
Abstract
The first two years of life is a critical window for good nutrition. Promoting infant and young child feeding (IYCF) practices in the first two years can help improve child survival and promote healthy growth and development. Assessment of IYCF practices is important, especially in developing countries like India where optimal IYCF practices can potentially prevent 12% of all deaths under 5 years of age, to promote awareness and intervene appropriately. The objective of our study is to generate evidence for the association between different types of mass media and appropriate IYCF practices in India, including optimal breastfeeding and appropriate complementary feeding practices. A positive association between them can point to intervention at scale. We analyzed data from India’s National Family Health Survey 5 (NFHS-5), 2019–2021. Multivariable logistic regression was used to examine the association of appropriate IYCF practices with mass media exposure. After controlling for demographics and socioeconomic status, the analyses showed that, overall, women who had exposure to television followed by newspaper and movies, had higher odds of adopting the recommended IYCF practices. The results also showed that the association of media exposure varied for different IYCF practices by geography. For instance, in the rural areas, television exposure was positively associated with all the IYCF practices, but in the urban areas, television exposure was positively associated with only early initiation of breastfeeding [OR 1.25; (95% CI 1.1–1.42)]. The study strengthens our understanding that an appropriate selection of mass media channels for intervention programs can promote IYCF practices at scale. Appropriately selecting the type of mass media to create awareness about different IYCF practices, in specific urban–rural settings, could help customize intervention programs to successfully influence IYCF behaviors.
Similar content being viewed by others

Introduction
Right food at the right time helps children grow and develop to their full potential. The first 1000 days of life, starting from the mother’s pregnancy to the child’s second birthday, is a critical window for good nutrition. Undernutrition in the first 2 years of age increases the risk of mortality, developing chronic diseases later in life, impaired cognitive development as well as diminished work capacity1,2. Globally, 45% of deaths among children under 5 years of age are linked to undernutrition, of which two thirds are attributed to sub-optimal infant and young child feeding (IYCF) practices, especially during the first year of life3,4,5. In developing countries like India, optimal IYCF practices can potentially prevent 12% of all deaths under 5 years of age4.
The World Health Organization (WHO) and the United Nations Children's Fund (UNICEF) recommendation for optimal IYCF includes breastfeeding practices like early initiation of breastfeeding within the first hour after birth (EIBF), exclusive breastfeeding (EBF) from birth to six months of age, and complementary feeding practices like timely introduction of nutritionally adequate and safe complementary foods at six months while continuing breastfeeding up to two years of age or beyond5. Promoting optimal IYCF practices can help improve child survival as well as promote healthy growth and development.
Prelacteal feeding, a common practice in India, includes giving something other than breastmilk to the newborn, such as honey or gripe water, and breastmilk substitutes like “baby formula”, during the first three days of life6,7. Feeding newborns anything other than breastmilk is highly discouraged under the global and national IYCF guidelines7,8,9. Prelacteal feeding also means that the infant is not exclusively breastfed. Moreover, prelacteal feeding can cause a delay in breastfeeding initiation as well as colostrum deprivation6,10. EIBF is important for both the mother and the child because the first breastmilk contains colostrum, which is highly nutritious and has antibodies that protect the newborn from diseases. EIBF also encourages bonding between the mother and her newborn, facilitating the production of regular breastmilk11.
Breastmilk is an uncontaminated nutritional source, which contains all the nutrients needed by children in the first six months of life. Hence, it is recommended that, for the first six months of their life, children are given nothing but breastmilk and be exclusively breastfed12,13. EBF is the foundation of optimum infant nutrition and has been found to reduce the risk of diarrheal diseases, upper respiratory tract infections and obesity in later life of the child14. Many studies have documented beneficial effects of breastfeeding on infant’s nutritional status and mortality15. Epidemiological evidence suggests that practicing both EIBF and EBF practices in combination is associated with higher reduction in mortality compared to practicing them individually16,17.
After the first six months, appropriate complementary feeding should be started for the child because breastmilk is no longer sufficient to meet the nutritional needs of an infant5. Timely introducing complementary foods like safe and nutritionally balanced solid, semi-solid or soft foods in addition to breast milk for children between 6 and 23 months, is essential for child growth and provides the foundation for good health throughout life18. Moreover, infants and young children need to be fed with minimum acceptable diet (MAD) to ensure appropriate growth and development19. According to the WHO, MAD is a combination of dietary diversity and minimum meal frequency and is different for breastfed and non-breastfed children20. We have limited our study to explore the MAD of breastfed children, which includes a variety of foods like fruits and vegetables including those rich in vitamin A, to ensure that nutrient requirements are met.
Despite the numerous benefits and advantages of appropriate IYCF practices, the prevalence of EBF, EIBF and appropriate complementary feeding in India remain low18,21. Poor IYCF practices lead to high prevalence of undernutrition like wasting and stunting19. The WHO/UNICEF emphasize the need for policies, including improvement of communication strategies, to increase awareness and uptake of, and support for IYCF practices. They also suggest that communication strategies should be appropriately selected for the target population and take their literacy levels and media access into consideration12.
Mass media
Mass media are critical in promoting health because their widespread penetration promotes broad reach to key audiences across geographic and other social boundaries, and the exposure to specific messages in the media is known to shape public knowledge, attitudes, beliefs, and behaviors22. Over the past few decades, media campaigns have been used to influence behavioral changes23,24. Creating awareness through mass media can encourage positive and discourage negative health related behaviors across populations25,26,27,28.
Literature suggests that altering the information and message environment, maximizing exposure to campaign messages, creativity of the messages and influencing the determinants of the behavior targeted in the campaign can ensure the success of mass media public health campaigns24. These factors can be extremely valuable in designing effective public health campaigns and achieving the desired goals.
To improve nutritional outcomes for children, pregnant women, and lactating mothers in India, in March 2018, the Ministry of Women and Child Development (MoWCD), Government of India launched a flagship program called the Prime Minister’s Overarching Scheme for Holistic Nourishment (POSHAN) Abhiyaan or the National Nutrition Mission29. One of the objectives of the mission is to build knowledge, attitudes, and behavioral intent about overall nutrition amongst their target populations. To achieve this, the mission is utilizing various platforms, including mass media, to create a people’s movement or Jan Andolan. The objective of our study is to generate evidence for the association between different types of mass media and appropriate IYCF practices in India, including optimal breastfeeding and appropriate complementary feeding practices, which are also the key themes of POSHAN Abhiyaan. Existing survey datasets do not capture data related to exposure specifically to IYCF messaging through mass media. Nevertheless, the inclusion of national campaigns on mass media by the MoWCD in both 2006 and 2018 can be seen as indicative of potential exposure to IYCF messaging29,30,31. Our findings can inform public health campaigns like POSHAN Abhiyaan to adjust their communication strategies to successfully achieve their goals to increase the adoption of appropriate IYCF behaviors.
Methods
Data source
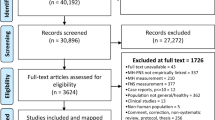
This study uses the women’s dataset from India’s National Family Health Survey (NFHS) 5, 2019–2021. The NFHS is a series of nationally representative cross-sectional surveys that provide data on a range of demographic, socioeconomic, maternal and child health outcomes; reproductive health; and family planning. NFHS-5 was conducted in two phases and gathered information from 636,699 households, 724,115 women aged 15–49 years and 101,839 men aged 15–54 years, with a response rate of 98%, 97% and 92%, respectively. Only the women who gave birth in the last 36 months were included in our analyses. The final analytical sample included 122,458 women.
Sample design
A sample design representative of the national, state/union territory and district level was adopted in each round of the survey. Every district was stratified into urban and rural areas. The rural stratums were sub-stratified based on the village population and the percentage of population belonging to the scheduled castes (SC) and scheduled tribes (ST). A sample of villages was selected as Primary Sampling Units (PSUs) within each rural sampling stratum. Prior to the PSU selection, the PSUs were sorted according to the literacy rate of women (only girls and women who were 6 years or older were included in the literacy rate calculation). Similarly, a sample of Census Enumeration Blocks (CEBs) was selected as PSUs within each urban sampling stratum. Prior to the selection of the PSUs, they were sorted according to the percentage of SC/ST population. In the second stage, twenty-two households were selected from each cluster with an equal probability systematic selection from a newly created list of households in the selected PSUs.
Outcome variables
The outcome variables in this study included the optimal IYCF practices for the women’s most recent pregnancy in the last 36 months, comprising of no prelacteal feeding, EIBF and EBF, and appropriate complementary feeding practices comprising of timely introduction of complementary foods and Minimum adequate diet (MAD) for breastfed children ages 6–23 months.
Optimal breastfeeding practices
No Prelacteal feeding Prelacteal feeding status was measured for children below 36 months of age. If a mother responded that her child was not given anything to drink other than breastmilk in the three days after the delivery, the child was categorized as “received no prelacteal feeding”.
Early initiation of breastfeeding (EIBF) EIBF was measured for children below 36 months of age. The child was categorized as to have “initiated early breastfeeding” if the child was put to the breast immediately after birth.
Exclusive breastfeeding (EBF) EBF was measured for currently breastfeeding children below six months of age. Children were categorized as “exclusively breastfed” if their mothers reported that they consumed nothing but breastmilk the previous day.
Appropriate complementary feeding practices
Timely introduction of complementary foods Timely introduction of complementary foods was measured for mothers with children between six to eight months of age. If the mother said that her child had consumed some solid, semi-solid, or soft foods the previous day, in addition to breastmilk, the child was categorized as having timely introduced complementary foods.
Minimum acceptable diet (MAD) for breastfed children ages 6–23 months MAD was measured for breastfeeding children between 6 and 23 months of age, who had received four or more food groups (i.e., solid, or semi-solid foods from at least four food groups not including the milk or milk products food group), and a minimum meal frequency, that is receiving solid or semi-solid food at least twice a day for breastfed infants 6–8 months and at least three times a day for breastfed children 9–23 months, the previous day.
Timely introduction of complementary foods and MAD for breastfed children ages 6–23 months variables were used as a proxy for appropriate complementary feeding practices.
Independent variables
Level of exposure to different types of media sources, like newspaper or magazine, radio, television, and movies at a cinema hall was measured by asking the women to indicate how often they read a newspaper or a magazine, listened to a radio, watched television, and went to a cinema hall or a theatre to see a movie. Women who responded, “at least once a week” (or “at least once a month” for movies) were considered to have “high exposure” to that media. Women who responded, “less than once a week” (“less than once a month” for movies) or “not at all” were considered to have “some exposure” and “no exposure”, respectively. Cumulative exposure to mass media was also measured by combining all four media types. Women who had “no exposure” to any type of media were categorized as having “no exposure” to any media. If they had “some exposure” or “high exposure” to one or more types of media, they were categorized as having “some/high exposure” to any media.
Covariates
Standard and commonly used questions were used to measure demographic and social factors: age of the mother, education, wealth status, caste, and religion.
Statistical analysis
Frequencies of key variables were obtained to describe the study sample. In this study, we conducted multivariable logistic regression to examine the associations between exposure to different types of media: newspaper or magazine, radio, television, and movies, and the recommended IYCF practices: no prelacteal feeding, EIBF, EBF, timely introduction of complementary foods and MAD for breastfed children ages 6–23 months. All the regression models were controlled for other media variables and the covariates. We also examined the association between cumulative mass media exposure (hereafter “any media”) and the recommended IYCF practices, controlling for the covariates. The data were analyzed and weighted using R version 4.3.1 (2023.06.16). Survey weights were included in the analysis and the survey-weighted logistic regression was performed using the R survey package. All the analyses were conducted in 2023.
Results
Descriptive characteristics
Our analysis of the NFHS-5 dataset showed that, in India, 84.6% mothers reported that their child did not receive any prelacteal feed (N = 116,908). However, only 41.7% mothers reported that their child was put to the breast immediately after birth (N = 122,458), hence initiating early breastfeeding. At the time of the survey, amongst the mothers who were currently breastfeeding their infants under six months of age, only 63.8% reported that their infant was being exclusively breastfed (N = 22,839). The rate of EBF was higher in the rural areas compared to the urban areas. Amongst the mothers who were currently breastfeeding their six to eight months old infants, only 45.9% reported timely introduction of complementary foods (N = 10,809). Rates of timely introduction of complementary foods were 8% higher in the urban areas compared to rural areas. Furthermore, merely 11% mothers reported that their 6–23 months old breastfeeding infants were being fed with a MAD (N = 53,144). (Table 1) This indicates that, apart from not giving prelacteal feed to infants, the prevalence of optimal IYCF practices is low in India, especially in rural India.
In terms of mass media exposure, 11.1%, 3.3%, 48.5% and 8.8% mothers reported having high exposure to newspaper or magazine, radio, television, and movies, respectively. (Table 1) However, a notable 22.5% of mothers reported no exposure to any type of mass media. This lack of media exposure was even more pronounced in rural areas, where 29% of mothers had no media exposure, while in urban areas, only 8.8% of mothers lacked any media exposure. Evidently, in India, penetration of all four forms of mass media is higher in urban areas compared to rural areas, and television penetration and reach are broad compared to other forms of mass media25.
Mass media and no prelacteal feeding
After adjusting for other media variables and covariates, our study found that, overall, women who had some newspaper or magazine exposure (Odds Ratio (OR) 0.91; 95% Confidence Interval (CI) 0.85–0.97) were associated with lower odds of not giving prelacteal feed to their infants compared to women who had no newspaper or magazine exposure. In contrast, women who had high television exposure (OR 1.13; 95% CI 1.06–1.21) and high movies exposure (OR 1.11; 95% CI 1.02–1.22) were associated with higher odds of not giving prelacteal feed to their infant compared to women who had no exposure to these TV and movies. After adjusting for the covariates, women who had some/high exposure to any media (OR 1.1; 95% CI 1.04–1.17) were associated with higher odds of not giving prelacteal feed to their infant compared to women who had no exposure to any media (Fig. 1).

Association between different types of mass media and optimal breastfeeding practices. The ORs are mutually adjusted for other media exposure variables as well as the covariates: age, educational attainment, wealth, caste and religion. The ORs for any media are adjusted for the covariates. (Sample sizes: No prelacteal feeding = 116,908, Early Initiation of Breastfeeding = 122,458, Exclusive Breastfeeding = 22,839).
In the rural areas, women who had some newspaper or magazine exposure (OR 0.89; 95% CI 0.83–0.96) were associated with lower odds of not giving prelacteal feed to their infants, and women who had high television exposure (OR 1.17; 95% CI 1.09–1.26) or some/high exposure to any media (OR 1.1; 95% CI 1.03–1.17) were associated with higher odds of not giving prelacteal feed to their infants compared to women who had no exposure to these media types. In the urban areas, women who had high movies exposure (OR 1.24; 95% CI 1.07–1.43) were associated with higher odds of not giving prelacteal feed to their infants compared to women who had no exposure to these media types.
Mass media and early initiation of breastfeeding
After adjusting for other media variables and covariates, overall, women who had some newspaper or magazine exposure (OR 0.92; 95% CI 0.87–0.96) were associated with lower odds of EIBF compared to women who had no newspaper or magazine exposure. Women who had high newspaper or magazine exposure (OR 1.14; 95% CI 1.07–1.22), some television exposure (OR 1.08; 95% CI 1.03–1.14) and high television exposure (OR 1.47; 95% CI 1.4–1.55) were associated with higher odds of EIBF compared to women who had no exposure to these media types. After adjusting for the covariates, women who had some/high any media exposure (OR 1.28; 95% CI 1.22–1.34) were associated with higher odds of EIBF compared to women who had no exposure to any media (Fig. 1).
In the rural areas, women who had some newspaper or magazine exposure (OR 0.9; 95% CI 0.85–0.95) and some radio exposure (OR 0.91; 95% CI 0.83–0.99) were associated with lower odds of EIBF compared to women who had no exposure to these media types. Women who had some (OR 1.07; 95% CI 1.01–1.13) and high television exposure (OR 1.55; 95% CI 1.47–1.64) were associated with higher odds of EIBF compared to no television exposure. Moreover, women who had some/high any media exposure (OR 1.28; 95% CI 1.22–1.34) were associated with higher odds of EIBF compared to women who had no exposure to any media. In the urban areas, women who had high radio exposure (OR 1.24; 95% CI 1.04–1.48), high television exposure (OR 1.25; 95% CI 1.1–1.42) and some/high any media exposure (OR 1.23; 95% CI 1.07–1.4) were associated with higher odds of EIBF compared to women who had no exposure to these media types.
Mass media and exclusive breastfeeding
After adjusting for other media variables and covariates, overall, women who had high television exposure (OR 1.14; 95% CI 1.03–1.26) were associated with higher odds of EBF compared to women who had no television exposure. After adjusting for the covariates, women who had some/high any media exposure (OR 1.11; 95% CI 1.01–1.22) were associated with higher odds of EBF compared to women who had no exposure to any media. (Fig. 1).
In the rural areas of India, women who had high television exposure (OR 1.21; 95% CI 1.08–1.35) and some/high any media exposure (OR 1.12; 95% CI 1.01–1.24) were associated with higher odds of EBF compared to women who had no exposure to these media types.
Mass media and timely introduction of complementary foods
After adjusting for other media variables and covariates, overall, women who had high television exposure (OR 1.54; 95% CI 1.33–1.78) were associated with higher odds of timely introducing complementary foods compared to women who had no television exposure. After adjusting for the covariates, women who had some/high any media exposure (OR 1.36; 95% CI 1.18–1.55) were associated with higher odds of timely introducing complementary foods compared to women who had no exposure to any media. (Fig. 2).

Association between different types of mass media and appropriate complementary feeding practices. The ORs are mutually adjusted for other media exposure variables as well as age, educational attainment, wealth, caste and religion. The ORs for any media are adjusted for the covariates. (Sample sizes: Complementary feeding = 10,809, Breastfeeding with MAD = 53,144).
In the rural areas, women who had some television exposure (OR 1.19; 95% CI 1.01–1.4) and high television exposure (OR 1.61; 95% CI 1.38–1.88) were associated with higher odds of timely introducing complementary foods compared to women who had no television exposure. Women who had some/high any media exposure (OR 1.39; 95% CI 1.2–1.6) were associated with higher odds of timely introducing complementary foods compared to women who had no exposure to any media.
Mass media and MAD for breastfed children ages 6–23 months
After adjusting for other media variables and covariates, our study also found that, overall, women who had some newspaper or magazine exposure (OR 1.19; 95% CI 1.06–1.32) and high television exposure (OR 1.19; 95% CI 1.07–1.33) were associated with higher odds of MAD for breastfed children ages 6–23 months compared to women who had no exposure to these media types. After adjusting for the covariates, women who had some/high any media exposure (OR 1.17; 95% CI 1.05–1.3) were associated with higher odds of MAD for breastfed children ages 6–23 months compared to women who had no exposure to any media.
In the rural areas, women who had some newspaper or magazine exposure (OR 1.15; 95% CI 1.02–1.3), high television exposure (OR 1.2; 95% CI 1.07–1.35) and some/high any media exposure (OR 1.17; 95% CI 1.05–1.31) were associated with higher odds of MAD for breastfed children ages 6–23 months compared to women who had no exposure to these media types. In the urban areas, women who had some newspaper or magazine exposure (OR 1.27; 95% CI 1.01–1.6) were associated with higher odds of MAD for breastfed children ages 6–23 months compared to women who had no newspaper or magazine exposure.
Discussion
Mass media are effective means of communicating health messages because of their potential to reach large audiences across boundaries, especially through underserved rural areas23,32. Routine exposure to mass media can shape public knowledge, attitudes, beliefs, and behaviors and encourage healthy behavioral changes22. The use of mass media campaigns for health promotion and disease prevention have resulted in mixed evidence for success23. However, campaigns aimed towards increasing the adoption of IYCF practices have been successful33,34. The descriptive characteristics of our study established the popularity of different types of mass media amongst our target population, which indicates that television has the maximum penetration followed by newspaper and magazines. Television and cinema have their own advantages when it comes to creating health awareness. Audio-visual media can deliver messages to the target audience without a literacy or geographic barriers. However, accessibility of television allows for a much wider reach compared to cinema. Understandably, mass media, especially television, have been a crucial channel for health intervention programs to disseminate nutrition information in India29,35.
In recent decades, many efforts have gone towards improving the rate of IYCF practices in India. The Food Nutrition Board, Ministry of Women and Child Development (MoWCD), Government of India (GoI), developed the National Guidelines on IYCF in 2004 and updated them in 2006, to reach the national goals for the optimal IYCF practices35. These guidelines were developed in congruence with the WHO/UNICEF Global Strategy on IYCF36. Under these guidelines, mass media were used to create a climate of nutritional awareness in the country by launching special programs on IYCF37. Between 2004 and 2006, advertising campaigns on nutritional issues, like IYCF, were released in different regional languages, including 27 video films telecasted by Doordarshan (an Indian public service broadcaster and one of the largest broadcasting organizations), a 30-episode radio program and, posters and charts30. In 2013, the Ministry of Health and Family Welfare (MoHFW), GoI also created an operational guideline to guide the interventions on optimal IYCF practices, and further enhance these practices in India38. In 2016, the MoWCD launched a program to support breastfeeding called the Mother’s Absolute affection or MAA, where the focus was on the importance of the first 1000 days, thereby recognizing the importance of improving IYCF practices35. The program’s objectives include generation of breastfeeding awareness to facilitate higher breastfeeding rates in the country. To achieve maximum penetration of breastfeeding messages, the program used mass media, such as print, electronic and audio-visual platforms, amongst other communication channels like interpersonal communication. Most recently, POSHAN Abhiyaan or the National Nutrition Mission was launched in 2018 by MoWCD, GoI. This mission aims to improve nutritional outcomes and build knowledge, attitudes, and behavioral intent about overall nutrition, including optimal IYCF practices, amongst their target populations through a Jan Andolan or mass movement by utilizing platforms like mass media. In our study, we observed a positive association between exposure to at least one of the four mass media sources and all five IYCF practices in rural areas and EIBF in urban areas. This suggests that mass media exposure has the potential to encourage mothers to adopt healthy IYCF practices, especially in rural areas.
Over 66% of women in India have no exposure to newspapers or magazines, 22% women have had no schooling and 28% of women are not literate39. These numbers are even higher in the rural areas. In our study, nationally and in rural areas, high newspaper or magazines exposure was associated with EIBF. Some newspaper or magazines exposure was associated with providing MAD to breastfeeding children between 6 and 23 months in both rural and urban areas. However, newspaper or magazine exposure was not associated or was negatively associated with other IYCF practices. This suggests that while disseminating information via print media has the potential to influence mothers to practice appropriate IYCF, it has limitations in terms of reach since it excludes audiences with low literacy levels. Using visual aids to disseminate information via print media may allow women to overcome the literacy barrier and access more information through print media40.
Previous studies have found radio exposure to be associated with higher rates of EIBF21. In our study, high radio exposure was positively associated with EIBF in the urban areas. As per NFHS-5 data, more women in urban areas listen to the radio than in the rural areas39. Our findings suggest that radio could be a good medium to create awareness about IYCF practices, especially when targeted to urban areas (Fig. 3).

Overview of the associations between different types of mass media and appropriate IYCF practices. The associations are mutually adjusted for other media exposure variables as well as age, educational attainment, wealth, caste and religion. The associations for any media are adjusted for age, educational attainment, wealth, caste and religion. [*p < 0.05. **p < 0.01. ***p < 0.001].
In a developing country like India, where percentage of illiteracy is high, television has a major role to play. Television is an equalizer in the context of health communication because it does not differentiate between audiences based on literacy. Moreover, the ubiquity of television exposure amongst our target population makes it an excellent medium to communicate health information. In our study, we found that even though more women in urban areas have exposure to television, television exposure was positively associated with all five IYCF practices in rural areas. Women in the rural areas of India have lower literacy levels compared to urban areas, likely due to limited access to schools and resources41. This suggests that disseminating messages to increase awareness about the benefits of IYCF practices via television could positively impact IYCF behaviors, especially among audiences with limited privileges. According to prior studies, when television is used as a medium to create knowledge, knowledge gaps resulting from the communication flow of messages are less likely to occur42. Our study suggests that using television as a medium to create awareness about IYCF practices, especially in the rural areas, could successfully promote the recommended IYCF behaviors. These findings complement our previous study that documents the effect of television on promoting maternal healthcare utilization in India25.
Our study also found significant associations between high movies exposure and no prelacteal feeding- nationally and in urban areas. As per NFHS-5 data, more women in urban areas than in the rural areas went to see movies in a cinema hall. This could be attributed to easier access to cinema halls in the urban areas43. Our findings suggest that messages disseminated via the cinema halls through advertisements, public service announcements or movies could create awareness about these practices, especially when targeted to the urban populations (Fig. 3).
Even though the penetration of mass media is higher in the urban areas, mass media exposure was associated with only a few optimal IYCF practices with no clear trend. Studies have found that the impact of mass media is greater among mothers in rural areas who have lower levels of education and other privileges44. Mothers with formal education have more knowledge about health, nutrition, and have a care-seeking behavior, which promotes the use of modern health services45. Moreover, the urban population could have better access to health-related information from other media sources, such as social media, as a higher proportion of women in urban areas than in rural areas have access to mobile phones and use the internet39. Hence, for them, mass media may not play a significant role in increasing awareness about maternal and child health practices.
According to the integrated theory of behavioral prediction, there are many factors that can impact the success of a mass media campaigns and lead to the desired health outcomes. For instance, an understanding of the determinants that can influence a health behavior is critical for the design and strategy of the campaign24. Campaigns will be most effective in influencing the human behavior by customizing health messages to influence the determinants leading to that behavior28. For instance, mass media campaigns have been found to increase the rate of EBF by promoting benefits of EBF in the first six months, highlighting the risks of giving water and other breastmilk substitutes, and also promoting positive social norms related to the practice34. Some authors also suggest that mass media alone may not be effective in influencing a behavior change and that combining mass media interventions with interpersonal counselling might be more conducive to positively influence IYCF behaviors34,46. Therefore, there could be additional barriers that need to be addressed to initiate a large change in social norms or cultural habits and improve the rate of recommended IYCF practices in India. Designing effective public health campaigns and combining mass media campaigns with additional interventions may improve the likelihood of success in future efforts to promote IYCF practices. Media campaigns, in complement with other strategic interventions at multiple levels may also reduce communication inequalities and promote healthy behavior changes47,48.
Our study is not without limitations. First, the cross-sectional design of the data prevents us from making causal inferences on the relationship between our exposure and outcome variables. However, the strong associations between media exposure and IYCF practices suggests the potential promise of media in promotion of appropriate IYCF practices. Second, NFHS data are self-reported. Thus, mothers who might be aware of the appropriate IYCF practices but did not practice them could have falsely reported their IYCF behaviors, leading to social desirability bias49. The self-reported nature of the data also makes our study susceptible to recall bias. Therefore, to minimize recall bias, we limited the age of the children while calculating the IYCF indicators. Finally, the NFHS-5 survey did not document frequency of mass media exposure through internet, social media, and mobile phones. Future surveys should also include information regarding internet, social media and mobile use and their implications on health-related behaviors. And future studies should examine the associations between these types of media and IYCF practices in India. NFHS-5 provides no information about the type of IYCF-related media content women in India are exposed to, thus, one can only speculate based on literature. Future studies should examine IYCF content (or lack thereof) in the media to obtain a complete picture of the kind of information encouraging (or not influencing) such behaviors.
Conclusion
This study strengthens our understanding of the associations between different types of mass media and the optimal IYCF practices in India and provides evidence that mass media may promote healthy IYCF behaviors. Appropriately selecting the type of mass media to create awareness about different IYCF practices, in specific urban–rural settings, could help customize intervention programs to successfully influence IYCF behaviors. However, additional interventions like overcoming literacy barriers, interpersonal counselling and policy support may also be required to initiate large changes in social norms and cultural habits associated with some of these practices.
Data availability
The dataset supporting the conclusions of this article is available in the Demographic and Health Surveys Program repository (https://dhsprogram.com).
References
Jones, A. D. et al. World Health Organization infant and young child feeding indicators and their associations with child anthropometry: A synthesis of recent findings. Matern. Child Nutr. 10, 1–17 (2014).
Dewey, K. G. & Begum, K. Long-term consequences of stunting in early life. Matern. Child Nutr. 7(Suppl 3), 5–18 (2011).
Black, R. E. et al. Maternal and child undernutrition: Global and regional exposures and health consequences. Lancet 371, 243–260 (2008).
Black, R. E. et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 382, 427–451 (2013).
Infant and Young Child Feeding. https://www.who.int/news-room/fact-sheets/detail/infant-and-young-child-feeding
Das, A. et al. Prelacteal feeding practice and maintenance of exclusive breast feeding in Bihar, India—Identifying key demographic sections for childhood nutrition interventions: A cross-sectional study. Gates Open Res. 3, 1 (2019).
Roy, M. P., Mohan, U., Singh, S. K., Singh, V. K. & Srivastava, A. K. Determinants of prelacteal feeding in rural northern India. Int. J. Prev. Med. 5, 658–663 (2014).
UNICEF. From the First Hour of Life: Making the Case for Improved Infant and Young Child Feeding Everywhere.
Operational Guidelines on Infant and Young Child Feeding Ministry of Women And Child Development Government of India.
Amele, E. A., Demissie, B. W., Desta, K. W. & Woldemariam, E. B. Prelacteal feeding practice and its associated factors among mothers of children age less than 24 months old in Southern Ethiopia. Ital. J. Pediatrics https://doi.org/10.1186/s13052-019-0604-3 (2019).
Leung, A. K., Sauve, R. S. & Calgory, F. Breast is best for babies (2005).
World Health Organization (WHO) & UNICEF. Global nutrition targets 2025: Breastfeeding policy brief. https://apps.who.int/iris/bitstream/handle/10665/149022/WHO_NMH_NHD_14.7_eng.pdf (2014).
Yadav, J., Shekhar, C. & Bharati, K. Variation and determinants of early initiation of breastfeeding in high and low neonatal mortality settings in India. J. Biosoc. Sci. https://doi.org/10.1017/S0021932021000092 (2021).
Ogbo, F. A. et al. Regional prevalence and determinants of exclusive breastfeeding in India. Int. Breastfeed. J. 14, 1–12 (2019).
Meshram, I. I. et al. Infant and young child feeding practices, sociodemographic factors and their association with nutritional status of children aged <3 years in India: Findings of the National Nutrition Monitoring Bureau survey, 2011–2012. Public Health Nutr. 22, 104–114 (2019).
Edmond, K. M. et al. Delayed breastfeeding initiation increases risk of neonatal mortality. Pediatrics https://doi.org/10.1542/peds.2005-1496 (2006).
Mullany, L. C. et al. Breast-feeding patterns, time to initiation, and mortality risk among newborns in Southern Nepal. J. Nutr. 138, 599 (2008).
Dhami, M. V., Ogbo, F. A., Osuagwu, U. L. & Agho, K. E. Prevalence and factors associated with complementary feeding practices among children aged 6–23 months in India: A regional analysis. BMC Public Health 19, 1034 (2019).
Torlesse, H. & Raju, D. Feeding of Infants and Young Children in South Asia (2018).
Indicators for assessing infant and young child feeding practices: Part 1 Definitions|UNHCR US. https://www.unhcr.org/us/media/indicators-assessing-infant-and-young-child-feeding-practices-part-1-definitions
Dibley, M. J. et al. Across-country comparisons of selected infant and young child feeding indicators and associated factors in four south Asian countries. Food Nutr. Bull. 31, 366–379 (2010).
Viswanath, K., Ramanadhan, S. & Kontos, E. Z. Mass Media. in Macrosocial Determinants of Population Health 275–294 (Springer New York, 2007). https://doi.org/10.1007/978-0-387-70812-6_13.
Wakefield, M. A., Loken, B. & Hornik, R. C. Use of mass media campaigns to change health behaviour. Lancet 376, 1261–1271 (2010).
Randolph, W. & Viswanath, K. Lessons learned from public health mass media campaigns: Marketing health in a crowded media world. Annu. Rev. Public Health 25, 419–437 (2004).
Dhawan, D., Pinnamaneni, R., Bekalu, M. & Viswanath, K. Association between different types of mass media and antenatal care visits in India: A cross-sectional study from the National Family Health Survey (2015–2016). BMJ Open 10, 42839 (2020).
Viswanath, K. et al. Individual and social determinants of COVID-19 vaccine uptake. BMC Public Health 21, 818 (2021).
Bekalu, M. A., Dhawan, D., McCloud, R., Pinnamaneni, R. & Viswanath, K. Adherence to COVID-19 mitigation measures among American adults: The need for consistent and unified messaging. Health Educ. Res. https://doi.org/10.1093/her/cyab002 (2021).
Dhawan, D., Bekalu, M., Pinnamaneni, R., Mccloud, R. & Viswanath, K. COVID-19 news and misinformation: Do they matter for public health prevention?. J Health Commun. 26, 799–808 (2021).
JAN ANDOLAN-Guidelines. https://icds-wcd.nic.in/nnm/NNM-Web-Contents/LEFT-MENU/Guidelines/JanAndolanGuidelines-English.pdf
Ministry of Women and Child Development, G. of I. Highlights of Nutrition Initiatives of FNB and MWCD during the last two years in the context of achieving Food and Nutrition Security in the country. http://motherchildnutrition.org/india/pdf/mcn-highlights-of-nutrition-initiatives.pdf (2006).
Malhotra, N. Inadequate feeding of infant and young children in India: Lack of nutritional information or food affordability?. Public Health Nutr. 16, 1723–1731 (2013).
Unite for sight. Health communication course: Module 5—The role of media in health promotion. Unite for Sight https://www.uniteforsight.org/health-communication-course/module5 (2010).
Bhutta, Z. A. et al. What works? Interventions for maternal and child undernutrition and survival. Lancet 371, 417–440 (2008).
Nguyen, P. H. et al. Exposure to mass media and interpersonal counseling has additive effects on exclusive breastfeeding and its psychosocial determinants among Vietnamese mothers. Matern. Child Nutr. https://doi.org/10.1111/mcn.12330 (2016).
Ministry of Health and Family Welfare. Ministry of Health and Family Welfare Government of India Programme for Promotion of Breastfeeding (2016).
Avula, R., Oddo, V. M., Kadiyala, S. & Menon, P. Scaling-up interventions to improve infant and young child feeding in India: What will it take?. Matern. Child Nutr. 13, e12414 (2017).
Ministry of Women and Child Development Food and Nutrition Board, G. of I. Indian National Guidelines on Infant and Young Child Feeding. Government of India (2004).
India Ministry of Health and Family Welfare (MoHFW). Guidelines for enhancing optimal infant and young child feeding practices (2013).
International Institute for Population Sciences. National Family Health Survey—5 (NFHS-5) 2019–21. International Institute for Population Sciences (2021).
Visual Communication Resources|Health Literacy|CDC. https://www.cdc.gov/healthliteracy/developmaterials/visual-communication.html
Ministry of Statistics and Program Implementation; Government of India. Education in India (2014).
Viswanath, K. & Finnegan, J. R. The knowledge gap hypothesis: Twenty-five years later. Ann. Int. Commun. Assoc. 19, 187–228 (1996).
‘Rural India largely excluded from Indian cinema’|Business Standard News. https://www.business-standard.com/article/news-ians/rural-india-largely-excluded-from-indian-cinema-118053000363_1.html
Fatema, K. & Lariscy, J. T. Mass media exposure and maternal healthcare utilization in South Asia. SSM Popul. Health 11, 100614 (2020).
Paul, S., Paul, S., Gupta, A. K. & James, K. S. Maternal education, health care system and child health: Evidence from India. Soc. Sci. Med. 296, 114740 (2022).
Graziose, M. M., Downs, S. M., Obrien, Q. & Fanzo, J. Systematic review of the design, implementation and effectiveness of mass media and nutrition education interventions for infant and young child feeding. Public Health Nutr. https://doi.org/10.1017/S1368980017002786 (2017).
Viswanath, K., McCloud, R. F. & Bekalu, M. A. Communication, health, and equity: Structural influences. In Routledge Handbook of Health Communication (eds Thompson, T. L. & Harrington, N. G.) 426–440 (Routledge, 2022).
Viswanath, K., Finnegan, J. & Gollust, S. Communication and health behavior in a changing media environment. In Health Behavior: Theory, Research, and Practice (eds Glanz, K. et al.) (Jossey-Bass, 2015).
Phillips, D. L. & Clancy, K. J. Some effects of “social desirability” in survey studies. Am. J. Sociol. 77, 921–940 (1972).
Acknowledgements
This research was supported by fundings from the Bill & Melinda Gates Foundation (Viswanath, PI), grant numbers INV-005090 and INV-009885. We are grateful for their financial support, which made this study possible. The funders had no role in the study design; in the collection, analysis, and interpretation of the data; in the writing of the report; and in the decision to submit the paper for publication.
Author information
Authors and Affiliations
Contributions
D.D. and K.V. conceived and designed the study. R.P. contributed to the design of the study. D.D. analyzed and interpreted the data and wrote the first draft of the manuscript. D.D., R.P., and K.V. contributed to the interpretation of the data and revised the manuscript for important intellectual content. All authors provided critical feedback on the manuscript and agree to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Dhawan, D., Pinnamaneni, R. & Viswanath, K. Association between mass media exposure and infant and young child feeding practices in India: a cross-sectional study. Sci Rep 13, 19353 (2023). https://doi.org/10.1038/s41598-023-46734-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-46734-4
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
