
Abstract
This study aimed to evaluate the accuracy of digital dental impressions obtained by intraoral scanning (IOS) for partial edentulous patients with maxillary defects by comparing them with conventional impression techniques. Ten subjects underwent an experimental procedure where three ceramic blocks were affixed to the healthy palate mucosa. Digital dental impressions were captured using IOS and subsequently imported into software. Conventional impressions obtained by silicone rubber were also taken and scanned. Linear distance and best-fit algorithm measurements were performed using conventional impression techniques as the reference. Twenty impressions were analyzed, which included 30 pairs of linear distances and 10 best-fit algorithm measurements. Regarding linear distance, paired two-sample t-test demonstrated no significant differences between IOS and model scanning in groups A and C, whereas significant differences were found in group B (P < 0.05). Additionally, ANOVA revealed significant differences among the groups (P < 0.05). No significant differences were found for the best-fit algorithm measurement of the dentition. IOS can provide accurate impressions for partial edentulous patients with maxillary defects and its accuracy was found to be comparable with conventional impression techniques. A functional impression may be needed to ensure accurate reproduction of soft and hard tissues in defect or flap areas.
Similar content being viewed by others


Introduction
Making dental impressions, which is usually considered to be the first step for dental procedures, is necessary in most clinical settings1. In clinical scenarios, conventional dental impressions obtained by alginate or silicone rubber were applied to measure the occlusal relationship and dentition. However, this method is associated with several drawbacks, including the significant time and cost involved in model fabrication, impression-taking, and model storage2. Furthermore, research has shown that conventional dental impressions are prone to inaccuracies due to factors such as potential distortion and expansion of gypsum casts, as well as changes in shape over time when impressions are sent to dental laboratories3,4,5. Digital dental impressions, which have been gradually applied in clinical practice, have emerged as a promising solution to the limitations of traditional dental impressions. Compared to conventional methods, digital dental impressions offer several advantages, such as real-time imaging and evaluation, less requirement for materials, and improved cost-effectiveness and communication6. Studies have shown that their accuracy can be acceptable in clinical settings compared with conventional ones7,8,9,10.
In general, digital dental impressions can be acquired either by scanning the conventional impressions or by IOS with an intraoral scanner. The accuracy of dental extraoral laboratory scanners has been evaluated in previous studies11,12. Data acquired using IOS is comparable to that obtained using conventional methods for single crowns and partial fixed prostheses13,14. Nevertheless, researchers have reported that extraoral scanners demonstrated higher accuracy measurements for the cross-arch measurement15. In addition, studies have found that prosthesis fabricated from model scanning has lower average discrepancies than those produced using IOS16.
Maxillary tumors can result in significant loss of hard and soft tissues, leading to maxillary defects and decreased quality of life for patients. Therefore, treatment of the maxillary defects should focus on minimizing potential problems and preserving quality of life. The fabrication of a maxillary obturator can help to address these issues, and reports have shown that patients experience improved satisfaction with the use of a maxillary obturator17,18. For partial edentulous patients with maxillary defects, conventional dental impressions using silicone rubber or alginate are still widely used in clinical practice due to their acceptable accuracy and feasibility19,20. Nonetheless, these patients may experience difficulties with mouth opening due to scar contracture or temporomandibular joint disease, which can impact the accuracy and feasibility of conventional dental impressions. Moreover, defective tissues of the upper palate and the penetration between the oral cavity and nasal cavity may cause materials to enter the nasopharynx cavity, bringing pain and discomfort to patients. Accordingly, making dental impressions for this specific clinical population, partial edentulous patients with maxillary defects, could be an enormous challenge for dentists during the clinical practice of dentistry.
With the rapid advancement of digital technology in dentistry, practitioners can now obtain 3D scans of hard and soft tissues and occlusion relationships using intraoral scanners. This method eliminates the drawbacks of conventional dental impressions and enables practitioners to digitally evaluate and design the maxillary obturator. Compared to conventional impression techniques, the use of IOS simplifies the workflow and avoids time consumption and potential deviations21. Trueness, which describes the congruence between a prototype STL dataset and a control STL dataset, is considered a crucial factor in determining the ability of IOS to capture dental impressions with high quality22,23.
The accuracy of IOS has been reported to decrease when scanning larger areas compared with a short span24,25. Therefore, the aim of the present study was to assess the accuracy of digital dental impressions obtained from IOS for partial edentulous patients with maxillary defects by comparing the linear distance and best-fit algorithm measurements with those obtained from conventional impression techniques in a quantitative manner.
Materials and methods
The present study was approved by the Institutional Review Board of the First Affiliated Hospital of Fujian Medical University, Fujian, PR CHINA (No. MRCTA, ECFAH of FMU [2020] 430). Written informed consents were obtained from ten partial edentulous patients with maxillary defects in full accordance with the ethical principles of the World Medical Association Declaration of Helsinki (version 2008). The following inclusion criteria were applied: (1) age ≥ 18 years; (2) mild to moderate limitation of mouth opening; (3) inability or refusal to undergo implant surgery due to physical conditions, but required prosthetic restoration. The excursion criteria were (1) severe mouth opening limitation; (2) tooth mobility > I.
Placement of ceramic blocks
Before the experiment, the dentition and mucosa of the subjects were isolated and dried using an air syringe, and cottons. To protect the mucosa of the defect areas, vaseline gauze was used. Three customized zirconia ceramic blocks (6 mm × 6 mm × 3 mm) were attached to the healthy palate mucosa of residual dentition and the defect area using medical tissue glue (Medical Tissue Glue, B. Braun Corp, China). The ceramic block at the anterior position of the residual dentition was marked as A block, the block placed near the defect area or flap area was labeled as B block, and the ceramic block at the posterior of the residual dentition was marked as C block.
Intraoral scanning
Each patient received both conventional impression-taking and IOS. The digital dental impression of IOS was before the conventional impression techniques procedure. Digital dental impressions were obtained using an intraoral scanner (TRIOS color, 3Shape, Denmark) by an experienced dentist. Starting from the occlusal-palatal side of posterior teeth in the first quadrant, the intraoral scanner was turned to the buccal side of the teeth in the second quadrant and then returned to the first quadrant. The mucosa of each patient was also scanned, and the scan data was saved and exported in the STL format (Figs. 1, 2).

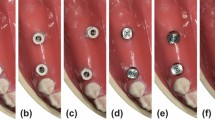
Images of the maxillary of subjects after ceramic blocks were pasted.

Digital dental impressions obtained by intraoral scanning.
Conventional impression techniques
For each participant, maxillary silicone rubber impressions (Meijiayin elastomer impression material type III, HuGe, China) were taken using full-arch metal stock impression trays in accordance with the manufacturer’s instructions under the same conditions. The dental impressions were then poured with dental stone (Die-stone, Heraeus Kulzer, USA) by the same experienced dentist. After 40 min, impression trays were removed from the stone models. The stone models were then scanned by using a desktop scanner (E2 lab scanner, 3shape, Denmark) and saved in STL format (Figs. 3, 4).

Maxillary plaster dental impressions obtained by silicone rubber using conventional impression techniques.

Digital dental impressions obtained by model scanning.
Measurement procedure
The scan files of IOS and model scanning were converted to three-dimensional (3D) images by a reverse engineering software program (Geomagic Wrap, Raindrop Geomagi, USA) for matching and data measurement. Two measurements were performed for each subject, the linear distance between each ceramic block and the corresponding tooth point and the best-fit algorithm measurement. The linear distance was defined as the distance between the central point of each ceramic block and the corresponding point of the residual teeth (Fig. 5). Three linear distances between ceramic blocks A, B, and C were measured. The measurements of linear distance between two ceramic blocks were the Euclidean distance calculated based on the data obtained in the software. The best-fit alignment measurement utilizes an iterative closest point algorithm to superimpose two meshes and minimize the difference between the two clouds of points and iteratively revise the transformation needed to minimize an error metric.26 The entire dataset obtained by IOS and conventional impression techniques was aligned to generate deviation maps containing information including median and average deviation and analyzed using the best-fit alignment method on the software (Fig. 6). Moreover, the dentition of each group of models was trimmed along the tooth neckline for further statistical analysis in the software (Fig. 7). The accuracy of the entire dataset best-fit algorithms alignment method has been demonstrated in the literature27.

Linear distance between ceramic block and corresponding tooth.

Models obtained by intraoral scanning and conventional impressions superimposed with best-fit algorithm.

Best-fit algorithm measurement of maxillary dental arch.
Statistical analysis
Data analysis was performed using SPSS 26.0 software (IBM SPSS Statistics, IBM, USA). Statistical analysis was performed using the Shapiro–Wilk test for normal distribution and Levene’s test for homogeneity of variance. A paired two-sample t-test was applied to assess the differences in the linear distance between the ceramic block and the corresponding point of the residual teeth in each group. The differences in linear distance between IOS and conventional impression techniques in the three blocks of each patient were recorded. Subsequently, the differences in three groups were compared using one way ANOVA test to evaluate the accuracy of digital impressions, and the least significant difference test was applied for further comparison in pairs. The best-fit algorithm measurement of the dentition was assessed using the Kolmogorov–Smirnoff test. In all statistical analyses, the level of significance was set to α = 0.05.
Ethics approval
The study protocol was approved by the Institutional Review Board of the First Affiliated Hospital of Fujian Medical University, Fujian, PR CHINA (Approval Number MRCTA, ECFAH of FMU [2020]430).
Informed consent
Interventions were undertaken with the understanding and written informed consent of each subject. The patients were treated in full accordance with ethical principles, including the World Medical Association Declaration of Helsinki (version 2008).
Results
Twenty digital dental impressions of ten eligible subjects were analyzed, which included 30 pairs of linear distances (IOS and model scanning) and 10 best-fit algorithm measurements of the dentition.
Linear distance
Overall, significant differences were found between IOS and conventional impression techniques in terms of the linear distance. Regarding the linear distance within each group, the paired t-test revealed no difference between IOS and conventional impression techniques in ceramic blocks of group A and group C, while significant differences were observed for group B (P < 0.05), indicating the deviations in digital dental impressions obtained by IOS compared to the conventional impression techniques in this area (Table 1). Moreover, the results of ANOVA showed that there were differences among groups (P < 0.05), indicating that the position of the ceramic block had an impact on the accuracy of digital dental impressions (Table 2). After using the least significant difference test, the results showed that there were significant differences in the linear distance of IOS and conventional impression techniques between group B and group C (P < 0.05), while no differences were found when comparing to group A, which demonstrated that ceramic block A had a relatively stable position with less displacement during the process of making dental impressions (Table 3).
Best-fit algorithm
The results from the best-fit algorithm measurement of the two groups showed that errors were basically concentrated in the maxillary defect areas (> 2 mm) (Fig. 6). The results of the Kolmogorov-Smirnoff test for residual dentition showed that there was no significant difference between IOS and conventional impression techniques (P = 0.18) (Table 4) (Fig. 7), indicating the dentition of digital dental impressions obtained by IOS can be acceptable in clinical settings.
Discussion
The present study was performed to evaluate the accuracy of IOS for partial edentulous patients with maxillary defects. In the present comparative clinical study, the feasibility of making dental impressions for partial edentulous patients with maxillary defects using IOS was illustrated and assessed, which provided references for clinical restorative treatment. To our knowledge, this is one of the first investigations which focus on digital dental impressions obtained by an intraoral scanner for this specific clinical population.
The accuracy of dental impressions is a critical step in ensuring predictable treatments and long-lasting restorations28. The accuracy of digital dental impressions has been demonstrated in several studies7,8,9,10. In clinical scenarios, three methods are currently used to obtain digital dental impressions, including IOS, extraoral model scanning, and cone beam compute tomography (CBCT). Trueness and precision are two components of accuracy, and this study assessed only the trueness of IOS as the evaluation of precision would require comparison between different datasets obtained using the same method. However, due to the discomfort associated with traditional dental impressions for partial edentulous patients with maxillary defects, this study avoided taking multiple impressions for the same patient. The accuracy of the model scanning has been verified and the silicone rubber impression material demonstrated excellent dimensional stability, detail reproducibility, and gypsum compatibility29. In addition, the comparison between the IOS and extraoral model scanning of conventional impression techniques has been applied in many different scenarios in previous studies30,31,32,33. On the other hand, CBCT was excluded from this study due to radiation and accuracy concerns.
Although widely used in the clinical practice of dentistry, conventional impression techniques obtained with silicone material may introduce inaccuracies due to the contraction of the impression material and expansion of the stone. In addition, this method is associated with several drawbacks, including the significant time and cost involved in model fabrication, impression-taking, and model storage2. With the rapid advancement of digital technology, the digital workflow with the help of IOS avoids the time consumption and potential deviations of impression preparation and gypsum pouring using conventional dental impression techniques. In addition, it is convenient for clinicians to re-scan and make up for the faults that occurred in the procedures of making impressions, while it might need to remake a new one if there is something wrong with conventional impression techniques. However, the accuracy of digital impressions obtained by IOS in the soft tissue of the maxillary remains controversial in the literature33. Nevertheless, when utilized appropriately, IOS can provide clinicians with valuable feedback, particularly regarding impression quality and the overall shape and geometry of preparations34.
To assess the accuracy of IOS, various measurement schemes have been adopted, mainly including linear distance and best-fit algorithm measurement35,36,37. In this study, best-fit algorithm measurement was selected for analysis due to its ability to reduce error compared to linear distance by using larger data sets and better detecting impression deviations. Moreover, this approach can visualize superposition results with the help of distance maps and evaluate the differences more intuitively. However, some research has suggested that the best-fit algorithm is not widely applicable due to its potential to automatically correct large differences in one region and cause registration errors in other areas, especially in large areas or soft tissues38. In addition, the different alignment protocols and versions among software may influence the results of best-fit algorithm measurement39. Linear distance was also used to measure the accuracy of complete dentition obtained by IOS in the literature10. Therefore, linear distance and best-fit algorithm measurement were used in this study to improve the reliability.
Previous studies have shown that applying markers on the mucosa can aid in the acquisition of digital dental impressions40. Several kinds of artificial markers have been applied to assess the evaluation of the accuracy of IOS for digital dental impressions. For example, a previous study fixed 4 metal spheres with composite aid to the mandibular teeth10. Other potential approaches include drawing irregular shapes and lines with a mixture of pressure-indicating paste and zinc oxide-eugenol cement41. In addition, Fang et al. injected flowable composite resin to six different sites on the hard palate and light-polymerized the resin to facilitate the application of IOS to make digital impressions of edentulous jaws with a broad palate42. In this study, to analyze the influence of mobility of soft tissue and tooth morphology on the accuracy of IOS, three customized zirconia ceramic blocks of 6 mm × 6 mm × 3 mm were placed at the anterior teeth, posterior teeth, and near the defect or flap area according to specifications. After cutting and sintering, the edges of the ceramic blocks were polished to ensure an error of less than 0.1 mm. Due to the lack of structure that needs to be recognized by an intraoral scanner, bonding ceramic blocks instead of resin or metal spheres can assist in matching generated images and reducing operation time during IOS by providing structure to be recognized by the intraoral scanner. On the other hand, the center of the ceramic block can be used for subsequent measurement and data analysis.
Paired t-test results showed no difference between group A and group C, while significant differences were observed in group B. This may be due to the ceramic block in group B being close to a defect or flap area with large mobility, resulting in deviations in digital dental impressions obtained by IOS compared to conventional impression techniques. In addition, the least significant difference test showed differences between group B and group C, while no differences were found when comparing with group A. This may be due to the ceramic block in group A being located on the palatal mucosa near the anterior teeth, which had a relatively stable position with less displacement during the process of making dental impressions. In contrast, the ceramic blocks in group C located near the hard-soft palate junction area may change position with the movement of the mucosa during operation. The inconspicuous change superimposed with displacement of the ceramic block in group B led to the differences in the accuracy of IOS between group B and group C. The results of the Kolmogorov–Smirnoff test for residual dentition indicated the digital dental impressions obtained by IOS can be acceptable in clinical settings. Therefore, the accuracy of digital dental impressions obtained by IOS can meet requirements for the fabrication of scaffolds, retainers and small connectors. However, results from best-fit algorithm measurement showed that errors were basically concentrated in the maxillary defect areas (> 2 mm) (Fig. 6). Therefore, when using digital dental impressions for a mental scaffold obturator in clinical practice, a functional impression should be combined to accurately reproduce the shape of soft and hard tissues in defect areas under functional status after scaffold and tooth setting are completed on the digital models to complete the fabrication of obturator.
This study has several limitations. First of all, using the model scanning of rubber dental impressions obtained by silicone material may introduce inaccuracies due to the contraction of the impression material, expansion of the stone, and resolution limitations of the non-industrial model scanner. In addition, due to the discomfort of partial edentulous patients with maxillary defects when making conventional dental impressions, the precision of IOS was not evaluated in this study. Finally, it must be taken into account that the sample size was relatively small, and future clinical research with a larger sample size should better analyze the potential distortions between IOS and conventional impressions and assess the feasibility and efficacy of IOS in clinical scenarios.
Conclusions
Based on the data analyzed in this study, the following conclusions were drawn:
-
1.
IOS can provide accurate digital dental impressions for partial edentulous patients with maxillary defects. The accuracy of IOS was found to be comparable to that of conventional impression techniques.
-
2.
The digital dental impressions obtained by IOS can be acceptable for the fabrication of scaffolds, retainers, and small connectors in clinical settings.
-
3.
To ensure accurate reproduction of soft and hard tissues in defect or flap areas, a functional impression may be needed in addition to the digital dental impression obtained by IOS.
Data availability
The data used or analyzed during the current study are available from the corresponding author upon reasonable request.
References
Walmsley, A. D., Pinsent, R. H. & Laird, W. R. Complete dentures: 1. Treatment planning and preliminary care. Dent. Update 18(6), 255 (1991) (257–260).
Lippold, C. et al. Methodological accuracy of digital and manual model analysis in orthodontics—A retrospective clinical study. Comput. Biol. Med. 62, 103–109 (2015).
Carrotte, P. V., Winstanley, R. B. & Green, J. R. A study of the quality of impressions for anterior crowns received at a commercial laboratory. Br. Dent. J. 174(7), 235–240 (1993).
Winstanley, R. B., Carrotte, P. V. & Johnson, A. The quality of impressions for crowns and bridges received at commercial dental laboratories. Br. Dent. J. 183(6), 209–213 (1997).
Millstein, P. L. Determining the accuracy of gypsum casts made from type IV dental stone. J. Oral Rehabil. 19(3), 239–243 (1992).
Punj, A., Bompolaki, D. & Garaicoa, J. Dental impression materials and techniques. Dent. Clin. N. Am. 61(4), 779–796 (2017).
Ender, A., Zimmermann, M., Attin, T. & Mehl, A. In vivo precision of conventional and digital methods for obtaining quadrant dental impressions. Clin. Oral Invest. 20(7), 1495–1504 (2016).
Nedelcu, R., Olsson, P., Nyström, I., Rydén, J. & Thor, A. Accuracy and precision of 3 intraoral scanners and accuracy of conventional impressions: A novel in vivo analysis method. J. Dent. 69, 110–118 (2018).
Abdel-Azim, T., Zandinejad, A., Elathamna, E., Lin, W. & Morton, D. The influence of digital fabrication options on the accuracy of dental implant-based single units and complete-arch frameworks. Int. J. Oral Maxillofac. Implants 29(6), 1281–1288 (2014).
Kuhr, F., Schmidt, A., Rehmann, P. & Wöstmann, B. A new method for assessing the accuracy of full arch impressions in patients. J. Dent. 55, 68–74 (2016).
Vlaar, S. T. & van der Zel, J. M. Accuracy of dental digitizers. Int. Dent. J. 56(5), 301–309 (2006).
Jacob, H. B., Wyatt, G. D. & Buschang, P. H. Reliability and validity of intraoral and extraoral scanners. Prog. Orthod. 16, 38 (2015).
Güth, J. F., Keul, C., Stimmelmayr, M., Beuer, F. & Edelhoff, D. Accuracy of digital models obtained by direct and indirect data capturing. Clin. Oral Invest. 17(4), 1201–1208 (2013).
Keul, C. et al. Fit of 4-unit FDPs made of zirconia and CoCr-alloy after chairside and labside digitalization—A laboratory study. Dent. Mater. 30(4), 400–407 (2014).
Lee, S. J., Kim, S. W., Lee, J. J. & Cheong, C. W. Comparison of intraoral and extraoral digital scanners: Evaluation of surface topography and precision. Dent. J. (Basel). 8(2), 52 (2020).
Wang, F., Hao, H., Tang, Q. & Lu, Y. Comparative evaluation of the morphological accuracy of dental crowns fabricated by different technologies. J. Prosthet. Dent. 125(4), 645–650 (2021).
Irish, J. et al. Quality of life in patients with maxillectomy prostheses. Head Neck 31(6), 813–821 (2009).
Rieger, J. M., Wolfaardt, J. F., Jha, N. & Seikaly, H. Maxillary obturators: The relationship between patient satisfaction and speech outcome. Head Neck 25(11), 895–903 (2003).
Kamarudin, K. H., Hattori, M., Sumita, Y. I. & Taniguchi, H. A chairside technique to add customized anterior acrylic resin teeth to a surgical obturator. J. Prosthet. Dent. 119(5), 852–854 (2018).
Mukohyama, H., Sasaki, M. & Taniguchi, H. Chairside modification of a surgical obturator: A clinical report. J. Prosthet. Dent. 91(6), 518–520 (2004).
Wismeijer, D., Mans, R., van Genuchten, M. & Reijers, H. A. Patients’ preferences when comparing analogue implant impressions using a polyether impression material versus digital impressions (Intraoral Scan) of dental implants. Clin. Oral Implants Res. 25(10), 1113–1118 (2014).
Goracci, C., Franchi, L., Vichi, A. & Ferrari, M. Accuracy, reliability, and efficiency of intraoral scanners for full-arch impressions: A systematic review of the clinical evidence. Eur. J. Orthod. 38(4), 422–428 (2016).
Ender, A. & Mehl, A. Accuracy in dental medicine, a new way to measure trueness and precision. J. Vis. Exp. 86, 51374 (2014).
Mennito, A. S. et al. Evaluation of the effect scan pattern has on the trueness and precision of six intraoral digital impression systems. J. Esthet. Restor Dent. 30(2), 113–118 (2018).
Mennito, A. S. et al. Evaluation of the trueness and precision of complete arch digital impressions on a human maxilla using seven different intraoral digital impression systems and a laboratory scanner. J. Esthet. Restor Dent. 31(4), 369–377 (2019).
Revilla-León, M. et al. Facial scanning accuracy depending on the alignment algorithm and digitized surface area location: An in vitro study. J. Dent. 110, 103680 (2021).
Revilla-León, M. et al. Best-fit algorithm influences on virtual casts’ alignment discrepancies. J. Prosthodont. 32(4), 331–339 (2023).
Rotar, R. N., Faur, A. B., Pop, D. & Jivanescu, A. Scanning distance influence on the intraoral scanning accuracy—An in vitro study. Materials (Basel). 15(9), 3061 (2022).
Flügge, T. V., Schlager, S., Nelson, K., Nahles, S. & Metzger, M. C. Precision of intraoral digital dental impressions with iTero and extraoral digitization with the iTero and a model scanner. Am. J. Orthod. Dentofac. Orthop. 144(3), 471–478 (2013).
Ender, A. & Mehl, A. Accuracy of complete-arch dental impressions: A new method of measuring trueness and precision. J. Prosthet. Dent. 109(2), 121–128 (2013).
Wei, D., Di, P., Tian, J., Zhao, Y. & Lin, Y. Evaluation of intraoral digital impressions for obtaining gingival contour in the esthetic zone: Accuracy outcomes. Clin. Oral Invest. 24(4), 1401–1410 (2020).
Chochlidakis, K. et al. Digital versus conventional full-arch implant impressions: A prospective study on 16 edentulous maxillae. J. Prosthodont. 29(4), 281–286 (2020).
Gan, N., Xiong, Y. & Jiao, T. Accuracy of intraoral digital impressions for whole upper jaws, including full dentitions and palatal soft tissues. PLoS One 11(7), e0158800 (2016).
Aswani, K., Wankhade, S., Khalikar, A. & Deogade, S. Accuracy of an intraoral digital impression: A review. J Indian Prosthodont. Soc. 20(1), 27–37 (2020).
Elbashti, M. E. et al. Precision and trueness of computerized optical impressions in maxillectomy defects: An in vitro 3D comparison. Int. J. Prosthodont. 32(3), 289–292 (2019).
Lo Russo, L. et al. Three-dimensional differences between intraoral scans and conventional impressions of edentulous jaws: A clinical study. J. Prosthet. Dent. 123(2), 264–268 (2020).
Moon, Y. G. & Lee, K. M. Comparison of the accuracy of intraoral scans between complete-arch scan and quadrant scan. Prog. Orthod. 21(1), 36 (2020).
Park, J. Y. et al. Evaluation of the marginal and internal gaps of three different dental prostheses: Comparison of the silicone replica technique and three-dimensional superimposition analysis. J. Adv. Prosthodont. 9(3), 159–169 (2017).
Pathak, V. K. & Singh, A. K. Investigating alignment effect on inspection accuracy of AM part using 3D scanner. J. Adv. Manuf. Syst. 16(2), 157–169 (2017).
Kim, R. J., Park, J. M. & Shim, J. S. Accuracy of 9 intraoral scanners for complete-arch image acquisition: A qualitative and quantitative evaluation. J. Prosthet. Dent. 120(6), 895–903 (2018).
Lee, J. H. Improved digital impressions of edentulous areas. J. Prosthet. Dent. 117(3), 448–449 (2017).
Fang, J. H., An, X., Jeong, S. M. & Choi, B. H. Digital intraoral scanning technique for edentulous jaws. J. Prosthet. Dent. 119(5), 733–735 (2018).
Acknowledgements
The authors thank all subjects who participated in the study. This study was funded by the Fujian Provincial Finance Department, grant number BPB-2022CYJ.
Author information
Authors and Affiliations
Contributions
R.C. and Y.C. established the research plans. S.Z. conducted the experiments. L.L., P.Q. and H.X. conducted the data analysis. R.C. wrote the main manuscript. Y.C. revised the manuscript. All authors have approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Cao, R., Zhang, S., Li, L. et al. Accuracy of intraoral scanning versus conventional impressions for partial edentulous patients with maxillary defects. Sci Rep 13, 16773 (2023). https://doi.org/10.1038/s41598-023-44033-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-44033-6
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
