
Abstract
The older adult is an influential group experiencing acute myocardial infarction, delaying treatment and causing a high mortality rate. Factors related to their delay differ from other age groups, and their specific characteristics are barriers to recognizing their symptoms and learning new information. Therefore, specific innovative methods related to their limitations and needs should be considered when developing interventions promoting on-time treatment. This study aims to review intervention details and their effects on knowledge, belief, decision-making, rate of calling 911, and mortality among community-dwelling older adults at risk or after a first myocardial infarction compared to receiving usual care or no intervention. The 12 databases were searched unlimitedly until July 30, 2022. The two researchers independently reviewed the articles, and the third reviewer broke the tight when disagreement was found. Data were extracted, kinds of interventions were grouped, and intervention details were summarized narratively. Finally, the selected outcomes were analyzed by meta-analysis using a fixed and a random-effects model. Eleven articles were for final review. Interventions were categorized into eight groups: direct mail, community-based, multi-group health education, innovation methods, tailored education, structured education, tricked intervention promoting memory and concern, and nurse-based case management. Finally, the meta-analysis found that only innovative methods could increase the rate of calling 911 and taking aspirin (Odd ratio = 2.55; 95% CI = 1.01-6.44). In contrast, there were no statistically significant differences in the rate of affecting time to first unplanned readmission or death and time delay to the emergency room. Results recommended that effective and specific interventions must be developed and strengthened to promote older adults surviving acute myocardial infarction.
Clinical Trial Registration Number: PROSPERO CRD42021247136.
Similar content being viewed by others



Introduction
The world population nowadays lives longer; their life expectancy is sixty and older1. Unfortunately, their extended lifetime is with functional decline and chronic diseases that cause their illness to become more complicated and hinder them from being detected and treated2,3. Reduced body reserve, Atypical presentation, Multiple pathologies, Polypharmacy, and Social adversity (RAMPS) can describe why it is complicated when providing care and treatment among older adults4. Reduced body reserve led to older persons' health conditions quickly deteriorating and their ability to wait less than other age groups because of lower energy reservation. Atypical presentation confuses older adults, their family members, and healthcare staff about the origin of problems, causing missed or delayed diagnosis and treatment. Multipatology causes them to use Poly medicine, and both join in making signs and symptoms more complicated. Finally, older adults need help from their family members and support from others in their community for emergency and long-term care situations, which is defined as Social adversity3. The five clinical features complicate older adults’ diagnosis, care, and treatment. It is a serious problem if older adults confuse their symptoms and delay treatment in an emergency, especially acute myocardial infarction (AMI), which needs quick and accurate responses within two hours, defined as the golden period2. The specific intervention aware of older adults’ limitations and needs to promote quick and accurate decisions and prevent treatment delay should be considered.
Background
AMI occurs when the blood flow that brings oxygen to the heart muscle is immediately and severely reduced or cut off because of plague rupture or acute vasoconstriction, causing an emergency2. AMI is a time-related recovery disease called time-is-muscle since the myocardial damage or recovery depends on the time the patients decide and receive treatment; however, delayed decision and high mortality rates are still found2. Studies reported that the patient with a longer interval between the onset of symptoms and treatment is likelier to experience complications and die than the patient who did not delay treatment5,6. This serious health problem is one of the leading causes of death in the developed world, with prevalence approaching three million people worldwide7. About every 40 s, someone in the United States has an AMI, and more than one million deaths in the United States annually2. Based on the National Health and Nutrition Examination Survey 2017 to March 2020 data, the prevalence of cardiovascular diseases in adults in the United States was 48.6% overall (about 127.9 million), which increases with age, and older adults substantially contribute to the mortality caused by cardiovascular morbidity8. In the same year, mortality data, cardiovascular diseases currently claim more lives each year; about 207 of 100,000 people died, and the leading cause is AMI and stroke2. According to data from 2005 to 2014 from the Atherosclerosis Risk in Communities Study, the estimated annual incidence of myocardial infarction is 605,000 new attacks and 200,000 recurrent attacks. Both cause cardiogenic shock and cardiac arrest, becoming the major cause of death2.
Around 5% of patients with AMI develop cardiogenic shock with a mortality of 40–50%, found outside the hospital while seeking treatment. The morbidity and mortality associated with AMI are proportionate to the time to receive treatment from the onset of symptoms9. Another study also reported that laypeople in the United States initiated cardiopulmonary resuscitation in 40.2% of out-of-hospital cardiac arrests in 202110. In the United States, sudden cardiac arrest and experience worse survival after sudden cardiac arrest were still high2. Every year, more than 356,000 Americans experience an out-of-hospital cardiac arrest, and 60 to 80 percent die before arriving at the hospital, and this is often found among females and older adults2,8. The atypical presentation often found among female and older adults, confusing them to decide to get treatment lately, might be the origin of the problem7.
Mortality associated with AMI is directly linked to the time to receive treatment and missed diagnoses9. Then, delayed decisions and treatment are areas of concern. Based on the systematic review, Huriani et al. reported that the mean time from symptom onset to first medical contact was 12.7 h, ranging from 10 min to 96 h. Older, female, illiterate, living in a rural area, and financially limited were associated with longer treatment delays. The lack of a developed emergency transportation system and poor communication and organization between community and interventional facilities were also cited as significant contributors to treatment delays11. Another cause of delay is the atypical presentation of AMI among older adults, which confuses them during their symptom recognition and decision-making9. American Heart Association reported that 805,000 patients experienced first and recurrent events2; however, about 170,000 are silent, and over 50% experience atypical symptoms of AMI8,9,12,13,14. The atypical presentation was found in over 50% of older adults, and two-thirds delayed the decision to get treatment9,12,14. Moreover, over half of this group are older adults who died before arriving at the hospital and have no chance to receive treatment, although AMI treatments are very effective12,14. Health professionals are aware of typical AMI presentation; however, atypical AMI is difficult to diagnose and confuses older adults, their family members, and healthcare staff. On the other hand, it is likely to impact delayed decision-making and cause high morbidity and mortality.
Khan et al. summarized that atypical presentations of myocardial infarction are vast; patients may have chest pain without typical characteristics of angina pectoris or may not have chest pain. Most patients were older adults and commonly presented with pain and discomfort in the abdomen, head, and neck regions9. The other two studies reported that atypical clinical features, such as neck pain, pain in the back, throat pain, ear discomfort, and hiccups, are not uncommon. Craniofacial pain can be the sole symptom in up to 6% of patients with AMI. Women and older adults need special mention as they often present with atypical symptoms, and a high index of suspicion is required9,12. A patient who is 50 years or older, having comorbidities such as diabetes, hypertension, dyslipidemia, history of tobacco or marijuana usage, and presenting with prodromal symptoms like shortness of breath, dizziness, fatigue, syncope, gastrointestinal discomfort or head/neck pain should be suspected for atypical AMI9. This atypical symptom can lead to delayed decision-making and diagnosis, suboptimal treatment, and detrimental outcomes. To avoid such mishaps, accurate and timely interpretation of atypical clinical symptomatology of AMI has a vital bearing on patient triage, treatment, and subsequent management9.
Beyond worsening health conditions and high mortality rates, AMI made up the cost of treatment for both direct and indirect costs. According to Healthcare Cost and Utilization Project data from the Agency for Healthcare Research and Quality for 2018, 481,780 percutaneous coronary interventions were performed in patients in the United States2. The average annual direct and indirect cost related to AMI in the United States was an estimated $407.3 billion from 2018 to 2019. The estimated direct costs related to AMI in the United States increased from $103.5 billion in 1996 to 1997 to $251.4 billion from 2018 to 2019. By event type, hospital inpatient stays accounted for the highest direct cost ($111.4 billion) from 2018 to 2019 in the United States8. If they delay treatment, they may experience complications, causing longer lengths of stay and higher treatment costs. All of the above reflect that AMI is an emergency and critical situation that needs appropriate and quick response to receive treatment on time to decrease worsening health conditions, mortality rate, and cost of treatment. This condition is associated with age and causes a high mortality rate for this group of people, especially those who died before arriving at the hospital and had no chance to get treatment. Then, delayed decision-making is an area of concern2.
In conclusion, older adult is a significant group of people who experience AMI and delay seeking treatment. The results from this situation are that most of this vulnerable group of people delayed seeking treatment and died before arriving at the hospital. Moreover, older adults who receive treatment late have high rates of long length-of-stay, high cost of treatment, in-hospital mortality, and mortality of 30 days after discharge9,11. Specific interventions to promote decision-making and prevent delay in seeking treatment among older adults from the literature review are needed to deal with this emergency and critical situation. The interventions to promote quick and accurate decisions to receive treatment on time are an area of concern. From an initial review, we found that several systematic reviews provided various pathways, techniques, materials, and contents of interventions to deal with this critical problem11,15,16. Unfortunately, these interventions are for all age groups of AMI patients; however, factors causing older adults to delay treatment differ from other age groups, especially atypical symptoms, knowledge, belief, and their functional decline related to aging. The specific interventions that promote decision-making and prevent delaying treatment for older adults are not promptly synthesized. This review was conducted to summarize all details and types of interventions to promote decision-making, prevent delaying treatment for older adults, and explore their effectiveness.
Aims
This study aimed first to review the components and details of AMI interventions to promote decision-making and prevent delaying treatment. Then, interventions’ details were summarized and guided for intervention development for a specific group of community-dwelling older adults. Secondly, the effects of the interventions on selected health outcomes among community-dwelling older adults were also explored and demonstrated.
Methods
Design
A systematic review with a narrative summary of interventions' details and a meta-analysis of selected health outcomes was undertaken. The Preferred Reporting Items of Systematic Reviews and Meta-Analysis (PRISMA) checklist guidelines and the standardized critical appraisal instruments from the Joanna Briggs Institute17 were used to conduct this review. The protocol to conduct this systematic review was prospectively registered and published with PROSPERO (CRD42021247136).
Search strategies
Keywords were identified for searching by using PICO as population, intervention, comparison, and outcomes. The population is community-dwelling older adults at risk or after a first myocardial infarction. The intervention is AMI interventions, the comparison is no intervention or usual care, and the outcome is decision-making and on-time treatment. The search terms for population included “older adult,” “older people,” “elderly,” “aging,” “senior citizen,” “chest pain,” “acute myocardial infarction,” “heart attack,” “acute coronary syndrome,” and “cardiac event.” The search terms for interventions are “health education,” “health literacy,” “community-based program,” “telehealth,” and “avatar health application.” The comparison search terms are “home visit” and “routine suggestion.” Finally, the search terms for outcomes are “knowledge,” “attitude,” “decision,” “time of delay,” “health-seeking,” “delayed time,” “pre-hospital delay,” “timely treatment,” and “seeking treatment.” The researchers used “OR” to connect wordings within the concept. However, “AND” was used to connect wordings between concepts. The search statement was developed and published in PROSPERO so another independent reviewer could duplicate and check.
Databases were unlimitedly searched for empirical articles up to July 30, 2022. The search was conducted in 12 databases: PubMed, CINAHL, SCOPUS, OVID, CENTRAL, ISI, ProQuest, ClinicalTrail.gov, Open grey, ThaiList, ThaiJO, and E-THESIS, using keywords.
Inclusion and exclusion criteria
The inclusion criteria included the studies (1) at least 80% of participants aged 60 or older, (2) were randomized controlled trials (RCT) or quasi-experimental studies and achieved 60% of scores from each critical appraisal tool, such as 8 out of 13 or 6 out of 9 from the Critical Appraisal for RCT and quasi-experimental studies, respectively, (3) reported components and details of the AMI interventions to promote decision-making and prevent delaying treatment, (4) reported relevant statistical results of the AMI interventions to promote decision-making and prevent delaying treatment, including knowledge, belief/attitude, calling 911 or EMS, mortality, readmission, appropriate action/taking aspirin, coping behavior/anxiety, awareness, time of delay/seeking, and malnutrition risk. Only three studies reported the quality of instruments, and (5) were published in English or Thai in both peer-reviewed journals or were thesis/dissertations. However, the study included hospitalized older adults, and the study included older adults with mild cognitive impairment or depression were excluded.
Critical appraisal
Evidence levels were indicated using the hierarchical evidence pyramid from the JBI18. Before including the research articles, the selected studies' quality was assessed using the critical appraisal tool from JBI; the Checklists for RCT and Quasi-Experimental Studies were applied for this review19,20. Moreover, grading was provided for each study, which was included in the table of result reports21.
Risk of bias
The selected studies were required to meet a positive response (i.e., “yes”) on a minimum of six out of nine for quasi-experimental studies and eight out of 13 for RCT19,20. Two reviewers independently assessed the risk-of-bias, and a risk-of-bias table was designed for each eligible study. Disagreements between review authors were resolved by mutual consensus and the third reviewer. Methodological quality was categorized into very low, low, moderate, and high-quality categories21. Critical appraisal results were also reported in narrative form and a table. All selected studies were reported their methodological quality and underwent data extraction and synthesis.
Study selection and data extraction
This process included two steps. First is a study selection. The two reviewers conducted the study selection independently for inclusion, with their decisions blinded. This process was completed in two stages, initially based on titles and abstracts screening and then by reviewing the full text of the articles retained in the first step. We resolved any disagreements regarding the selection of studies by consensus. The two reviewers recorded any decisions in reference management software, Rayyan reference management. This step yielded a PRISMA Flow Chart after the screening process.
The second step is data extraction. Before starting this process, the codebook and data extraction forms were developed. The characteristics of each included study were extracted using a data extraction form, which included (1) the studies’ authors, (2) study designs, (3) settings, (4) participants, (5) levels of evidence certainty and methodological quality, (6) components of the AMI interventions; (7) times of outcomes measuring; and (8) the statistical results for selected outcomes of the AMI interventions. A codebook was revised after pilot testing with five studies. After that, two reviewers conducted data extraction independently, and disagreements between the reviewers were solved through mutual discussion. We attempted to contact included study investigators for unreported data or additional details needed for the meta-analysis generation; four studies were found, and the principal study investigators were contacted. Finally, we received all the information and statistics needed.
Data analysis
Qualitative results
The contents and details of programs or interventions were extracted and synthesized to support the first aim. The narrative methods were applied for this section. Moreover, themes were set to categorize groups of interventions. Essential and specific details included in the AMI interventions from selected studies were provided under each theme. These details help guide the effective intervention for practice and future study. Finally, some of the selected outcomes were impossible to include for meta-analysis due to the heterogeneity of the study population, outcome measures, time of measuring, and data analysis across the studies; the p-values of these selected outcomes were provided and reported in the table.
Quantitative results
We included studies reporting odds ratios (unadjusted or adjusted OR) of calling 911 and taking aspirin among AMI patients with and without intervention. Hazard ratios were used to conduct a pooled analysis of the association between people receiving an intervention and those without any intervention regarding affecting time to first unplanned readmission or death. The standardized mean differences were used to analyze the association between people receiving an intervention and those without any intervention regarding delay time to the ER. A meta-analysis was conducted only for categories with sufficient available data, typically requiring more than one study to combine the outcomes.
The DerSimonian and Laird based on the inverse-variance weighted average approach for meta‐analyses with random effects were applied if the study heterogeneity was high22. However, if necessary, the fixed-effect model with inverse-variance weights was also applied if the study heterogeneity was low. The supposed clinical or considerable statistical heterogeneity was present (Statistically significant when p-value < 0.10 using a chi-squared test (Cochran Q test) and I2 > 50%). In that case, the findings with a narrative approach following synthesis without meta-analysis guidelines were applied. Publication bias was visually assessed using Begg’s funnel plots and statistically assessed with Egger’s test. The analyses were conducted using statistical software of STATA version 16. Finally, results were reported following the PRISMA guideline for reporting systematic review and meta-analysis.
Validity, reliability, and rigor
A research team from different disciplines and expertise conducted this study. The systematic review experts and librarians worked together to develop a search statement, select essential databases related to the study topic, and search for articles together. The team developed and proved the systematic review protocol and search statement. The principal researcher prospectively registered a study protocol before conducting this systematic review and strictly followed the protocol to reduce bias and increase validity and reliability. An independent review was provided for all processes. A third independent researcher provided a third opinion that helped break the tight when disagreement was found. Moreover, if primary researchers did not provide sufficient data for generating meta-analysis, we contacted the corresponding author via provided e-mails. Fortunately, we received all we needed from the corresponding authors. Finally, statisticians took part in data analysis, especially meta-analysis generation, to confirm the accuracy of data analysis for this study.
Results
The initial search found 60,739 articles from 12 databases, and 8,659 articles were the rest after duplicate. Based on the inclusion and exclusion criteria, 11 articles were selected for the final comprehensive review. The PRISMA flow diagram of the information flow during the review process is displayed in Fig. 1.
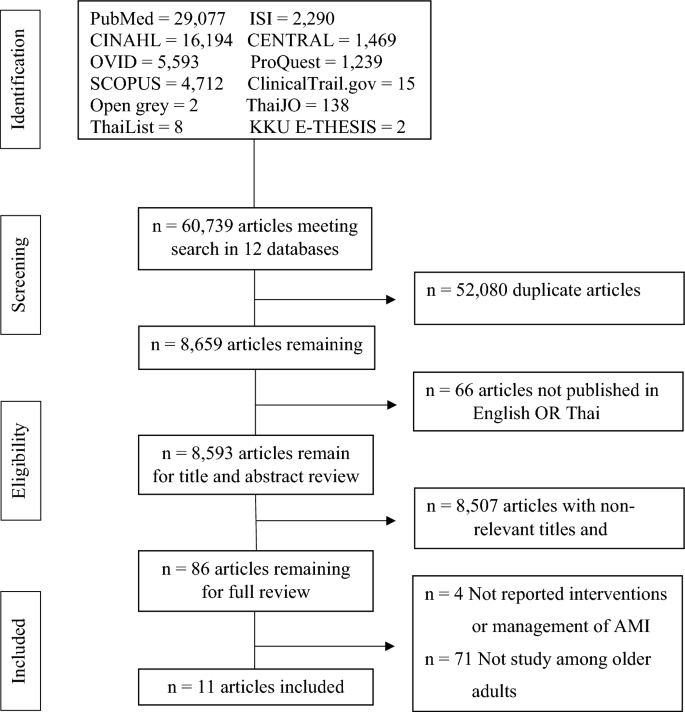
Flow chart of the review process and results.
Characteristics of included studies
Of 11 studies23,24,25,26,27,28,29,30,31,32,33, eight were conducted before 201223,24,25,26,27,28,29,30. Nine studies were in the USA23,24,25,26,27,28,29,30,31, and two were in Germany32,33. Ten studies aimed to explore the effectiveness of intervention/health education on health outcomes24,25,26,27,28,29,30,31,32,33; however, one focused only on elevating the use of emergency services (call 911 or call for emergency medical service: EMS)23. The research designs were nine randomized controlled trials23,24,25,26,27,29,31,32,33 and two quasi-experimental studies28,30. The interventions included a direct mail intervention23, a community-based intervention program24, a Rapid Early Action for Coronary Treatment (REACT) trial25, three Heart Attack Survival Kit23,27,29, two structured/tailored educational/counseling interventions28,30, a Health education-Matters Of Your Heart using the acronym FACTSS & CURB31, and two nurse-based case management for older patients32,33. Five teams used multiple pathways24,26,27,32,33, including face-to-face/home visits, direct mail/telephone, and advertisement. The other five teams used only face-to-face/home visits25,28,29,30,31; another used only direct mail/telephone23. Eleven studies reported the selected outcomes based on the inclusion criteria, including knowledge, belief/attitude, calling 911 or EMS, mortality, readmission, appropriate action/taking aspirin, coping behavior/anxiety, awareness, time of delay/seeking, and malnutrition risk. Only three studies reported the quality of instruments (Table 1).
The major conditions of the study were risk people and people with CAD/AMI—nine implemented interventions in the community24,25,27,28,29,30,31,32,33. Seven studies were conducted among 100% of older adults26,27,28,29,30,32,33, and four were mixed age group, of which over 80% was people aged 60 and older23,24,25,31. Eight studies included both sexes23,24,26,27,29,30,32,33, nine included mixed ethnicity23,24,25,27,28,30,31,32,33, and six reported income23,25,26,27,28,30. Their interventions were eight face-to-face/acronym/teaching24,25,26,27,29,31,32,33. Seven studies were conducted for longer than six months23,24,25,27,29,32,33. Nine studies were not prospectively registered protocols23,24,25,26,27,28,29,30,31. Intervention details included essential information to understand AMI, detect symptoms, and prevent delayed treatment; however, nine focused on overall symptoms or physical reactions23,24,25,26,27,28,30,31,33. Seven studies provided enough detailed interventions that researchers or readers could follow the intervention step by step for their practice24,26,28,29,30,32,33. Only three studies reported that they gave incentives to their participants28,29,31. Eight studies did not report activities for their control groups23,24,25,26,27,29,30,31. Six studies measured outcomes two times (pre-posttest)25,28,29,30,31,32,33. The number enrolled in each group ranged between 50 and 226,958 participants. Significant results were found in the knowledge of AMI30, AMI symptoms26,28, risk factors28, perception28,30, functional status33, hand grip33, aspirin taking26,27,29, and the number of calling 91125,26,27,29 (Table 2). Ten studies were level 1.c of evidence23,24,25,26,27,28,29,30,32,33, and critical appraisal ranked 8–12 for RCT (Table 3) and 6–9 for quasi-experimental study (Table 4). Finally, seven studies were graded as high level23,24,25,26,29,30,32 (Table 5).
Systematic review findings
The interventions found in this review were eight, including direct mail, community-based intervention, multi groups health education, innovative methods of using heart attack survival kits and firefighters, tailored educational/counseling intervention, structured education, and counseling intervention, tricked intervention promoting memory and concern, and nurse-based case management. Types of intervention were grouped, and intervention details and content were provided to guide program development and future study. Moreover, how to deliver and implement interventions was also provided for duplicating in future studies if needed.
Direct mail
The first intervention was a direct mail campaign in which a Brochure was mailed every two months. The information brochure provided detailed information on acute myocardial infarction symptoms and treatment in a neutral tone. The emotional message was designed to reduce the emotional response of fear, embarrassment, and bothering that could prevent or delay appropriate health behavior. The suggestion for decision-making was the family member's responsibility, not part of the patient's. Unfortunately, Meischke et al. did not provide details of the information or critical message in the brochure; only the concept and principle were found23.
Community-based intervention
A community-based intervention program was used to reduce out-of-hospital delays. The education message focused on chest pain and other ischemic symptoms, with action if symptoms persisted for 15 min or more. Multiple media channels were used to deliver the message to the general public physicians. Moreover, nurses, paramedics, and other healthcare providers helped deliver the message to high-risk groups. This health education program sequentially emphasized different themes, including general awareness of AMI symptoms and the need for rapid action, development of a Heart Attack Survival Plan, AMI in women, variability of AMI symptoms, bystander response to heart attacks, and use of 9–1-1 to reinforce the primary message24.
Multi-component strategies & groups health education
The multi-component strategies and groups of health education started with meeting focus groups of AMI patients, relatives, and health care professionals. This meeting found key points for AMI survival, symptom recognition, and the need to act fast by calling 911. The advice was to call 911 for ambulance transport to the hospital if experiencing symptoms persisted for 15 min or longer. This intervention included four strategies. First community organization, in which health professionals and leaders of their relevant organizations in each community constituted a local advisory group. Second, public education targeted all residents of the intervention communities with an 18-month program that included six themes. There was a general awareness of AMI symptoms and appropriate action, MI survival plan, women and MI, MI symptom recognition, bystander response to MI, and the importance of contacting EMS. Third, professional education included physicians, nurses, rehabilitation staff, ED staff, and ambulance staff. They should deeply understand AMI and prompt response in emergencies. Finally, the physician taught patients with a history of coronary heart disease (CHD) or CHD risk factors25.
The innovation method of using heart attack survival kit & firefighters
The program under the Heart Attack Survival Kit (HASK) project included a heart attack survival kit, red cardboard containing essential information, and a group discussion. A heart attack survival kit contained the following: eye-catching design and adhesive strips for permanent placement in the home; list of the warning signs of AMI; strong recommendation to call 911; strong recommendation to take an aspirin for chest pain; one 325 mg. uncoated adult aspirin, primary step for cardiopulmonary resuscitation (CPR), and space to write in medications/allergies and essential phone numbers. A red cardboard flyer shaped like a door hanger was provided with essential information about AMI and how to act when experiencing AMI. Finally, group discussion issues around cardiac emergencies with seniors in their communities were set26,27,29. This innovation program, delivered face-to-face by local firefighters, is designed to increase the utilization of 911 and self-administration of aspirin for seniors experiencing chest pain.
The step-by-step program started with passive-consent letters mailed to the homes of all eligible people in intervention areas (24,582 homes), indicating that a local firefighter would personally deliver a HASK soon unless the participant indicated on a self-addressed postcard that such a visit was not welcomed; the eligible individuals returned the postcard. Two weeks after the passive-consent letters were mailed, local firefighters delivered the kits to the homes of the remaining seniors in King County, Washington. More than 300 local firefighters were trained face-to-face by the staff of this study to discuss the contents of the HASK and to assess and respond to barriers to calling 911 and taking aspirin for chest pain29.
Tailored educational/counseling intervention
The Tailored educational/counseling intervention included essential information about the pathophysiology of AMI, Symptoms of AMI, the importance of quick responding, appropriate action in AMI situations, a rehearsal plan, and take-home questions. For the step-by-step intervention, all section was provided: (1) act in time, (2) what is a heart attack?, (3) the importance of rapid treatment of heart attack, (4) the ten most common symptoms of MI, (5) expectation and expected reaction to heart attack, (6) step to survival and rehearsing plan, (7) what factors increase one's risk? (8) take-home questions28.
Structured education and counseling intervention
The highlights of this intervention were specific details of intervention related to preventive behaviors and delaying treatment in AMI situations and a clear program direction by providing a step-by-step approach. This program included five steps. The first was educational and counseling intervention with details. Second, participants were given educational and counseling intervention, including information about typical and atypical symptoms of AMI, how symptoms may vary, and actions to take in the event of AMI symptoms. An advisory form was given to each participant after the intervention. The form, designed by the NHAAP, listed what the participant may feel if experiencing an evolving AMI, medication instructions, directions to call 911 and ask for an ambulance, and the location of the nearest 24-h emergency department. Participants who received the intervention were asked to place the advisory form in a prominent place in their homes. Third, the participants were asked to repeat the information to ensure comprehension. The fourth was that the intervention was delivered in a one-to-one session with the participant and lasted 30 to 60 min, depending on the participant's interest, questions, and comments. Finally, the participants recruited at the senior center were asked to refrain from discussing the study with others to avoid contamination between groups30.
Tricked intervention promoting memory and concern
One study applied a trick by using abbreviations with keywords to promote female older adult memory and concern. Because female older adults experienced prodromal and atypical/different symptoms of AMI with others, specific symptoms were provided, and acronyms were developed for easy memories. The deliberate misspelling of FACTSS was highlighted for the women to help them remember the long list of warning signs. Prodromal symptoms were FACTSS, which stood for fatigue, anxiety, chest discomfort, tummy (indigestion), shortness of breath, and sleeping difficulties. The MI symptoms were CURB, which represented chest sensation or pain, unusual fatigue, pain radiating back, jaw, or arm pain, and breathing difficulties. The health education matters of your heart using the acronym FACTSS & CURB was applied among female older adults. The program was delivered in the community to groups of women. A script for the researchers to follow provided consistent information to each group. Immediately after the presentation, the subjects took the post-test, the same as the pre-test31.
A nurse-based case management
The nurse-based intervention is complex, combining components from case management and disease management. Case management focuses on individual care problems of older adults and facility of care coordination; however, disease management pays attention to identifying problems regarding managing AMI symptoms and providing information and individual education. The case-management intervention consisted of a nurse-based follow-up for one year, including home visits and telephone calls. Key elements of the intervention were to detect problems or risks and to give advice regarding a wide range of aspects of disease management, such as symptom management and medication use. A nurse-based case management program includes three steps. First was the initial session, after giving informed consent (so-called “heart book”), followed by home visits. The home visit was arranged 7 to 14 days after discharge, and telephone calls and telephone interviews (at least every three months) were performed. The study nurse assesses the risk level during the first home visit based on compliance, social network, and comorbidities. The higher the risk level, the more contacts (telephone and home visits) were arranged by the study nurse. Finally, the final assessment after 12 months was conducted32. However, another study was a case-management intervention consisting of a nurse-based follow-up for three years. This intervention included home visits and telephone calls. The case-management intervention consisted of a three-year nurse-based follow-up, including home visits and telephone calls, risk management, and symptom management33.
Meta-analysis findings
The meta-analysis showed that people receiving a Kit via home by an Emergency Medical Technician or via direct mail or delivered face-to-face by local firefighters had a higher odd of calling 911 and taking aspirin than those without any intervention (OR 2.55, 95% CI 1.01–6.44) as shown in Fig. 2. Publication bias was visually assessed using Begg’s funnel plots and statistically assessed with Egger’s test. Based on publication bias analysis, this figure visually indicates the skewness of the effect sizes observed, as shown in Fig. 3. In addition, the left-sided test for funnel plot asymmetry using Egger’s regression test was significant (p = 0.043), supporting the conclusion that significant publication bias was present.

Forest plot for the odd ratios of calling 911 and taking aspirin among AMI patients with and without an intervention: The midpoint of each line illustrates the odds ratio; the horizontal line indicates the confidence interval, and the diamond shows the pooled odds ratio. The red and gray vertical lines indicate the overall effect-size and null-effect values, respectively.

Funnel plot of effect sizes included in the meta-analyses for calling 911 and taking aspirin among AMI patients with and without intervention.
The meta-analysis showed no association between people receiving home-based and nurse-based interventions and those without any intervention regarding time to first unplanned readmission or death (HR 0.94, 95% CI 0.77–1.11), as shown in Fig. 4. Publication bias was visually assessed using Begg’s funnel plots and statistically assessed with Egger’s test. Based on publication bias analysis, this figure provides no visual indication of the skewness of the effect sizes observed, as shown in Fig. 5. The left-sided test for funnel plot asymmetry using Egger’s regression test was non-significant (p = 0.604), supporting the conclusion that non-significant publication bias was present.

Forest plot for the hazard ratios of affecting time to first unplanned readmission or death among AMI patients with and without an intervention: The midpoint of each line illustrates the hazard ratio; the horizontal line indicates the confidence interval, and the diamond shows the pooled hazard ratio. The red and gray vertical lines indicate the overall effect-size and null-effect values, respectively.

Funnel plot of effect sizes included in the meta-analyses for affecting time to first unplanned readmission or death among AMI patients with and without intervention.
Finally, the meta-analysis showed no association between people receiving community-based and direct mail intervention and those without any intervention regarding delay time to ER (Standardized mean difference = 0.21, 95% CI − 0.20 to 0.62), as shown in Fig. 6. Publication bias was visually assessed using Begg’s funnel plots and statistically assessed with Egger’s test. Based on publication bias analysis, this figure visually indicates the skewness of the effect sizes observed, as shown in Fig. 7. The left-sided test for funnel plot asymmetry using Egger’s regression test was non-significant (p = 0.441), supporting the conclusion that no significant publication bias was present.

Forest plot for the standardized mean difference of time delay to ER among AMI patients with and without an intervention: The midpoint of each line illustrates the mean difference; the horizontal line indicates the confidence interval, and the diamond shows the pooled mean difference. The red and gray vertical lines indicate the overall effect-size and null-effect values, respectively.

Funnel plot of effect sizes included in the meta-analyses for time delay time to ER among AMI patients with and without intervention.
Discussion
This comprehensive systematic review and meta-analysis synthesized evidence from 11 studies conducted in the USA and Germany focusing on the effectiveness of intervention/health education on health outcomes. Eight of eleven studies were conducted before 2012. It was possible that, in the US and Germany, there are public health policies to call 911 to promote community awareness of emergency health conditions such as AMI and stroke and the need to call 911 since 2000, both at the public and school levels34,35. However, the atypical presentation of AMI remains an important issue, especially in older adults and women, to prevent delayed diagnostics and treatments7,9,28. Moreover, although morbidity and mortality rates are declining for AMI in most high-income countries, it is rising at an alarming pace for low to middle-income countries10. Therefore, AMI intervention for older adults is still needed, mainly conducted on low-middle incomes.
The number of participants in each group ranged from 50 to 226,958 participants. The range is relatively broad because some interventions were conducted as a national community intervention or national campaign23,25,27. However, some interventions focused on the individual level28,30,31. This systematic review focused on older adults’ studies; most were conducted among women. Older adults and women are areas of concern since they both were the significant groups experiencing atypical presentation, delay in seeking treatment, and result in a high mortality rate7,9,28.
The meta-analysis found that people who received any of the three interventions, including receiving a Kit via home by an Emergency Medical Technician, via direct mail, or delivered face-to-face by local firefighters, were more likely to call 911 and take aspirin in an emergency than those who did not receive any intervention. Specifically, the odds of calling 911 and taking aspirin were 2.55 times higher for those who received an intervention, with a 95% confidence interval ranging from 1.01 to 6.44, which is similar to the findings of previous studies36,37,38. However, the study conducted by Mikulík et al. and Fogle et al. observed that the readiness of older adults to call 911 in response to a stroke improved when they were exposed to a video-based educational program34,39. In addition, a low-intensity educational campaign, which involved donated advertising media to increase stroke awareness, was unsuccessful. Then, the effectiveness of using different pathways should be explored.
This meta-analysis suggests that providing people with a Kit and information about emergency services can effectively encourage them to seek help in an emergency26,2729. However, it is essential to note that the effectiveness of these interventions may vary depending on the specific context and population being studied. Overall, the findings of this meta-analysis can be helpful for healthcare professionals, emergency responders, and policymakers in designing effective interventions to promote prompt and appropriate responses to emergencies.
Interestingly, many interventions with different pathways were applied to promote knowledge, decision-making, appropriate action, and time to seek treatment; however, based on the meta-analysis, only the odds of calling 911 and taking aspirin were improved. This result might be because the intervention may suit general people but not fit older adults. Older adults own specific characteristics regarding the aging process and their socio-demographic status. First, their aging process and pathogenesis limit older adults’ skills in perceiving information, learning, and understanding compared to younger adults40,41. Because the aging process and its pathogenesis limit older adults’ vision, hearing, attention, concentration, and ability to remember information, providing health education or interventions for this group must adhere to the limitations and older adults’ requirements42,43. As older adults had reduced memorization ability, the program was designed to have practices to enhance skills and ability to manage the symptoms independently. Moreover, repetitive self-practice would enable practitioners to learn effectively, understand reasons, and achieve sustainable learning43. Teaching procedures and periods were not too long. The stimuli transmitted through the five senses, namely, the ears, eyes, nose, tongue, and skin, produce more learning outcomes than stimuli transmitted through one sense only. The practice helped turn the abstract into concrete for better understanding41,43.
Second is their socio-demographic status. Older adults have limitations regarding their education, so this condition is an obstacle in accessing, receiving, and understanding health information in taking care of themselves. These include poor reading and listening skills and fear of being scolded by service providers. Their limitations hindered these people from essential and updated health information, so less behavioral modification and appropriate action in illness were found in this age group44. Nilnate et al. found that older adults have low to moderate health literacy scores45. The limitation of education plus the deterioration of their ears and eyes affect self-care management skills and competency for accessing, understanding, and reporting health knowledge. Therefore, teaching older people should take a short time, be divided into sessions, and consist of explanations and practices. Practices must be simple and uncomplicated in a suitable place, with repeated teaching and training sessions. The teaching style must consider the context and culture of older people while using the proper media, large visible text, simple language, and age-friendly colors to be seen easily and clearly. In addition, teaching materials should be available for older people to take home and review41,42,43. Participation in the teaching and practice process would promote learning, memorization, and practicing with confidence40,43. All principles of giving health education to older adults should be considered when developing interventions to solve the delay in seeking treatment in acute myocardial infarction situations.
Limitations
Four limitations were found in this study. First, some selected outcomes were impossible for meta-analysis; only three variables were included. Second, publication bias was also found in this study; this should be aware when applying results. Third, Egger’s test can lead to misleading results when the number of studies is small; this concern should be considered when interpreting the results. Finally, all studies were from only two countries (USA and Germany); results from this systematic review would limit especially details of intervention from the narrative method because their interventions were developed based on the context of study settings. Then, only the principles should be applied.
Conclusion and recommendation
Older adult is a significant group experiencing AMI and delaying treatment, causing a high mortality rate. Factors related to their delay differ from other age groups, and their specific characteristics and aging process limit them from recognizing their symptoms and learning new information. This study revealed that the included interventions might not suit and be adequate for older adults to survive the AMI situation because their specific characteristics and aging process would not be a concern when developing intervention. Therefore, specific interventions related to their limitations and needs should be considered when developing interventions for future study and practice.
Data availability
The datasets generated and/or analyzed during the current study are not publicly available due to prohibited laws (and/or rules, regulations, and contracts). However, they are available from the corresponding author upon reasonable request.
References
World Health Organization. Aging and Health. Retrieved April 4, 2023, from https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (2022).
American Heart Association. 2023 Heart Disease and Stroke Statistics Update Fact Sheet. 2023 Statistics Update—At-a-Glance Statistics. Retrieved April 4, 2023, from https://professional.heart.org/en/science-news/-/media/453448D7D79948B39D5851D1FF2A0CFE.ashx (2023).
Limpawattana, P. Geriatric Syndromes and Interesting Health Issues (Geriatric Medicine Department of Internal Medicine Faculty of Medicine Khon Kaen University, 2018).
Assantachai, P. Concerted actions toward healthy aging in ASEAN countries. Siriraj Medical Journal 73(9), 633–634. https://doi.org/10.33192/Smj.2021.81 (2021).
De Luca, G., Suryapranata, H., Ottervanger, J. P. & Antman, E. M. Time delay to treatment and mortality in primary angioplasty for acute myocardial infarction: Every minute of delay counts. Circulation 109(10), 1223–1225. https://doi.org/10.1161/01.CIR.0000121424.76486.20 (2004).
Hanifi, N., Rezaee, E. & Rohani, M. Time-to-treatment and its association with complications and mortality rate in patients with acute myocardial infarction: A prospective cohort study. J. Emerg. Nurs. 47(2), 288-298.e4. https://doi.org/10.1016/j.jen.2020.05.013 (2021).
Sweis, R.N., & Jivan, A. Acute Myocardial Infarction (Northwestern University Feinberg School of Medicine, 2022). Retrieved April 8, 2023, from https://www.msdmanuals.com/professional/cardiovascular-disorders/coronary-artery-disease/acute-myocardial-infarction-mi#top.
Tsao, C. W. et al. Heart disease and stroke statistics—2023 update: A report from the American Heart Association. Circulation 147(8), e93–e621. https://doi.org/10.1161/CIR.0000000000001123 (2023).
Khan, I. A., Karim, H. R., Panda, C. K., Ahmed, G. & Nayak, S. Atypical presentations of Myocardial Infarction: A systematic review of case reports. Cureus 15(2), e35492. https://doi.org/10.7759/cureus.35492 (2023).
Beza, L., Leslie, S. L., Alemayehu, B. & Gary, R. Acute coronary syndrome treatment delay in low to middle-income countries: A systematic review. Int. J. Cardiol. Heart Vasc. 35, 100823. https://doi.org/10.1016/j.ijcha.2021.100823 (2021).
Huriani, E., Wahid, I., Machmud, R. & Abdullah, K. L. Patient education strategies among patients with Acute Myocardial Infarction: A systematic review. Open Access Maced. J. Med. Sci. 10, 405–12 (2022).
Banharak, S., Prasankok, C. & Lach, W. H. Factors related to a delay in seeking treatment for acute myocardial infarction in older adults: An integrative review. Pac. Rim Int. J. Nurs. Res. 24(4), 553–568 (2020).
Lastre-Amell, G. et al. A Systematic Literature Review of Treatment Costs for Patients with Acute Myocardial Infarction. Retrieved April 17, 2023, from https://www.lareferencia.info/vufind/Record/CO_1d9ea7de8bca2c8e0ff60f01aabea068 (2019).
Toshima, T. et al. Unmet needs for emergency care and prevention of prehospital death in acute myocardial infarction. J. Cardiol. 77(6), 605–612. https://doi.org/10.1016/j.jjcc.2020.11.013 (2021).
Hoschar, S., Albarqouni, L. & Ladwig, K. H. A systematic review of educational interventions aiming to reduce prehospital delay in patients with acute coronary syndrome. Open Heart 7(1), e001175. https://doi.org/10.1136/openhrt-2019-001175 (2020).
Wang, L. Y. T. et al. Health information needs and dissemination methods for individuals living with ischemic heart disease: A systematic review. Patient Educ. Couns. 108(107594), 1–8. https://doi.org/10.1016/j.pec.2022.107594 (2023).
Aromataris, E., & Munn, Z. JBI Manual for Evidence Synthesis. Retrieved April 24, 2023 from https://synthesismanual.jbi.global. https://doi.org/10.46658/JBIMES-20-01 (2020).
Aromataris, E., & Munn, Z. JBI Manual for Evidence Synthesis. Retrieved October 2, 2023 from https://jbi.global/sites/default/files/2019-05/JBI-Levels-of-evidence_2014_0.pdf. (2019).
Tufanaru, C., Munn, Z., Aromataris, E., Campbell, J. & Hopp, L. Chapter 3: Systematic reviews of effectiveness. In Joanna Briggs Institute Reviewer’s Manual (eds Aromataris, E. & Munn, Z.) (The Joanna Briggs Institute, 2017).
Tufanaru, C., Munn, Z., Aromataris, E., Campbell, J. & Hopp, L. Chapter 3: Systematic reviews of effectiveness. In JBI Manual for Evidence Synthesis (eds Aromataris, E. & Munn, Z.) (JBL Global, 2020).
Schünemann, H., Brożek, J., Guyatt, G. & Oxman, A. GRADE Handbook. Retrieved April 8, 2023, from https://gdt.gradepro.org/app/handbook/handbook.html?fbclid=IwAR04O97yy (2013).
DerSimonian, R. & Laird, N. Meta-analysis in clinical trials revisited. Contemp. Clin. Trials 45(Pt A), 139–145. https://doi.org/10.1016/j.cct.2015.09.002 (2015).
Meischke, H. et al. “Call fast, Call 911”: A direct mail campaign to reduce patient delay in acute myocardial infarction. Am. J. Public Health 87(10), 1705–1709 (1997).
Hedges, J. R. et al. Impact of community intervention to reduce patient delay time on the use of reperfusion therapy for acute myocardial infarction rapid early action for coronary treatment (REACT) trial. Acad. Emerg. Med. 7(8), 862–872 (2000).
Luepker, R. V. et al. Effect of a community intervention on patient delay and emergency medical service use in acute coronary heart disease: The Rapid Early Action for Coronary Treatment (REACT) Trial. J. Am. Med. Assoc. 284(1), 60–67 (2000).
Meischke, H., Eisenberg, M., Schaeffer, S. & Henwood, D. K. The heart attack survival kit’ project: An intervention designed to increase seniors’ intentions to respond appropriately to symptoms of acute myocardial infarction. Health Educ. Res. 15(3), 317–326 (2000).
Meischke, H., Diehr, P., Rowe, S., Cagle, A. & Eisenberg, M. Evaluation of a public education program delivered by firefighters on early recognition of a heart attack. Eval. Health Prof. 27(1), 3–21. https://doi.org/10.1177/0163278703261199 (2004).
Lefler, L. L. C. Increasing Accuracy of Risk Perceptions and Knowledge of Myocardial Infarction Symptoms Among Older, Black, and White High-Risk Women. A dissertation submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy, University of Arkansas for Medical Sciences (2006).
Meischke, H., Diehr, P., Rowe, S., Cagle, A. & Eisenberg, M. A community intervention by firefighters to increase 911 calls and aspirin use for chest pain. Acad. Emerg. Med. 13(4), 389–395. https://doi.org/10.1197/j.aem.2005.10.021 (2006).
Tullmann, D. F., Haugh, K. H., Dracup, K. A. & Bourguignon, C. A randomized controlled trial to reduce delay in older adults seeking help for symptoms of acute myocardial infarction. Res. Nurs. Health 30(5), 485–497. https://doi.org/10.1002/nur.20245 (2007).
Kalman, M. et al. Education to increase women’s knowledge of female myocardial infarction symptoms. J. N. Y. State Nurse Assoc. 43, 11–16 (2013).
Meisinger, C. et al. Effects of a nurse-based case management compared to usual care among aged patients with myocardial infarction: Results from the randomized controlled KORINNA study. BMC Geriatr. 13(1), 1–10 (2013).
Kirchberger, I. et al. Effects of a 3-year nurse-based case management in aged patients with acute myocardial infarction on rehospitalization, mortality, risk factors, physical functioning, and mental health. A secondary analysis of the randomized controlled KORINNA study. PLoS ONE 10(3), e0116693. https://doi.org/10.1371/journal.pone.0116693 (2015).
Fogle, C. C. et al. Public education strategies to increase awareness of stroke warning signs and the need to call 911. J. Public Health Manag. Pract. 14(3), e17–e22. https://doi.org/10.1097/01.PHH.0000316496.78282.47 (2008).
Zalenski, R. J. et al. National Heart Attack Alert Program position paper: Chest pain centers and programs for the evaluation of acute cardiac ischemia. Ann. Emerg. Med. 35(5), 462–471 (2000).
Eppler, E., Eisenberg, M. S., Schaeffer, S., Meischke, H. & Larson, M. P. 911 and emergency department use for chest pain: Results of a media campaign. Ann. Emerg. Med. 24(2), 202–208. https://doi.org/10.1016/s0196-0644(94)70131-8 (1994).
Cannuscio, C. C. et al. A strained 9–1-1 system and threats to public health. J. Community Health 41(3), 658–666. https://doi.org/10.1007/s10900-015-0142-x (2016).
Volevach, E., Maršálková, H., Bobek, J., Svobodová, V. & Mikulik, R. Educational program improved senior preparedness to call 911 as a response to stroke. J. Stroke Cerebrovasc. Dis. 30(11), 106047. https://doi.org/10.1016/j.jstrokecerebrovasdis.2021.106047 (2021).
Mikulík, R. et al. Calling 911 in response to stroke: No change following a four-year educational campaign. Cerebrovasc. Dis. 32(4), 342–348. https://doi.org/10.1159/000330339 (2011).
Reinhardt, L. Health Education for Older Adults. Retrieved August 27, 2022, from https://www.elitelearning.com/resource-center/nursing/health-education-for-older-adults/ (2015).
National Institute on Aging. Tips for Improving Communication with Older Patients. Retrieved August 27, 2022, from https://www.nia.nih.gov/health/tips-improvingcommunication-older-patients (2017).
Kececi, A., & Bulduk, S. Health education for the elderly. In Geriatrics (ed. Craig, A.) ISBN: 978-953-51-0080-5 (InTech, 2012). http://www.intechopen.com/books/geriatrics/health-education-for-elderly-people (2012).
Kim, M. Y. & Oh, S. Nurses’ perspectives on health education and health literacy of older patients. Int. J. Environ. Res. Public Health 17, 6455–6466. https://doi.org/10.3390/ijerph17186455 (2020).
Sittikan, S. & Jongudomkarn, D. Barriers to access of primary healthcare by people with low income in urban communities: a qualitative study. J. Nurs. Sci. Health 43(1), 19–29 (2020).
Nilnate, W., Hengpraprom, S. & Hanvoravongchai, P. Level of health literacy in Thai elders Bangkok, Thailand. J. Health Res. 30(5), 315–321 (2016).
Acknowledgements
We would like to thank those who contributed to this study. Special thanks are extended to the librarian who supports search statement development and the searching process. We thank our colleagues for always supporting us in finding the full paper so we received all we needed. Lastly, special appreciation is extended to the principal researchers we tried to contact to provide us with statistics essential in generating meta-analysis.
Funding
This research was supported by the Gerontological Nursing Research Cluster, Faculty of Nursing, Khon Kaen University, Thailand (Grant Number GNRC63-001). Appreciation is extended to this research cluster and organization for making this research possible.
Author information
Authors and Affiliations
Contributions
All authors have agreed on the final version and meet at least one of the following criteria (recommended by the ICMJE: http://www.icmje.org/recommendation/): Substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; Drafting the article or revising it critically for important intellectual content.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Banharak, S., Metprommarat, A., Mahikul, W. et al. Effectiveness of acute myocardial infarction interventions on selected outcomes among community dwelling-older adults: a systematic review and meta-analysis. Sci Rep 13, 18538 (2023). https://doi.org/10.1038/s41598-023-45695-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-45695-y
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
