
Abstract
There is controversial evidence about the relationship between consumption of legumes and nuts with metabolic disturbances. The present study was undertaken to explore the association of legumes and nuts intake with metabolic health status among Iranian adults. This cross-sectional study was conducted on 527 adults (45.7% female, aged 20–65 years) chosen through a multistage cluster random-sampling approach. Dietary intakes of individuals were assessed using a validated food frequency questionnaire. Fasting blood samples were gathered to evaluate biochemical parameters. Metabolic health status of subjects was determined according to the criteria defined by Wildman. Data of covariates were collected using pre-tested procedures. The overall prevalence of metabolic unhealthy (MU) phenotype was 42.5%. After controlling all confounders, participants with highest intake of legumes and nuts had lower odds of MU status, compared with the lowest intake (OR 0.35; 95% CI 0.18–0.71). This association was stronger in normal-weight rather than overweight/obese adults and also in women rather than men. Higher consumption of legumes and nuts was additionally related to decreased odds of hyperglycemia, hypertriglyceridemia, and hypertension. A marginally inverse association was observed between legumes and nuts intake with low brain-derived neurotrophic factor (BDNF) levels, in fully-adjusted model (ORT3 vs. T1 0.50; 95% CI 0.25–1.01). Each tertile increase in legumes and nuts intake was marginally related to higher adropin levels (\(\beta\) = 4.06; P = 0.07). In conclusion, this study demonstrated that higher intake of legumes and nuts is associated with lower chance of MU both in normal weight and overweight/obese adults. The association may be facilitated through serum BDNF and adropin.
Similar content being viewed by others


Introduction
Obesity, currently affecting about one-third of the world’s population, is considered as a major public health threat, due to its effect on risk of chronic diseases such as type 2 diabetes mellitus, cardiovascular diseases (CVDs), and some types of cancers1,2,3. However, recently the concept of metabolic health status has challenged the role of obesity in determining risk of chronic diseases. To be more exact, a subgroup of obese individuals with a favorable metabolic profile who are known as metabolically healthy obese (MHO) is less likely to have chronic diseases compared to metabolically unhealthy obese (MUO) individuals4. Additionally, a high risk of cardiometabolic disorders has been reported in normal-weight individuals with a metabolically unhealthy (MU) profile5,6. Therefore, it seems that metabolic status could be a better predictor for risk of chronic diseases than obesity, and maintaining a healthy metabolic status could be considered a beneficial strategy for reducing risk of chronic diseases.
During recent decades, emerging evidence has pointed to the metabolic role of hormones such as adropin and brain-derived neurotrophic factor (BDNF). Findings of experimental investigations indicated that these secreted molecules could control metabolism of glucose and lipid and regulate energy hemostasis7,8. Decreased serum levels of adropin and BDNF have been also reported in people with metabolic disorders such as obesity, diabetes mellitus, and CVDs9,10,11. Some reports have also indicated that modifiable factors such as dietary intakes and physical activity could affect adropin and BDNF levels12,13,14,15,16. It is postulated that adropin and BDNF play key roles in determining metabolic health status. Therefore, altering their serum levels is probably one of the mechanisms through which behavioral interventions improve metabolic health status.
Previous studies have suggested lifestyle modification as a beneficial approach for improving metabolic parameters. During recent decades, many epidemiological and clinical studies have highlighted the role of diet, among other lifestyle factors, on metabolic status17. A great body of evidence from observational and interventional studies has demonstrated the beneficial role of healthy dietary patterns, such as Mediterranean diet, dietary approach to stop hypertension (DASH) diet and plant-based diets on metabolic status18,19,20. These dietary patterns are rich in fruits, vegetables, whole grains, legumes, and nuts. Among plant-based foods, legumes, and nuts may affect the metabolic parameters potentially, due to their favorable content of nutrients and bioactive compounds such as vegetable protein, fiber, unsaturated fatty acids, vitamins, minerals, phytosterols, and phytochemicals21,22.
The relationship between dietary intake of legumes and nuts with metabolic syndrome (MetS) or its components has been investigated in previous studies. However, the results of these studies are contradictory. Some epidemiological evidences suggest that dietary intake of legumes and nuts is associated with a reduced risk of MetS or its components23,24,25,26,27, while other studies have shown conflicting results28,29,30,31,32. A recently published investigation has evaluated the link of nuts and legumes intake with metabolic health status in Iranian adolescents33, but no previous study has investigated this relationship among adults, especially in Middle Eastern populations. Therefore, the purpose of this study was to investigate the association of nuts and legumes intake with metabolic health status in Iranian men and women adults, considering the potential underlying role of BDNF and adropin.
Materials and methods
Study design and population
This cross-sectional study was performed in 2021, on a sample of Iranian adults living in Isfahan, Iran. According to a multistage cluster random-sampling approach, all adults working as teachers, school managers, employees, assistants or crews in several schools of different educational districts of Isfahan were selected. Based on a previous published study34, 49.4% of Iranian adults might have metabolic disorders; so, considering type 1 error of 0.05 (confidence interval (CI) of 0.95), precision (d) of 4.5% and power of 80%, 474 subjects were minimally required for this study. Nevertheless, due to high prevalence of covid-19 pandemic and its potential impact on data collection, 600 individuals were invited to participate in our investigation. Response rate was 90.5%. Individuals with the following characteristics were not included in our study: (1) having a history of type 1 diabetes, cardiovascular diseases, stroke and cancer; (2) being pregnant or lactating; (3) following a special diet. Exclusion criteria were: (1) having left more than 70 items on the food frequency questionnaire (FFQ) unfilled; (2) reporting energy intake outside of 800–4200 kcal/day; (3) refusing blood draw. Finally, a total of 527 adults aged 20 to 65 years old were eligible to be included in this analysis. Each participant signed a written informed permission. Local Ethics Committee of Isfahan University of Medical Sciences approved the protocol of this study (no. 3402104).
Assessment of dietary intakes
We evaluated dietary intakes of participants using a Willett-format semi-quantitative 168-item FFQ. Validity of this questionnaire has been approved through a prior validation research which found reasonable correlations between the food intakes determined by this questionnaire and those acquired from several 24-h dietary recalls35. A comparison of nutrient intakes derived from this FFQ on two occasions, 1 year apart, indicated reliability of this tool as well35. All Participants were guided by a registered dietitian to fill out the FFQ by describing the frequency and amount of their eaten foods during the last year. Afterward, the portions of ingested items were changed to g/day using household measurements36. Lastly, data of all food items were input into the Nutritionist IV program to calculate daily energy and nutritional intakes.
Assessment of anthropometric indices and blood pressure
Weight, height and waist circumference (WC) of participants were assessed by two skilled dietitians, with little clothing and no shoes. The body composition analyzer (Tanita MC-780MA, Tokyo, Japan) was utilized to determine weight (to the nearest 0.1 kg). Height was measured using a tape measure fixed on the wall (to the nearest 0.1 cm). Then, body mass index (BMI) was computed by dividing weight (kg) by height squared (m2). WC was evaluated after a normal breath with no outside pressure on the body and by applying an unstretched flexible tape measure (to the nearest 0.1 cm). Blood pressure (BP) of each person was taken after sitting for five minutes with an empty bladder and no prior exercise. A digital sphygmomanometer (OMRON, M3, HEM-7154-E, Japan) with an accuracy of 0.5 mmHg was used to assess BP. The measurements were conducted twice, with intervals of 5–10 min, and average of the measurements was reported as the final BP.
Assessment of biochemical parameters
A 10-mL peripheral blood sample was drawn from each subject, after an overnight fasting for 12 h. The Biosystem A15 auto-analyzer with different enzymatic colorimetric methods was used to assess concentrations of some special biochemical parameters including: (1) triglyceride (TG) (glycerol phosphate oxidase (GPO)); (2) fasting blood glucose (FBG) (glucose oxidase (GOD)); (3) high-density lipoprotein cholesterol (HDL-c) (cholesterol oxidase (CHOD)). Other serum parameters were also measured using the commercial enzyme-linked immunosorbent assay (ELISA) kits as follows: (1) high sensitive C-reactive protein (hs-CRP) (turbidimetry kit, latex enhanced turbidimetric method, Delta.DP); (2) insulin (Monobined Inc. Lake Forest, CA 92630, USA); (3) BDNF and adropin (Zellbio, Veltlinerweg, Germany). Insulin resistance (IR) was calculated through Homeostasis Model Assessment Insulin Resistance (HOMA-IR) formula: HOMA-IR = [FBG (mmol/L) × fasting insulin (mU/L)]/22.537. First decile of serum BDNF concentration was considered as low serum BDNF levels (serum BDNF < 0.47 ng/mL).
Assessment of metabolic health status
Metabolic health of participants was evaluated using the criteria defined by Wildman et al.38. According to this definition, subjects with normal-weight (18.5 \(\le\) BMI < 25) or overweight/obesity (BMI \(\ge\) 25) were considered to have metabolically unhealthy normal-weight (MUNW) and metabolically unhealthy overweight/obese (MUOW) profiles, if they had more than two of the following risk factors: (1) high FBG levels (\(\ge\) 100 mg/dL); (2) decreased HDL-c levels (\(<\) 40 mg/dL for males or \(<\) 50 mg/dL for females); (3) elevated TG levels (\(\ge\) 150 mg/dL); (4) hypertension (BP \(\ge\) 130/85 mmHg); (5) IR (HOMA-IR > 90th percentile or > 3.99); (6) elevated inflammatory protein hs-CRP levels (> 90th percentile, or > 6.14 mg/L). In contrast, other normal-weight and overweight/obese participants with less than two of the above-mentioned parameters were known as metabolically healthy normal-weight (MHNW) and metabolically healthy overweight/obese (MHOW), respectively.
Assessment of other variables
Data on sex, age, marital status, education and smoking were collected through a self-reported questionnaire. Furthermore, a validated questionnaire was applied to evaluate socioeconomic status (SES) of participants39. This questionnaire assessed individuals in terms of the number of family members, homeownership, type of car, having laptops/computers and traveling in the year. Physical activity (PA) was also measured using a validated International Physical Activity Questionnaire-short form (IPAQ-SF) that evaluates three categories of activity including walking, moderate-intensity activities, and vigorous-intensity activities40. The data from this questionnaire were converted to Metabolic Equivalent minutes per week (MET.min/week) and participants were categorized as inactive (< 600 MET.min/week), minimally active (≥ 600 to < 3000 MET.min/week), or active (≥ 3000 MET.min/week).
Statistical analysis
Energy-adjusted intake of legumes and nuts was computed based on residual method. Then, participants were classified according to tertiles of energy-adjusted legumes and nuts intake. Continues and categorical variables were reported as mean ± SD/SE and number (percentage), respectively. We used one-way ANOVA and chi-square test to compare characteristics of subjects across tertiles of energy-adjusted legumes and nuts intake. Dietary intakes of individuals were also assessed through ANCOVA by adjusting sex, age and energy intake. Possible associations between intake of legumes and nuts with metabolic unhealthy (MU) status and its components were determined using binary logistic regression. Confounding effects of potential variables (including age, sex and energy intake in the first model, education, marital status, smoking status, SES and PA in the second model, intake of fruits, vegetables, dairy, whole and refined grains in the third model, and BMI in the last model) were controlled in the analyses41,42. All odds ratios (ORs) were calculated by considering the first tertile of legumes and nuts as the reference. Tertiles of energy-adjusted legumes and nuts intake were regarded as an ordinal variable in logistic regression models to evaluate trend of ORs across tertiles of legumes and nuts intake. Stratified analyses were also conducted by BMI categories (normal-weight vs. overweight/obese) and sex (women vs. men). Multivariable-adjusted odds of low BDNF values (< 0.47 ng/mL) in tertiles of energy-adjusted legumes and nuts intake were determined by considering the effects of age, sex, PA, high BP, high TG and high FBG. In addition, linear regression analysis was applied to assess adropin levels in tertiles of energy-adjusted legumes and nuts intake with adjusting age, sex, energy intake, PA and BMI as covariates. SPSS software version 26 (IBM, Chicago, IL) was utilized for all analyses and P-values < 0.05 were regarded to be statistically significant.
Ethical approval and consent to participate
The study procedure was performed according to declaration of Helsinki and STROBE checklist. All participants provided informed written consent. The study protocol was approved by the local Ethics Committee of Isfahan University of Medical Sciences.
Consent to participate
Informed consent was obtained from all participants involved in the study.
Results
This study was conducted on 527 adults (45.7% female) with an average age of 42.66 (± 11.19 SD) years. Participants had a mean weight of 75.77 (± 14.59 SD) kg and BMI range of 16.60 to 59.80 kg/m2. Prevalence of MU status among all participants was 42.5%, which 20.5% of them had normal weight and 79.5% had overweight/obesity.
General characteristics of participants across energy-adjusted tertiles of legumes and nuts intake are shown in Table 1. Individuals in the top tertile of legumes and nuts intake were more likely to be male, had a lower body weight and also lower prevalence of hypertriglyceridemia, compared to those at the bottom tertile. However, no substantial differences were observed in other demographic and cardiometabolic variables including age, BMI, WC, education, marital status, smoking, SES, PA, high BP, high FBG, IR (high HOMA-IR score), high hs-CRP, low HDL-c, low BDNF values and adropin levels.
Dietary intakes of subjects across energy-adjusted tertiles of legumes and nuts intake are illustrated in Table 2. Participants with higher consumption of legumes and nuts had also higher intakes of proteins, dietary fiber, folate, magnesium and potassium, and lower intakes of total energy and refined grains. While, consumptions of fruits, vegetables, meats, fish, whole grains, dairy, carbohydrates, fats, vitamin C and calcium did not differ significantly across tertiles of legumes and nuts intake.
Figure 1 represents the prevalence of MU status across energy-adjusted tertiles of legumes and nuts intake. Prevalence of MU phenotype was 50.9% in first tertile, 40.3% in the second tertile and 36.4% in the third tertile of legumes and nuts intake. This prevalence was significantly different across tertiles of legumes and nuts intake (Pvalue = 0.02).

Prevalence of metabolically unhealthy (MU) status across energy-adjusted tertiles of legumes and nuts intake in the study population.
Crude and multivariable-adjusted ORs for MU phenotype across energy-adjusted tertiles of legumes and nuts intake are reported in Table 3. In comparison with the first tertile of legumes and nuts intake, individuals at the last tertile had a decreased odds of MU status in crude model (ORT3 vs. T1 0.55; 95% CI 0.36–0.85). After controlling potential variables, this association was strengthened (ORT3 vs. T1 0.35; 95% CI 0.18–0.71). A significant decreasing trend was also observed for MU phenotype across tertiles of legumes and nuts intake in all models (Ptrend = 0.01). Each tertile increase in intake of legumes and nuts was significantly associated with reduced odds of MU status in crude and maximally-adjusted models as well. Stratified analysis by BMI revealed an inverse relationship between legumes and nuts intake and likelihood of MUNW profile among normal-weight participants, in both crude (ORT3 vs. T1 0.35; 95% CI 0.14–0.87) and fully-adjusted (ORT3 vs. T1 0.15; 95% CI 0.03–0.85) models. Among participants with overweight/obesity, legumes and nuts intake was marginally associated with reduced odds of MUOW profile in crude model (ORT3 vs. T1 0.60; 95% CI 0.36–1.00). This association was strengthened after considering confounders (ORT3 vs. T1 0.29; 95% CI 0.12–0.69).
Table 4 presents the association between MU status and intake of legumes and nuts, stratified by sex. Among women, an inverse association was observed between dietary intake of legumes and nuts with MU status in both crude (ORT3 vs. T1 0.46; 95% CI 0.23–0.94) and fully-adjusted (ORT3 vs. T1 0.28; 95% CI 0.09–0.091) models. Legumes and nuts intake of men was not substantially related to MU phenotype in crude model (ORT3 vs. T1 0.68; 95% CI 0.40–1.19). However, by adjusting potential confounders this association became marginally significant (ORT3 vs. T1 0.40; 95% CI 0.16–1.00).
Crude and multivariable-adjusted ORs for metabolic health components across energy-adjusted tertiles of legumes and nuts intake are shown in Table 5. In crude model, participants with the highest intake of legumes and nuts had lower odds of hypertriglyceridemia and hypertension, compared to the lowest intake. However, by controlling all confounders, higher consumption of legumes and nuts was significantly associated with decreased likelihood of hyperglycemia (ORT3 vs. T1 0.38; 95% CI 0.16–0.89), hypertriglyceridemia (ORT3 vs. T1 0.48; 95% CI 0.25–0.92), hypertension (ORT3 vs. T1 0.37; 95% CI 0.18–0.76), and marginally related to reduced odds of low HDL-cholesterolemia (ORT3 vs. T1 0.41; 95% CI 0.16–1.09) and high hs-CRP levels (ORT3 vs. T1 0.39; 95% CI 0.14–1.07).
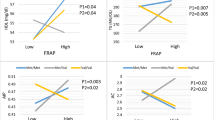
The average serum levels of BDNF and adropin among participants were 1.25 ng/mL and 56.59 pg/mL, respectively. Multivariate-adjusted ORs for low BDNF levels across tertiles of legumes and nuts intake are depicted in Fig. 2. Compared to the reference group, higher intake of legumes and nuts was marginally related to decreased likelihood of low BDNF levels, in both crude (ORT3 vs. T1 0.56; 95% CI 0.28–1.10) and multivariable-adjusted (ORT3 vs. T1 0.50; 95% CI 0.25–1.01) models. As shown in Fig. 3, linear regression analysis revealed that each tertile increment in legumes and nuts intake was substantially associated with an increase of 4.78 pg/mL in levels of adropin in crude model (95% CI 0.47–9.09; Pvalue = 0.03). After adjusting all covariates, a marginally significant direct association was observed between each tertile increase in legumes and nuts intake with adropin levels (\(\beta\) = 4.06; 95% CI − 0.32, 8.44; Pvalue = 0.07). No significant differences were found in circulating BDNF and adropin levels between individuals with metabolically healthy and unhealthy phenotypes, even after stratifying analysis by sex or age categories (Supplemental Figs. 1, 2).

Multivariable-adjusted odds ratio and 95% confidence intervals for low BDNF levels across tertiles of legumes and nuts intake. Model 1: Adjusted for age and sex; Model 2: More adjustments for physical activity, history of high blood pressure, high triglyceride and high fasting blood glucose. Ptrend was obtained by the use of tertiles of legumes and nuts intake as an ordinal variable in the model.

Linear association between tertiles of legumes and nuts intake with adropin levels. All values are regression coefficients and 95% confidence intervals. Tertiles of legumes and nuts intake were considered as an ordinal variable in linear regression analysis. Model 1: Adjusted for age, sex, and energy intake; Model 2: More adjustments for physical activity and BMI.
Discussion
The findings of the present cross-sectional study showed that more than 40% of the Iranian population had an MU phenotype with a significantly higher prevalence among obese/overweight than normal-weight individuals (79.5% vs. 20.5%). Higher consumption of legumes and nuts was associated with lower odds of MU phenotype both in normal-weight and obese/overweight individuals. This association was more prominent among females. A significant inverse relationship was also found between legumes and nuts intake with some components of metabolic health status including hyperglycemia, hypertriglyceridemia, and hypertension. These beneficial associations might be facilitated through higher BDNF and adropin levels.
Non-communicable diseases (NCDs), mainly CVDs, cancers, respiratory diseases, and diabetes, account for over 70% of deaths worldwide43. Among the modifiable lifestyle behaviors increasing the risk of NCDs, diet plays a key role through its contribution in metabolic disturbances44. Therefore, dietary intake assessments and implementing early clinical interventions could be beneficial approaches for reducing risk of metabolic disturbances and related NCDs. Findings of this study revealed that daily consumption of more than 54 g of legumes and nuts could reduce MU odds. Therefore, providing nutritional education and interventions to consume a healthy diet containing appropriate amounts of legumes and nuts is recommended as a beneficial approach to reduce risk of MU status.
To the best of our knowledge, this report is the first observational study investigating the relationship between the intake of legumes and nuts with metabolic health status. However, legume and nut intake in relation to MetS or its components has been investigated previously and revealed controversial results. Contrary to our results, a cross-sectional study involving 420 Iranian female nurses has failed to find any association between the consumption of legumes and nuts with MetS or its components28. Additionally, a systematic review and meta-analysis of 7 observational studies containing 56,028 participants demonstrated no significant association between legume intake and odds of MetS41. However, the beneficial effect of legume intake on total cholesterol and low-density lipoprotein cholesterol (LDL-c) as well as BP in obese and overweight individuals has been reported by two other studies45,46. A meta-analysis of 11 observational studies showed an inverse significant association between nut intake and risk of MetS42. There are also other reports on the protective role of nut consumption on cardiometabolic disorders. Nut intake has been shown to have a favorable effect on HOMA-IR and fasting insulin in a meta-analysis of 40 randomized controlled trials47. In addition, the beneficial effect of nut consumption on hypertension has been reported in other studies48. However, in a meta-analysis of 6 randomized controlled trials, no significant association was found between total nut intake and lipid profile49. These discrepant findings can be explained by different genetic backgrounds and dietary habits of the studied population, tools used to assess dietary intakes, and controlling for various confounders.
Many NCDs in adulthood, especially endocrine dysfunctions, have roots in health status, lifestyle and dietary intakes in childhood. According to a cohort survey by Liang et al., children with obesity had higher risk of diabetes in adulthood50. Another study also revealed that childhood risk factors including unhealthy diets had long-term effects on metabolic health and CVD risk in adulthood51. Therefore, maintaining the health status in early life would be of great importance in every society. In our previous study, we discovered that higher intake of legumes and nuts was associated with lower odds of metabolic unhealthy among Iranian adolescents aged 12 to 18 years33. The same findings were obtained in the current investigation in adults. Although there were no sufficient data regarding the metabolic status of the present study participants in their childhood, it could be mentioned that the current metabolic status of these individuals might be affected by their childhood lifestyle. Therefore, it would be more valuable to modify food habits and intakes from childhood and adolescence in order to prevent the occurrence of many diseases in adulthood.
Our results showed that the inverse association between legumes and nuts intake with MU phenotype was more prominent in females. This finding might be explained by healthier dietary knowledge and behavior among women than men52. Also, better metabolic profiles among women due to the differences in substrate use, accumulation and metabolism in important metabolic organs including liver, skeletal muscle and fat tissue may explain the observed finding53. Furthermore, premenopausal women have reduced odds of metabolic disturbances which highlights the key role of sex-hormones in metabolic health53. In addition, the observed association was stronger among normal-weight rather than over weight/obese subjects. Different physiological responses to environmental factors, such as diet, and differences in accuracy of reported food intakes might explain the observed findings. However, further studies are required to confirm these hypotheses.
We found a marginally inverse association between low BDNF levels with legumes and nuts intake. A positive linear association was also observed between levels of adropin and legumes and nuts intake. So far, several studies have examined the association between some dietary factors with BDNF and adropin levels in both animals and humans12,13,16,54. A clinical trial conducted on Spanish adults found that the Mediterranean diet supplemented by nuts was related to reduced odds of low BDNF levels55. There were no other related investigations that examined the association of legumes or nuts intake with BDNF and adropin levels. The current epidemiologic study revealed no substantial differences in BDNF or adropin levels between metabolically healthy and unhealthy groups. Although some previous studies have documented that higher concentrations of BDNF and adropin were related to decreased odds of metabolic disorders through regulating energy hemostasis and its related signaling pathways7,8,9, there are insufficient data regarding this association and the possible mechanisms. Our findings could broaden insights into further related studies.
The inverse relationship between the intake of legumes and nuts with MU phenotype can be explained by several feasible mechanisms. Legumes and nuts are rich in fiber, minerals, and bioactive compounds which might have beneficial effects on metabolic health status. Magnesium content of legumes and nuts plays an important role in decreasing inflammation and insulin resistance56,57. Additionally, a large body of evidence indicates that dietary fiber contributes in improving metabolic health status components such as hypertension, dyslipidemia, insulin sensitivity, and inflammatory biomarkers levels58. Another explanation for the beneficial influence on metabolic health status may be the antioxidant and anti-inflammatory properties of bioactive phytochemicals such as polyphenols which have modulatory effects on metabolic processes59. Moreover, low glycemic index of legumes and nuts reduces the risk of insulin resistance and improves metabolic health status60.
The current study has several limitations that should be acknowledged. The study does not provide evidence for a causal relationship between the consumption of legumes and nuts with MU, due to its cross-sectional design. Self-reported dietary intakes might be subject to recall bias and misclassification, despite using a validated FFQ for assessment of dietary intakes. In addition, due to low amounts of nuts intake in our study population, no separate analysis was performed for nuts and legumes intake. On the other hand, to the best of our knowledge, this is the first study that investigates the links between the intake of legumes and nuts with metabolic health status in a somehow representative sample of Iranian adults. Furthermore, a relatively comprehensive definition of metabolic health status (Wildman et al. method) was used that includes an inflammatory index (hs-CRP) in addition to HOMA-IR and traditional cardiometabolic risk factors. The confounding role of several variables was also taken into account in the statistical analyses. The final strength of the study was the assessment of serum levels of adropin and BDNF which rarely have been investigated in epidemiological studies of nutrition.
In summary, a significant relationship was found between consumption of legumes and nuts with decreased odds of MUNW and MUOW phenotypes, particularly among females. Higher consumption of legumes and nuts was also inversely associated with hyperglycemia, hypertriglyceridemia, and hypertension. The association might be facilitated through BDNF and adropin. Further population-based prospective studies are warranted to confirm these findings.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Abbreviations
- BP:
-
Blood pressure
- BMI:
-
Body mass index
- BDNF:
-
Brain-derived neurotrophic factor
- CI:
-
Confidence interval
- CHOD:
-
Cholesterol oxidase
- CVDs:
-
Cardiovascular diseases
- DASH:
-
Dietary approach to stop hypertension
- DBP:
-
Diastolic blood pressure
- ELISA:
-
Enzyme-linked immunosorbent assay
- FBG:
-
Fasting blood glucose
- FFQ:
-
Food frequency questionnaire
- GOD:
-
Glucose oxidase
- GPO:
-
Glycerol phosphate oxidase
- HDL-c:
-
High-density lipoprotein cholesterol
- HOMA-IR:
-
Homeostasis model assessment insulin resistance
- hs-CRP:
-
High sensitive C-reactive protein
- IR:
-
Insulin resistance
- IPAQ-SF:
-
International physical activity questionnaire-short form
- LDL-c:
-
Low-density lipoprotein cholesterol
- MET:
-
Metabolic equivalent
- MetS:
-
Metabolic syndrome
- MHNW:
-
Metabolically healthy normal-weight
- MHO:
-
Metabolically healthy obesity
- MHOW:
-
Metabolically healthy overweight/obesity
- MU:
-
Metabolically unhealthy
- MUNW:
-
Metabolically unhealthy normal-weight
- MUO:
-
Metabolically unhealthy obesity
- MUOW:
-
Metabolically unhealthy overweight/obesity
- NCDs:
-
Non-communicable diseases
- OR:
-
Odds ratio
- PA:
-
Physical activity
- SBP:
-
Systolic blood pressure
- SD:
-
Standard deviation
- SE:
-
Standard error
- SES:
-
Socioeconomic status
- T:
-
Tertile
- TG:
-
Triglycerides
- WC:
-
Waist circumference
References
Scherer, P. E. & Hill, J. A. Obesity, diabetes, and cardiovascular diseases: A Compendium. Circ. Res. 118, 1703–1705 (2016).
Calle, E. E. & Kaaks, R. Overweight, obesity and cancer: Epidemiological evidence and proposed mechanisms. Nat. Rev. Cancer 4, 579–591 (2004).
Chooi, Y. C., Ding, C. & Magkos, F. The epidemiology of obesity. Metabolism 92, 6–10 (2019).
Stefan, N., Häring, H.-U., Hu, F. B. & Schulze, M. B. Metabolically healthy obesity: Epidemiology, mechanisms, and clinical implications. Lancet Diabetes Endocrinol. 1, 152–162 (2013).
Stefan, N., Schick, F. & Häring, H.-U. Causes, characteristics, and consequences of metabolically unhealthy normal weight in humans. Cell Metab. 26, 292–300 (2017).
Rubin, R. What’s the best way to treat normal-weight people with metabolic abnormalities? JAMA 320, 223–225 (2018).
Ali, I. I., D’Souza, C., Singh, J. & Adeghate, E. Adropin’s role in energy homeostasis and metabolic disorders. Int. J. Mol. Sci. 23, 8318 (2022).
Rothman, S. M., Griffioen, K. J., Wan, R. & Mattson, M. P. Brain-derived neurotrophic factor as a regulator of systemic and brain energy metabolism and cardiovascular health. Ann. N.Y. Acad. Sci. 1264, 49–63 (2012).
Han, W. et al. Alterations of irisin, adropin, preptin and BDNF concentrations in coronary heart disease patients comorbid with depression. Ann. Transl. Med. 7, 298 (2019).
Rozanska, O., Uruska, A. & Zozulinska-Ziolkiewicz, D. Brain-derived neurotrophic factor and diabetes. Int. J. Mol. Sci. 21, 841 (2020).
Wu, L. et al. Low serum adropin is associated with coronary atherosclerosis in type 2 diabetic and non-diabetic patients. Clin. Chem. Lab. Med. 52, 751–758 (2014).
St-Onge, M. P. et al. Fasting plasma adropin concentrations correlate with fat consumption in human females. Obesity 22, 1056–1063 (2014).
Stevens, J. R. et al. Inverse association between carbohydrate consumption and plasma adropin concentrations in humans. Obesity 24, 1731–1740 (2016).
Fujie, S. et al. Aerobic exercise training-induced changes in serum adropin level are associated with reduced arterial stiffness in middle-aged and older adults. Am. J. Physiol.-Heart Circ. Physiol. 309, H1642–H1647 (2015).
Walsh, J. J. & Tschakovsky, M. E. Exercise and circulating BDNF: Mechanisms of release and implications for the design of exercise interventions. Appl. Physiol. Nutr. Metab. 43, 1095–1104 (2018).
Gravesteijn, E., Mensink, R. P. & Plat, J. Effects of nutritional interventions on BDNF concentrations in humans: A systematic review. Nutr. Neurosci. 25, 1425–1436 (2022).
Castro-Barquero, S., Ruiz-León, A. M., Sierra-Pérez, M., Estruch, R. & Casas, R. Dietary strategies for metabolic syndrome: A comprehensive review. Nutrients 12, 2983 (2020).
Godos, J. et al. Adherence to the Mediterranean diet is inversely associated with metabolic syndrome occurrence: A meta-analysis of observational studies. Int. J. Food Sci. Nutr. 68, 138–148 (2017).
Phillips, C. M., Harrington, J. M. & Perry, I. J. Relationship between dietary quality, determined by DASH score, and cardiometabolic health biomarkers: A cross-sectional analysis in adults. Clin. Nutr. 38, 1620–1628 (2019).
Kahleova, H., Levin, S. & Barnard, N. Cardio-metabolic benefits of plant-based diets. Nutrients 9, 848 (2017).
Bouchenak, M. & Lamri-Senhadji, M. Nutritional quality of legumes, and their role in cardiometabolic risk prevention: A review. J. Med. Food 16, 185–198 (2013).
Kim, Y., Keogh, J. & Clifton, P. M. Nuts and cardio-metabolic disease: A review of meta-analyses. Nutrients 10, 1935 (2018).
O’Neil, C. E., Fulgoni, V. L. & Nicklas, T. A. Tree Nut consumption is associated with better adiposity measures and cardiovascular and metabolic syndrome health risk factors in US Adults: NHANES 2005–2010. Nutr. J. 14, 1–8 (2015).
Fernández-Montero, A. et al. Nut consumption and incidence of metabolic syndrome after 6-year follow-up: The SUN (Seguimiento Universidad de Navarra, University of Navarra Follow-up) cohort. Public Health Nutr. 16, 2064–2072 (2013).
Ibarrola-Jurado, N. et al. Cross-sectional assessment of nut consumption and obesity, metabolic syndrome and other cardiometabolic risk factors: The PREDIMED study. PLoS ONE 8, e57367 (2013).
Hosseinpour, N. S. et al. Legume Intake is Inversely Associated with Metabolic Syndrome in Adults (2012).
Sajjadi, F. et al. Relationship between legumes consumption and metabolic syndrome: Findings of the Isfahan Healthy Heart Program. ARYA Atheroscler. 10, 18 (2014).
Ghosn, B. et al. Lack of association between nuts and legumes consumption and metabolic syndrome in young Iranian nurses. Clin. Nutr. ESPEN 46, 173–178 (2021).
Hassannejad, R. et al. Long-term nuts intake and metabolic syndrome: A 13-year longitudinal population-based study. Clin. Nutr. 38, 1246–1252 (2019).
Yu, S., Guo, X., Yang, H., Zheng, L. & Sun, Y. An update on the prevalence of metabolic syndrome and its associated factors in rural northeast China. BMC Public Health 14, 1–9 (2014).
de Oliveira, E. P., McLellan, K. C. P., de Arruda Silveira, L. V. & Burini, R. C. Dietary factors associated with metabolic syndrome in Brazilian adults. Nutr. J. 11, 1–7 (2012).
Strand, M. A., Perry, J., Wang, P., Liu, S. & Lynn, H. Risk factors for metabolic syndrome in a cohort study in a north China urban middle-aged population. Asia Pac. J. Public Health 27, 255–265 (2015).
Heshmatipour, H. et al. Association of legumes and nuts consumption with metabolic health status in Iranian overweight and obese adolescents. Sci. Rep. 13, 5784 (2023).
Rahmanian, K., Shojaei, M. & Sotoodeh Jahromi, A. Prevalence and clinical characteristics of metabolically unhealthy obesity in an Iranian adult population. Diabetes Metab. Syndr. Obes. Targets Ther. 12, 1387–1395 (2019).
Mirmiran, P., Esfahani, F. H., Mehrabi, Y., Hedayati, M. & Azizi, F. Reliability and relative validity of an FFQ for nutrients in the Tehran lipid and glucose study. Public Health Nutr. 13, 654–662 (2010).
Ghaffarpour, M., Houshiar-Rad, A. & Kianfar, H. The manual for household measures, cooking yields factors and edible portion of foods. Tehran Nashre Olume Keshavarzy 7, 42–58 (1999).
Swaroop, J. J., Rajarajeswari, D. & Naidu, J. Association of TNF-α with insulin resistance in type 2 diabetes mellitus. Indian J. Med. Res. 135, 127–130 (2012).
Wildman, R. P. et al. The obese without cardiometabolic risk factor clustering and the normal weight with cardiometabolic risk factor clustering: Prevalence and correlates of 2 phenotypes among the US population (NHANES 1999–2004). Arch. Intern. Med. 168, 1617–1624 (2008).
Garmaroudi, G. R. & Moradi, A. Socio-economic status in Iran: A study of measurement index. Payesh (Health Monitor) 9, 137–144 (2010).
Moghaddam, M. B. et al. The Iranian version of international physical activity questionnaire (IPAQ) in Iran: Content and construct validity, factor structure, internal consistency and stability. World Appl. Sci. J. 18, 1073–1080 (2012).
Jiang, Y.-T. et al. Relationship between legume consumption and metabolic syndrome: A systematic review and meta-analysis of observational studies. Nutr. Metab. Cardiovasc. Dis. 30, 384–392 (2020).
Zhang, Y. & Zhang, D.-Z. Relationship between nut consumption and metabolic syndrome: A meta-analysis of observational studies. J. Am. Coll. Nutr. 38, 499–505 (2019).
World Health Organization. Noncommunicable Diseases Country Profiles 2018 (2018).
Olatona, F., Onabanjo, O., Ugbaja, R., Nnoaham, K. & Adelekan, D. Dietary habits and metabolic risk factors for non-communicable diseases in a university undergraduate population. J. Health Popul. Nutr. 37, 1–9 (2018).
Bazzano, L. A., Thompson, A. M., Tees, M. T., Nguyen, C. H. & Winham, D. M. Non-soy legume consumption lowers cholesterol levels: A meta-analysis of randomized controlled trials. Nutr. Metab. Cardiovasc. Dis. 21, 94–103 (2011).
Reyneke, G. L., Beck, E. J., Lambert, K. & Neale, E. P. The effect of non-oil seed legume intake on blood pressure: A systematic review and meta-analysis of randomized controlled trials. Adv. Nutr. 14, 637 (2023).
Tindall, A. M., Johnston, E. A., Kris-Etherton, P. M. & Petersen, K. S. The effect of nuts on markers of glycemic control: A systematic review and meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 109, 297–314 (2019).
Mohammadifard, N. et al. The effect of tree nut, peanut, and soy nut consumption on blood pressure: A systematic review and meta-analysis of randomized controlled clinical trials. Am. J. Clin. Nutr. 101, 966–982 (2015).
Gunathilake, M., Van, N. T. H. & Kim, J. Effects of nut consumption on blood lipid profile: A meta-analysis of randomized controlled trials. Nutr. Metab. Cardiovasc. Dis. 32, 537–549 (2022).
Liang, Y. et al. Childhood obesity affects adult metabolic syndrome and diabetes. Endocrine 50, 87–92 (2015).
Shrestha, R. & Copenhaver, M. Long-term effects of childhood risk factors on cardiovascular health during adulthood. Clin. Med. Rev. Vasc. Health 7, 1 (2015).
Leblanc, V., Bégin, C., Corneau, L., Dodin, S. & Lemieux, S. Gender differences in dietary intakes: What is the contribution of motivational variables? J. Hum. Nutr. Dietet. 28, 37–46 (2015).
Goossens, G. H., Jocken, J. W. & Blaak, E. E. Sexual dimorphism in cardiometabolic health: The role of adipose tissue, muscle and liver. Nat. Rev. Endocrinol. 17, 47–66 (2021).
Cysneiros, R. M. et al. Qualitative analysis of hippocampal plastic changes in rats with epilepsy supplemented with oral omega-3 fatty acids. Epilepsy Behav. 17, 33–38 (2010).
Sánchez-Villegas, A. et al. The effect of the Mediterranean diet on plasma brain-derived neurotrophic factor (BDNF) levels: The PREDIMED-NAVARRA randomized trial. Nutr. Neurosci. 14, 195–201 (2011).
Belin, R. J. & He, K. Magnesium physiology and pathogenic mechanisms that contribute to the development of the metabolic syndrome. Magnes. Res. 20, 107–129 (2007).
Song, Y. et al. Magnesium intake, C-reactive protein, and the prevalence of metabolic syndrome in middle-aged and older US women. Diabetes Care 28, 1438–1444 (2005).
Ajani, U. A., Ford, E. S. & Mokdad, A. H. Dietary fiber and C-reactive protein: Findings from national health and nutrition examination survey data. J. Nutr. 134, 1181–1185 (2004).
Zhang, H. & Tsao, R. Dietary polyphenols, oxidative stress and antioxidant and anti-inflammatory effects. Curr. Opin. Food Sci. 8, 33–42 (2016).
Zhang, J.-Y. et al. The association between glycemic index, glycemic load, and metabolic syndrome: A systematic review and dose-response meta-analysis of observational studies. Eur. J. Nutr. 59, 451–463 (2020).
Acknowledgements
The authors wish to thank all students who kindly participated in our study.
Funding
The financial support for conception, design, data analysis and manuscript drafting comes from Isfahan University of Medical Sciences, Isfahan, Iran (No. 3402104).
Author information
Authors and Affiliations
Contributions
M.J.A., D.P., S.A.T., F.S., Z.H., E.M., S.M., and P.S. contributed in conception, design, data collection, data interpretation, manuscript drafting, approval of the final version of the manuscript, and agreed for all aspects of the work.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Assi, M.J., Poursalehi, D., Tirani, S.A. et al. Legumes and nuts intake in relation to metabolic health status, serum brain derived neurotrophic factor and adropin levels in adults. Sci Rep 13, 16455 (2023). https://doi.org/10.1038/s41598-023-43855-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-43855-8
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
