
Abstract
Detecting when others are looking at us is a crucial social skill. Accordingly, a range of gaze angles is perceived as self-directed; this is termed the “cone of direct gaze” (CoDG). Multiple cues, such as nose and head orientation, are integrated during gaze perception. Thus, occluding the lower portion of the face, such as with face masks during the COVID-19 pandemic, may influence how gaze is perceived. Individual differences in the prioritisation of eye-region and non-eye-region cues may modulate the influence of face masks on gaze perception. Autistic individuals, who may be more reliant on non-eye-region directional cues during gaze perception, might be differentially affected by face masks. In the present study, we compared the CoDG when viewing masked and unmasked faces (N = 157) and measured self-reported autistic traits. The CoDG was wider for masked compared to unmasked faces, suggesting that reduced reliability of lower face cues increases the range of gaze angles perceived as self-directed. Additionally, autistic traits positively predicted the magnitude of CoDG difference between masked and unmasked faces. This study provides crucial insights into the effect of face masks on gaze perception, and how they may affect autistic individuals to a greater extent.
Similar content being viewed by others

Introduction
Eye gaze is a salient social cue. It reveals the focus of another individual’s attention, and, importantly, whether or not we are the focus of their attention. Thus, successful navigation of our social world depends on our ability to efficiently discern the focus of others’ gaze. Given its important role, it is perhaps not surprising that humans can detect subtle differences in gaze direction1,2 and are sensitive to detecting direct gaze from an early age3. This efficient detection of direct gaze plays an important role in the ability to understand the actions and intentions of others4.
While the ability to detect direct gaze is well refined, a liberal range of gaze angles is typically perceived as being self-directed (e.g.5,6,7). The range of gaze angles that one perceives as being self-directed is termed the “cone of direct gaze” (CoDG5). The width of the CoDG is approximately 9.55° in horizontal diameter (e.g.5,8), which broadly corresponds with the width of the human face9. Under more ambiguous conditions (e.g. gaze viewed from afar or in the dark) the width of the CoDG may be wider. Thus, when observers are less certain regarding where another individual is looking, they adopt a more liberal criterion and tend to overestimate the range of gaze angles perceived as being directed towards themselves10,11,12. Indeed, Balsdon and Clifford8 found that observers were more likely to judge gaze as direct in stimuli with increasing levels of eye-region noise (i.e. reduced reliability); faces wearing transparent sunglasses were least likely to lead observers to overestimate the range of gaze angles perceived as being directed towards them (i.e. a direct gaze bias), while opaque sunglasses were most likely to lead to a direct gaze bias. This overestimation of direct gaze under conditions of uncertainty minimises the risk of missing potential social interactions or failing to identify possible social threats. These are both, arguably, higher costs to pay than mistakenly perceiving averted gaze as direct7.
Although an individual’s CoDG width is a relatively stable trait13, there is considerable between-participant variability in the range of gaze angles perceived as self-directed (e.g.6,14,15,16). Certain characteristics may make observers more likely than others to perceive gaze as direct. For instance, individuals with high levels of social anxiety tend to exhibit a wider CoDG than those with lower levels of social anxiety6,17,18. In contrast, individuals with more autistic traits possess a narrower CoDG, suggesting that they are less likely than those with fewer autistic traits to overestimate direct gaze19. However, other studies report conflicting results; for example, Pell and colleagues20 found that individuals with Autism Spectrum Conditions (ASC) were as likely as non-autistic individuals to overestimate the perception of direct gaze when eye-region information was unreliable (i.e. when noise was added to the eye-region of faces).
Accurate gaze judgements are not based solely on the eye region, and can necessitate the integration of various directional cues, such as the angle of the nose7,21, and the direction in which the head22,23,24,25 or body26 is pointing. Misalignment between these different directional cues causes increased gaze uncertainty, resulting in an overestimation of direct gaze in averted compared to direct-facing heads11,25.
The relevance of different cues (e.g. eye orientation, head orientation, nose angle, or body orientation) during gaze perception, and their relative weightings, varies depending on the viewing condition5, context8, frame of reference27, and the cue’s reliability28. For instance, reduced reliability of, and consequently, increased observer uncertainty in, one cue (e.g. the eyes) likely reduces its relative weighting while increasing the weighting of another cue (e.g. the head)5. Perrett and colleagues28 suggest that while directional cues from the eyes are weighted heavily as a default, increased weighting is assigned to head orientation when information from the eyes is unreliable (e.g. when viewed from afar). Thus, under conditions where the reliability of eye-region cues is reduced, observers (1) exhibit a wider CoDG, and (2) rely more heavily on other available directional cues.
There is also evidence of individual differences in the relative weighting assigned to different directional cues. While non-autistic individuals weight eye-region cues more heavily than head orientation cues, autistic individuals may weight directional information from the body and head more than the eye-region29,30. Consistent with such findings, autistic individuals tend to exhibit a reduced propensity to fixate on the eye-region (e.g.31,32,33) and an increased propensity to fixate on the mouth-region in certain contexts (e.g.31). This pattern of decreased attention to the eye-region could be explained by the gaze aversion or gaze indifference hypotheses. Individuals exhibiting gaze aversion may purposefully avoid looking at others’ eyes because they find them aversive34,35,36,37. In contrast, individuals exhibiting gaze indifference may look less towards others’ eyes because they are not sensitive to the social significance of gaze38,39,40.
As multiple cues are integrated during gaze perception, it is possible that a reduction in the reliability of any cue, not just the eye-region, may influence the way in which gaze is perceived. While several studies have examined how eye-region reliability influences gaze perception (e.g.8,10), little is known about how a reduction in the reliability of other directional cues affects the perception of gaze. This is particularly relevant to investigate in the autistic population as autistic observers may rely less on eye-region cues for gaze perception, and thus might be disproportionately affected by a reduction in the reliability of other directional cues.
In many countries, the use of face masks was mandated during the COVID-19 pandemic in order to limit the spread of the virus among the population. As they occlude a large portion of the face, these masks could significantly affect social perception and interaction. Indeed, face masks impair the ability to recognise familiar and unfamiliar faces41,42, emotional facial expressions (43,44 though see45), and the intelligibility of speech46.
A recent study found that face masks do not alter gaze cueing of attention47; however, it is possible that the precision with which gaze is perceived may be reduced when directional cues from the lower face (e.g. nose angle) are occluded. This would manifest as increased gaze ambiguity and, consequently, an overestimation of direct-gaze (i.e. an increase in the width of the CoDG). Indeed, two recent studies, published subsequent to completion of data collection for the present study, reported an increase in the width of the CoDG when perceiving gaze in masked compared to unmasked faces48,49. Additionally, the relative extent to which people weight eye-region and non-eye-region cues during gaze perception could affect the extent to which face masks impact their perception of gaze direction. For example, in line with the gaze aversion hypothesis34,35,36,37, autistic individuals, who may rely more heavily on non-eye-region directional cues (e.g. nose angle or head orientation) during gaze perception, might not shift their gaze to the eye-region when non-eye-region cues are occluded. Consequently, they may experience increased gaze ambiguity, and thus a larger increase in CoDG width. Alternatively, in line with the gaze indifference hypothesis38,39,40, the presence of face masks could induce autistic individuals to attend more to the, arguably, more informative eye-region cues. Such an effect might reduce the influence of other directional cues, resulting in more sensitive perception of direct gaze, and thus a narrower CoDG.
Few studies have examined how face masks, which occlude the lower portion of the face, influence gaze perception. Further, individual differences in the impact of face masks on gaze perception is unclear. Accordingly, this pre-registered study investigated whether, and how, a reduction in the reliability of lower face cues affects gaze perception. Participants viewed both masked and unmasked faces that were either facing directly toward them (i.e. direct head orientation) or averted away from them (i.e. averted head orientation). The orientation of the eyes of the faces were also manipulated such that they varied from looking 15° to the left of the observer to looking 15° to the right of the observer, generating 13 unique eye orientations (i.e. − 15°, − 12°, − 9°, − 6°, − 3°, − 1°, 0°, 1°, 3°, 6°, 9°, 12°, 15°). Participants were asked to judge whether or not faces were looking at them in a two-alternative forced choice (2AFC) task. We measured the width of the CoDG for each participant, while also examining whether participant-reported autistic traits modulate the relationship between face masks and gaze perception.
Results
Figure 1 shows the group-averaged responses to the 2AFC task. The peaks of the curves represent the eye orientation, in degrees, at which participants mostly perceive direct gaze across Mask Conditions and Head Orientations. The results of the linear mixed-effects model (Table 1, Fig. 2) revealed that the CoDG was 0.3° wider in the masked condition (estimated marginal mean (EMM) = 11°; SE = 0.23; CI [10.6, 11.5]) compared to the unmasked condition (EMM = 10.7°; SE = 0.23; CI [10.3, 11.2]) (β = − 0.16; SE = 0.06, t (416.92) = − 2.52; p = 0.012; CI [− 0.29, − 0.04]). The CoDG was 0.7° wider for averted heads (EMM = 11.2°; SE = 0.23; CI [10.8, 11.7]) compared to direct-facing heads (EMM = 10.5°; SE = 0.23; CI [10.1, 11.0]) (β = − 0.34; SE = 0.06, t (416.94) = − 5.32; p < 0.001; CI [− 0.46, − 0.22]). No significant interaction between Mask Condition and Head Orientation was observed (Fig. 2a). We found a significant effect of Sex (β = − 0.56; SE = 0.23, t (148.76) = − 2.49; p = 0.013; CI [− 1.01, − 0.12]), where the CoDG for males was 1.1° wider (EMM = 11.4°; SE = 0.36; CI [10.73, 12.2]) than for females (EMM = 10.3°; SE = 0.26; CI [9.81, 10.80]). Autistic traits did not significantly predict the width of the CoDG, nor did they interact with Head Orientation or Mask Condition (Fig. 2b).

Responses to the 2AFC task. The filled points show the actual proportion of responses, while the solid lines represent the fitted data. The horizontal dashed line represents the point of subjective equality (PSE). Data are averaged over all participants for illustration purposes.

(a) Individual CoDG widths plotted as a function of Mask Condition and Head Orientation, jittered proportionally to the density. Boxplots represent 25th and 75th percentiles, while whiskers represent upper and lower values within 1.5*interquartile range. (b) Each participant’s CoDG width is plotted as a function of the Mask Condition, Head Orientation, and the participant’s self-reported autistic traits measured by the Comprehensive Autistic Trait Inventory (CATI50).
Exploratory analysis
Contrary to expectations, we found no evidence to suggest that autistic traits influence the width of the CoDG or that they interact with Mask Condition. As noted in the Introduction, it is possible that some autistic individuals who exhibit gaze aversion34,35,36,37 place greater reliance on non-eye-region cues during gaze perception and, therefore, when these cues are occluded, may experience an increase in gaze ambiguity (i.e. widening of CoDG). However, other autistic individuals who exhibit gaze indifference38,39,40, may shift their attention to attend to the eye-region when other cues are unreliable, which may lead to more sensitive perception of gaze (i.e. narrowing of CoDG). If these contrasting effects were both present within our data, it might preclude the ability to detect an effect of autistic traits in our model.
To investigate this possibility, we conducted an exploratory analysis wherein we computed a composite ‘Mask Effect’ score for each participant, for both direct and averted heads (n.b. this was not pre-registered). This Mask Effect was calculated by subtracting the width of the CoDG in the unmasked condition from the masked condition. As we hypothesised that participants reporting more autistic traits may show either a greater widening or a greater narrowing of the CoDG, we converted Mask Effect scores into absolute values in order to characterise the overall effect of face masks on gaze perception, regardless of the direction of this effect.
We fit linear mixed-effects models using restricted maximum-likelihood to investigate whether Mask Effect is predicted by autistic traits, Head Orientation, and their interaction. Participants were entered as random effects and sex and age were entered as fixed-effect covariates (formula: Mask Effect ~ Autistic Traits * Head Orientation + Age + Sex + (1 | Participant)). Twelve influential observations (3.9%) were excluded based on the criterion Cook’s D greater than 4 times the group average Cook’s D (> 0.10).
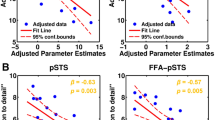
The results (Table 2, Fig. 3) revealed that Mask Effect was significantly predicted by autistic traits (β = 0.14; SE = 0.05, t (141.87) = 2.87; p = 0.005; CI [0.05, 0.24]) such that individuals reporting more autistic traits were more affected by the presence of a face mask (i.e. the magnitude of the Mask Effect was greater for those reporting more compared to fewer autistic traits). Additionally, a significant interaction was observed between autistic traits and Head Orientation (β = 0.12; SE = 0.05, t (142.81) = 2.75; p = 0.007; CI [0.04, 0.21]). We conducted a simple slopes analysis to investigate this two-way interaction; this revealed that the slope of autistic traits was significantly different from zero in the direct head condition (β = 0.27, SE = 0.07, t = 3.99, p < 0.001) but not in the averted head condition (β = 0.02, SE = 0.07, t = 0.25, p = 0.80).

Each participant’s absolute Mask Effect score, representing the overall effect of face masks, is plotted as a function of Head Orientation and the participant’s self-reported autistic traits as measured by the CATI. The shaded grey areas represent the standard error of the estimates.
Discussion
This study examined how wearing a face mask impacts upon judgments of direct gaze in the observer. We found that the CoDG was wider for masked faces compared to unmasked faces, and that masks influenced direct gaze judgment to a greater extent in individuals with high autistic traits.
Although recent studies have investigated how face masks affect emotion perception43,44, person perception41,42, and speech intelligibility46, little is known about whether, and how, they affect gaze perception. Our results suggest that much like when eye-region cues are less reliable, a reduction in the reliability of lower face cues increases gaze direction uncertainty, thereby increasing the range of angles at which gaze is perceived as self-directed10,11,12. Two recent studies, published subsequent to completion of data collection for the present study, also reported an increase in the width of the CoDG when perceiving gaze in masked compared to unmasked faces48,49. While the width of the CoDG increased only slightly for masked faces in our study (0.3°), this is closely aligned with an increase of 0.28° reported by48. It is important to note that this pattern of increased CoDG was not observed uniformly across all participants. In the present study, 59% of participants exhibited a wider CoDG for masked faces compared to unmasked faces, while 41% of participants showed the opposite effect. This corresponds to the findings of48 who found that 61% of participants exhibited a wider CoDG for masked faces in comparison to unmasked faces. While the data from the present study do not enable an unequivocal explanation for this finding, as we go on to discuss, one possible explanation relates to individual differences between participants.
The CoDG was 0.7° wider when observers perceived gaze in averted heads compared to direct-facing heads. It is likely that misalignment between head and eye cues increases observer uncertainty when perceiving gaze, which could lead to a more liberal threshold for assuming that gaze is self-directed10,11. We did not find a significant interaction between Mask Condition and Head Orientation. This suggests that the presence of face masks does not lead to a greater increase in observer uncertainty in averted compared to direct-facing heads, nor does it improve observer accuracy in averted heads by redirecting attention to the eye-region of masked faces, thereby reducing any bias caused by a misaligned head orientation.
Interestingly, we found that sex significantly predicted the width of the CoDG in our sample, such that males had a wider CoDG than females. A number of other studies have also shown that males are more likely to overestimate direct gaze than females (e.g.51,52). Studies suggest that females are more accurate at perceiving gaze than males (e.g.53,54), which may be explained by their increased fixations towards the eyes of others55. Accordingly, it is possible that females are more sensitive to discriminating between averted and direct gaze, hence their narrower CoDG.
A further aim of this study was to examine whether autistic traits modulate the effect of face masks on the CoDG. Our primary analysis found no evidence to suggest that autistic traits predict the width of the CoDG, nor that they interact with Mask Condition or Head Orientation. However, as noted in the Introduction, some autistic individuals may rely more heavily on non-eye-region directional cues during gaze perception29,30. In the absence of these cues, participants who exhibit gaze aversion34,35,36,37,56 might be less likely to redirect their attention to the eye-region, which could result in increased gaze uncertainty and a wider CoDG. In contrast, autistic observers who typically attend less to the eye region because they do not find the eyes engaging or informative because of a gaze indifference38,39,40, rather than because they find them aversive, may redirect their attention to the eye-region, resulting in more precise gaze judgments and a narrower CoDG. The presence of both of these effects within our data would mean that under masked conditions, some participants with more autistic traits would show a narrowing of the CoDG, while others would show a widening of the CoDG. These opposing effects would thus cancel out the other and preclude the ability of our main analysis to detect any effect related to autistic traits.
To test this hypothesis, we conducted an exploratory analysis which examined the relationship between autistic traits and the overall impact of face masks on gaze perception (i.e. the magnitude of the difference between masked and unmasked conditions, independent of the direction of this difference). We found that participants who reported more autistic traits exhibited a larger mask effect compared to participants who reported fewer autistic traits (i.e. they showed a greater magnitude of widening or narrowing of the CoDG in the masked relative to the unmasked condition). This supports the suggestion that occluding the lower part of the face results in a widening of the CoDG for some autistic individuals and a narrowing of the CoDG for others. As noted above, one possible factor that could explain this difference is the extent to which an individual exhibits gaze aversion, which could relate to underlying social anxiety. While we captured a measure of social anxiety in this study, this was too highly correlated with our measure of autistic traits to enable an examination of the effect of social anxiety in those with high autistic traits. Future research should seek to recruit autistic individuals with and without comorbid social anxiety disorders, as well as identify other characteristics that could explain the differential effects of face masks on CoDG. In view of the extensive literature examining social anxiety, social reward processing, and gaze aversion/indifference in autistic populations, we would recommend these constructs as preliminary targets for future research.
Our exploratory analysis also demonstrated an interaction between autistic traits and head orientation, whereby the heightened mask effect in participants with more autistic traits was observed only for direct-facing heads. One possible explanation for the observed difference in this effect between direct-facing and averted heads relates to the gaze aversion and gaze indifference hypotheses. The effect of face masks may be magnified in individuals exhibiting gaze aversion or gaze indifference. Direct-facing heads may be perceived as more aversive than averted heads by individuals who exhibit gaze aversion; this may result in greater gaze uncertainty in the masked condition due to avoidance of the eye-region. Conversely, observers who exhibit gaze indifference may greatly benefit from an occlusion of lower-face cues in the masked condition. When lower-face cues are unreliable they may shift their attention to the eye-region and perceive gaze with greater sensitivity; this effect may be magnified in direct-facing heads as the bias from an averted head is reduced.
It is important to highlight certain limitations of the present study. Firstly, this study was conducted entirely online. While online research has seen a recent surge in popularity, it is not without its inherent limitations, such as reduced control over participants and the conditions in which studies are completed. That said, previous studies have successfully conducted similar experiments online (e.g.57) and recent work has demonstrated reasonable concordance between measures collected online and in a lab setting (e.g.58,59). Nonetheless, it would be beneficial for future work to replicate this study in a lab setting. Additionally, data were collected in the UK and USA between May and December 2022. COVID-19 restrictions, such as mandatory face masks in public spaces, had only recently been lifted in the UK at this time, while face masks were still mandatory in many US states. Country-specific mask requirements, and subsequent experience with masks, may have an effect on how participants from different countries perceive gaze in masked vs unmasked faces; examination of such effects was beyond the scope of the present study.
Secondly, in prioritising experimental control over ecological validity, only a static, computer-generated, white male face was presented to participants. While this enabled greater systematic control in generating various combinations of eye and head angles, we acknowledge that gaze perception in dynamic, real-life social interactions is far less predictable, and that it may differ depending on the sex of the face presented to participants (e.g.52,60).
Finally, although we enriched our sample by recruiting an additional group of participants with confirmed autism spectrum diagnoses, we did not set out to compare gaze perception between autistic and non-autistic individuals. Future work should seek to build on the present findings by examining the effect of masks on CoDG in autistic and non-autistic groups matched in terms of IQ, age, and sex. Additionally, it would be interesting for future work to include eye-tracking to examine differences in visual gaze patterns to masked and unmasked faces, both between and within these groups.
The results of this study indicate that, overall, the occlusion of lower face cues increases gaze uncertainty, which results in an overestimation of direct-gaze, similar to when eye-region cues are unreliable8,10,11. However, our findings suggest that individuals with more autistic traits are disproportionately affected by the presence of face masks, which manifests as a widening of the CoDG (i.e. more uncertainty) in some observers, and a narrowing of the CoDG (i.e. higher precision) in others. Understanding the factors that might explain why an autistic individual experiences a widening or a narrowing of the CoDG under these conditions is a key question to be addressed by future work in this area. As the use of face masks is expected to remain higher than pre-pandemic levels61, it is imperative that research examines the impact of such interventions on social interactions. This study provides crucial insights into how the impact of face masks on gaze perception may affect autistic individuals to a greater extent.
Methods
Participants
Participants were recruited online either via Amazon’s Mechanical Turk (MTurk) or the University of Reading SONA systems. In order to ensure an adequate spread of autistic traits, we enriched our sample by recruiting additional autistic participants from the University of Reading Centre for Autism adult participant database (n.b. this aspect of the study was not pre-registered. The results of an analysis excluding autistic participants are presented in Supplementary Materials 1). Participants who are registered on this database have a confirmed clinical autism spectrum diagnosis from a registered health professional. Participants were reimbursed for approximately 40 min of their time.
Studies investigating individual differences are more likely to find small effect sizes62. We conducted an a-priori power analysis for correlations in G*Power63 which showed that a sample of N = 120 participants can detect small-medium (0.25) correlations with 80% power (n.b. we pre-registered a sample of N = 120). Due to over-recruiting to account for data loss, and the additional recruitment of participants with ASC diagnoses, a total of N = 163 participants was tested in this study. This sample comprised n = 99 recruited from MTurk, n = 29 recruited from SONA, and n = 35 recruited through our autism database. Participants were only included for analysis if they obtained a total attention score of 75% or more (see details of attention checks in the “Procedure” section); n = 161 were included for analysis following this criterion. After applying the exclusion criteria detailed in the “Data analysis” section, n = 157 participants were retained for analysis (Mage = 37.59, SD = 13.39, 103 females).
All participants provided written informed consent, and ethical approval was granted by the University of Reading, School of Psychology and Clinical Language Sciences Ethics Committee (ethical approval number: 2022-061-BC), which adheres to the ethical guidelines presented in the 6th (2008) Declaration of Helsinki.
Stimuli
One male face stimulus was generated using Daz software (http://www.daz3d.com/). The orientation of the eyes of this stimulus were manipulated such that they varied from looking 15° degrees to the left of an observer to 15° to the right of an observer, generating 13 unique eye orientations (i.e. − 15°, − 12°, − 9°, − 6°, − 3°, − 1°, 0°, 1°, 3°, 6°, 9°, 12°, 15°). Additionally, the head orientation of the stimulus was manipulated to either directly face the observer (0°), or be turned to their left (− 15°) or right (15°) (Fig. 4). For the purpose of reducing the effect of stimulus asymmetry on gaze perception, the face was flipped along the vertical axis for half of the trials. A second set of stimuli was generated using Daz software by adding a surgical-type face mask to the first set.

Example masked and unmasked faces with eyes oriented 0° and with heads (a) oriented − 15° to the left of an observer, (b) directly facing the observer (0°), or (c) oriented 15° to the right of an observer.
Procedure
The experimental task (Fig. 5) was hosted on Gorilla Experiment Builder64, and participants were only able to complete the task from a laptop or desktop computer. Each trial began with a central fixation cross presented for 500 milliseconds (ms). A blank screen then appeared for 100 ms, before the stimulus was displayed (image size: 425 × 543 pixels) at full resolution for 750 ms. After the presentation of the stimulus, participants were asked to respond as to whether or not the face was looking at them. In a 2AFC task, participants used the ‘Y’ and ‘N’ letters on their keyboard to record ‘Yes’ and ‘No’ responses respectively (n.b. no explicit instructions were given regarding which fingers participants should use to respond). The next trial started after participants made a response.

Example trial sequence. Each trial began with a central fixation cross presented for 500 ms. A blank screen then appeared for 100 ms, before the stimulus was displayed for 750 ms.
With 8 repetitions of each combination of eye orientation (13 levels), head orientation (3 levels), and mask condition (2 levels), each participant completed 624 trials in total across 8 blocks. Masked and unmasked conditions were presented across separate blocks. Breaks could be taken in between blocks of trials. Participants firstly completed 6 practice trials to familiarise themselves with the task. The practice task displayed only trials for which the answer to the question ‘Was the person looking at you?’ was relatively clear (e.g. a head oriented 0° with eyes also oriented 0° should be a simple ‘Yes’ response, while a head turned − 15° with eyes also oriented − 15° should be a simple ‘No’ response).
As the task was completed online, attention checks were presented randomly throughout to ensure participants were adequately engaged. To reduce the likelihood of submission from bots or random responses from participants, we included free-text responses to simple questions (e.g. ‘Was the face wearing a face mask?’, ‘What is your age?’).
Participants completed the CATI as a measure of self-reported autistic traits. The mean of our full sample of participants (M = 119.53, SD = 34.65) is reflective of the mean typically found in a non-autistic sample50. English and colleagues50 suggested that a cut-off of 134 on the CATI best discriminates autistic from non-autistic participants. With the exception of two individuals, all participants recruited through our autism database scored above this threshold (M = 161.97, SD = 18.61). As an increased width of CoDG has been associated with social anxiety6,17,18, we also administered the Social Interaction Anxiety Scale (SIAS65). Peters66 defined the SIAS cut-off score for social anxiety as 36; our full sample of participants exhibited slightly elevated levels of social anxiety (M = 37.12, SD = 19.37). Both the CATI and SIAS questionnaires included two attention questions to reduce the likelihood of participants responding randomly to the questionnaire items.
Data analysis
Cone of direct gaze calculation
The CoDG was calculated by fitting curves to the values for eye orientation, similar to the methodologies presented in previous studies of this nature (e.g.14,24). Specifically, a pair of logistic curves were fitted to model the probability of a participant considering gaze as self-directed given the eye orientation. One curve was fitted to eye orientations to the right of, and including, 0 degrees. A second curve was fitted to the eye orientations to the left of, and including, 0 degrees. The logistic functions had unique locations, but shared a common slope parameter, to aid in making the fitting more robust. The curves were fitted by minimising the sum of squared residuals for both functions concurrently. We extracted the 50% probabilities (i.e. the PSE) of considering gaze as direct for both the left and right gaze directions [the code is publicly available on our project OSF page (https://osf.io/gtjc2/?view_only=945076407acb49f68ca4139c58fecad3)]. The width of the CoDG was calculated as the sum of the absolute left and right-side PSE.
Analysis
Using the lmerTest package67 in R (version 4.1.2) we fit linear mixed-effects models using restricted maximum-likelihood to investigate whether the width of the CoDG is predicted by the presence of a face mask, autistic traits, head orientation, and their interaction. Participants were entered as random effects (formula: CoDG ~ Mask Condition * Autistic Traits * Head Orientation + Age + Sex + (1 | Participant)). Autistic traits and age were mean-centred and scaled. Data from the two averted head orientations (i.e. − 15° and 15°) were averaged in order to compare responses between averted and direct-facing heads. Due to high correlation between scores from the CATI and SIAS (r = 0.78, p < 0.001), SIAS could not be entered as a covariate in this model; results from a model including SIAS are presented in Supplementary Materials 2.
Thirty-eight influential observations (5.9%) were excluded from the model based on the criterion Cook’s D greater than 4 times the group average Cook’s D (> 0.12). Significance of fixed effects were determined using Satterthwaite approximations of degrees of freedom using the lmerTest package, limiting Type-1 errors but maintaining power68.
Data availability
The data and stimuli from this pre-registered (https://aspredicted.org/FMT_D8G) study are publicly available online (https://osf.io/gtjc2/?view_only=945076407acb49f68ca4139c58fecad3), and we report all data exclusions and measures obtained.
References
Gibson, J. J. & Pick, A. D. Perception of another person’s looking behavior. Am. J. Psychol. 76(3), 386–394. https://doi.org/10.2307/1419779 (1963).
Martin, W. W. & Rovira, M. L. An experimental analysis of discriminability and bias in eye-gaze judgment. J. Nonverbal Behav. 5, 155–163. https://doi.org/10.1007/BF00986132 (1981).
Farroni, T., Csibra, G., Simion, F. & Johnson, M. H. Eye contact detection in humans from birth. Proc. Natl. Acad. Sci. 99(14), 9602–9605. https://doi.org/10.1073/pnas.152159999 (2002).
Baron-Cohen, S. The eye direction detector (EDD) and the shared attention mechanism (SAM): Two cases for evolutionary psychology. In Joint Attention: Its Origins and Role in Development (eds Moore, C. & Dunham, P. J.) 41–59 (Lawrence Erlbaum Associates Inc, 1995).
Gamer, M. & Hecht, H. Are you looking at me? Measuring the cone of gaze. J. Exp. Psychol. Hum. Percept. Perform. https://doi.org/10.1037/0096-1523.33.3.705 (2007).
Gamer, M., Hecht, H., Seipp, N. & Hiller, W. Who is looking at me? The cone of gaze widens in social phobia. Cogn. Emot. 25(4), 756–764. https://doi.org/10.1080/02699931.2010.503117 (2011).
Langton, S. R., Honeyman, H. & Tessler, E. The influence of head contour and nose angle on the perception of eye-gaze direction. Percept. Psychophys. 66, 752–771. https://doi.org/10.3758/BF03194970 (2004).
Balsdon, T. & Clifford, C. W. How wide is the cone of direct gaze?. R. Soc. Open Sci. https://doi.org/10.1098/rsos.180249 (2018).
Zhuang, Z., Landsittel, D., Benson, S., Roberge, R. & Shaffer, R. Facial anthropometric differences among gender, ethnicity, and age groups. Ann. Occup. Hyg. 54, 391–402. https://doi.org/10.1093/annhyg/meq007 (2010).
Mareschal, I., Calder, A. J. & Clifford, C. W. Humans have an expectation that gaze is directed toward them. Curr. Biol. 23(8), 717–721. https://doi.org/10.1016/j.cub.2013.03.030 (2013).
Mareschal, I., Otsuka, Y. & Clifford, C. W. A generalized tendency toward direct gaze with uncertainty. J. Vis. 14(12), 27–27. https://doi.org/10.1167/14.12.27 (2014).
Martin, W. W. & Jones, R. F. The accuracy of eye-gaze judgement: A signal detection approach. Br. J. Soc. Psychol. 21(4), 293–299. https://doi.org/10.1111/j.2044-8309.1982.tb00551.x (1982).
Lobmaier, J. S., Savic, B., Baumgartner, T. & Knoch, D. The cone of direct gaze: A stable trait. Front. Psychol. https://doi.org/10.3389/fpsyg.2021.682395 (2021).
Ewbank, M. P., Jennings, C. & Calder, A. J. Why are you angry with me? Facial expressions of threat influence perception of gaze direction. J. Vis. 9(12), 16–16. https://doi.org/10.1167/9.12.16 (2009).
Harbort, J., Spiegel, J., Witthöft, M. & Hecht, H. The effects of social pressure and emotional expression on the cone of gaze in patients with social anxiety disorder. J. Behav. Ther. Exp. Psychiatry 55, 16–24. https://doi.org/10.1016/j.jbtep.2016.11.004 (2017).
Gianotti, L. R., Lobmaier, J. S., Calluso, C., Dahinden, F. M. & Knoch, D. Theta resting EEG in TPJ/pSTS is associated with individual differences in the feeling of being looked at. Soc. Cognit. Affect. Neurosci. 13(2), 216–223. https://doi.org/10.1093/scan/nsx143 (2018).
Schulze, L., Renneberg, B. & Lobmaier, J. S. Gaze perception in social anxiety and social anxiety disorder. Front. Hum. Neurosci. 7, 872. https://doi.org/10.3389/fnhum.2013.00872 (2013).
Jun, Y. Y., Mareschal, I., Clifford, C. W. & Dadds, M. R. Cone of direct gaze as a marker of social anxiety in males. Psychiatry Res. 210(1), 193–198. https://doi.org/10.1016/j.psychres.2013.05.020 (2013).
Matsuyoshi, D. et al. Individual differences in autistic traits predict the perception of direct gaze for males, but not for females. Mol. Autism 5(1), 1–4. https://doi.org/10.1186/2040-2392-5-12 (2014).
Pell, P. J. et al. Intact priors for gaze direction in adults with high-functioning autism spectrum conditions. Mol. Autism 7, 1–10. https://doi.org/10.1186/s13229-016-0085-9 (2016).
Ricciardelli, P. & Driver, J. Effects of head orientation on gaze perception: How positive congruency effects can be reversed. Q. J. Exp. Psychol. 61(3), 491–504. https://doi.org/10.1080/1747021070125545 (2008).
Wollaston, W. H. On the apparent direction of eyes in a portrait. Philos. Trans. R. Soc. Lond. 114, 247–256. https://doi.org/10.1098/rstl.1824.0016 (1824).
Anstis, S. M., Mayhew, J. W. & Morley, T. The perception of where a face or television portrait is looking. Am. J. Psychol. 82(4), 474–489 (1969).
Balsdon, T. & Clifford, C. W. A bias-minimising measure of the influence of head orientation on perceived gaze direction. Sci. Rep. https://doi.org/10.1038/srep41685 (2017).
Otsuka, Y., Mareschal, I., Calder, A. J. & Clifford, C. W. Dual-route model of the effect of head orientation on perceived gaze direction. J. Exp. Psychol. Hum. Percept. Perform. https://doi.org/10.1037/a0036151 (2014).
Moors, P., Germeys, F., Pomianowska, I. & Verfaillie, K. Perceiving where another person is looking: The integration of head and body information in estimating another person’s gaze. Front. Psychol. https://doi.org/10.3389/fpsyg.2015.00909 (2015).
Williams, E. H. & Chakrabarti, B. The integration of head and body cues during the perception of social interactions. Q. J. Exp. Psychol. https://doi.org/10.1177/17470218231181001 (2023).
Perrett, D. I., Hietanen, J. K., Oram, M. W. & Benson, P. J. Organization and functions of cells responsive to faces in the temporal cortex. Philos. Trans. R. Soc. Lond. Ser. B Biol. Sci. 335(1273), 23–30. https://doi.org/10.1098/rstb.1992.0003 (1992).
Ashwin, C., Hietanen, J. K. & Baron-Cohen, S. Atypical integration of social cues for orienting to gaze direction in adults with autism. Mol. Autism 6(1), 1–10. https://doi.org/10.1186/2040-2392-6-5 (2015).
Mihalache, D. et al. Perceiving gaze from head and eye rotations: An integrative challenge for children and adults. Dev. Sci. https://doi.org/10.1111/desc.12886 (2020).
Dalton, K. M. et al. Gaze fixation and the neural circuitry of face processing in autism. Nat. Neurosci. 8(4), 519–526. https://doi.org/10.1038/nn1421 (2005).
Jones, W., Carr, K. & Klin, A. Absence of preferential looking to the eyes of approaching adults predicts level of social disability in 2-year-old toddlers with autism spectrum disorder. Arch. Gen. Psychiatry 65(8), 946–954. https://doi.org/10.1001/archpsyc.65.8.946 (2008).
Spezio, M. L., Adolphs, R., Hurley, R. S. & Piven, J. Analysis of face gaze in autism using “Bubbles”. Neuropsychologia 45(1), 144–151. https://doi.org/10.1016/j.neuropsychologia.2006.04.027 (2007).
Kylliäinen, A. & Hietanen, J. K. Skin conductance responses to another person’s gaze in children with autism. J. Autism Dev. Disord. 36, 517–525. https://doi.org/10.1007/s10803-006-0091-4 (2006).
Joseph, R. M., Ehrman, K., McNally, R. & Keehn, B. Affective response to eye contact and face recognition ability in children with ASD. J. Int. Neuropsychol. Soc. 14(6), 947–955. https://doi.org/10.1017/S1355617708081344 (2008).
Hutt, C. & Ounsted, C. The biological significance of gaze aversion with particular reference to the syndrome of infantile autism. Behav. Sci. 11(5), 346–356. https://doi.org/10.1002/bs.3830110504 (1966).
Kliemann, D., Dziobek, I., Hatri, A., Steimke, R. & Heekeren, H. R. Atypical reflexive gaze patterns on emotional faces in autism spectrum disorders. J. Neurosci. 30(37), 12281–12287. https://doi.org/10.1523/JNEUROSCI.0688-10.2010 (2010).
Moriuchi, J. M., Klin, A. & Jones, W. Mechanisms of diminished attention to eyes in autism. Am. J. Psychiatry 174(1), 26–35. https://doi.org/10.1176/appi.ajp.2016.15091222 (2017).
Senju, A. & Johnson, M. H. The eye contact effect: Mechanisms and development. Trends Cognit. Sci. 13(3), 127–134. https://doi.org/10.1016/j.tics.2008.11.009 (2009).
Cohen, I. L., Vietze, P. M., Sudhalter, V., Jenkins, E. C. & Brown, W. T. Parent-child dyadic gaze patterns in fragile X males and in non-fragile X males with autistic disorder. J. Child Psychol. Psychiatry 30(6), 845–856. https://doi.org/10.1111/j.1469-7610.1989.tb00286.x (1989).
Freud, E., Stajduhar, A., Rosenbaum, R. S., Avidan, G. & Ganel, T. The COVID-19 pandemic masks the way people perceive faces. Sci. Rep. 10(1), 22344. https://doi.org/10.1038/s41598-020-78986-9 (2020).
Carragher, D. J. & Hancock, P. J. Surgical face masks impair human face matching performance for familiar and unfamiliar faces. Cognit. Res. Princ. Implic. 5(1), 1–15. https://doi.org/10.1186/s41235-020-00258-x (2020).
Carbon, C. C. Wearing face masks strongly confuses counterparts in reading emotions. Front. Psychol. https://doi.org/10.3389/fpsyg.2020.566886 (2020).
Gori, M., Schiatti, L. & Amadeo, M. B. Masking emotions: Face masks impair how we read emotions. Front. Psychol. https://doi.org/10.3389/fpsyg.2021.669432 (2021).
Ruba, A. L. & Pollak, S. D. Children’s emotion inferences from masked faces: Implications for social interactions during COVID-19. PLoS ONE https://doi.org/10.1371/journal.pone.0243708 (2020).
Truong, T. L. & Weber, A. Intelligibility and recall of sentences spoken by adult and child talkers wearing face masks. J. Acoust. Soc. Am. 150(3), 1674–1681. https://doi.org/10.1121/10.0006098 (2021).
Dalmaso, M., Zhang, X., Galfano, G. & Castelli, L. Face masks do not alter gaze cueing of attention: Evidence from the COVID-19 pandemic. i-Perception https://doi.org/10.1177/2041669521105848 (2021).
Lobmaier, J. S. & Knoch, D. Face masks have a limited effect on the feeling of being looked at. Front. Neurosci. https://doi.org/10.3389/fnins.2022.1028915 (2022).
Liu, J. et al. Masked face is looking at me: Face mask increases the feeling of being looked at during the COVID-19 pandemic. Front. Neurosci. https://doi.org/10.3389/fnins.2022.1056793 (2022).
English, M. C. et al. The Comprehensive Autistic Trait Inventory (CATI): Development and validation of a new measure of autistic traits in the general population. Mol. Autism 12(1), 1–23. https://doi.org/10.1186/s13229-021-00445-7 (2021).
Lobmaier, J. S., Tiddeman, B. P. & Perrett, D. I. Emotional expression modulates perceived gaze direction. Emotion 8(4), 573. https://doi.org/10.1037/1528-3542.8.4.573 (2008).
Slepian, M. L., Weisbuch, M., Adams, R. B. Jr. & Ambady, N. Gender moderates the relationship between emotion and perceived gaze. Emotion 11(6), 1439. https://doi.org/10.1037/a0026163 (2011).
Guéguen, N. & Jacob, C. Direct look versus evasive glance and compliance with a request. J. Soc. Psychol. 142(3), 393–396. https://doi.org/10.1080/00224540209603907 (2002).
Bayliss, A. P., Pellegrino, G. D. & Tipper, S. P. Sex differences in eye gaze and symbolic cueing of attention. Q. J. Exp. Psychol. 58(4), 631–650. https://doi.org/10.1080/02724980443000124 (2005).
Hall, J. K., Hutton, S. B. & Morgan, M. J. Sex differences in scanning faces: Does attention to the eyes explain female superiority in facial expression recognition?. Cogn. Emot. 24(4), 629–637. https://doi.org/10.1080/02699930902906882 (2010).
Tottenham, N. et al. Elevated amygdala response to faces and gaze aversion in autism spectrum disorder. Soc. Cognit. Affect. Neurosci. 9(1), 106–117. https://doi.org/10.1093/scan/nst050 (2014).
Lavan, N., Chan, W. Y., Zhuang, Y., Mareschal, I. & Shergill, S. S. Direct eye gaze enhances the ventriloquism effect. Atten. Percept. Psychophys. 84(7), 2293–2302. https://doi.org/10.3758/s13414-022-02468-5 (2022).
Backx, R., Skirrow, C., Dente, P., Barnett, J. H. & Cormack, F. K. Comparing web-based and lab-based cognitive assessment using the Cambridge Neuropsychological Test Automated Battery: A within-subjects counterbalanced study. J. Med. Internet Res. https://doi.org/10.2196/16792 (2020).
Hilbig, B. E. Reaction time effects in lab-versus Web-based research: Experimental evidence. Behav. Res. Methods 48, 1718–1724. https://doi.org/10.3758/s13428-015-0678-9 (2016).
Vuilleumier, P., George, N., Lister, V., Armony, J. & Driver, J. Effects of perceived mutual gaze and gender on face processing and recognition memory. Vis. Cogn. 12(1), 85–101. https://doi.org/10.1080/13506280444000120 (2005).
Rab, S., Javaid, M., Haleem, A. & Vaishya, R. Face masks are new normal after COVID-19 pandemic. Diabetes Metab. Syndr. 14(6), 1617–1619. https://doi.org/10.1016/j.dsx.2020.08.021 (2020).
Schäfer, T. & Schwarz, M. A. The meaningfulness of effect sizes in psychological research: Differences between sub-disciplines and the impact of potential biases. Front. Psychol. https://doi.org/10.3389/fpsyg.2019.00813 (2019).
Faul, F., Erdfelder, E., Lang, A. G. & Buchner, A. G* Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 39(2), 175–191. https://doi.org/10.3758/BF03193146 (2007).
Anwyl-Irvine, A. L., Massonnié, J., Flitton, A., Kirkham, N. & Evershed, J. K. Gorilla in our midst: An online behavioral experiment builder. Behav. Res. Methods 52, 388–407. https://doi.org/10.3758/s13428-019-01237-x (2020).
Mattick, R. P. & Clarke, J. C. Development and validation of measures of social phobia scrutiny fear and social interaction anxiety. Behav. Res. Ther. 36(4), 455–470. https://doi.org/10.1016/S0005-7967(97)10031-6 (1998).
Peters, L. Discriminant validity of the social phobia and anxiety inventory (SPAI), the social phobia scale (SPS) and the social interaction anxiety scale (SIAS). Behav. Res. Ther. 38(9), 943–950. https://doi.org/10.1016/S0005-7967(99)00131-X (2000).
Kuznetsova, A., Brockhoff, P. B. & Christensen, R. H. lmerTest package: Tests in linear mixed effects models. J. Stat. Softw. 82, 1–26. https://doi.org/10.18637/jss.v082.i13 (2017).
Luke, S. G. Evaluating significance in linear mixed-effects models in R. Behav. Res. Methods 49, 1494–1502. https://doi.org/10.3758/s13428-016-0809-y (2017).
Acknowledgements
EHW, NT and BC were supported by the Medical Research Council (Grant Reference: MR/S036423/1) and the University of Reading during this work. We thank Siobhan MacDonald for assistance with data collection for this study.
Author information
Authors and Affiliations
Contributions
The study was conceptualised by E.H.W. and B.C., and designed by E.H.W. and N.T. Preparation of materials for data collection was performed by E.H.W. E.H.W. and G.M. performed data analysis. All authors contributed to the writing of the manuscript, and read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
This paper was posted as a preprint at Psyarxiv (https://psyarxiv.com/xgvbu). The authors declare no competing interests. For the purpose of open access, the authors have applied a Creative Commons attributing (CCBy) licence to any Author Accepted Manuscript arising.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Williams, E.H., Thompson, N.M., McCray, G. et al. Autistic traits modulate the influence of face masks on gaze perception. Sci Rep 13, 14921 (2023). https://doi.org/10.1038/s41598-023-41900-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-41900-0
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
