36. It is also possible that people with a higher education level had better socioeconomic status, thus had better access to healthcare facilities, and could afford better treatment37. A worsening economic situation causes more stress, which burdens sexual function. These would explain the high prevalence of ED in those not working and low household income.
In terms of occupation, non-governmental employees were more likely to have moderate to severe ED than government employees. There was no apparent reason for this. The aetiology of these observations is most likely complex. Working conditions, stressors, and lifestyle issues are almost certainly related. Several studies, however, indicated that particular types of occupations were associated with ED. According to the MMAS longitudinal study, men in blue-collar jobs were more likely to acquire ED than men in white-collar jobs38. In their review, Burnett et al. discovered a probable risk relationship between environmental exposures and ED. Environmental toxicants have been postulated to have a detrimental effect on erectile function primarily through their effects on the neurological and hormonal systems39.
There was a statistical difference in moderate to severe ED by comparing physical activity level. Lack of physical activity and sedentary lifestyles were strongly associated with ED40. A study by Cheng et al. concluded that moderate to high levels of physical activity reduced ED risk41. ED patients reported that moderate to vigorous-intensity aerobic exercise would enhance their sexual well-being42. An active lifestyle is the best way to increase nitric oxide (NO) and testosterone levels, improve body image, and reduce stress and anxiety43. A strategic plan is required to enhance physical activity among the population by promoting active commuting among adults and strengthening the knowledge of physical activity in the community. The transformation of sedentary lifestyles and increased physical activity might help to combat the growing epidemics of obesity and age-related diseases such as cardiovascular disorders, chronic illnesses, and ED—an unforeseen positive side effect of regular physical activity adopting in our lives.
Our study discovered that no significant association between moderate to severe ED and chronic disease (Diabetes, Hypertension, and Hypercholesterolemia) or risky behaviour (obesity, smoking, and alcohol consumption). These patterns were also observed in a few studies among the younger population28,44. One possible reason is that the study's youthful population suffered from these modifiable risk factors but had not yet experienced the consequences of these problems, which all have a detrimental effect on the vascular system over time45.
These findings suggest that ED issues in Malaysia need immediate attention and collaboration with multidisciplinary teams to handle this issue. The introduction of a formal sexual reproductive health education via a comprehensive syllabus or programs should begin from a younger age and be suited for multiethnicity and multicultural countries like Malaysia. Furthermore, advocate on expanding health promotion services, significantly to halt the progress of NCD and risky lifestyle through talks, campaigns, and social media promotion. In addition, a collaboration with multiagency is vital to raise awareness of sexual reproductive health among the community. Finally, healthcare workers should empower themselves with knowledge and training programs on diagnosing and managing ED. A future research design may be necessary to close the knowledge gap in ED in various community settings.
The study's main strength was the nationally representative sample, which allows the results to be applied to the entire Malaysian population. The large sample size ensures sufficient statistical capacity when estimating the prevalence and its associated factors. Furthermore, the validity of our self-reported data was assured by the use of structured questionnaires, self-administered data collection, and firm quality control during the survey duration. However, a few drawbacks to this research should be listed. Firstly, the cross-sectional study design eliminates the probability of a causal relationship between the associated factors and ED. Secondly, a wide range of age categories, as well as the fact that the results were focused on self-perceptions rather than clinical evaluations, could present information bias such as recall bias and misreporting that might obscure the actual issues.
Conclusion
In conclusion, ED is prevalent in Malaysia, with 31.6% of sexually active men aged 18 years and above complaining of moderate to severe ED. Age 60 years and above, single or divorcee, low educational level, non-governmental employees, and physically inactive men were significantly associated with moderate to severe ED. Therefore, focused public health interventions are necessary to improve education in sexual health, increase health promotion programs, and promote healthy ageing across the population.
Data availability
The data used to support the findings of this study are available from the corresponding author upon reasonable request.
References
Organization, W. H. Developing sexual health programmes: A framework for action (World Health Organization, 2010).
Montorsi, F. et al. Summary of the recommendations on sexual dysfunctions in men. J. Sex. Med. 7(11), 3572–3588 (2010).
Van Hemelrijck, M. et al. The global prevalence of erectile dysfunction: A review. BJU Int. 124(4), 587–599 (2019).
Ayta, I., McKinlay, J. & Krane, R. The likely worldwide increase in erectile dysfunction between 1995 and 2025 and some possible policy consequences. BJU Int. 84(1), 50–56 (1999).
Gratzke, C. et al. Anatomy, physiology, and pathophysiology of erectile dysfunction. J. Sex. Med. 7(1), 445–475 (2010).
Allen, M. S. & Walter, E. E. Erectile dysfunction: An umbrella review of meta-analyses of risk-factors, treatment, and prevalence outcomes. J. Sex. Med. 16(4), 531–541 (2019).
Wessells, H. et al. Erectile dysfunction. J. Urol. 177(5), 1675–1681 (2007).
Bell, C. et al. Prescribing patterns and costs associated with erectile dysfunction drugs in England: A time trend analysis. BJGP Open 5(2) (2021).
Dong, J.-Y., Zhang, Y.-H. & Qin, L.-Q. Erectile dysfunction and risk of cardiovascular disease: Meta-analysis of prospective cohort studies. J. Am. Coll. Cardiol. 58(13), 1378–1385 (2011).
Pastuszak, A. W. et al. Erectile dysfunction as a marker for cardiovascular disease diagnosis and intervention: A cost analysis. J. Sex. Med. 12(4), 975–984 (2015).
Fisher, W. A. et al. Erectile dysfunction (ED) is a shared sexual concern of couples II: Association of female partner characteristics with male partner ED treatment seeking and phosphodiesterase type 5 inhibitor utilization. J. Sex. Med. 6(11), 3111–3124 (2009).
Institute of Public Health. National Health and Morbidity Survey (NHMS). Non-Communicable Diseases: Risk Factors and Other Health Problems (2019).
Tan, H. M. et al. Prevalence and correlates of erectile dysfunction (ED) and treatment seeking for ED in Asian Men: The Asian Men’s Attitudes to Life Events and Sexuality (MALES) study. J. Sex. Med. 4(6), 1582–1592 (2007).
Malaysia, D. O. S. Household income estimates and incidence of poverty report, Malaysia, 2020 (2021).
Rosen, R. C. et al. Development and evaluation of an abridged, 5-item version of the International Index of Erectile Function (IIEF-5) as a diagnostic tool for erectile dysfunction. Int. J. Impot. Res. 11(6), 319–326 (1999).
Lim, T. et al. Cross-cultural adaptation and validation of the English version of the International Index of Erectile Function (IIEF) for use in Malaysia. Int. J. Impot. Res. 15(5), 329–336 (2003).
Tang, Z. et al. Comparison of the simplified International Index of Erectile Function (IIEF-5) in patients of erectile dysfunction with different pathophysiologies. BMC Urol. 14(1), 1–6 (2014).
Coban, S. et al. Does metabolic syndrome increase erectile dysfunction and lower urinary tract symptoms?. Urol. J. 11(4), 1820 (2014).
Ponholzer, A. et al. Prevalence and risk factors for erectile dysfunction in 2869 men using a validated questionnaire. Eur. Urol. 47(1), 80–86 (2005).
Iami, A. et al. MP40-15 chronological change in erectile dysfunction and its risk factors (A Community-Based Longitudinal Survey). J. Urol. 201, e592–e593 (2019).
Feldman, H. A. et al. Impotence and its medical and psychosocial correlates: Results of the Massachusetts Male Aging Study. J. Urol. 151(1), 54–61 (1994).
Nordin, R. B. et al. Prevalence and predictors of erectile dysfunction in adult male outpatient clinic attendees in Johor, Malaysia. Singap. Med. J. 60(1), 40 (2019).
Mariappan, P. & Chong, W. L. Prevalence and correlations of lower urinary tract symptoms, erectile dysfunction and incontinence in men from a multiethnic Asian population: Results of a regional population-based survey and comparison with industrialized nations. BJU Int. 98(6), 1264–1268 (2006).
Çayan, S. et al. Prevalence of erectile dysfunction in men over 40 years of age in Turkey: Results from the Turkish Society of Andrology Male Sexual Health Study Group. Turk. J. Urol. 43(2), 122 (2017).
Geerkens, M. J. et al. Sexual dysfunction and bother due to erectile dysfunction in the healthy elderly male population: Prevalence from a systematic review. Eur. Urol. Focus 6(4), 776–790 (2020).
Korneyev, I. et al. Prevalence and risk factors for erectile dysfunction and lower urinary tract symptoms in Russian Federation men: Analysis from a national population-based multicenter study. Int. J. Impot. Res. 28(2), 74–79 (2016).
Tan, J. et al. Erectile dysfunction in Singapore: Prevalence and its associated factors—a population-based study. Singap. Med J 44(1), 20–26 (2003).
Calzo, J. P. et al. Erectile dysfunction in a sample of sexually active young adult men from a us cohort: Demographic, metabolic and mental health correlates. J. Urol. 205(2), 539–544 (2021).
Nguyen, H. M. T., Gabrielson, A. T. & Hellstrom, W. J. Erectile dysfunction in young men—a review of the prevalence and risk factors. Sex. Med. Rev. 5(4), 508–520 (2017).
Capogrosso, P., Montorsi, F. & Salonia, A. Erectile dysfunction in young patients is a proxy of overall men’s health status. Curr. Opin. Urol. 26(2), 140–145 (2016).
Montorsi, F. et al. The ageing male and erectile dysfunction. BJU Int. 92(5), 516–520 (2003).
Lewis, R. W. et al. Definitions/epidemiology/risk factors for sexual dysfunction. J. Sex. Med. 7(4), 1598–1607 (2010).
Chew, K.-K. et al. Original Research–Epidemiology: Male erectile dysfunction: Its prevalence in Western Australia and associated sociodemographic factors. J. Sex. Med. 5(1), 60–69 (2008).
Kongkanand, A., T.E.D.E.S. Group. Prevalence of erectile dysfunction in Thailand. Int. J. Androl. 23, 77–80 (2000).
Laumann, E. O. et al. Sexual problems among women and men aged 40–80 y: Prevalence and correlates identified in the Global Study of Sexual Attitudes and Behaviors. Int. J. Impot. Res. 17(1), 39–57 (2005).
Kałka, D. et al. Modifiable risk factors for erectile dysfunction: An assessment of the awareness of such factors in patients suffering from ischaemic heart disease. Int. J. Impot. Res. 28(1), 14–19 (2016).
Laumann, E. O., Paik, A. & Rosen, R. C. Sexual dysfunction in the United States: prevalence and predictors. Jama 281(6), 537–544 (1999).
Aytaç, I. A. et al. Socioeconomic factors and incidence of erectile dysfunction: Findings of the longitudinal Massachussetts Male Aging Study. Soc. Sci. Med. 51(5), 771–778 (2000).
Burnett, A. L. Environmental erectile dysfunction: Can the environment really be hazardous to your erectile health?. J. Androl. 29(3), 229–236 (2008).
Selvin, E., Burnett, A. L. & Platz, E. A. Prevalence and risk factors for erectile dysfunction in the US. Am. J. Med. 120(2), 151–157 (2007).
Cheng, J. et al. Physical activity and erectile dysfunction: Meta-analysis of population-based studies. Int. J. Impot. Res. 19(3), 245–252 (2007).
Silva, A. B. et al. Physical activity and exercise for erectile dysfunction: Systematic review and meta-analysis. Br. J. Sports Med. 51(19), 1419–1424 (2017).
Allen, M. S. Physical activity as an adjunct treatment for erectile dysfunction. Nat. Rev. Urol. 16(9), 553–562 (2019).
Martins, F. G. & Abdo, C. H. N. Erectile dysfunction and correlated factors in Brazilian men aged 18–40 years. J. Sex. Med. 7(6), 2166–2173 (2010).
Rosen, R. C. et al. Epidemiology of erectile dysfunction: The role of medical comorbidities and lifestyle factors. Urol. Clin. 32(4), 403–417 (2005).
Acknowledgements
The authors would like to thank the Director General of Health Malaysia for his permission to publish this article. They would also like to thank all research team members and data collectors for their contributions and commitment in this study. They are also grateful for the kind cooperation of all respondents.
Author information
Authors and Affiliations
Contributions
M.S.R. conceptualized the study. M.F.M.A., M.A.A.R., C.Z.L., A.B.S. and M.S.A.K. were responsible for data acquisition. M.S.R. and M.F.M.A. were responsible for analysis and interpretation of data. M.A.M.D., S.B.I., and Z.M.S. provided technical input and review the manuscript. M.S.R., M.F.M.A., M.A.A.R. and C.Z.L. wrote the manuscript. All authors reviewed and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Rezali, M.S., Mohamad Anuar, M.F., Abd Razak, M.A. et al. Prevalence and associated factors of moderate to severe erectile dysfunction among adult men in Malaysia. Sci Rep 13, 21483 (2023). https://doi.org/10.1038/s41598-023-48778-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-48778-y
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
