
Abstract
Evidence on the harms and benefits of social media use is mixed, in part because the effects of social media on well-being depend on a variety of individual difference moderators. Here, we explored potential neural moderators of the link between time spent on social media and subsequent negative affect. We specifically focused on the strength of correlation among brain regions within the frontoparietal system, previously associated with the top-down cognitive control of attention and emotion. Participants (N = 54) underwent a resting state functional magnetic resonance imaging scan. Participants then completed 28 days of ecological momentary assessment and answered questions about social media use and negative affect, twice a day. Participants who spent more than their typical amount of time on social media since the previous time point reported feeling more negative at the present moment. This within-person temporal association between social media use and negative affect was mainly driven by individuals with lower resting state functional connectivity within the frontoparietal system. By contrast, time spent on social media did not predict subsequent affect for individuals with higher frontoparietal functional connectivity. Our results highlight the moderating role of individual functional neural connectivity in the relationship between social media and affect.
Similar content being viewed by others

Introduction
Over 4.5 billion people around the world use social media, with the average daily user engaging in 2.5 h in 20221. The wild popularity and proliferation of social media have prompted scientific investigation into potential effects of social media use on health2. One insight we have gained from the past decade of research is that the question of how social media relate to well-being does not have a single answer. Social media influence people differently, because different people engage with social media contents differently3. Consistent with this view, emerging evidence highlights that the relationship between social media and well-being is inconsistent4,5,6,7. For example, a recent large-scale meta-analysis of 226 studies showed that although social media use was associated with small improvement in social well-being, the benefit also came at the cost of increased negative emotions such as depression and anxiety8. Furthermore, some of these effects varied according to a range of moderators, suggesting that the effects of social media may depend on a number of factors that vary across the individual, platform, context, and more5. Various candidate moderators have been examined, including demographics, personality traits, types of social media use, and media content8. However, little is known as to whether individual differences in intrinsic functional neural architectures may moderate different links between social media use and symptoms of psychopathology or well-being.
Individual differences in the brain systems that support cognitive control, in general, including over one’s emotions, may be a key moderator for the relationship between social media use and affective outcomes. Neurocognitive control circuits support attention to different stimuli9 and may guide whether and to which aspects of social media contents one attends, as well as the interpretation and re-interpretation of perceived contents10. Resting state functional connectivity, or the synchronous activity between different regions of the brain at rest, offers one way to observe the function of circuits that underlie cognitive control11. In particular, the frontoparietal system has been implicated in cognitive control of affective processes12,13,14 in individuals with15 and without psychopathology16. The frontoparietal system is composed of dorsolateral prefrontal cortex and posterior parietal cortex9 and is extensively interconnected with other systems, such as default mode and attention systems17, that support distinct and competing psychological processes underlying the regulation of social and affective experiences18,19.
In support of the frontoparietal systems’ connection to emotion outcomes, problematic negative emotions have been associated with disrupted resting state functional connectivity within brain systems involved in emotion regulation20,21. Specifically, differences in frontoparietal connectivity, including both the hypo- and hyper-connectivity, have been implicated in increased negative affect (vs. other types of emotion more generally) and are a widespread feature of virtually every major mood disorder22. Differences in the frontoparietal system, such as hypoconnectivity between its constituent regions22,23, have been linked to difficulty regulating responses to emotionally salient information, resulting in emotion dysregulation24.
More specifically, how may the functional connectivity within the frontoparietal system relate to the ways people experience social media? By design, social media platforms are replete with information that may affect emotion. Some include potential sources of positive affect such as faces and personal narratives of close others25. However, social media can increase a risk of harm to one’s overall mental health26 (United States) by increasing negative affect via multiple mechanisms, for example, by serving as a source of negative news contents27, online aggression28, and other social information that could negatively impact well-being for certain individuals (e.g., individuals who are prone to social comparison29). When exposed to emotionally salient information on social media, weaker connectivity among the nodes of the frontoparietal system may signal a reduced ability to regulate affective responses, for example by diverting attention from negative contents or (re)interpreting content in adaptive ways10, potentially increasing negative affect following social media engagement.
Compared to the robust link between disrupted frontoparietal functional connectivity and psychopathology22,23, the role of resting state frontoparietal functional connectivity in negative affect among non-clinical populations—which may comprise a large portion of the social media users—is less clear15. Studies examining how functional connectivity within neural structures relates to the affective experience and difficulties in regulating negative emotions in non-clinical populations could elucidate how complex social stimuli, such as social media contents, may relate to people’s everyday affective experience and well-being more broadly. Examining how frontoparietal connectivity relates to people’s day-to-day affective outcomes can also help test ideas about psychological processes involved in social media effects that might not be accessible via self-reports alone.
The current study examined potential neural moderators of the within-person temporal link between time spent on social media and subsequent affect. We assessed resting state intrinsic connectivity within the frontoparietal system because this system is implicated in the cognitive control of emotion. We specifically focused on negative affect outcomes following social media use, based on previous evidence on potential harms of social media on mental health26, as well as the role of frontoparietal functional connectivity in negative affect regulation22. We first tested whether lower frontoparietal connectivity would be associated with greater self-reported negative emotions (i.e., depression and anxiety) and difficulties in emotion regulation. Next, using an intensive, longitudinal ecological momentary assessment (EMA) design, we examined the within-person temporal relationship between the amount of time spent on social media and subsequent negative affect. We further explored whether the link between social media use and subsequent negative affect would be moderated by individual differences in resting state frontoparietal functional connectivity. We hypothesized that lower frontoparietal connectivity would be associated with a stronger link between social media use and subsequent negative affect.
Methods
Data, code, and protocol availability
Data and analysis scripts are available at https://github.com/cnlab/social_media_brain/. The current study reports a subset of data from a parent study, and the methodological details on participant recruitment, data collection, and functional magnetic resonance imaging (fMRI) data preprocessing have also been described in the study protocol paper30 and a study that examined alcohol use behavior31 that is not the focus of the current report.
Participants and procedure
This multisite study recruited students attending two urban universities in the United States of America who belonged to different campus groups at the time of recruitment. Based on the initial online survey responses, 111 participants who met the fMRI eligibility criteria visited the laboratories, completed surveys that assessed their baseline levels of depression and anxiety, completed an fMRI visit, and had usable data. All participants who completed fMRI were invited to an initial round of EMA that did not contain any social media use questions, and hence was not the focus of the current report. About nine months (mean = 307.8 days; median = 280 days; SD = 135.75; range = 85–533) after the fMRI scan, at the start of the coronavirus (COVID-19) pandemic, all participants were once again invited to complete another round of 28-day EMA that included both the social media use and affect measures relevant to the current investigation. In this round, 54 of the participants who completed the baseline fMRI also finished the EMA portion of the study with usable data (Mage = 20.35 years; SDage = 1.32; 37 women, 16 men, 1 indicated to be “Other” gender; 26 White, 16 Asian, 2 Black, 3 Latino/a, and 7 Multiracial).
Eligibility criteria for the fMRI visit included standard MRI eligibility criteria (no metal in body, not claustrophobic, not pregnant/nursing, and weighs less than 350 lb due to the scanner weight limit), older than 18 years of age, fluent in English, not currently studying abroad, and having no history of serious medical history, psychiatric hospitalization, or substance abuse. Exclusion criteria as part of a parent study that are unrelated to the current report included having never had alcohol or consuming less than one drink in a typical drinking occasion, and not having at least two friends who drink alcohol, one more than the self and the other less than the self. This study was approved by the University of Pennsylvania Institutional Review Board and the Army Research Office’s Human Research Protection Office. All experiments were performed in accordance with the Declaration of Helsinki and with relevant guidelines/regulations. All participants provided informed consent and were paid for their participation. Online surveys were conducted via Qualtrics, scanner tasks were presented using PsychoPy232, and the EMA prompts and participants’ responses were delivered via the LiveData app (www.lifedatacorp.com).
Resting state fMRI
Data acquisition and preprocessing
Resting-state fMRI (rs-fMRI) and structural images were acquired using 3 Tesla Siemens Prismas with 64-channel head coils at the University of Pennsylvania Center for Functional Neuroimaging and at the Mortimer B. Zuckerman Mind Brain Behavior Institute at Columbia University. The acquisition protocols were identical across sites. For the resting state scan, we collected 300 continuous echo-planar imaging (EPI) functional volumes with the following parameters: voxel size = 3 × 3 × 3 mm; 42 slices; field of view (FOV) = 210 mm; time repetition (TR) = 1000 ms; time echo (TE) = 30 ms; multiband acceleration factor (MBAF) = 3; flip angle = 62. During the resting state scan, participants were instructed to keep their eyes open and focus on a fixation cross for 5 min. A MPRAGE anatomical scan was also collected using the following sequence: voxel size = 0.9 × 0.9 × 1.0 mm; 160 slices; FOV = 240 mm; TR = 1850 ms; TE = 3.91 ms; flip angle = 8. The neuroimaging data were preprocessed using fMRIPrep (Version 20.0.6)33 based on Nipype 1.4.234,35. Please see Supplemental Information 1 [SI1] for details of the structural image preprocessing.
The rs-fMRI were preprocessed with the following steps: (1) slice time correction with AFNI 2016020736 and (2) motion correction using rigid body translation and rotation with FSL 5.0.937. The functional and structural images were aligned using Freesurfer. We calculated various confounds (e.g., framewise displacement [FD], DVARS, global signal) for each TR. Across the 300 total volumes of the participants included in the current study, the average FD was 0.13 mm (SD = 0.05), the average standardized DVARS was 1.24 (SD = 0.09), and on average, 0.2% (SD = 0.25) of the scans showed spikes across 300 volumes. We further denoised resting-state data using the XCP Engine pipeline (Version 1.0)38. Specifically, the following motion-related confounds were removed from BOLD sequences: (1) de-meaning and detrending, (2) de-spiking using AFNI’s 3dDespike utility, (3) bandpass filtering (0.01–0.08 Hz), (4) 36-parameter confound regression including 6 realignment parameters, mean signal in white-matter, cerebrospinal fluid, and mean global signal, as well as the first power and quadratic expansions of their temporal derivatives. Please see [SI1] for additional information on the preprocessing and [SI2] for more details and effectiveness of our motion correction.
Frontoparietal functional connectivity
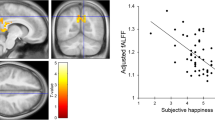
The frontoparietal system was defined based on a previously established functional brain parcellation from the Power 264 atlas39, which provides a coarse resolution of brain networks. We selected 25 regions or nodes that were defined by 5 mm diameter spheres around the center coordinate (Fig. 1, [SI3] for MNI coordinates), that represent the frontoparietal system. We extracted BOLD time series of each node and calculated within-person Pearson’s correlation coefficients between every pair of node time courses. We applied a Fisher z-transform to the correlation coefficients within each participant, on a per-participant basis, and focused on positive coefficients given the ambiguity of interpreting negative edges due to regression of the global signal during preprocessing of the rs-fMRI data40,41,42. Available correlation coefficients from edges between 25 nodes within the frontoparietal system were then averaged to indicate a summary index of average frontoparietal functional connectivity per participant. To explore additional levels of granularity, we also examined functional connectivity within subregions of the frontoparietal system to further understand which specific subsystems43 were responsible for the hypothesized results [SI4]. In addition, as control measures, we repeated main analyses using functional connectivity within the visual and auditory systems [SI5]. Results from intraclass correlation coefficient (ICC) analyses indicated moderate reliability across the whole brain (ICC = 0.56) and within the frontoparietal system (ICC = 0.52).

Frontoparietal nodes. The frontoparietal system consisted of 25 frontoparietal nodes defined by Power et al., 2011, with 5 mm diameter spheres around the center coordinate.
Positionality statement
Mindful that our identities can influence our approach to science, the authors wish to provide the reader with information about our backgrounds. With respect to gender, when the manuscript was drafted, seven authors self-identified as women, four as men, and two as non-binary. With respect to race, nine authors self-identified as White, three as Asian, and one as Black. None of the authors are current college students (i.e., the main population sampled).
Citation diversity statement
Recent work in several fields has identified a bias in citation practices such that papers from women and other minority scholars are under-cited relative to the number of such papers in the field44,45. Here we sought to consider choosing references that reflect the diversity of the field in thought, form of contribution, gender, and other factors. We obtained the predicted gender of the first and last author of each reference by using databases that store the probability of a first name being carried by a woman46. By this measure, our references contain 25.18% woman(first)/woman(last), 8.87% man/woman, 25.58% woman/man, and 40.38% man/man. This method is limited in that a) names, pronouns, and social media profiles used to construct the databases may not, in every case, be indicative of gender identity and b) it cannot account for intersex, non-binary, or transgender people.
Measures
Ecological momentary assessment surveys
Throughout the 28-day EMA period, participants received two surveys per day via mobile app in the morning (8AM) and evening (6PM) that assessed their social media use and current affect, described below.
Time spent on social media
Participants retroactively reported how much time they spent on social media since the last survey. Participants self-determined what they meant by social media (“Since the previous survey, how much time have you spent on social media?”), and chose one of the following options: 0 = have not checked social media, 1 = less than 10 min, 2 = 10–30 min, 3 = 31–60 min, 4 = 1–2 h, 5 = 2–3 h, 6 = 3–4 h, or 7 = more than 4 h. We then converted the original scores into minutes, by taking the midpoint value of the answer range: 0 = 0 min, 1 = 5 min, 2 = 20 min, 3 = 45 min, 4 = 90 min, 5 = 150 min, 6 = 210 min, 7 = 270 min). All findings remained consistent using raw scores [SI6].
Current negative affect
Participants answered four separate questions that assessed their current levels of negative affect (How negative / sad / anxious / angry do you feel right now?) on a scale of 1 (not at all) to 100 (extremely) with higher scores indicating higher negative affect. To ensure appropriate reliability to detect within-person change over time (reliability of change [Rc])47, four items were combined to create mean negative affect scores (Rc = 0.752). Surveys also included two positive affect items (How positive/happy do you feel right now?), which we combined to produce mean positive affect scores (Rc = 0.830) [SI7].
Self-report surveys
Participants self-reported their levels of depression, anxiety, emotion dysregulation, and demographic information prior to the fMRI scan.
Depression
Depressive symptoms were measured by the 10-item Center for Epidemiologic Studies Depression Scale (CES-D)48. Items were rated on a 0 (rarely or none of the time) to 3 (most or all the time) scale. Scores were coded such that higher values indicate higher depressive symptom severity, then summed with a score range of 0–30. The scale’s internal consistency in the current study (α = 0.80) was high.
Anxiety
The 20-item State-Trait Anxiety Inventory (STAI)49 measured participants’ levels of anxiety symptoms. Items were rated on a 1 (not at all) to a 4 (very much) scale. Scores were coded such that higher values indicate higher levels of anxiety, then summed with scores ranging from 20 to 80. The scale’s internal consistency in the current study (α = 0.89) was high.
Emotion dysregulation
The short form 18-item Difficulties in Emotion Regulation Scale (DERS)50,51 measured the degree of difficulty experienced when regulating emotions. Items were rated on a 1 (almost never) to a 5 (almost always) scale. Scores were coded such that higher values indicate greater difficulty regulating emotions and were then averaged. DERS consists of six subscales measuring different types of difficulty in emotion regulation; we report the overall score in the main text, since our goal was to examine the general levels of emotion dysregulation. Please see [SI8] for individual subscale results. The scale’s internal consistency in the current study (α = 0.90) was high.
Demographics
Participants self-reported their age, gender, race/ethnicity, and perceived status within their communities using the MacArthur Scale of Subjective Social Status52. The race/ethnicity variable was converted to indicate White, Asian, Black, Latino/a, and Multiracial (i.e., selected more than one race/ethnicity option).
Analysis plan
We explored five hypotheses using three separate models. First, three linear regression models tested the associations between individual differences in average resting state frontoparietal connectivity and (1) depression (CES-D), (2) anxiety (STAI), and (3) emotion dysregulation (DERS).
Next, we used the “lmer” function of the lme4 package in R (ver.1.1-26)53 to perform a multilevel analysis. The model included the amount of time spent on social media, frontoparietal connectivity, and their interaction term as predictors of subsequent negative affect. To focus on within-person relationships, the time-varying predictor variable was within-person standardized. That is, we created a within-person standardized version of the time-spent-on-social-media variable, and each person’s time series had a mean of 0 and a standard deviation of 1. This allowed us to focus on within-person changes (i.e., in comparison to an individuals’ usual level) while holding the between-person differences in time spent on social media constant. To account for potential issues with combining multisite data, we included the site as a second level variable (i.e., participants nested within sites). Using this model, we tested whether (4) longer social media use during the period since the previous time point would subsequently predict more negative affect (EMA measures were obtained concurrently but the temporal association was assumed based on the retroactive wording of the social media use question; we focused on all temporal relationships, including morning-to-evening and evening-to-morning). In the same model, we further explored whether (5) the temporal link between social media use and negative affect would be moderated by individual differences in resting state frontoparietal functional connectivity. The slope of the time spent on social media was allowed to vary randomly across participants.
We then conducted follow-up simple slopes analysis, using the “sim_slopes” function of the interactions package in R (ver.1.1.3)54. Simple slopes analysis involves extracting predicted values of the relationship between predictor and outcome variables at different levels of a moderator, using all of the data directly from the multilevel model55. Using this method, we explored whether the relationship between social media use and negative affect varied across three different levels of frontoparietal functional connectivity, including at the mean and one standard deviation below/above the group mean level of connectivity. We also explored the possibility that the negative/positive affect at a previous time point would predict later social media use, and whether these links might be moderated by frontoparietal functional connectivity [SI9].
All analysis controlled for the study condition as part of a parent study that is not the focus of the current investigation. Analyses also controlled for demographic variables including age, gender, race/ethnicity, and self-reported social status. The multilevel model initially did not converge, and we removed covariates that accounted for no variance until the model converged, which resulted in the removal of the social status covariate. Simple slopes analysis models failed to converge when participants were nested within sites; the site variable was therefore removed for the simple slopes analysis. All results remained robust without controlling for these potential covariates [SI10]. All main results were robust to false discovery rate correction [SI11]. Unstandardized beta coefficients (b) and 95% confidence intervals (CI) are reported. All reported p values are two-tailed. Analyses were performed in R (v3.6.1, www.r-project.org) using the R-studio interface (v1.2.1335). Coefficients and statistics for all models are reported in [SI12].
Results
Time spent on social media
Throughout the 28-day EMA period, all participants reported at least some (i.e., non-zero) minutes of social media use. On average, participants reported having used social media on about 23 out of 28 days (M = 23.37 days, SD = 7.08, median = 26 days, range = 1–28). Participants spent about an hour on social media per use (assessed twice per day; M = 60.82 min, SD = 52.69 min, median = 44 min, range = 0–270 min), which translated into roughly 2 h of daily social media use. This rate was comparable to the average daily social media use among the U.S. adults (2 h 14 min)1.
Associations between functional connectivity and depression, anxiety, and emotion regulation
To assess whether individual differences in resting state functional connectivity within the frontoparietal system relate to emotional dysfunction, we examined its relationship to self-reported levels of depression, anxiety, and difficulty in emotion regulation measured at baseline. Participants who showed lower average frontoparietal connectivity also self-reported higher levels of depression (N = 51; b = − 43.043, 95%CI [− 73.05, − 13.03], p = 0.006) and anxiety (N = 51; b = − 70.947, 95%CI [− 136.70, − 5.20], p = 0.035), as well as greater difficulty regulating emotions (N = 52; b = − 4.069, 95%CI [− 7.86, − 0.28], p = 0.036) (Fig. 2).

Frontoparietal functional connectivity, depression, anxiety, and difficulty regulating emotion. Stronger resting state functional connectivity within the frontoparietal system was associated with lower self-reported depression (A), lower self-reported anxiety (B), and greater self-reported difficulty regulating emotions (C) among college students. CES-D = Center for Epidemiologic Studies Depression Scale; DERS = Difficulties in Emotion Regulation Scale; FC (z’) = Fisher r-to-z transformed functional connectivity scores; STAI = State-Trait Anxiety Inventory.
Relationships among social media use, functional connectivity, and subsequent negative affect
A multilevel model examined the relationship between social media use and negative affect, and whether this relationship varied by individual differences in resting state frontoparietal functional connectivity (N = 54; 2424 observations). Spending more than one’s usual number of minutes on social media since the previous time point predicted greater increases in negative affect (b = 4.382, 95%CI [1.37, 7.40], p = 0.006). In the same model, we also observed that this link was moderated by average frontoparietal functional connectivity, such that greater functional connectivity was associated with a weaker relationship between social media use and negative affect (b = − 17.154, 95%CI [− 31.10, − 3.21], p = 0.019).
Results from follow-up simple slopes analyses showed that more minutes spent on social media predicted feeling more negative for individuals with lower than average (b = 1.551, 95%CI [0.71, 2,39], p = 0.001) or at the mean (b = 0.746, 95%CI [0.15, 1.34], p = 0.017) levels of frontoparietal functional connectivity. By contrast, time spent on social media was not associated with subsequent negative affect among individuals with higher-than-average levels of frontoparietal functional connectivity (b = − 0.058, 95%CI [− 0.90, 0.78], p = 0.892) (Fig. 3).

Simple slopes analysis depicting the temporal relationship between time spent on social media and subsequent negative affect. Individuals with the weakest and mean levels of resting state functional connectivity within the frontoparietal system at baseline reported greater increases in negative affect following longer than their usual social media use, using time varying reports collected twice a day. By contrast, time spent on social media was not associated with subsequent negative affect for individuals with stronger frontoparietal functional connectivity. FC = functional connectivity; SD = standard deviation.
We also explored the reverse of the shown temporal relationship between social media use and subsequent affect. Specifically, we tested whether feeling positive or negative at a previous time point would predict the number of minutes spent on social media reported at a later time point, and whether this relationship would be moderated by frontoparietal functional connectivity; we found no such relationships [SI9]. In addition, none of the frontoparietal system’s specific subsystems, alone, moderated the link between time spent on social media and negative affect [SI4], suggesting that the interaction effect was unique to the average frontoparietal functional connectivity. We also examined positive affect as an outcome and found no significant effect of minutes spent on social media and subsequent positive affect, or an interaction between time spent on social media and frontoparietal connectivity [SI7].
Discussion
Social media have become part of many individuals’ daily routines and may affect users’ day-to-day experiences. The past decade of research suggests that the effects of social media engagement likely vary by individual differences that shape the user experience5. The current study explored whether individual differences in functional connectivity within the frontoparietal system moderated the relationship between social media use and subsequent affect.
As a potential neural moderator of the relationship between social media experiences and affective experiences, we focused on the average resting state functional connectivity within the frontoparietal system implicated in cognitive control of emotion12,13. In our non-clinical college sample, lower average frontoparietal functional connectivity was associated with higher depressive and anxiety symptoms, as well as greater difficulties in regulating emotions. These results suggest that the previously shown link between hypoconnectivity within the frontoparietal system and depression/anxiety22,23 may generalize to individuals without major psychopathology. Furthermore, weaker frontoparietal connectivity may signal a risk for emotion dysregulation. Future studies may examine whether changes in frontoparietal connectivity covary with different profiles of negative affect and emotion regulation capacities in a wider range of non-clinical populations to determine its role in everyday affective experience.
Does spending time on social media lead to feeling worse, or does feeling bad lead to longer social media use? Indeed, social media use is a tempting solution for a quick mood fix, and people may seek social media to regulate emotions56,57. However, we did not observe any evidence of positive or negative affect preceding longer/shorter social media use [SI9], suggesting that affect might not be a significant predictor of minutes spent on social media. Instead, our data showed that the reverse might be true, where spending longer than one’s typical amount of time on social media may precede feeling worse. Previous studies found that passive, as opposed to active, social media use that involves mindlessly scrolling with low engagement with other users58 was associated with negative emotions such as increased depression59 and anxiety symptoms60. Although we did not assess whether participants were actively or passively engaged with social media, nor what types of social media they engaged with (i.e., participants self-determined what they meant by social media), it is possible that longer use in our data may reflect increases in passive use and/or transitioning from active to passive use. Admittedly, time spent on social media might be too coarse an indication of the patterns of engagement8,61, but may still provide a rough guideline for a point of intervention. For example, future studies may leverage existing smartphone functionalities to track and limit screen time (e.g., iPhone's Screen Time function), and identify optimal timing of interventions designed to reduce use.
Weaker average functional connectivity within the frontoparietal system was a risk factor for negative affect following social media use. Specifically, spending longer time on social media predicted subsequently feeling worse for those with weaker frontoparietal functional connectivity. This result suggests that social media might pose greater risk to children and adolescents who show immaturities in the development of frontoparietal connectivity62, cognitive control of negative emotions63, and overall emotion regulation capacities64.
Although our study did not include measures of a domain general cognitive control capacity, results suggest that resting state hypoconnectivity within the frontoparietal system may underlie deficits in cognitive control that support emotion regulation in depression23. By contrast, stronger frontoparietal connectivity may signal more efficient engagement of executive control that supports emotion regulation in response to salient social information. If this is the case, then efforts to mitigate potential negative effects of social media use may benefit by focusing on specific individual emotion regulation capacities as well as exposures to daily stressors that may disrupt the ability to regulate emotions65; future research is needed to test these possibilities. It is also possible that frontoparietal connectivity may preemptively facilitate the filtering of incoming information9, selectively engaging with the types of information that are less likely to worsen emotions, and/or preventing rumination or worries when triggered. Given the constantly shifting nature of information processing in the social media environment, these types of regulation likely occur spontaneously. Future studies may examine whether consciously altering frontoparietal activity, via mindfulness66 or reappraisal10 strategies, may help improve the affective outcomes of social media use.
We note several limitations of this study. First, we relied on self-reported minutes of social media use, which did not distinguish different types of use and may suffer from recall bias and moderate reliability67. We also relied on a single-item measure of social media use8, which may result in overestimation among light users and underestimation among heavy users68. Our use of longitudinal EMA methods that assessed social media use at multiple timepoints per day might have circumvented some of these recall concerns, but does not tell us what people were doing in their use. Therefore, objectively logged and/or more fine-grained measures of the type of social media use will be important to refine these findings.
Second, the EMA survey was conducted at the onset of the COVID-19 pandemic, when there was a surge of negative news on social media (though we note that negative content such as polarizing news69 has been endemic in social media environments outside the pandemic context). We also note that in the same dataset, consuming specifically COVID-related news did not significantly interact with frontoparietal connectivity to predict negative affect (b = − 16.056, 95%CI [− 33.64, 1.53], p = 0.080). Future studies may test the generalizability of the current findings in additional contexts.
Third, we mainly focused on the within-level functional connectivity of the frontoparietal system. However, the frontoparietal system is closely interconnected with other systems (e.g., default mode and attention systems17), and may be influenced by the functioning of other systems (e.g., salience system70). Given that the frontoparietal recruitment likely involves dynamic configurations between networks across the brain more broadly, it is possible that between network dynamics, or functional coupling between systems, in addition to variability within the frontoparietal system, could play important roles in the context of cognitive control. Furthermore, frontoparietal systems are defined differently across different parcellations with potential overlap across different definitions of the granular functions of control they support. In this initial investigation of the relationship between social media use, which is a broad class of activities, and emotional experience, we began with a commonly used atlas that balances trade-offs between broad network definitions and more granular subsystem specificity. Given that there were statistical interactions between the frontoparietal system as defined in this study and social media use on subsequent affect, future research that is more granular both in terms of the bounds of what types of social media use, and the specific subsystems or patterns of connectivity within and between systems16,71, could be helpful16,71.
Fourth, psychological processes underlying frontoparietal connectivity should be interpreted with careful considerations for individual- and symptom-specific contexts. Although frontoparietal hypoconnectivity has been found in depression, suggesting reduced communication among neural systems involved in emotion regulation23, strong connectivity may not always reflect adaptive emotion processing. For example, over-recruitment of the frontoparietal–posterior cingulate cortex–precuneus system has been associated with cognitive anxiety, suggesting allocation of working memory and attention systems to potential sources of threat72,73. In fact, rather than hyper- or hypo-functional connectivity, the flexibility of frontoparietal functional connectivity might be important to interact with the ever-changing social media environments. Emotion regulation flexibility, or the ability to regulate emotions in ways that recognize and adapt to situational demands74, has been proposed to be the key to healthy psychological functioning75,76. Similarly, being able to efficiently recruit nodes of the frontoparietal system when necessary may be key to regulating negative emotions, which our data cannot address since our study did not include tasks that explicitly required regulation of negative affect. Researchers may combine and compare frontoparietal functioning at rest and while actively regulating emotions77, and link the brain data to the degree of emotion regulation success.
Fifth, we acquired relatively short, 5 min of resting state fMRI data. Although some previous studies showed that the strength of functional connectivity was stable with this amount of data78, and our use of relatively fast sampling rate (1 s TR) and multiband acquisition likely benefited the short resting state fMRI scan79, we encourage future studies on this topic to acquire longer resting state data to improve reliability. Sixth, we note that the current study was a multisite study that involved data collection from two separate universities. Although we used the same scanner model and the same acquisition protocol across sites and modeled participants as nested within sites in our multilevel model where possible, combining multisite fMRI data can introduce site-related confounds80. Finally, previous studies support that social media use can increase both positive and negative health outcomes, and depends on the type of engagement8. Although we did not observe any associations between time spent on social media and positive affect [SI7], the link between social media use and negative affect that we observed in the current study does not preclude that other social benefits may exist.
In conclusion, this study provides initial evidence that individual differences in average resting state functional connectivity within the frontoparietal system moderate the relationship between time spent on social media and subsequent negative affect. These results are consistent with previous neurocognitive models of negative emotions and emotion regulation in which disrupted communication within the nodes of functional networks may relate to dysregulation of negative emotional experience. More broadly, the current findings suggest potential venues for interventions that consider individual differences in how people respond to social media and the temporal dynamics of social media use that may influence psychological well-being.
Data and code availability
Data and analysis scripts are available at https://github.com/cnlab/social_media_brain/.
References
Kemp, S. Digital 2022: Global overview report. DataReportal—Global Digital Insights https://datareportal.com/reports/digital-2022-global-overview-report (2022).
Hancock, J., Liu, S. X., Luo, M. & Mieczkowski, H. Psychological well-being and social media use: A meta-analysis of associations between social media use and depression, anxiety, loneliness, eudaimonic, hedonic and social well-being. SSRN Electron. J. https://doi.org/10.2139/ssrn.4053961.
Boer, M., Stevens, G. W. J. M., Finkenauer, C. & van den Eijnden, R. J. J. M. The complex association between social media use intensity and adolescent wellbeing: A longitudinal investigation of five factors that may affect the association. Comput. Hum. Behav. 128, 107084 (2022).
Orben, A. Teenagers, screens and social media: A narrative review of reviews and key studies. Soc. Psychiatry Psychiatr. Epidemiol. 55, 407–414 (2020).
Orben, A., Dienlin, T. & Przybylski, A. K. Social media’s enduring effect on adolescent life satisfaction. Proc. Natl. Acad. Sci. U. S. A. 116, 10226–10228 (2019).
Kreski, N. et al. Social media use and depressive symptoms among United States adolescents. J. Adolesc. Health 68, 572–579 (2021).
Odgers, C. L., Schueller, S. M. & Ito, M. Screen time, social media use, and adolescent development. Annu. Rev. Dev. Psychol. https://doi.org/10.1146/annurev-devpsych-121318-084815 (2020).
Hancock, J. T., Liu, S. X., Luo, M. & Mieczkowski, H. Social media and psychological well-being. In The Psychology of Technology: Social Science Research in the Age of Big Data, (pp (ed. Matz, S. C.) vol. 451, 195–238 (American Psychological Association, xvi, 2022).
Ptak, R. The frontoparietal attention network of the human brain: Action, saliency, and a priority map of the environment. Neuroscientist 18, 502–515 (2012).
Buhle, J. T. et al. Cognitive reappraisal of emotion: A meta-analysis of human neuroimaging studies. Cereb. Cortex 24, 2981–2990 (2014).
Greicius, M. Resting-state functional connectivity in neuropsychiatric disorders. Curr. Opin. Neurol. 21, 424–430 (2008).
Lindquist, K. A. & Barrett, L. F. A functional architecture of the human brain: Emerging insights from the science of emotion. Trends Cogn. Sci. 16, 533–540 (2012).
Kober, H. et al. Functional grouping and cortical–subcortical interactions in emotion: A meta-analysis of neuroimaging studies. Neuroimage 42, 998–1031 (2008).
Ochsner, K. N. & Gross, J. J. The cognitive control of emotion. Trends Cogn. Sci. 9, 242–249 (2005).
Rodman, A. M., Jenness, J. L., Weissman, D. G., Pine, D. S. & McLaughlin, K. A. Neurobiological markers of resilience to depression following childhood maltreatment: The role of neural circuits supporting the cognitive control of emotion. Biol. Psychiatry 86, 464–473 (2019).
Weissman, D. G. et al. Earlier adolescent substance use onset predicts stronger connectivity between reward and cognitive control brain networks. Dev. Cogn. Neurosci. 16, 121–129 (2015).
Spreng, R. N., Sepulcre, J., Turner, G. R., Stevens, W. D. & Schacter, D. L. Intrinsic architecture underlying the relations among the default, dorsal attention, and frontoparietal control networks of the human brain. J. Cogn. Neurosci. 25, 74–86 (2013).
Barrett, L. F. & Satpute, A. B. Large-scale brain networks in affective and social neuroscience: Towards an integrative functional architecture of the brain. Curr. Opin. Neurobiol. 23, 361–372 (2013).
Andrews-Hanna, J. R., Smallwood, J. & Spreng, R. N. The default network and self-generated thought: Component processes, dynamic control, and clinical relevance. Ann. N. Y. Acad. Sci. 1316, 29–52 (2014).
Li, J., Chen, J., Kong, W., Li, X. & Hu, B. Abnormal core functional connectivity on the pathology of MDD and antidepressant treatment: A systematic review. J. Affect. Disord. 296, 622–634 (2022).
Iwabuchi, S. J. et al. Localized connectivity in depression: A meta-analysis of resting state functional imaging studies. Neurosci. Biobehav. Rev. 51, 77–86 (2015).
Menon, V. Large-scale brain networks and psychopathology: A unifying triple network model. Trends Cogn. Sci. 15, 483–506 (2011).
Kaiser, R. H., Andrews-Hanna, J. R., Wager, T. D. & Pizzagalli, D. A. Large-scale network dysfunction in major depressive disorder: A meta-analysis of resting-state functional connectivity. JAMA Psychiatry 72, 603–611 (2015).
Banks, S. J., Eddy, K. T., Angstadt, M., Nathan, P. J. & Phan, K. L. Amygdala–frontal connectivity during emotion regulation. Soc. Cogn. Affect. Neurosci. 2, 303–312 (2007).
Andrews, M. E., Pei, R., Lauharatanahirun, N., Paul, A. M. & Falk, E. B. Social Media and the Social Brain.
United States. The U.S. Surgeon General's Advisory, Social media and youth mental health. Office of the Surgeon General. https://www.hhs.gov/sites/default/files/sg-youth-mental-health-social-media-advisory.pdf (2023).
Rainie, L., Keeter, S. & Perrin, A. Trust and Distrust in America: Many Americans think declining trust in the government and in each other makes it harder to solve key problems. They have a wealth of ideas about what’s gone wrong and how to fix it (Pew Research Center, 2019).
Ferguson, C. J. Does the internet make the world worse? Depression, aggression and polarization in the social media age. Bull. Sci. Technol. Soc. 41, 116–135 (2021).
Vogel, E. A., Rose, J. P., Okdie, B. M., Eckles, K. & Franz, B. Who compares and despairs? The effect of social comparison orientation on social media use and its outcomes. Personal. Individ. Differ. 86, 249–256 (2015).
Cosme, D. et al. Study protocol: Social health impact of network effects (SHINE) study. https://doi.org/10.31234/osf.io/cj2nx (2022).
Kang, Y. et al. Purpose in life, neural alcohol cue reactivity and daily alcohol use in social drinkers. Addiction 117, 3049–3057 (2022).
Peirce, J. et al. PsychoPy2: Experiments in behavior made easy. Behav. Res. 51, 195–203 (2019).
Esteban, O. et al. fMRIPrep: A robust preprocessing pipeline for functional MRI. Nat. Methods 16, 111–116 (2019).
Gorgolewski, K. et al. Nipype: A flexible, lightweight and extensible neuroimaging data processing framework in python. Front. Neuroinform. 5, 13 (2011).
Gorgolewski, K. J. et al. Nipype. Softw. Zenodo. https://doi.org/10.5281/zenodo (2018).
Cox, R. W. & Hyde, J. S. Software tools for analysis and visualization of fMRI data. NMR Biomed. 10, 171–178. https://doi.org/10.1002/(sici)1099-1492(199706/08)10:4/5<171::aid-nbm453>3.0.co;2-l (1997).
Jenkinson, M., Bannister, P., Brady, M. & Smith, S. Improved optimization for the robust and accurate linear registration and motion correction of brain images. Neuroimage 17, 825–841 (2002).
Ciric, R. et al. Benchmarking of participant-level confound regression strategies for the control of motion artifact in studies of functional connectivity. Neuroimage 154, 174–187 (2017).
Power, J. D. et al. Functional network organization of the human brain. Neuron 72, 665–678 (2011).
Chai, X. J., Castañón, A. N., Ongür, D. & Whitfield-Gabrieli, S. Anticorrelations in resting state networks without global signal regression. Neuroimage 59, 1420–1428 (2012).
Murphy, K., Birn, R. M., Handwerker, D. A., Jones, T. B. & Bandettini, P. A. The impact of global signal regression on resting state correlations: Are anti-correlated networks introduced?. Neuroimage 44, 893–905 (2009).
Fox, M. D., Zhang, D., Snyder, A. Z. & Raichle, M. E. The global signal and observed anticorrelated resting state brain networks. J. Neurophysiol. 101, 3270–3283 (2009).
Dixon, M. L. et al. Heterogeneity within the frontoparietal control network and its relationship to the default and dorsal attention networks. Proc. Natl. Acad. Sci. U. S. A. 115, E1598–E1607 (2018).
Dion, M. L., Sumner, J. L. & Mitchell, S. M. Gendered citation patterns across political science and social science methodology fields. Polit. Anal. 26, 312–327 (2018).
Mitchell, J. P., Banaji, M. R. & Macrae, C. N. The link between social cognition and self-referential thought in the medial prefrontal cortex. J. Cogn. Neurosci. 17, 1306–1315 (2005).
Zhou, D. et al. Gender diversity statement and code notebook v1.0. https://github.com/dalejn/cleanBib (2020).
Cranford, J. A. et al. A procedure for evaluating sensitivity to within-person change: Can mood measures in diary studies detect change reliably?. Personal. Soc. Psychol. Bull. 32, 917–929 (2006).
Radloff, L. S. The CES-D scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1, 385–401 (1977).
Spielberger, C. D., Gorsuch, R. L. & Lushene, R. E. STAI Manual for the State-trait Anxiety Inventory (‘Self-evaluation Questionnaire’) (Consulting Psychologists Press, 1970).
Gratz, K. L. & Roemer, L. Multidimensional assessment of emotion regulation and dysregulation: Development, factor structure, and initial validation of the difficulties in emotion regulation scale. J. Psychopathol. Behav. Assess. 26, 41–54 (2004).
Victor, S. E. & Klonsky, E. D. Validation of a brief version of the difficulties in emotion regulation scale (DERS-18) in five samples. J. Psychopathol. Behav. Assess. 38, 582–589 (2016).
Adler, N., Stewart, J. & Others. The MacArthur scale of subjective social status. San Francisco: MacArthur Research Network on SES & Health (2007).
Bates, D., Mächler, M., Bolker, B. & Walker, S. Fitting linear mixed-effects models Usinglme4. J. Stat. Softw. https://doi.org/10.18637/jss.v067.i01 (2015).
Long, J. A. Interactions: Comprehensive, user-friendly toolkit for probing interactions. 2019. Sci. Rep. 12, 12184 (2022).
Aiken, L. S., West, S. G. & Reno, R. R. Multiple Regression: Testing and Interpreting Interactions (SAGE, 1991).
O’Day, E. B. & Heimberg, R. G. Social media use, social anxiety, and loneliness: A systematic review. Comput. Hum. Behav. Rep. 3, 100070 (2021).
Thomas, V., Balzer Carr, B., Azmitia, M. & Whittaker, S. Alone and online: Understanding the relationships between social media, solitude, and psychological adjustment. Psychol. Pop. Media 10, 201–211 (2021).
Montague, E. & Xu, J. Understanding active and passive users: The effects of an active user using normal, hard and unreliable technologies on user assessment of trust in technology and co-user. Appl. Ergon. 43, 702–712 (2012).
Escobar-Viera, C. G. et al. Passive and active social media use and depressive symptoms among United States adults. Cyberpsychol. Behav. Soc. Netw. 21, 437–443 (2018).
Thorisdottir, I. E., Sigurvinsdottir, R., Asgeirsdottir, B. B., Allegrante, J. P. & Sigfusdottir, I. D. Active and passive social media use and symptoms of anxiety and depressed mood among icelandic adolescents. Cyberpsychol. Behav. Soc. Netw. 22, 535–542. https://doi.org/10.1089/cyber.2019.0079 (2019).
Valkenburg, P. M., van Driel, I. I. & Beyens, I. The associations of active and passive social media use with well-being: A critical scoping review. New Media Soc. 24, 530–549 (2022).
Hwang, K., Velanova, K. & Luna, B. Strengthening of top-down frontal cognitive control networks underlying the development of inhibitory control: A functional magnetic resonance imaging effective connectivity study. J. Neurosci. 30, 15535–15545 (2010).
Martin, R. E. et al. Longitudinal changes in brain structures related to appetitive reactivity and regulation across development. Dev. Cogn. Neurosci. 38, 100675 (2019).
Silvers, J. A., Buhle, J. T. & Ochsner, K. N. The Neuroscience of Emotion Regulation: Basic Mechanisms and Their Role in Development, Aging, and Psychopathology (Oxford University Press, 2013).
Stawski, R. S., Sliwinski, M. J., Almeida, D. M. & Smyth, J. M. Reported exposure and emotional reactivity to daily stressors: The roles of adult age and global perceived stress. Psychol. Aging 23, 52–61 (2008).
Taren, A. A. et al. Mindfulness meditation training and executive control network resting state functional connectivity: A randomized controlled trial. Psychosom. Med. 79, 674–683 (2017).
Parry, D. A. et al. A systematic review and meta-analysis of discrepancies between logged and self-reported digital media use. Nat. Hum. Behav. 5, 1535–1547 (2021).
Scharkow, M. The accuracy of self-reported internet use—A validation study using client log data. Commun. Methods Meas. 10, 13–27 (2016).
Allcott, H., Braghieri, L., Eichmeyer, S. & Gentzkow, M. The welfare effects of social media. Am. Econ. Rev. 110, 629–676 (2020).
Menon, V. & Uddin, L. Q. Saliency, switching, attention and control: A network model of insula function. Brain Struct. Funct. 214, 655–667 (2010).
Chen, Y.-Y., Yim, H. & Lee, T.-H. Negative impact of daily screen use on inhibitory control network in preadolescence: A two-year follow-up study. Dev. Cogn. Neurosci. 60, 101218 (2023).
Bijsterbosch, J., Smith, S., Forster, S., John, O. P. & Bishop, S. J. Resting state correlates of subdimensions of anxious affect. J. Cogn. Neurosci. 26, 914–926 (2014).
Li, H. et al. Disruption of the structural and functional connectivity of the frontoparietal network underlies symptomatic anxiety in late-life depression. Neuroimage Clin. 28, 102398 (2020).
Aldao, A., Sheppes, G. & Gross, J. J. Emotion regulation flexibility. Cogn. Ther. Res. 39, 263–278 (2015).
Kashdan, T. B. & Rottenberg, J. Psychological flexibility as a fundamental aspect of health. Clin. Psychol. Rev. 30, 865–878 (2010).
Bonanno, G. A. & Burton, C. L. Regulatory flexibility: An individual differences perspective on coping and emotion regulation. Perspect. Psychol. Sci. 8, 591–612 (2013).
Uchida, M. et al. Emotion regulation ability varies in relation to intrinsic functional brain architecture. Soc. Cogn. Affect. Neurosci. 10, 1738–1748 (2015).
Van Dijk, K. R. A. et al. Intrinsic functional connectivity as a tool for human connectomics: Theory, properties, and optimization. J. Neurophysiol. 103, 297–321 (2010).
Demetriou, L. et al. A comprehensive evaluation of increasing temporal resolution with multiband-accelerated protocols and effects on statistical outcome measures in fMRI. Neuroimage 176, 404–416 (2018).
Feis, R. A. et al. ICA-based artifact removal diminishes scan site differences in multi-center resting-state fMRI. Front. Neurosci. 9, 395 (2015).
Acknowledgements
We thank Silicia Lomax, Faustine Corbani, José Carreras-Tartak, Yi Zhang, and Sky Zhang for research assistance. This work was supported by Army Research Office [to E.B.F., W911NF1810244], Mind and Life Institute [to Y.K.], and Hopelab [to Y.K. and E.B.F.]. The content is solely the responsibility of the authors and does not represent the views of the funding agencies.
Author information
Authors and Affiliations
Contributions
Conceptualization: D.S.B., D.L.S., E.B.F., K.N.O., P.J.M., Y.K. Methodology: D.L.S., J.A., Y.K. Formal analysis for this paper: J.A., L.M.T., Y.K. Investigation: D.C., O.S., Y.K. Data Curation: D.C., E.B.F., J.A., Y.K. Writing—Original Draft: Y.K. Writing—Review and Editing: All authors. Supervision: D.S.B., D.L.S., E.B.F., K.N.O., P.J.M. Project administration: D.C., D.S.B., D.L.S., E.B.F., N.K.O., P.J.M., Y.K., Z.M.B. Funding acquisition: D.S.B., E.B.F., K.N.O., P.J.M.
Corresponding authors
Ethics declarations
Competing interests
Emily Falk, Ph.D. is on the scientific advisory board for Kumanu. The rest of the authors have no financial interest to declare.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kang, Y., Ahn, J., Cosme, D. et al. Frontoparietal functional connectivity moderates the link between time spent on social media and subsequent negative affect in daily life. Sci Rep 13, 20501 (2023). https://doi.org/10.1038/s41598-023-46040-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-46040-z
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
