
Abstract
The study was conducted to determine thecorrelation between the selected measures of aerobic physical efficiency and changes in the temple surface temperature in response to light and heavy exercise. 25 physically active men aged 19–25 were recruited for the study. They performed a graded exercise test on a cycle ergometer to measure maximum power (Pmax) and a test verifying the value of maximum oxygen uptake (VO2max). Then, two 3-min submaximal efforts with constant-intensity of 2.2 W·kgLBM−1 and 5 W·kgLBM−1, respectively were performed. During the constant-intensity efforts, the temperature of the temple surface was measured. Then, the difference between the temperature of the temple measured at the end of the exercise and the temperature measured at the beginning of the exercise was calculated (ΔT1-2.2, ΔT1-5, respectively). It was shown that ΔT1-2.2 correlated statistically significantly with VO2max (ml·min−1·kg−1) (r = 0.49; p = 0.01) and Pmax (W·kg−1) (r = 0.41, p = 0.04). Moreover, ΔT1-5 correlated statistically significantly with VO2max (l·min−1) (r = − 0.41; p = 0.04). Changes in body surface temperature in response to light exercise positively correlate with measurements of aerobic physical efficiency, such as VO2max and Pmax. When the exercise intensity is high (5 W·kgLBM−1), the correlation between exercise body temperature changes and VO2max becomes negative.
Similar content being viewed by others

Introduction
Cardiovascular fitness assessment is used, among other things, to predict the risk of early mortality due to cardiovascular failure1. The size and nature of the cardiovascular response to physical effort depends on the type of effort undertaken and the conditions in which the effort is undertaken. Numerous publications concern the reactions of the circulatory system and thermoregulation processes during and after efforts, undertaken in conditions of heat2,3 and cold4. It has also been researched how the type of exercise, its duration and intensity affect the process of the thermoregulation assessed on the basis of thermal radiation from the skin. In order to assess the efficiency of the circulatory system, measurements such as maximum/peak oxygen uptake (VO2max)5, heart rate recovery (HRR)6, exercise stroke volume (SV)7, sinus heart rate variability (HRV)8 are used. Previous articles have described the correlation between VO2max and changes in body surface temperature recorded during high-intensity exercise and those recorded during the recovery after high-intensity exercise9,10. The correlation of thermal parameters with heart rate recovery (HRR) and heart rate variability (HRV) recovery was also described10. Available reasearch9,10 indicates that body surface temperature measurement during exercise and recovery can be used to assess the efficiency of the circulatory system. There are two possible explanations for the above-described relationship between selected measures of cardiovascular fitness and the size of the thermal response to exercise. Firstly, an increase in the intensity of energy metabolism leads to increased production of thermal energy11. Energy metabolism in the efforts applied in the previous studies9,10 was largely dependent on the VO2max value, as the oxygen uptake in such efforts was recorded at a level close to VO2max12,13. Secondly, muscle and skin blood flow during exercise determines thermal energy transport to the body surface14, affecting the body surface temperature12. At the same time, muscle15 and skin14 blood flow during exercise are conditioned by the stroke volume, which is one of the determinants of VO2max15. Moreover, efficiently removing thermal energy may alleviate physiological stress and thus affect HRR and HRV recovery10.
So far9, thermal parameters measured at body surface were assessed in a test similar to sprint interval training, consisting of 4 efforts of 30 s each, performed at maximum intensity. Such a test leads to a significant disturbance of the acid–base balance16, and high production of phosphates and ammonia, which contribute to the rapid development of fatigue17,18. Therefore, this form of testing is very burdensome to the subjects. In addition, sprinting efforts such as the Wingate test may sometimes lead to syncope 19. For the reasons above, it was reasonable to look for a different research protocol to assess changes in body temperature induced by exercise. In subsequent studies, it was proposed to perform a more extended effort, lasting 3 min, with a power of 110% of the maximum power of the progressive test (110% Pmax)10. Such efforts lead to lower blood lactate levels20 compared to repeated sprints lasting 30 s each14. In addition, efforts performed with a power of 110% Pmax are used in performance diagnostics to verify peak oxygen uptake obtained in progressive tests13,21. However, the procedure described by Jastrzębska et al.10 has some shortcomings. First of all, it requires the subjects to make two visits 24 h apart in the laboratory, forcing them to submit to the guidelines during the entire research process (no stimulants, sleep time, etc.). Secondly, in this procedure, circulatory fitness is already assessed in the progressive test (GXT) on the basis of peak oxygen uptake, so performing an indirect assessment of circulatory fitness on the basis of thermal parameters in a test performed the next day seems to have little merit. In view of the above, it seems reasonable to seek an alternative procedure. Such a procedure should not require the prior use of a progressive test as a test to determine the intensity of effort for thermal performance.
Previous studies conducted by the team used high- and very high-intensity efforts. A sprint interval training test (4 × 30 s with maximum power)9 or a 3-min maximum effort with a power of 110% of Pmax determined in the progressive test are efforts intended for athletes. People who do not train, with low physical activity will not be able to properly perform the above-mentioned efforts due to too low muscle strength of the lower limbs and too rapid increase of fatigue22. Taking into account the fact that circulatory failure often affects people with lower physical activity and thus a lower level of physical efficiency, it seems right to look for a relationship between non-invasively measured thermal parameters from the body surface in response to efforts with submaximal intensities and parameters already used in the assessment of cardiovascular fitness.
In the search for the right test procedure, selecting the intensity of the effort is the key. It has been shown that maximum power in progressive exercise tests23, as well as oxygen uptake, and the intensity of energy metabolism during rest and submaximal work correlate with lean body mass24. Therefore, we decided that power in submaximal efforts shall be normalized to lean body mass. The study aimed to determine the strength of the relationship between selected measures of cardiovascular fitness and changes in body surface temperature recorded during light and heavy exercise of constant intensity normalized to lean body mass in young people. We assumed that exercise and recovery changes in body surface temperature would correlate with VO2max, Pmax and HRR.
Material and methods
Participants
25 non-smoking men aged 19–25 were recruited to participate in the study. Participants were enrolled into the study on the condition of participation in intensity spinning training. It was assumed that the participants would be excluded upon any threat to their health and wellbeing. In order to assess those:
-
Medical history of each participant was gathered, with special emphasis of cardiovascular and respiratory system
-
Resting blood pressure was measured before each effort test. It was assumed that individuals with diagnosed hypertension will be excluded from the effort tests. Hypertension was defined as the value of diastolic pressure over 90 mmHg and systolic pressure exceeding 140 mmHg, as reported by Schweiger et al.25. We accepted a margin of few mmHg because of the influence of stress on blood pressure26. Resting pulse rate was measured for each participant before taking the effort tests to exclude any individuals with tachycardia.
Additionally, each participant was required to take antigen test against COVID19 IgM. Any participant with positive results of such test were excluded from the study. The characteristics of the participants are presented in Table 1. All the subjects had participated in training on spinning bikes twice a week, for 60 min, for at least 6 months preceding the study. During that time, two types of trainings were undertaken. The first type consisted of HIIT trainings incorporating several maximum-effort trainings lasting 3–4 min, intermitted with active resting. The other type was threshold trainings consisted of high-intensity efforts close to functional threshold power (FTP), intermitted with active resting. Preliminary analysis of physical efficiency of the participants consisted of reviewing their FTP data, as defined in the procedure reported by Klitzke Borszcz et al.27 in 20-min maximal effort. The average FTP was 3.07 ± 0.59 W∙kg−1.
Test procedure
Before the study, the consent of the University Ethics Committee was obtained for implementing the project described in this work (Consent number: 39/2019). After the study procedures were explained, written informed consent has been obtained from all participants. The study consisted of three exercise tests. On the first day, a progressive test was performed, and then, after a 24-h break, a test verifying the VO2max value was performed, according to the previously described procedure13. After another 72 h, a test consisting of two submaximal efforts was performed. Study participants were instructed to have at least 9-h long night rest, abstain from alcohol, caffeine and intense physical effort for 48 h prior to the study and between each laboratory test. Participants were advised to intake at least 100 g carbohydrates in 3 h prior to the effort tests. In the course of effort tests and 48 h prior to the fist test, paricipants were asked to ingest 1.2–1.4g/kg of protein28, 3000 kcal29, and drink at least 2 l of water.
Graded exercise test (GXT)
Prior to the graded exercise test, body composition was measured using near-infrared Futrex 6100/XL analyzer (Futrex, Hagerstown, USA). The analyzer head was applied to the anterior midline and in the midway of the biceps brachii of the dominant hand using the measure provided by the manufacturer. Then the measurement of the body fat content expressed in kilograms, the percentage of body weight, and lean body mass (LBM) was performed. The analyzer was calibrated prior to each measurement with the manufacturer-supplied optical standard. Before GXT and directly after the test, blood pressure was measured with aneroid sphygmomanometer (Riester, Germany). All measurements were taken by the same person to avoid any bias. Subsequently, initial and post-exercise stroke volume (SV) was measured with the following formula30:
where SV—stroke volume (ml), PP—the difference between post-exercise systolic and diastolic blood pressure (mm Hg), DBP–post-exercise diastolic pressure (mm Hg).
The GXT was conducted on a Lode Excalibur Sport ergometer (Lode BV Groningen, Netherlands), calibrated before the study started. The effort began with a load of 50 W. Every 3 min, the load was increased by 50 W until the subject refused to continue the effort or until the pedaling rate fell below 60RPM. If a participant was unable to complete an entire 3 min stage, 0.28 W per second missed was subtracted from the work rate at that stage. The highest power output determined in the GXT was taken to be the measure of maximal aerobic power (Pmax). During the test, respiratory parameters were measured using a Quark CPET ergo spirometer (Cosmed, Milan, Italy). The ergo spirometer was calibrated before testing with a standard gas mixture of 5% carbon dioxide, 16% oxygen, and 79% nitrogen. Breathing air was analyzed breath-by-breath to measure oxygen uptake (VO2) and carbon dioxide excretion (VCO2). The measurements were then averaged over 30-s intervals. The highest oxygen uptake value obtained was considered the peak oxygen uptake in the GXT (VO2peak1).
VO2max value was verified with a test with a power of 110% Pmax following the previously described procedure13 on the day following the GXT. As in the graded exercise test, respiratory parameters were measured during the verification test. The parameters were then averaged in 30-s intervals. The highest oxygen uptake value obtained in the verification test was considered the peak oxygen uptake of this test (VO2peak2). Subsequently, the higher value of VO2peak1 and VO2peak2 was considered the maximum oxygen uptake (VO2max).
The constant-intensity exercise test consisted of two exercises lasting 3 min each and was performed with an intensity of 2.2 W∙kg−1 of lean body mass (2.2 W∙kgLBM−1) and 5 W∙kgLBM−1, respectively. The intensity of the efforts was selected in W∙kgLBM−1 because muscle power depends on lean body mass31. By normalizing the load considering LBM, we intended to obtain similar work intensity for each subject. The load sizes were selected based on the data from the GXT. In the GXT we did not observe an increase in lactate concentration above 2 mmol l−1, nor an increase in VE∙VO2–1 equivalent in any of the subjects up to an intensity of ≈ 2.2 W∙kgLBM−1. Therefore, based on the criteria described by MacIntosh et al.32, we considered an effort of 2.2 W∙kgLBM−1 to be a low-intensity effort. We then determined that at an intensity of ≈ 5 W∙kgLBM−1, none of the subjects was able to continue the GXT. Therefore, we considered the intensity of 5 W∙kgLBM−1 as a heavy effort. Each of the efforts mentioned above was followed by a passive break lasting 7 min. Figure 1 shows the scheme of the submaximal efforts test.

Diagram showing the course of a constant-intensity exercise test.
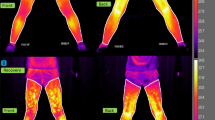
During the constant-intensity exercise test, the density of thermal radiation from the body surface was measured using a Sonel KT384 thermal imaging camera (Sonel SA, Świdnica, Poland). The camera has a resolution of IR 384 × 288, a spectral range of 8−14 μm, thermal sensitivity of 0.08 ℃. The software provided by the manufacturer (Sonel ThermoAnalyze) converted the radiation density into body surface temperature expressed in ℃. During the playback of the recorded video, individual frames were analyzed. The average temperature was recorded within a square field (10 pixels on a side), marked individually on the temple, as in previous publications9,10. The center of the thermal analysis field was located halfway between the hairline and the end of the eyebrow arch. The lower edge of the analysis field was located at the height of the lateral end of the brow arch. Immediately before the start of each test effort, the initial temperature of the temple surface was indicated (T-2.2baseline, T-5baseline). Subsequent measurements of the temple surface temperature were made immediately after each test effort (T-2.2end, T-5end) and after 2 min of recovery after each test effort (T-2.2rest, T-5rest). Then, the differences between T-…end and T-…baseline were calculated for each test effort (ΔT1-2.2; ΔT1-5, respectively) and the differences between T-…rest and T-…end (ΔT2-2.2; ΔT2-5, respectively), similar to the calculations made by Jastrzębska et al.10.
The heart rate was recorded using a V800 cardiofrequency meter (Polar, Oy, Finland). Based on the heart rate recording, the contraction rates were indicated for 1′ (HRR1′), 2′ (HRR2′), 3′ (HRR3′), 4′ (HRR4′), 5′ (HRR5′) and 6′ (HRR6′) minutes of restitution after each test effort. Then, changes in heart rate during recovery were calculated as the difference between the heart rate measured in the final phase of each test effort and the corresponding recovery value: HRR1′ (ΔHRR1′), HHR2′ (ΔHRR2′), HRR3′ (ΔHRR3′), HRR4 (ΔHRR4′), HRR5′ (ΔHRR5′), HRR6′ (ΔHRR6′), similar to Suzic Lazic et al.33.
Statistical analysis
Statistical analysis and visualisations of the data were prepared using Statistica 13 software (Statsoft Polska, Cracow, Poland). The Shapiro–Wilk W test was used to evaluate the measured data distribution. Only post-exercise SV normalized to body weight and LBM differed significantly from the normal distribution. Repeated measures analysis of variance was used to assess the differences between T-…baseline, T-…end, T-…rest at each intensity of the submaximal exercise test.
Strength of the relationship between changes in the temple surface temperature and measures of cardiovascular fitness (and physical efficiency) was determined using the simple Pearson correlation. For the data statistically different from normal distribution Spearman rank test was used.
Using the formula for the critical value of the correlation coefficient, the minimum group size was calculated, assuming that the acceptable level of statistical significance (α) is 0.05 and the correlation strength should be very high (r ≥ 0.7). The following formula was used:
Based on this, we determined that the minimum number of participants is 8 at t ≈ 2.44.
Institutional review board statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by Ethics Committee of the University School of Physical Education in Wroclaw (protocol code: 39/2019; date of approval: 26 November 2019).
Results
Table 2 presents the basic statistics of the analyzed variables. The effect of repeated measurements on the temple surface temperature during exercise with a power of 2.2 W∙kgLBM−1 was not detected. The effect of repeated measurements was demonstrated for the temperature of the temple surface during exercise with a power of 5 W∙kgLBM−1 (F = 12.70; η2 = 0.35; p = 0.00). A post hoc test revealed a statistically significant difference between T-5end and either T-5baseline or T-5rest.
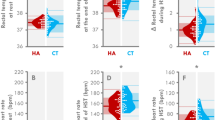
A statistically significant correlation (r = 0.49; p < 0.05) was found between ΔT1-2.2 and VO2max expressed in ml min−1 kg−1 (Fig. 2B). The correlations between ΔT1-2.2 and the other parameters (Fig. 2A,D,E,F) were trivial (r = 0.1–0.3) or moderate (Fig. 2C) (r > 0.03) and statistically insignificant. In the analysis of the effort with an intensity of 5 W∙kgLBM−1, a statistically significant correlation (r = − 0.41; p < 0.05) was found only between ΔT1-5 and VO2max expressed in min−1 (Fig. 3A). The correlations with other parameters were insignificant with level of strength weak (r < 0.1; Fig. 3F), trivial (r = 0.1–0.3; Fig. 3B–E).

Pearson’s correlation plots between maximal oxygen uptake and changes in body surface temperature during exercise with an intensity of 2.2 W·kgLBM−1.

Pearson’s correlation plots between maximal oxygen uptake and body surface temperature changes during 5 W·kgLBM−1 intensity exercise.
Baseline SV normalized to body weight and LBM correlated with ΔT1-2.2 (Table 3). In the analyses concerning the GXT maximum power, a statistically significant correlation was found only between ΔT1-2.2 and Pmax expressed in W kg−1. In addition, a correlation with the required threshold of statistical significance was found between HRR1’ and ΔT2-2.2 and between HRR3’ and ΔT1-5 (Table 3).
Discussion
It is assumed that during short-term and intense exercise, skin blood flow decreases due to vasoconstriction, which has been described by several authors34,35,36. The decreasing volume of skin blood flow causes the temperature of the body surface to decrease during short-term and intense exercise performed at the ambient temperature of approx. 20 °C2. Also, the studies described in this paper showed that the body surface temperature decreased immediately after the exercise with the power of 5 W∙kgLBM−1. Comparative studies revealed differences between athletes and untrained people in the dynamics of exercise changes in body surface temperature37,38. Moreover, negative correlations were found between selected parameters of cardiovascular fitness (and physical capacity) and thermal responses to exercise9,10. The results of these correlations indicated that high efficiency of the circulatory system is associated with a relatively significant decrease in temple temperature during exercise. The data presented herein confirm the previous findings, as we obtained a statistically significant negative correlation between ΔT1-5 and VO2max expressed in absolute values.
The statistical analysis results for the data recorded during exercise with a power of 2.2 W∙kgLBM−1 indicate a positive correlation between ΔT1-2.2 and Pmax normalized to body weight and a positive correlation between ΔT1-2.2 and VO2max normalized to body weight. In addition, a positive correlation between ΔT1-2.2 and SVbaseline normalized to body weight and normalized to LBM was demonstrated. The direction of this correlation is opposite to the compounds described by Hebisz et al.9, Jastrzębska et al.10 and the relationships described above regarding the effort with the power of 5 W∙kgLBM−1. We believe that the reason for obtaining the opposite direction of correlation for the data collected during exercise with the power of 2.2 W∙kgLBM−1 is the use of lower intensity of the test effort compared to Hebisz et al.9 and Jastrzębska et al.10. As mentioned above, during high-intensity exercise, in its initial phase, body surface temperature decreases2. However, if the exercise is of low intensity, in its initial phase, the decrease in body surface temperature is smaller than during intense exercise2. These differences may be due to different blood flow patterns depending on the intensity of exercise performed12,36. In addition, during light exercise, after a temporary decrease, blood flow begins to increase36, which can increase body surface temperature. The correlation results presented in this paper indicate that the magnitude of the increase in body surface temperature during low-intensity exercise is related to the level of aerobic capacity.
When exercise is short-term and intense, the body surface temperature measured immediately after exercise is lower than that measured before exercise10. Then, a significant increase in body surface temperature is observed during the recovery after exercise9,10. It was also shown that recovery changes in temple temperature after intense exercise strongly and positively correlated with measures of cardiovascular fitness and aerobic physical efficiency9,10. This study showed that the change in body surface temperature was statistically significantly correlated only with HRR1 after exercise with an intensity of 2.2 W kgLBM−1. Therefore, the data presented in this paper indicate that the relationship between ΔT2 and the applied measures of physical capacity is insignificant. The only correlation that reached the required level of statistical probability concerns the value of the heart rate measured at restitution. This is a negligible effect because it was assumed that heart rate recovery is strongly related to cardiovascular fitness when analyzed as ΔHRR39,40. Therefore, the analysis of ΔT2 after exercise with a power less than or equal to 5 W∙kgLBM−1 is not an efficient way to assess the efficiency of the cardiovascular system.
The correlations presented in this work indicate that approx. 17–24% of exercise capacity (VO2max or Pmax) can be explained by exercise thermal responses to efforts less than or equal to 5 W∙kgLBM−1. Earlier studies, which used exercise tests of greater intensity, exceeding the power of the progressive test, achieved greater correlation strength9,10 however they were performed by cyclists, characterized by higher physical capacity. Therefore, we believe that the test procedure used in this study does not allow for accurate diagnosis of cardiovascular fitness or aerobic physical capacity using ΔT1 or ΔT2 in efforts performed with an intensity of up to 5 W∙kgLBM−1. For diagnostic purposes, it may be better to measure changes in body surface temperature during efforts of greater intensity than 5 W∙kgLBM−1, as was done in the study by Hebisz et al.9 and Jastrzębska et al.10.
Limitations. The main reasoning behind this study is demonstrating the relationship between post-exercise changes in body surface temperature and measures of cardiovascular fitness. Due to the low power of the relationships described in this study is moderate, further research may be warranted to eliminate the methodological limitations of our research. The study sample of 25 men is relatively small, which makes it difficult to generalize the conclusions resulting from the research performed. Therefore, research planned in the future should include the recruitment of a larger research group. Moreover, we couldn’t control if participants implemented our recommendations on the amount of sleep and the principles of nutrition during the study period. This is a significant limitation of our research, as sleep has a considerable impact on restitution processes such as muscle regeneration, nervous system and immune system41, and sleep deprivation impairs athletes’ performance42. Therefore, future studies with short time between exercise tests will have to implement monitoring of the quality of sleep.
Conclusions.
Changes in body surface temperature in response to exercise positively correlate with measures of aerobic exercise capacity, such as VO2max and Pmax, when exercise is of moderate intensity. When the exercise intensity is high (5 W kgLBM−1), the correlation between exercise body temperature change and VO2max becomes negative. These results indicate that the relationship between body surface temperature and aerobic physical performance depends on the intensity of the test effort. The strength of these correlations is too low to be used to determine aerobic exercise capacity based on temporal thermal radiation. Other papers have found correlations at the level of ≈ 0.8–0.9 between VO2max and submaximal VO2 measured at the anaerobic threshold or at the respiratory compensation point43 or correlations at the level of ≈ 0.9 between VO2max and HRmax∙HRrest−144 among people with a similar level of performance to our research group. Finally, futer studies shoul investigate the potential role of thermoregulatory efficiency in the relationshoi between body surface temperature and aerobic exercise capacity.
Data availability
The data presented in this study are available on request from the corresponding author.
References
Raghuveer, G. et al. American Heart Association young hearts athero, hypertension and obesity in the young committee of the council on lifelong congenital heart disease and heart health in the young. Cardiorespiratory fitness in youth: An important marker of health: A scientific statement from the American Heart Association. Circulation 142(7), e101–e118. https://doi.org/10.1161/CIR.0000000000000866 (2020).
Périard, J. D., Eijsvogels, T. M. H. & Daanen, H. A. M. Exercise under heat stress: thermoregulation, hydration, performance implications, and mitigation strategies. Physiol. Rev. 101(4), 1873–1979. https://doi.org/10.1152/physrev.00038.2020 (2021).
Kenney, W. L., Wolf, S. T., Dillon, G. A., Berry, C. W. & Alexander, L. M. Temperature regulation during exercise in the heat: Insights for the aging athlete. J. Sci. Med. Sport 24(8), 739–746. https://doi.org/10.1016/j.jsams.2020.12.007 (2021).
Chen, F., Fu, M., Li, Y., Shen, S. & Guo, X. Modelling and experimental study of thermo-physiological responses of human exercising in cold environments. J. Thermal Biol. 109, 103316. https://doi.org/10.1016/j.jtherbio.2022.103316 (2022).
Hansen, M. T. et al. Accuracy of a clinical applicable method for prediction of VO2max using seismocardiography. Int. J. Sports Med. 44(9), 650–656. https://doi.org/10.1055/a-2004-4669 (2023).
Fan, L. M., Collins, A., Geng, L. & Li, J. M. Impact of unhealthy lifestyle on cardiorespiratory fitness and heart rate recovery of medical science students. BMC Public Health 20(1), 1012. https://doi.org/10.1186/s12889-020-09154-x (2020).
Nystoriak, M. A. & Bhatnagar, A. Cardiovascular effects and benefits of exercise. Front. Cardiovasc. Med. 5, 135. https://doi.org/10.3389/fcvm.2018.00135 (2018).
Souza, H. C. D., Philbois, S. V., Veiga, A. C. & Aguilar, B. A. Heart rate variability and cardiovascular fitness: What we know so far. Vasc. Health. Risk. Manag. 17, 701–711. https://doi.org/10.2147/VHRM.S279322 (2021).
Hebisz, R., Hebisz, P., Borkowski, J., Wierzbicka-Damska, I. & Zatoń, M. Relationship between the skin surface temperature changes during sprint interval testing protocol and the aerobic capacity in well-trained cyclists. Physiol. Res. 68(6), 981–989. https://doi.org/10.33549/physiolres.934114 (2019).
Jastrzębska, A. D., Hebisz, R. & Hebisz, P. Temporal skin temperature as an indicator of cardiorespiratory fitness assessed with selected methods. Biology (Basel). 11(7), 948. https://doi.org/10.3390/biology11070948 (2022).
Kenny, G. P. & McGinn, R. Restoration of thermoregulation after exercise. J. Appl. Physiol. 122(4), 933–944. https://doi.org/10.1152/japplphysiol.00517.2016 (2017).
Hebisz, R., Hebisz, P., Zatoń, M. & Michalik, K. Peak oxygen uptake in a sprint interval testing protocol vs. maximal oxygen uptake in an incremental testing protocol and their relationship with cross-country mountain biking performance. Appl. Physiol. Nutr. Metab. 42(4), 371–376. https://doi.org/10.1139/apnm-2016-0362 (2017).
Hebisz, P., Jastrzębska, A. D. & Hebisz, R. Real assessment of maximum oxygen uptake as a verification after an incremental test versus without a test. Front. Physiol. 12, 739745. https://doi.org/10.3389/fphys.2021.739745 (2021).
Low, D. A., Jones, H., Cable, N. T., Alexander, L. M. & Kenney, W. L. Historical reviews of the assessment of human cardiovascular function: interrogation and understanding of the control of skin blood flow. Eur. J. Appl. Physiol. 120(1), 1–16. https://doi.org/10.1007/s00421-019-04246-y (2020).
Joyner, M. J. & Casey, D. P. Regulation of increased blood flow (hyperemia) to muscles during exercise: A hierarchy of competing physiological needs. Physiol. Rev. 95(2), 549–601. https://doi.org/10.1152/physrev.00035.2013 (2015).
Hebisz, R., Hebisz, P., Borkowski, J. & Zatoń, M. Differences in physiological responses to interval training in cyclists with and without interval training experience. J. Hum. Kinet. 50, 93–101. https://doi.org/10.1515/hukin-2015-0147 (2016).
Ulupınar, S. et al. Effects of sprint distance and repetition number on energy system contributions in soccer players. J. Exerc. Sci. Fit. 19(3), 182–188. https://doi.org/10.1016/j.jesf.2021.03.003 (2021).
Morcillo, J. A. et al. Relationships between repeated sprint ability, mechanical parameters, and blood metabolites in professional soccer players. J. Strength Cond. Res. 29(6), 1673–1682. https://doi.org/10.1519/JSC.0000000000000782 (2015).
Horiuchi, M., Nishida, A., Dobashi, S. & Koyama, K. Comparisons between normobaric normoxic and hypoxic recovery on post-exercise hemodynamics after sprint interval cycling in hypoxia. Front. Physiol. 13, 843574. https://doi.org/10.3389/fphys.2022 (2022).
Messonnier, L. A., Chatel, B., Emhoff, C. W., Blervaque, L. & Oyono-Enguéllé, S. Delayed rebound of glycemia during recovery following short-duration high-intensity exercise: Are there lactate and glucose metabolism interactions?. Front. Nutr. 8, 734152. https://doi.org/10.3389/fnut.2021.734152 (2021).
Follador, L. et al. Physiological, perceptual, and affective responses to six high-intensity interval training protocols. Percept. Mot. Skills. 125(2), 329–350. https://doi.org/10.1177/0031512518754584 (2018).
Villanueva, I. R. et al. Comparison of constant load exercise intensity for verification of maximal oxygen uptake following a graded exercise test in older adults. Physiol. Rep. 9(18), e15037. https://doi.org/10.14814/phy2.15037 (2021).
Maciejczyk, M., Wiecek, M., Szymura, J., Szygula, Z. & Brown, L. E. Influence of increased body mass and body composition on cycling anaerobic power. J. Strength Cond. Res. 29(1), 58–65. https://doi.org/10.1519/JSC.0000000000000727 (2015).
Pourhassan, M. et al. Relationship between submaximal oxygen uptake, detailed body composition, and resting energy expenditure in overweight subjects. Am. J. Hum. Biol. 27(3), 397–406. https://doi.org/10.1002/ajhb.22666 (2015).
Schweiger, V., Niederseer, D., Schmied, C., Attenhofer-Jost, C. & Caselli, S. Athletes and hypertension. Curr. Cardiol. Rep. 23(12), 176. https://doi.org/10.1007/s11886-021-01608-x (2021).
Wright, B. J., O’Brien, S., Hazi, A. & Kent, S. Increased systolic blood pressure reactivity to acute stress is related with better self-reported health. Sci. Rep. 4, 6882. https://doi.org/10.1038/srep06882 (2014).
Klitzke Borszcz, F., Tramontin, A. F. & Costa, V. P. Reliability of the functional threshold power in competitive cyclists. Int. J. Sports Med. 41(3), 175–181. https://doi.org/10.1055/a-1018-1965 (2020).
Kato, H., Suzuki, K., Bannai, M. & Moore, D. R. Protein requirements are elevated in endurance athletes after exercise as determined by the indicator amino acid oxidation method. PLoS ONE 11(6), e0157406. https://doi.org/10.1371/journal.pone.0157406 (2016).
Burke, L. M., Hawley, J. A., Wong, S. H. & Jeukendrup, A. E. Carbohydrates for training and competition. J. Sports Sci. 29(Suppl 1), 17–27. https://doi.org/10.1080/02640414.2011.585473 (2011).
Mokasheva, E. N. et al. Rapid assessment of cardiovascular system parameters using cardiorespiratory indices. Biol. Bull. Rev. 13, 310–315. https://doi.org/10.1134/S2079086423040072 (2023).
Coelho-E-Silva, M. J. et al. Allometric modeling of Wingate test among adult male athletes from combat sports. Medicina (Kaunas) 56(9), 480. https://doi.org/10.3390/medicina56090480 (2020).
MacIntosh, B. R., Murias, J. M., Keir, D. A. & Weir, J. M. What is moderate to vigorous exercise intensity?. Front. Physiol. 12, 682233. https://doi.org/10.3389/fphys.2021.682233 (2021).
Suzic Lazic, J. et al. Heart rate recovery in elite athletes: The impact of age and exercise capacity. Clin. Physiol. Funct. Imaging 37(2), 117–123. https://doi.org/10.1111/cpf.12271 (2017).
Johnson, J. M. Exercise and the cutaneous circulation. Exerc. Sport Sci. Rev. 20, 59–97 (1992).
Kamon, E. & Belding, H. S. Dermal blood flow in the resting arm during prolonged leg exercise. J. Appl. Physiol. 26(3), 317–320 (1969).
Simmons, G. H. et al. Increased brachial artery retrograde shear rate at exercise onset is abolished during prolonged cycling: Role of thermoregulatory vasodilation. J. Appl. Physiol. (1985) 110(2), 389–397. https://doi.org/10.1152/japplphysiol.00936.2010 (2011).
Formenti, D. et al. Thermal imaging of exercise-associated skin temperature changes in trained and untrained female subjects. Ann. Biomed. Eng. 41(4), 863–871. https://doi.org/10.1007/s10439-012-0718-x (2013).
Galan-Carracedo, J., Suarez-Segade, A., Guerra-Balic, M. & Oviedo, G. R. The dynamic and correlation of skin temperature and cardiorespiratory fitness in male endurance runners. Int. J. Environ. Res. Public. Health. 16(16), 2869. https://doi.org/10.3390/ijerph16162869 (2019).
Hirsh, D. S. et al. Association of heart rate recovery and maximum oxygen consumption in patients with chronic congestive heart failure. J. Heart Lung Transplant. 25(8), 942–945. https://doi.org/10.1016/j.healun.2006.04.006 (2006).
Pakkala, A., Veeranna, N. & Kulkarni, S. B. A comparative study of cardiopulmonary efficiency in athletes and non-athletes. J. Indian Med. Assoc. 103(10), 522–527 (2005).
Taheri, M. & Valayi, F. Aerobic exercise improves attention and quality of sleep among professional volleyball players. Sleep Hypn. 21(1), 69–72. https://doi.org/10.5350/Sleep.Hypn.2019.21.0174 (2019).
Paryab, N., Taheri, M., Irandoust, K. & Mirmoezzi, M. Effects of melatonin on neurological function and maintenance of physical and motor fitness in collegiate student-athletes following sleep deprivation. Int. J. Sport Stud. Health. 3(2), e110657. https://doi.org/10.5812/intjsh.110657 (2020).
Wiecha, S. et al. VO2max prediction based on submaximal cardiorespiratory relationships and body composition in male runners and cyclists: A population study. Elife 12, e86291. https://doi.org/10.7554/eLife.86291 (2023).
Uth, N., Sørensen, H., Overgaard, K. & Pedersen, P. K. Estimation of VO2max from the ratio between HRmax and HRrest–the Heart Rate Ratio Method. Eur. J. Appl. Physiol. 91(1), 111–115. https://doi.org/10.1007/s00421-003-0988-y (2004).
Acknowledgements
We would like to express our gratitude to Anna Janicka and Maciej Rymarczyk for their support with data collection during the study.
Funding
This work was supported by the University School of Physical Education in Wrocław under Grant Number PN/BK/2020/07.
Author information
Authors and Affiliations
Contributions
A.D.J., R.H. and P.H.: conceptualization; A.D.J., R.H. and P.H.: project administration; R.H. and P.H.: methodology; A.D.J., R.H. and P.H.: collected data; R.H.: validation; R.H.: visualization, R.H.: writing-original draft preparation A.D.J. and P.H.: writing-review, and editing; A.D.J.: supervision. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Jastrzębska, A.D., Hebisz, R. & Hebisz, P. Assessing aerobic physical efficiency through temple surface temperature measurements during light, heavy exercise, and recovery. Sci Rep 13, 15882 (2023). https://doi.org/10.1038/s41598-023-43012-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-43012-1
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
