
Abstract
The prevalence of erectile dysfunction (ED) and premature ejaculation (PE) has been investigated in many population-based studies in different regions of the world. However, reliable data are lacking for Eastern Europe. Therefore, the aim of this study was to analyze the prevalence, effect on quality of life, and treatment-related behaviors for ED and PE in a population-representative sample of Polish men. We used an Internet interview format and rigorously adapted, widely accepted instruments for ED and PE evaluation. The study included 3001 men, representative for age and place of residence and adequate proportions of respondents from urban and rural areas. The prevalence of ED was 30.1–61.1%, and the prevalence of PE was 19.3–38.1%; there were no differences between urban and rural areas. Whereas the prevalence of ED increased with age, the prevalence of PE did not increase. More than 50% of respondents with ED and more than 60% of respondents with PE had concerns about their quality of life. However, less than one fourth of participants with ED and PE were seeking treatment, most of whom received treatment. The results of our nationwide analysis, reflecting the entire Polish population of men, are consistent with other epidemiologic studies of ED and PE and may support educational campaigns and health improvement programs in Poland.
Similar content being viewed by others

Introduction
Erectile dysfunction (ED) and premature ejaculation (PE) represent significant concerns in the sexual life of men. Both conditions lead to multiple issues in personal and social functioning, impairment of physical, mental, and emotional health, and finally to decreased overall well-being and quality of life1.
A substantial group of large epidemiological studies have been focused on evaluating ED and PE at the population level in many parts of the world. Perhaps interestingly, these studies yielded disparate results, with the overall ED prevalence varying from 3 to 76.5%2, and the overall PE prevalence being from 2 to 60%3. Such wide disparities are often due to differences in the selected study population, e.g., hospital- versus community- versus population-based, age, survey methodology, participant population size, data collection method, definition of disorder or symptoms, and culture or ethnicity.
Despite the many existing epidemiological studies, reliable data for ED and PE are still lacking for Central and Eastern Europe. Even in large-scale and population-representative European studies conducted to ascertain the prevalence of ED or PE, countries from Central and Eastern Europe have not been included2,4. Although there are some population-level analyses on ED from Central (e.g., Austria5) and Eastern (e.g., Russia6) Europe, these studies have been performed in single cities (e.g., the Austrian study was limited to the Vienna area5) or burdened with a significant selection bias in terms of sample representativeness (e.g., the Russian study included patients presenting to hospitals and outpatient departments for any illness6). In sum, no large population-representative study in any country of this region has been conducted to reliably evaluate the prevalence of ED and PE. Indeed, experts stipulate that, for high-quality research, investigators should use generally accepted and professionally adapted instruments, ideally in surveying representative pools7. Population estimates of ED and PE are needed to increase general awareness, promote physical and mental health, and start appropriate educational programs. These data also tempt multidisciplinary frameworks for national health improvement programs and service deliveries instituted with appropriate allocation of resources by governments and healthcare systems.
Poland is the largest country in Central Europe8,9; by land area, Poland is the third largest in Eastern Europe, after Russia and Ukraine, and the farthest east of the European Union countries10. Until now, no reliable and population representative study on ED and PE has been conducted in Poland. Poland and other Central and Eastern European countries are demographically unique, having homogeneous or even supra-ethnic uniformity; particularly for Poland, ≥ 99% of residents are Caucasian and ≥ 90% of residents are of Polish identity11. Such unique population features need to be considered when discussing population-based studies for any symptoms or disorders. Further, healthcare-related behavior may vary significantly between countries and regions because of local cultural norms that may inhibit individuals from admitting or discussing their health issues, especially when it comes to sensitive topics like sexual life12. Indeed, Central-Eastern Europe is often considered a distinct cultural entity, and Slavic people are culturally different from other European people13. Additionally, a relatively high number of people in Poland live in rural regions. Most data from elsewhere on prevalence, burden, and treatment-related behaviors for ED and PE may not be fully transferable to Poland because the epidemiological data originate from industrialized areas, including data publicized as being from low- or middle-income countries, with no comparisons between urban and rural areas. An analysis of treatment behaviors is particularly important for ED because medical attention for this condition may uncover other serious and asymptomatic morbidities early in the course of disease (e.g., diabetes, hypertension, coronary artery disease, depression)1. Considering all these factors, our understanding of the prevalence and true burden of ED and PE in Poland is limited. Fortunately, the importance of population-based studies has gained attention in Poland and Central-Eastern Europe14. This new focus is related mainly to the increasing awareness of the detrimental impact of ED and PE on health-related quality of life. Therefore, the aim of this study was to reliably evaluate the prevalence, effect on quality of life, and treatment-related behaviors for ED and PE in a population-representative sample of adult men aged ≥ 18 years in all geographical regions of Poland.
Methods
This study was a population-based, representative, and cross-sectional investigation performed to provide estimates (stratified by age and place of residence) of ED and PE in Poland (running title: ED POLAND). We followed standardized guidelines and well-established recommendations for reporting observational studies15.
Study design
We conducted computer-assisted web interviews (CAWI) between 1 September and 1 November 2022. Given the sensitive nature of the survey subject, and after considering the general applicability of large-scale studies on sex life, we implemented a CAWI system to guarantee the anonymity of the men respondents, to encourage their participation, and to avoid interviewer bias. We opted out of face-to-face interviews and telephone surveys because direct contact between interviewers and participants could have distorted our results. Moreover, previous studies have demonstrated that results from Internet surveys on sexual health (including the Men’s Attitudes to Life and Sexuality, the Global Study of Sexual Attitudes and Behaviors, and the Premature Ejaculation Prevalence and Attitudes) were not different from those obtained by other methods, such as telephone surveys or mailed questionnaires4. Because 93.33% of households in Poland had Internet access for 2022, with no significant differences between urban and rural areas (the Eurostat data and the Central Statistical Office of Poland data16), web interviews are justified for reliable population-based studies. Pilot web-surveys with cognitive debriefing comments (n = 200) were conducted before data collection to ensure that lay persons correctly understood the survey questions. All questions and terms were presented in Polish.
The most recent population census (2021) and the proportionate quota sampling method were employed to construct a population-representative sample of respondents (i.e., to ensure that the data would represent the general population)17. The quota controls included age and place of residence (for both geographical regions, all 16 states/voivodships in Poland, and type/size of places of living, urban and rural). For both urban and rural areas, we used definitions provided by the Central Statistical Office of Poland to appropriately cover these two types of regions: (1) urban areas (cities and towns) including areas located within the administrative boundaries of cities and towns; (2) rural areas (countryside) including areas outside the administrative boundaries of the cities, which consist of areas of rural gminas and rural parts of urban–rural gminas18.
The IPSOS Poland administered the survey19. The IPSOS is a research agency with relevant international quality certificates (PKJPA, PKJBI, OFBOR, ESOMAR) and prospective population-level databases of respondents, e.g., pre-existing Internet panels (at the time of this study, the total Polish IPSOS panel had about 50,000 members)19. The panel members, extracted by quota controls, were sent e-mail inviting them to participate in a confidential survey (5,800 members were extracted to receive the invitation). A unique Uniform Resource Locator (URL) was sent to each participant. All responses, during the entire study period, were collected on a web server with appropriate Secure Sockets Layer (SSL) certificate that authenticates a website identity and enables an encrypted connection. During data collection, there were regular quality-control and stratification checks. After data collection, post-stratification weights were calculated to correct any imbalances based on differences in response rates that were not detected during data collection. The weights were computed by ranking the completed interviews to the marginals for the matching variables (i.e., age and place of residence) before all statistical analyses. In addition, to exclude fraudulent responses, participants were excluded if they answered the survey too slowly (more than 10 min per page) and too quickly (a response time of less than 20% of the average response time).
Measures
General demographic data were collected for each respondent, including age, level of education, employment status, and marital status.
ED was assessed using the five-item International Index of Erectile Function (IIEF-5)20, the most used2 and the consensual instrument for the evaluation of male sexual function1. PE was evaluated with the Premature Ejaculation Diagnostic Tool (PEDT)21, a valid screening instrument for PE22 that captures the essence of the multidimensional definition of PE1. Both questionnaires were rigorously translated and adapted into Polish23,24, and they are recommended by the European Association of Urology1.
Participants were also asked about their overall (‘If you were to spend the rest of your life in your current condition, how would you describe your overall well-being?’) and sex-specific (‘In the past 4 weeks, how were you satisfied with your sex life?’) quality of life, treatment-related behaviors (i.e., treatment seeking, receiving, satisfaction, and continuation), relevant comorbidities (i.e., arterial hypertension, myocardial infarction, any cardiac disease, diabetes, overweight, lipid disorders, stroke, any pulmonary disease, depression, any surgeries in abdomen or pelvis) and lifestyle habits (i.e., smoking, alcohol intake). All comorbidities were self-reported; we did not seek validation from medical records.
Objectives
The primary study objective was to estimate the prevalence of ED and PE in men aged ≥ 18 years in Poland. Because previous studies were based on different thresholds of IIEF-5 and PEDT scores to assess ED and PE prevalence, we decided to adapt diverse definitions of various score intervals to make our results reliably comparable with multiple studies. For ED prevalence, definition I: IIEF-5 score of 21 points or less; definition II: IIEF-5 score of 16 points or less. For PE prevalence, definition I: PEDT score of 9 points or more; definition II: PEDT score of 11 points or more.
Secondary study objectives included the prevalence of different levels of ED severity (17–21 points from IIEF-5 indicating mild ED; 12–16 mild to moderate ED; 8–11 moderate ED; 5–7 severe ED), the effect of ED and PE on overall and sex-specific quality of life, the treatment behaviors for ED and PE, the correlations between ED/PE and relevant comorbidities/lifestyle habits, and the direct relation between ED and PE.
Statistics
Quantitative variables were characterized by means, standard deviations, medians, minimum and maximum values (ranges), and 95% confidence intervals (CIs). Categorical variables were presented with numbers and percent. The Shapiro–Wilk test was used to test a normal distribution and the Leven (Brown-Forsythe) test was used to test the hypothesis of equal variances. Differences between two groups were tested with the Student t-test (in the absence of homogeneity of variance, the Welch test was used) or with the Mann–Whitney U test (model of unrelated variables) or with the Wilcoxon pair order test (model of related variables). Differences between more than two groups were tested with the F test (ANOVA) or Kruskal–Wallis test (model of unrelated variables) or with the Friedman test (model of related variables). When statistically significant differences between groups were obtained, post hoc tests were used (Tukey test for F test, Dunn test for Kruskal–Wallis test). For categorical variables, Chi-square test was applied (with Yates correction, assessment of Cochran conditions, and Fisher exact test, if applicable). The Pearson and/or Spearman correlation coefficients were calculated to establish relationships, strengths, and directions between variables. To analyse the effect of comorbidities and lifestyle habits on ED and PE, we also used logistic regression models. For regression models, we included results of the questionnaires as raw data (raw scores). Statistical significance was considered at p < 0.05. STATISTICA (StatSoft Inc., 2014, version 12.0.) was used to conduct data analysis.
For sample size calculation, we followed the methodology that was used in other population-based studies of ED/PE25,26,27,28. Thus, we computed the sample size based on the population age distribution, available from the recent census17, and expected ED/PE prevalence. Assuming a 95% confidence interval, we calculated that 2200 men in Poland would exceed the required sample size for estimating ED/PE prevalence. However, after analysing the recent census with general recommendations for future population-representative analyses, and after consulting with two independent teams of epidemiologists with relevant healthcare backgrounds, the sample size was raised to 3000 respondents. This increase in sample size provided smaller margins of error with no negative effects on any statistical analyses17. With a national sample of 3000, there was a 95% certainty that the overall survey results would be between ± 1–2% of what they would have been had we polled the entire adult male Polish population.
Ethics approval
The study was performed in compliance with Good Clinical Practice and in accordance with the Declaration of Helsinki. The Research Ethics Committee of Jagiellonian University Medical College, Krakow, Poland approved the study (1072.6120.331.2021); in addition, the study was registered with ClinicalTrials.gov (NCT05462171).
Consent to participate
All participants provided informed consent.
Results
In all, 3001 men from across the country participated in the survey (response rate: 51.7%). Given the large sample size, the respondents were categorized into six age groups, 18–24, 25–34, 35–44, 45–54, 55–64, and ≥ 65 (10.3%, 19.5%, 23.4%, 18.3%, 19.3%, 9.2%, respectively, percent of all respondents). Most of the participants had at least secondary education, were employed, and married. More respondents lived in urban areas than in rural regions (75.8 vs. 24.2%). Table 1 presents detailed demographic characteristics.
Prevalence of ED
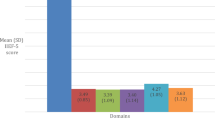
The prevalence of ED was 61.1% based on IIEF-5 score of 21 points or less (definition I), and the prevalence was 30.1% based on IIEF-5 score of 16 points or less (definition II). With both definitions, the prevalence of ED increased with age (Fig. 1; p < 0.0001, Spearman’s correlation coefficient R = −0.63). In all age groups, except for ≥ 65, ‘mild’ ED was the most prevalent ED severity category. In the ≥ 65 age group, ‘mild to moderate’ ED was the most prevalent group. In addition, the severity of ED increased with age (p < 0.0001, Spearman’s correlation coefficient R = −0.51).

Prevalence (A) and distribution of severity (B) for ED based on the two study definitions: definition I—IIEF-5 score of 21 points or less; definition II—IIEF-5 score of 16 points or less. (N = 3001).
We did not find any difference in ED prevalence across all geographical regions (voivodships) of Poland. There were also no significant correlations between ED prevalence and urban/rural status (definition I p = 0.4211, definition II p = 0.9101). However, other basic demographical parameters had important effects on ED prevalence. The prevalence of ED was lowest among men who had higher education, were employed, and married (Fig. 2; p < 0.0001 for all comparisons).

Education- (A), employment- (B), and marital status-specific (C) prevalence of ED based on the two study definitions: definition I—IIEF-5 score of 21 points or less; definition II—IIEF-5 score of 16 points or less.
Prevalence of PE
The prevalence of PE was 38.1% based on PEDT score of 9 points or more (definition I), and the prevalence was 19.3% based on PEDT score of 11 points or more (definition II). There were no differences in PE prevalence between age groups (Fig. 3; definition I p = 0.6143, definition II p = 0.0623).

Prevalence of PE based on the two study definitions: definition I—PEDT score of 9 points or more; definition II—PEDT score of 11 points or more. (N = 3001).
The PE prevalence did not differ across all geographical regions (voivodships) of Poland. There were also no significant correlations between PE prevalence and urban/rural status (definition I p = 0.6143, definition II p = 0.1673). We did not observe correlations between PE and education, employment, and marital status (p > 0.05 for all comparisons).
Effect of ED and PE on overall quality of life
ED and PE had negative effects on overall quality of life. With definition I for ED, 48.7% of the respondents were ‘mixed’, ‘moderately dissatisfied’, or ‘dissatisfied’ with their overall quality of life. Corresponding data for ED definition II were 56.1%.
With definition I for PE, 53.9% of the respondents were ‘mixed’, ‘moderately dissatisfied’, or ‘dissatisfied’ with their overall quality of life. With definition II for PE, 58.7% of the survey participants responded similarly.
We also found that the more severe the ED or PE, the worse the overall quality of life (for ED: p < 0.01, Spearman's Rank correlation coefficient R = −0.33; for PE: p < 0.0001, Spearman's Rank correlation coefficient R = 0.30).
Effect of ED and PE on sex-specific quality of life
The effects of ED and PE on sex-specific quality of life were more profound. According to definition I, 51.6% of the ED individuals reported that they were ‘mixed’, ‘moderately dissatisfied’, or ‘dissatisfied’ with the quality of their sex life. With ED definition II, 61.3% responded similarly.
Approximately 56% of the PE individuals classified by definition I reported that they were ‘mixed’, ‘moderately dissatisfied’, or ‘dissatisfied’ with the quality of their sex life. With PE definition II, 58.3% of the survey participants responded similarly.
We also found that the more severe the ED or PE, the worse the sex-specific quality of life (for ED: p < 0.01, Spearman's Rank correlation coefficient R = -0.37; for PE: p < 0.0001, Spearman's Rank correlation coefficient R = 0.28).
Treatment behaviors for ED
Among respondents with IIEF-5 score of 21 points or less (definition I), 16.1% (n = 295) were seeking treatment and most of them (80.3%, n = 237) received treatment. For respondents with IIEF-5 score of 16 points or less (definition II), 23.4% (n = 211) were seeking treatment, and, again, many of these persons received treatment (78.2%, n = 165). For the respondents who received treatment, most continued treatment (87.3%, n = 207, for definition I; 89.1%, n = 147, for definition II) and most were satisfied with their therapy (80.2%, n = 190, for definition I; 77.0%, n = 127, for definition II).
We found that men with severe ED were more likely to seek treatment (p < 0.01), to continue the treatment (p = 0.0239), and to be satisfied with the treatment (p = 0.0037).
Urban/rural status did not affect any treatment behavior for ED (p = 0.6978).
Treatment behaviors for PE
Among respondents with PEDT score of 9 points or more (definition I), 14.4% (n = 165) were seeking treatment and most of them (76.4%, n = 126) received treatment. For respondents with PEDT score of 11 points or more (definition II), 15.4% (n = 89) were seeking treatment, and, again, most of these persons received treatment (80.9%, n = 72). For the respondents who received treatment, most continued (84.9%, n = 107, for definition I; 77.8%, n = 56, for definition II) and were satisfied (77.8%, n = 98, for definition I; 75.0%, n = 54, for definition II).
We found that men with severe PE were more likely to seek treatment (p = 0.0001) and to continue the treatment (p = 0.0422).
There were no differences between urban and rural areas in treatment behaviors for PE (p = 0.7804).
Correlations between ED/PE and relevant comorbidities/lifestyle habits
In a univariate logistic regression analysis, we found positive correlations between ED and arterial hypertension, myocardial infarction, any other cardiac disease, diabetes, overweight, lipid disorders, stroke, any pulmonary disease, depression, any surgeries in abdomen or pelvis, and alcohol intake. A multivariable logistic regression analysis disclosed correlations between ED and depression, any pulmonary disease, and lipid disorders. Detailed descriptions are presented in Table 2.
In both univariate and multivariable logistic regression analyses, we did not observe any correlations between PE and relevant comorbidities/lifestyle habits (Table 2).
Relationship between ED and PE
We found a significant correlation between ED and PE; the likelihood of PE increased with the severity of ED (Spearman's Rank correlation coefficient R = −0.25, p < 0.01). The results are presented in Table 3.
Discussion
This study is the first population-representative epidemiological analysis of ED and PE conducted in a country of Central and Eastern Europe. We included respondents aged ≥ 18 years from all geographical regions of the country with adequate proportions of participants from urban and rural areas. We relied on instruments that are widely accepted and generally used for ED and PE evaluation, and we employed regular quality-control checks. Therefore, our investigation provides reliable, consistent, and valid population-level estimates of ED and PE prevalence, their effects on quality of life, and the treatment behaviors of affected individuals. We showed that ED and PE were highly prevalent and had negative effects on overall and sex-specific quality of life. However, most Polish men did not seek treatment for these conditions.
In a systematic review, Kessler et al. concluded that the global prevalence of ED was 13.1–71.2% as determined by studies based on the IIEF/IIEF-52. Pooled results revealed the highest prevalence in Europe (up to 76.5%) and the lowest prevalence in South America (up to 55.2%). The authors suggested that the geographical disparities in ED prevalence were likely determined by genetic, environmental, lifestyle, and, importantly, cultural factors. Our observation (n = 3001) of ED in 30.1–61.1% of men aged ≥ 18 appears broadly comparable with data from population-based studies performed in other countries and regions. Similarly, our analysis confirmed a trend of increasing ED prevalence with increasing age. However, although ED prevalence varies across countries and regions, we need to recognize that ED affects people worldwide, and it is a serious public health concern. Moreover, we need to consider that, to some extent, all factors that influence ED (i.e., genetic, environmental, lifestyle, cultural) do not appear to affect ED occurrence. As the population has become older, and as obesity, diabetes, and hypertension become more prevalent, ED is becoming more common.
Until now, only one study was conducted to assess the population burden of ED in Poland. In 2006, Haczyski et al. analyzed the data reported by 340 randomly chosen physicians who were asked to interview five to twenty consecutive patients aged at least 40 years about the presence of ED29. From 3,552 returned questionnaires, the authors estimated an ED prevalence of 42.7%. However, since this finding was reported, the investigation has been questioned because the results were not based on a population-representative sample but were based on clinical convenience samples of special patient populations. Critically, results of studies of clinical populations cannot be extrapolated to the general population25. Some experts correctly suggest that men who frequently visit their physicians are more likely to be diagnosed with ED, often because of their comorbidities. Further, Haczynski et al. did not exploit a widely used and rigorously adapted instrument to assess ED; instead, they used their own questions that were not universally vetted. Although the study of Haczynski et al. laid the foundations for ED research in Poland, recent improvements in assessing erectile function have triggered the need to determine the true burden of ED in Poland. This determination requires the use of a reliable and generally accepted questionnaire for ED evaluation of a representative pool of men. Finally, there has never been an assessment of seeking professional help, treatment receiving, treatment satisfaction, and treatment continuation for ED in Poland. In view of all these concerns, we instituted the ED POLAND study to assess the true burden of ED in Poland.
The prevalence of PE has not been analysed to an extent similar to that of ED. Because there is lack of a clear and universally accepted definition of PE30,31,32, current diagnostic criteria are variable and largely rely on subjective measurements3. Further, experts recently proposed a new taxonomy for PE that encompasses other unaddressed and crucial clinical aspects of PE33. In addition, there is no consensus on normal ejaculatory latency time, perception of it varies by country, and diagnosis can further depend on whether it is assessed by patients or their partners. These limitations have impeded research on the prevalence of PE and the wide discrepancy in PE prevalence estimates has been well described1. The Global Study of Sexual Attitudes and Behaviors showed that approximately one-third of all men may have PE, but there were significant geographical differences34. The lowest prevalence was reported in the Middle East (12.4%), whereas the highest recorded prevalence occurred in Southeast Asia (30.5%). Notably, to assess PE, the study used only a single-item self-reported question about the reduction in ejaculatory latency time. Importantly, because bother is important for patient stratification, diagnosis, and treatment1, the current recommendation is that only individuals who report bothersome PE should be targeted (i.e., men with (1) reduced ejaculatory latency time, (2) negative personal consequences, such as distress, bother, frustration, and/or the avoidance of sexual intimacy, (3) and perceived lack of control over ejaculation)1,33. As a patient’s perception of PE is both an important component of diagnosis or treatment success and often subjective and highly individual, validated screening instruments that include relevant symptom burden of the disease seem to be optimal in population-based analyses1. Interestingly, the evolution in methodology of studies to assess PE prevalence has been noted; whereas some older studies estimated PE prevalence from single questions that asked about early ejaculation or that used crude time-intervals to ejaculation 35,36, recent studies were based on validated instruments for PE screening37,38,39. Therefore, we used the PEDT, a questionnaire that has demonstrated high sensitivity and specificity in identifying PE1, and its validity has been widely accepted in estimating PE prevalence in other large population-based analyses1,37,38,39. With the PEDT, we revealed a PE prevalence of 19.3–38.1%. In the United States Global Online Sexuality Survey study that also was based on the PEDT, 49.6% of respondents were classified as having PE38. In contrast, with the same instrument the PE prevalence was 12.1% in a Korean cohort of married couples40. These results agree with those reported from Italy and Australia, where PEDT-assessed PE prevalence was estimated to be 15.6%41 and 16%42, respectively. When we consider differences in methods of measuring PE and study populations, overall PE prevalence in our study appears consistent with international analyses. Moreover, in our study, we did not find an association between PE prevalence and age, an observation consistent with other global analyses4,39,43.
We confirmed that ED and PE had negative effects on overall and sex-specific quality of life. Importantly, the degree of bother caused by ED and PE may be independent of how researchers define ED and PE44. Although these conditions are not life-threatening, they result in withdrawal from sexual intimacy and may lead to anxiety, depression, anger, frustration, poor self-esteem, guilt, and lack of confidence. In additions, partners of ED and PE patients may be negatively impacted by ED and PE due to relationship difficulties and sexual dissatisfaction. The occurrence of ED may even negatively affect work productivity because men with ED have higher rates of absenteeism due to psychosocial and physical reasons45. Generally, many studies demonstrated that men with ED and PE experience a deterioration in psychological, social, physical, and economic well-being compared with men who do not have these conditions44.
The low rate of treatment seeking despite the negative effects of ED and PE on multiple aspects of life is a significant public health concern. We showed that only 16.1–23.4% of respondents with ED and 14.4–15.4% of those with PE were seeking treatment. Fortunately, most of these individuals received treatment, they continued the treatment, and they were satisfied with the treatment. The low percentage of people with ED and PE who sought treatment has been reported elsewhere. An Asian study showed that only 21% of men with ED sought medical care46. The results of European Burden of Illness Study (conducted in France, Germany, Italy, Spain, and the United Kingdom) showed that more than half of European men with self-reported ED did not discuss their condition with their physician47. For PE patients, a study from Turkey demonstrated that 22.4% of PE individuals were actively looking for treatment48. In Spain, a population-based study showed that only 16.7% of participants with PE were active in seeking information about the condition49. Barriers to seeking treatment include embarrassment, anxiety, social stigma, and treatment cost. In addition, often people are simply unaware that there may be treatment for their ailment; this issue is particularly important for men with PE. The knowledge about treatment-related behaviors may significantly support educational campaigns, health improvement programs, and resource allocation. Without adequate information about treatment, individuals cannot take optimal treatment seeking action. Finally, we can speculate that a true communication gap exists between Polish patients with PE or ED and their physicians.
We investigated a significant correlation between ED and PE at the population level. Therefore, our results support recent recommendations based on the new taxonomic clinical entity of the loss of control of erection and ejaculation33. Comorbidity of ED and PE has been reported50,51, and experts hypothesized a vicious cycle of ED and PE33. On the one hand, a man striving to control his ejaculation instinctively reduces his level of excitement, leading to ED. On the other hand, a man attempting to have an erection tries to increase his excitation, and the resulting overexcitement can undermine ejaculatory control52. Because the standard screening for ED and PE may lead to false positive results (up to 33%)53, experts propose introduction of the loss of control of erection and ejaculation as the primary definition of a disorder that is viewed as two deeply interrelated sexual symptoms33. Importantly, introducing this novel disorder may help to avoid consideration of ED and PE as completely separate entities.
A strong point of our study was an adequate representation of the entire population, with well-balanced demographic characteristics, and appropriate proportions of urban and rural area participants. We also employed the recent census to stratify our variables. Because our sample size was large (n = 3001), the results were within ± 1–2% of statistical error for the national population, making our analysis one of the most accurate in the current literature of ED and PE prevalence for a single country. We used well-established and rigorously adapted diagnostic tools for ED and PE evaluation together with many other questions. Before conducting the study, we extensively reviewed the literature to select appropriate instruments and to adapt appropriate cut-offs for these instruments. Although some investigators who performed population-level studies adapted the most widely used IIEF-5 threshold of 21 points or less to recognise ED2, other studies have been based on a lower threshold of 16 points or less, e.g., the Boston Area Community Health Survey54. The threshold of 16 points or less combines patients characterized as ‘no ED’ and ‘mild ED’ and makes a stricter estimate of ED, sometimes even considered as a clinically significant ED25. For the same reason, i.e., to make our results broadly comparable and to present population estimates that can be compared with multiple studies, we adapted two thresholds of PEDT: 9 or more (the threshold that combined respondents with ‘probable PE’ and ‘PE’21), and 11 or more (a stricter definition that comprised only respondents with ‘PE’21). Importantly, other investigators used this approach of two different PEDT cut-offs in population-based studies of PE21,37,55,56. Thus, our population-based analysis, that was planned in line with the current guidelines and recommendations, provides a clear view of the prevalence and related effects of ED and PE in Poland.
A main limitation of our study was the use of self-reports to measure ED and PE without medical evaluation. We did not also investigate the sexual orientation of respondents. In addition, we did not investigate the prevalence of lifelong and acquired PE. Nevertheless, because there is no consensus on definitions of lifelong and acquired PE, this assessment of lifelong and acquired PE was also omitted from other population-based studies43. To evaluate overall and sex-specific quality of life, we used only single questions. We did not ask about all factors that may interfere with the quality of life (e.g., psychological well-being, financial income, interpersonal relationships) as we had to limit the number of questions in our survey to foster respondent compliance. Because this study was conducted in Poland, results may not be generalizable elsewhere, especially for treatment-related behaviors. However, similar findings on behaviors related to treatment have been reported in other countries.
Conclusions
This investigation was the first nationwide, population-representative epidemiological study of ED and PE performed in Poland. ED and PE were prevalent conditions and had negative effects on quality of life. However, less than one fourth of respondents with ED or PE were seeking treatment. Our findings agree with other epidemiologic reports of ED and PE conducted in different regions of the world, and our findings can support educational campaigns and health improvement programs for patients with ED and PE.
Data availability
All data generated or analysed during this study are included in this published article.
References
European Association of Urology (EAU), Non-Oncology Guidelines; Sexual and Reproductive Health, Publicated: 2022 [Accessed: 2023 February]. Available from: https://uroweb.org/guidelines/sexual-and-reproductive-health.
Kessler, A., Sollie, S., Challacombe, B., Briggs, K. & Van Hemelrijck, M. The global prevalence of erectile dysfunction: A review. BJU Int 124, 587–599 (2019).
Montorsi, F. Prevalence of premature ejaculation: A global and regional perspective. J. Sex Med. 2(Suppl 2), 96–102 (2005).
Porst H, Montorsi F, Rosen RC, et al. the premature ejaculation prevalence and attitudes (PEPA) survey: Prevalence, comorbidities, and professional help-seeking. European urology 2007. 51, 816–823; discussion 824.
Madersbacher, S. et al. Prevalence and risk factors for erectile dysfunction in Austria: Analysis of a health screening project. Wien Klin Wochenschr 115, 822–830 (2003).
Korneyev, I. A. et al. Prevalence and risk factors for erectile dysfunction and lower urinary tract symptoms in Russian Federation men: analysis from a national population-based multicenter study. Int J Impot Res 28, 74–79 (2016).
Bouwman, I. I. et al. Do lower urinary tract symptoms predict cardiovascular diseases in older men? A systematic review and meta-analysis. World J Urol 33, 1911–1920 (2015).
Organisation for Economic Co-operation and Development (OECD), OECD Library; Constitutions of Central and Eastern European Countries and the Baltic States, Publicated: 1995 [Accessed: 2023 February]. Available from: https://www.oecd-ilibrary.org/docserver/5kml6gf26mvk-en.pdf?expires=1678475807&id=id&accname=guest&checksum=5E447E991C079D0CBDF07E3D3B2D7CCF.
World Bank Group, World Bank; Poland At-A-Glance, Publicated: 2019 [Accessed: 2023 February]. Available from: https://www.worldbank.org/en/country/poland.
Publications Office of the European Union; Country profile, Publicated: 2004 [Accessed: 2023 February]. https://european-union.europa.eu/principles-countries-history/country-profiles/poland_en.
Glowny Urzad Statystyczny (GUS), Narodowy Spis Powszechny, Struktura narodowo-etniczna, językowa i wyznaniowa ludności Polski [National-ethnic, linguistic and religious structure of Poland. National Census of Population and Housing 2011] (in Polish); Publicated: 2015 [Cited: 2023 February] ISBN 978-83-7027-597-6.
Welch, L. C., Botelho, E. M. & Tennstedt, S. L. Race and ethnic differences in health beliefs about lower urinary tract symptoms. Nurs. Res. 60, 165–172 (2011).
Jarczak, J. et al. Mitochondrial DNA variability of the Polish population. Eur J Hum Genet 27, 1304–1314 (2019).
Przydacz, M., Golabek, T., Dudek, P., Lipinski, M. & Chlosta, P. Prevalence and bother of lower urinary tract symptoms and overactive bladder in Poland, an Eastern European Study. Sci. Rep. 10, 19819 (2020).
von Elm, E. et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 370, 1453–1457 (2007).
Glowny Urzad Statystyczny (GUS), Spoleczenstwo informacyjne w Polsce w 2022 r. Publicated: 2022 [Cited: 2023 February]. Available from: https://stat.gov.pl/download/gfx/portalinformacyjny/pl/defaultaktualnosci/5497/2/12/1/spoleczenstwo_informacyjne_w_polsce_w_2022_r.pdf.
Glowny Urzad Statystyczny (GUS), Narodowe Spisy Powszechne; Publicated: 2021 [Cited: 2023 January]. Available from: https://stat.gov.pl/spisy-powszechne/.
Glowny Urzad Statystyczny (GUS) Regional Statistics. Classification of Territorial Units. Administrative Division of Poland Types of Gminas and Urban and Rural Areas Publicated: 2022 [Cited: 2023 February]. Available from: https://stat.gov.pl/en/regional-statistics/classification-of-territorial-units/administrative-division-of-poland/types-of-gminas-and-urban-and-rural-areas/.
Program Kontroli Jakosci Pracy Ankieterow (PKJPA), Organizacja Firm Badania Opinii i Rynku (OBFOR); Publicated: 2000 [Cited: 2023 February]. Available from: https://www.pkjpa.pl.
Rosen, R. C., Cappelleri, J. C., Smith, M. D., Lipsky, J. & Peña, B. M. Development and evaluation of an abridged, 5-item version of the International Index of Erectile Function (IIEF-5) as a diagnostic tool for erectile dysfunction. Int J Impot Res 11, 319–326 (1999).
Symonds, T. et al. Development and validation of a premature ejaculation diagnostic tool. Eur. Urol. 52, 565–573 (2007).
Pivonello, R. et al. Sex disparities in COVID-19 severity and outcome: Are men weaker or women stronger?. Neuroendocrinology 111, 1066–1085 (2021).
Przydacz, M., Chlosta, M., Zembrzuski, M., Wiatr, T. & Chlosta, P. Polish translation and cross-cultural adaptation of the five-item International Index of Erectile Function. Cent European J Urol 75, 216–219 (2022).
Symonds, T. et al. Further evidence of the reliability and validity of the premature ejaculation diagnostic tool. Int J Impot Res 19, 521–525 (2007).
Mak, R., De Backer, G., Kornitzer, M. & De Meyer, J. M. Prevalence and correlates of erectile dysfunction in a population-based study in Belgium. Eur. Urol. 41, 132–138 (2002).
Chen, K. K. et al. Prevalence of erectile dysfunction and impacts on sexual activity and self-reported intercourse satisfaction in men older than 40 years in Taiwan. Int J Impot Res 16, 249–255 (2004).
Chew, K. K., Stuckey, B., Bremner, A., Earle, C. & Jamrozik, K. Male erectile dysfunction: its prevalence in Western australia and associated sociodemographic factors. J Sex Med 5, 60–69 (2008).
Quilter, M., Hodges, L., von Hurst, P., Borman, B. & Coad, J. Male Sexual function in New Zealand: A population-based cross-sectional survey of the prevalence of erectile dysfunction in men aged 40–70 years. J Sex Med 14, 928–936 (2017).
Haczynski, J. et al. The prevalence of erectile dysfunction in men visiting outpatient clinics. Int J Impot Res 18, 359–363 (2006).
Serefoglu, E. C. et al. An evidence-based unified definition of lifelong and acquired premature ejaculation: report of the second International Society for Sexual Medicine Ad Hoc Committee for the Definition of Premature Ejaculation. J Sex Med 11, 1423–1441 (2014).
Althof, S. E. et al. An update of the International Society of Sexual Medicine’s guidelines for the Diagnosis and treatment of premature ejaculation (PE). Sex. Med. 2, 60–90 (2014).
Shindel, A. W. et al. Disorders of ejaculation: An AUA/SMSNA guideline. J Urol 207, 504–512 (2022).
Colonnello, E., Ciocca, G., Limoncin, E., Sansone, A. & Jannini, E. A. Redefining a sexual medicine paradigm: Subclinical premature ejaculation as a new taxonomic entity. Nat Rev Urol 18, 115–127 (2021).
Laumann, E. O. et al. Sexual problems among women and men aged 40–80 y: Prevalence and correlates identified in the Global Study of Sexual Attitudes and Behaviors. Int J Impot Res 17, 39–57 (2005).
Laumann, E. O., Paik, A. & Rosen, R. C. Sexual dysfunction in the United States: Prevalence and predictors. JAMA 281, 537–544 (1999).
Nolazco, C. et al. Prevalence of sexual dysfunctions in Argentina. Int J Impot Res 16, 69–72 (2004).
Lee, S. W. et al. The prevalence of premature ejaculation and its clinical characteristics in Korean men according to different definitions. Int J Impot Res 25, 12–17 (2013).
Shaeer, O. The global online sexuality survey (GOSS): The United States of America in 2011 Chapter III–Premature ejaculation among English-speaking male Internet users. J Sex Med 10, 1882–1888 (2013).
Karabakan, M. et al. The prevalence of premature ejaculation in young Turkish men. Andrologia 48, 895–899 (2016).
Hwang, I., Yang, D. O. & Park, K. Self-reported prevalence of and attitudes toward premature ejaculation in a community-based study of married couples. World J Mens Health 31, 70–75 (2013).
Lotti, F. et al. Clinical correlates of erectile dysfunction and premature ejaculation in men with couple infertility. J Sex Med 9, 2698–2707 (2012).
McMahon, C. G., Lee, G., Park, J. K. & Adaikan, P. G. Premature ejaculation and erectile dysfunction prevalence and attitudes in the Asia-Pacific region. J Sex Med 9, 454–465 (2012).
Brock, G. B. et al. Canadian male sexual health council survey to assess prevalence and treatment of premature ejaculation in Canada. J Sex Med 6, 2115–2123 (2009).
Elterman, D. S. et al. The quality of life and economic burden of erectile dysfunction. Res Rep Urol 13, 79–86 (2021).
Goldstein, I. et al. The association of erectile dysfunction with productivity and absenteeism in eight countries globally. Int. J. Clin. Pract. 73, e13384 (2019).
Nicolosi, A., Glasser, D. B., Kim, S. C., Marumo, K. & Laumann, E. O. Sexual behaviour and dysfunction and help-seeking patterns in adults aged 40–80 years in the urban population of Asian countries. BJU Int 95, 609–614 (2005).
Jannini, E. A. et al. Health-related characteristics and unmet needs of men with erectile dysfunction: A survey in five European countries. J Sex Med 11, 40–50 (2014).
Ates E, Yildiz AE, Kazici HG, et al. The importance of inquiring the ejaculation function in men with premature ejaculation who do not actively seek treatment. Archivio italiano di urologia, andrologia : organo ufficiale [di] Societa italiana di ecografia urologica e nefrologica 2022. 94, 80–86.
Prieto-Castro R, Puigvert-Martinez AM, Artigas-Feliu R, et al. Opinions, attitudes, and perceptions in relation to erectile dysfunction and premature ejaculation in the undiagnosed spanish male population. Results of the PANDORA Project. J Sex Med 2020. 17, 1495–1508.
Corona, G. et al. Interplay between premature ejaculation and erectile dysfunction: A systematic review and meta-analysis. J Sex Med 12, 2291–2300 (2015).
Kamnerdsiri, W. A., Rodríguez Martinez, J. E., Fox, C. & Weiss, P. Clinical correlation between erectile function and ejaculatory function in the Czech male population. PLoS ONE 13, e0199588 (2018).
Jannini, E. A., Lombardo, F. & Lenzi, A. Correlation between ejaculatory and erectile dysfunction. Int. J. Androl. 28(Suppl 2), 40–45 (2005).
McMahon, C. G. Screening for erectile dysfunction in men with lifelong premature ejaculation: Is the Sexual Health Inventory for Men (SHIM) reliable?. J Sex Med 6, 567–573 (2009).
Kupelian, V., Link, C. L., Rosen, R. C. & McKinlay, J. B. Socioeconomic status, not race/ethnicity, contributes to variation in the prevalence of erectile dysfunction: results from the Boston Area Community Health (BACH) Survey. J Sex Med 5, 1325–1333 (2008).
Smith, J. F., Breyer, B. N. & Shindel, A. W. Predictors of sexual bother in a population of male North American medical students. J Sex Med 8, 3363–3369 (2011).
Tang, W. S. & Khoo, E. M. Prevalence and correlates of premature ejaculation in a primary care setting: A preliminary cross-sectional study. J Sex Med 8, 2071–2078 (2011).
Acknowledgements
The authors are indebted to the study participants.
Funding
This study was supported by unrestricted grants from the Jagiellonian University Medical College and Polpharma Pharmaceuticals. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. The authors’ work was independent of the funders.
Author information
Authors and Affiliations
Contributions
Conceptualization: MP MC PC. Formal analysis: MP PR. Funding acquisition: MP PC. Investigation: MP MC PR PC. Methodology: MP. Project administration: MP. Resources: MP PC. Supervision: MP. Validation: MP. Visualization: MP. Writing – original draft: MP. Writing – review & editing: MP MC PR PC.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Przydacz, M., Chlosta, M., Rajwa, P. et al. Population-level prevalence, effect on quality of life, and treatment behavior for erectile dysfunction and premature ejaculation in Poland. Sci Rep 13, 13168 (2023). https://doi.org/10.1038/s41598-023-39968-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-39968-9
This article is cited by
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
