
Abstract
This network meta-analysis was done to thoroughly evaluate the available literature on the use of different hemostatic agents for dental extraction in patients under oral antithrombotic therapy, aiming to identify the agent with the best/worst performance in bleeding control. Considering that such patients have a higher risk of bleeding, choosing the right hemostatic is essential. Twenty-three randomized clinical trials articles were included after completing the literature search. Cyanoacrylate tissue adhesive showed a reduction in the odds of postoperative bleeding events compared with conventional methods (i.e., gauze/cotton pressure, sutures), with a tendency toward a statistical significance (OR 0.03, P = 0.051). Tranexamic acid was the only agent that demonstrated a significantly lower risk of developing postoperative bleeding events (OR 0.27, P = 0.007). Interestingly, chitosan dental dressing and collagen plug had the shortest time to reach hemostasis. However, they ranked last among all hemostatic agents, regarding bleeding events, revealing higher odds than conventional measures. Therefore, it is concluded that the use of cyanoacrylate tissue adhesive and tranexamic acid gives favorable results in reducing postoperative bleeding events following dental extractions. Although chitosan dental dressing and collagen exhibited a faster time to reach hemostasis, they led to a higher occurrence of bleeding events.
Similar content being viewed by others


Introduction
Dental extraction is a common procedure performed in oral and maxillofacial surgery clinics1. Numerous potential complications may accompany this procedure, manifesting during the peri- and/or postoperative phase2,3. Bleeding is among the most encountered and important complications to consider. Post-extraction bleeding is normally managed with conventional methods (i.e., gauze/cotton pressure, sutures). However, these measures may not be sufficient in situations where a higher degree of bleeding is anticipated, as in patients under oral antithrombotic therapy (OAT). These patients have an increased postoperative risk of hemorrhage, in addition to the possibility for a prolonged bleeding time once this event occurs4,5.
To reduce the risk of hemorrhage with patients taking antithrombotic medications, it was suggested earlier to stop or modify their drug regimen for a certain period before undergoing dental extractions. Nevertheless, the elevated possibility of developing thromboembolism events5, along with other reports demonstrating the ability to properly control postoperative bleeding with these individuals utilizing hemostatic measures6,7, led this protocol to become suboptimal. Several studies have investigated the outcome of dental extraction without stopping or modifying the antithrombotic treatment. Their results revealed that, when obtaining sufficient hemostasis upon the completion of this procedure, tooth extraction could be done safely without any adjustment to the patients’ antithrombotic therapy8,9,10,11. Consequently, this step is not justified and has become less popular.
Although tooth extraction has been shown to be safe in patients with higher bleeding risk, postoperative bleeding events have still been reported12. Therefore, finding the best supplementary measures for achieving more effective hemostasis has become vital.
Hemostatic agents have been introduced as a method to secure better hemostasis. Several agents were presented and compared, whether with conventional measures or with other agents13. Yet, the best agent among all the available options is still undetermined. Previous systematic reviews have been presented on this topic. However, these studies either lacked quantitative synthesis14, or focused on the effect of hemostatic agents in general, compared with the conventional measures15. Thus, understanding which agent or agents provide better bleeding control, as well as the ones with less desirable outcomes, would be of a high value.
A recent method of conducting meta-analyses has been proposed, the network meta-analysis. This type of analysis allows for making indirect comparisons between different materials used for the same purpose (hemostatic agents in this case), based on the results of the available direct comparisons, i.e., documented clinical trials16. This offers more insight into the hemostatic agents currently used and enriches the available information on their potential. A previous network meta-analysis has been performed on this topic17. Nevertheless, the authors combined all types of oral surgical procedures and did not focus on dental extraction in particular. Furthermore, only the agents with the best potential in bleeding control were mentioned and discussed, without emphasis on the ones that may lead to a higher occurrence of postoperative bleeding events. Out of these points, the goal of this network meta-analysis was to thoroughly evaluate the literature on the use of different hemostatic agents for dental extraction, attempting to provide evidence on the agents with the best or worst performance in bleeding control in patients under OAT.
Results
Search outcomes
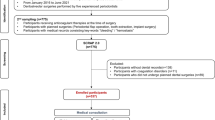
There were 1655 identified studies. After removing the duplicates, and screening the titles and abstracts, 82 articles were qualified for the full-text assessment stage. Of these, 59 studies were excluded (Supplementary Table 1). As a result, the search process ended with including 23 articles in this study, 22 of which were eligible for meta-analysis. Figure 1 is the PRIMSA flowchart of the search process and outcomes.

PRISMA flowchart of the search process and outcomes.
Study characteristics
Thirteen studies allocated different patients for each group7,18,19,20,21,22,23,24,25,26,27,28,29, while nine had a split-mouth design6,30,31,32,33,34,35,36,37. In addition, one investigation had some of the patients being allocated to more than one group (split-mouth for some cases)38. Three studies recruited patients on antithrombotic therapy in general without specifying25,30,33, while 14 publications stated that patients were on anticoagulants, and 6 investigations enrolled patients on antiplatelet drugs6,22,31,32,34,35.
The type of extraction was simple in 19 studies, surgical in one26, both simple and surgical two27,28, while this was not specified in one publication29.
The hemostatic agents used were Chitosan dental dressing19,30,31,33,34,35,36,37, Oxidized regenerated cellulose6,27,32, Tranexamic acid20,21,24,28,29,38, Fibrin sponge or adhesive18,27,38, Collagen plug18,34,37, Bismuth subgallate18, Gelatin sponge19,22,23,26, Feracrylum20, Epsilon aminocaproic acid7,29, Ankaferd blood stopper25, and Cyanoacrylate tissue adhesive26.
Sixteen studies had a group that received conventional measures, which were the application of gauze pressure20,24,25,31,36,38, cotton pressure30, or sutures6,7,21,22,23,28,32. Two studies applied gauze pressure, however, used sutures when the case necessitated33,35.
The time to reach hemostasis was reported in eleven studies. Eight of them compared a hemostatic agent with conventional measures21,24,25,30,31,33,35,36, while 3 compared different agents26,34,37. When the agents were compared with conventional measures, six studies stated that hemostatics led to significantly less time to reach hemostasis, whereas 2 studies did not report information about statistical significance25,31.
Sixteen studies reported information related to postoperative bleeding events. Among these, five compared different agents18,19,26,27,29, while the rest compared one or more hemostatic agents to conventional methods6,7,20,21,22,23,25,28,32,35,38. The postoperative period to record bleeding events lasted up to 10 days26. There was no significant difference between the hemostatic agents and the conventional methods in all studies. In contrast, when evaluating different agents, cyanoacrylate tissue adhesive resulted in significantly fewer bleeding events, as opposed to using a gelatin sponge26, while the latter demonstrated a statistical significance compared with chitosan19. Moreover, both fibrin and bismuth subgallate were significantly better than collagen18. Table 1 summarizes the characteristics of the included studies.
Risk of bias
Upon implementing the RoB2 tool, eight studies showed a low risk of bias7,18,21,28,31,32,34,37. These studies had a clear randomization process, well-described intervention with no potential deviation from it, and no/little loss to follow-up, in addition to an appropriate and clear measuring and reporting of the outcome. Moreover, fourteen studies had some concerns6,19,20,22,23,25,26,27,29,30,33,35,36,38, mostly due to an unclear randomization process, while one investigation was judged to be of a high risk of bias24. The main reason was the questionable method of measuring/reporting the outcome (Supplementary Fig. 1).
Data synthesis and network meta-analysis
Time to reach hemostasis
Nine studies were included in this network meta-analysis21,25,30,31,33,34,35,36,37, having 5 methods used to achieve hemostasis. The type of extraction was simple in all of these studies. Figure 2 illustrates the comparisons performed in the included investigations. Substantial heterogeneity and inconsistency between the studies were found (I2 = 98.3%, Q = 288.97, P < 0.0001). The results of this meta-analysis revealed that chitosan dental dressing, as well as collagen plug led to significantly faster hemostasis, compared with the conventional methods (SMD = − 9.78, 95% CI − 12.78 to − 6.78, and SMD = − 10.13, 95% CI − 15.53 to − 4.73, respectively) (Table 2, Supplementary Table 2). This was based on direct and indirect evidence, respectively. The league table also indicated that ankaferd blood stopper led to a significantly longer time to reach hemostasis, compared with chitosan (SMD = 7.39, 95% CI 0.33 to 14.45), based on indirect evidence (Table 2). Treatment ranking revealed that chitosan and collagen are likely to perform best in reducing the time to reach hemostasis (Fig. 3).

Network meta-analysis geometry of the comparisons available on the time to reach hemostasis. Each node represents an intervention. The line between 2 nodes represents a direct comparison that has been conducted in a clinical trial. The thicker the line, the more direct comparisons available. The color of the node is based on the number and risk of bias of the studies that included the relevant agent, where green and yellow represent “low risk” and “some concerns”, respectively. The color of the line is based on the risk of bias in the majority of the studies that included the relevant comparison. Ankaferd ankaferd blood stopper, col.plug collagen plug, conven conventional methods, TA tranexamic acid, chtio chitosan dental dressing.

Forest plot to show the ranking of the available interventions with regards to the time to reach hemostasis.
Bleeding events
Sixteen studies reported information related to this outcome6,7,18,19,20,21,22,23,25,26,27,28,29,32,35,38, based on 12 different methods used. Figure 4 demonstrates the comparisons performed among these investigations. Low heterogeneity (I2 = 12.5%) and inconsistency (Q = 3.10; P-value = 0.69) were noted. Tranexamic acid was the only agent that showed a significant difference compared with conventional methods (OR 0.27, 95% CI 0.10 to 0.69). In addition, cyanoacrylate tissue adhesive showed a tendency towards statistical significance (OR 0.03, 95% CI 0.0008 to 1.02, P = 0.051) (Table 3, Supplementary Table 3), based on indirect evidence. Comparing different agents, bismuth subgallate and fibrin showed significantly lower odds of postoperative bleeding events, as opposed to collagen plug. This was based on direct evidence. As for the indirect evidence, chitosan dental dressing demonstrated significantly higher odds, compared with cyanoacrylate and tranexamic acid. Collagen plug also showed significantly higher odds than cyanoacrylate and tranexamic acid (Table 3). Treatment ranking revealed that cyanoacrylate tissue adhesive is likely to show the best results. However, tranexamic acid had the narrowest confidence interval (with statistical significance). Chitosan dental dressing and collagen plug ranked last among all hemostatic agents (Fig. 5).

Network meta-analysis geometry of the comparisons available on bleeding events. Ankaferd ankaferd blood stopper, col.plug collagen plug, conven conventional methods, TA tranexamic acid, chtio chitosan dental dressing, EACA Epsilon aminocaproic acid, bis.sub Bismuth subgallate, fib fibrin gel.spo gelatin sponge, cyano cyanoacrylate tissue adhesive, cellulose Oxidized regenerated cellulose, fer Feracrylum.

Forest plot to show the ranking of the available interventions with regards to bleeding events.
Bleeding events in anticoagulated patients
Eleven investigations were analyzed, including 11 different treatments7,18,19,20,21,23,26,27,28,29,38. Figure 6 shows the methods compared in the analyzed studies. Moderate heterogeneity (I2 = 32.3%), with no significant inconsistency (Q = 1.33; P-value = 0.7217) was seen. Similarly, tranexamic acid only showed statistical significance, compared with conventional methods (OR 0.24, 95% CI 0.08 to 0.77) (Table 4, Supplementary Table 4). Concerning different agents, bismuth subgallate demonstrated significantly lower odds of postoperative hemorrhage events than collagen plug. Chitosan dental dressing indicated significantly higher odds, compared with cyanoacrylate and tranexamic acid. Collagen plug showed significantly higher odds than tranexamic acid. These comparisons were based on indirect evidence (Table 4). Treatment ranking revealed that cyanoacrylate tissue adhesive had the lowest odds of postoperative bleeding. However, tranexamic acid obtained the narrowest confidence interval. Chitosan dental dressing and collagen plug also ranked the worst among all hemostatic agents (Fig. 7).

Network meta-analysis geometry of the comparisons available on bleeding events in anticoagulated patients.

Forest plot to show the ranking of the available interventions with regards to bleeding events in anticoagulated patients.
Bleeding events after simple tooth extraction
As the majority of the studies recruited patients undergoing simple dental extractions, a subgroup analysis was performed, in order to further validate the evidence provided from the previous analyses, including more homogenous investigations. Twelve studies, with 11 treatments, were analyzed6,7,18,19,20,21,22,23,25,32,35,38. Figure 8 illustrates the comparisons performed among these clinical trials. The level of heterogeneity was moderate (I2 = 34.3%) and no significant inconsistency was identified (Q = 6.13, P-value = 0.11). Tranexamic acid also showed a significant effect in reducing bleeding events, compared with the conventional measures (OR 0.12, 95% CI 0.02 to 0.71) (Table 5, Supplementary Table 5). When comparing different hemostatic agents, bismuth subgallate and fibrin demonstrated significantly lower odds of postoperative hemorrhage than collagen plug based on direct evidence. The same was noted when comparing tranexamic acid and collagen plug, as indicated by the indirect evidence (Table 5). Treatment ranking revealed that tranexamic acid is likely to perform best among all hemostatic agents, while chitosan and collagen ranked last, as described in the previous analyses (Fig. 9). The meta-analysis done with 7 studies7,18,19,20,21,23,38 including anticoagulated patients who underwent simple tooth extraction also showed a similar trend (Supplementary Figs. 2, 3, Supplementary Tables 6 and 7).

Network meta-analysis geometry of the comparisons available on bleeding events after simple (i.e., non-surgical) tooth extraction.

Forest plot to show the ranking of the available interventions with regards to bleeding events after simple tooth extraction.
Confidence in the evidence of network meta-analysis outcomes
The certainty of evidence for all outcomes is presented in Supplementary Tables 8–12. Chitosan and collagen plug were the agents that demonstrated a significant difference compared with conventional measures, regarding the time to achieve hemostasis. However, the compared studies had potential bias, heterogeneity, and incoherence, leading to a low to very low level of evidence. The level of evidence for all other comparisons under this outcome was also concluded to be either low or very low.
As for bleeding events in antithrombotic patients in general or anticoagulated patients in particular, the evidence on the efficacy of tranexamic acid was downgraded by one level to become moderate. The reason was the possible heterogeneity between the studies.
With respect to the comparison between agents that demonstrated statistical significance, these were also at a moderate to low level of evidence.
The indirect evidence on the superiority of tranexamic acid compared with collagen plug was high when analyzing all studies, however, it was downgraded to moderate when the analysis was done on anticoagulated patients specifically, due to the imprecision of the result. In addition, the evidence was further downgraded to be low when including studies with simple extraction only, because of the potential bias in the analyzed investigations as well as the imprecision of the overall outcome.
Discussion
As presented in this study, numerous hemostatic agents have been used and compared with conventional methods for bleeding control after dental extractions. Choosing one agent over the other or concluding which method is more effective was not possible, especially since only some agents have been compared and the majority have been used in different studies. Consequently, this network meta-analysis was conducted, aiming to provide a comprehensive evaluation of the available hemostatic agents and give an idea on the agents that perform best in bleeding control, as well as the ones with unfavorable results.
Among all hemostatic agents compared in this network meta-analysis, cyanoacrylate tissue adhesive ranked as the one with the least odds of postoperative bleeding in patients on antithrombotic therapy. This agent resulted in a notable decrease in the risk of postoperative bleeding events (OR 0.03). Cyanoacrylate tissue adhesive has been presented as an alternative to the conventional methods of hemostasis, and applied in several surgical procedures26,39,40, including tooth extraction26. It has gained increased interest, due to its efficacy in bleeding control26, adherence to soft and hard tissues41,42, antimicrobial potential, as well as its relatively easy application, which aids in effective tissue handling and results in overall shorter operation time41,43. Cyanoacrylate tissue adhesive has also been compared with sutures for mandibular third molar surgery in several studies on healthy patients, and led to a lower occurrence of postoperative bleeding events43,44, as well as a reduction in the degree of pain44,45. It is worth mentioning that although no significant difference was noted in this study, the high end of the 95% CI was 1.02, which indicates a tendency towards statistical significance (P = 0.051). Therefore, all previous studies, accompanied by the evidence presented in this network meta-analysis, indicate the efficacy of this hemostatic agent in reducing the chance of postoperative bleeding when applied for closing the site after surgical extraction.
The only agent that showed statistical significance in reducing postoperative hemorrhage events was tranexamic acid. It demonstrated an approximate 70% decrease in the likelihood of developing postoperative bleeding events (OR 0.27), with a narrow confidence interval, revealing the high possibility of this outcome to be clinically meaningful, rather than just hypothetical. This hemostatic agent has been used for a long time in bleeding control in oral surgery, benefiting from its low systemic resorption when applied topically46,47. A previous meta-analysis concluded that tranexamic acid was effective in reducing postoperative bleeding events, compared with other agents or a placebo48. Another systematic review pointed out that this agent seems to provide better results in bleeding control, however, conclusive evidence is still unavailable14. The outcome of the present meta-analysis confirms what is stated in the literature, showing the superiority of tranexamic acid in reducing the occurrence of postoperative bleeding events. Therefore, it should be among the first options to consider when performing dental extractions in patients on OAT.
The efficacy of tranexamic acid and cyanoacrylate, concluded from this meta-analysis, is in line with an earlier report on different oral surgical procedures17. However, the most notable finding was probably the one regarding chitosan dental dressing and collagen plug. As shown in the analysis of time to reach hemostasis, these agents ranked the highest, revealing a high statistical significance (SMD = − 9.78, P < 0.0001 and SMD = − 10.13, P = 0.0002, respectively), i.e., a major reduction in the time to achieve hemostasis. Conversely, they ranked last in controlling post-extraction bleeding events, when the analysis was done on antithrombotic patients in general or anticoagulated patients only. Their efficacy was even worse than the conventional methods of hemostasis. This could also support the ‘low/very low’ level of evidence on their effectiveness in reducing the time to reach hemostasis. Chitosan in general promotes wound healing, enhances the production of platelet-derived growth factors49, and has been shown to possess antimicrobial characteristics50, which also play a role in the overall healing of extraction sites. In contrast, some chitosan dressings have poor mechanical properties51,52, which could lead to later dislodgement from the socket, and consequently, postoperative bleeding. Moreover, collagen has very good biocompatibility and cell adhesion. This porous or fibrous sponge is non-toxic and can be used in various clinical scenarios where hemostasis is needed53. Similar to chitosan, collagen possesses low mechanical strength and an unpredictable biodegradation rate53,54,55. Although prompt hemostasis is secured with the use of this agent, these disadvantages may contribute to the bleeding events present at a later stage. Therefore, considering all the previous points, and based on the results of this meta-analysis, choosing other hemostatic agents, such as tranexamic acid is preferable over the use of collagen or chitosan dressing. It is also noteworthy that when the analysis was done on patients taking anticoagulants, gelatin sponge performed worse than conventional measures. A possible cause is that sponges can expand multiple times in size compared with their baseline size, which might negatively affect blood clot formation in small sockets in certain cases15,56. This should also be considered when managing bleeding from extraction sockets, aiming to use the most suitable method of hemostasis.
Certain limitations in this study should be kept in mind. The low number of trials with patients on antiplatelet drugs did not allow for conducting meta-analysis including studies with only these patients. The overall small number of studies also resulted in performing only one analysis with patients on OAT in general, with regards to the time to reach hemostasis. The extracted teeth were not specified in the analyzed investigations (e.g., molar versus anterior teeth). This may have affected the occurrence of bleeding events, because more difficult cases might have a higher risk of postoperative bleeding events. Additionally, most of the included studies showed a potential risk of bias. Along with other factors, this led to having a lower level of evidence and less confidence in the outcome of this network meta-analysis. Therefore, future studies with more direct comparisons between the available agents would be of high importance, to further explore and validate the conclusions drawn in this meta-analysis, and to assess whether its outcome could be applied to patients under antiplatelet therapy as well.
Conclusions
Within the limitations of this study, it is concluded that the use of cyanoacrylate tissue adhesive and tranexamic acid gives favorable results in reducing postoperative bleeding events following dental extractions. Although chitosan dental dressing and collagen exhibited a faster time to reach hemostasis, they led to a higher occurrence of bleeding events and ranked last among all other hemostatic methods.
Methods
This study was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA), with the extension for network meta-analysis57, and was registered in the PROSPERO database (registration number CRD42023408207).
The PICOS protocol was implemented to develop a suitable focused question and include potential investigations:
-
Population (P): patients under OAT who are in need of dental extractions.
-
Intervention (I): the use of hemostatic agents following tooth extraction.
-
Comparator (C): the use of conventional methods of hemostasis (i.e., gauze/cotton pressure, sutures).
-
Outcomes (O): time to reach hemostasis, and peri-/postoperative bleeding events.
-
Study design (S): randomized clinical trials (RCTs).
As a result, the focused question of this study was: in antithrombotic patients receiving dental extractions (P), what is the efficacy of different hemostatic agents (I) in bleeding control (O), compared with the conventional measures of hemostasis (C), based on the results of randomized clinical trials (S)?
Search strategy
Database search was carried out in 3 search engines: PubMed/Medline, Cochrane Central Register of Controlled Trials (CENTRAL), and Scopus. In addition, an extensive search process was done in the grey literature, aiming to find more eligible studies, as well as unpublished investigations if available.
A combination of free keywords and Medical Subject Heading search terms (i.e., MeSH) was inserted in databases during the search process (Supplementary Table 13).
Study selection
Eligible investigations had to fulfill the PICOS criteria stated previously. Studies where hemostasis was achieved with the help of other methods (e.g., electrocautery), reports that do not address the focused question (e.g., different surgical procedures, irrelevant measurements), in addition to trials where the control group stopped or modified their drug regimen were excluded from this meta-analysis.
Screening of potential studies was performed independently by two reviewers (B.M and S.J). This process was done using the Rayyan website (Rayyan, Qatar Computing Research Institute, Qatar Foundation)58. Whenever any disagreement took place regarding the inclusion/exclusion of any study, it was resolved by discussion or consulting a third reviewer (A.P). Upon the completion of the database/grey literature search, all the references of the included studies were also screened, to find more eligible articles, if available. The date of ending the literature search was March 20, 2023.
Data extraction
The information recorded from the eligible studies were the type of patient allocation (i.e., different patients for each group or split-mouth), patient condition (i.e., on anti-thrombotic therapy or anti-coagulant/platelet medication when specified), the type of dental extraction (simple/surgical), the hemostatic agent(s) used, the conventional method used to stop bleeding (if any), the number of patients/extractions from all groups, the time to achieve hemostasis, and postoperative bleeding events and their time of occurrence.
Risk of bias
The revised Cochrane risk-of-bias tool for randomized trials (RoB 2) was used to assess the risk of bias in the eligible studies in this network meta-analysis59. This tool contains 5 domains (randomization process, deviations from the intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result) to check and evaluate. The level of bias for the included studies was determined using the Excel tool of RoB2.
Statistical analysis
A frequentist network meta-analysis (NMA) was performed using R software, version 4.2.2, utilizing “netmeta” and “dmetar” packages, implementing the random effect model. To avoid network disconnection, and because gauze/cotton pressure was used alone or with sutures, or depending on the case in the control groups of some studies33,35, the reference group in this meta-analysis was set as “conventional”, which included the application of gauze/cotton pressure with/without the use of sutures. Considering the slight variations in the definition of hemostasis in the included studies, NMA results regarding the continuous data of the time to reach hemostasis were obtained utilizing the standardized mean difference (SMD) and 95% confidence interval (CI), while the dichotomous data on bleeding events were analyzed implementing the odds ratio (OR) and 95% CI. Negative outcome measures for continuous data, as well as values lower than 1 for dichotomous data, indicated beneficial effects, i.e., a greater reduction in the time to reach hemostasis or bleeding events, respectively. In addition, negative ranges of confidence intervals for continuous data and ranges that did not include the value of 1 in the dichotomous data revealed statistical significance. A subgroup analysis was done on studies recruiting only patients undergoing simple (i.e., non-surgical) tooth extraction, as well as those taking anticoagulants. Heterogeneity was measured with I2-static, in which I2 values of 25%, 50%, and 75% represented low, moderate, and high heterogeneity, respectively60. Moreover, inconsistency between direct and indirect estimates was evaluated by the net-split function in the “netmeta” package of R software and measured by Cochran’s Q statistics for multivariate meta-analysis61.
P-scores were used to rank the treatments, where a higher value means better performance62. Network graphs and forest plots were generated to illustrate the relevant comparisons and treatment rankings, respectively.
Quality of evidence
The certainty of evidence was evaluated following the GRADE system63, which ranks the level of evidence as “high”, “moderate”, “low”, or “very low”, assessing several points (risk of bias, imprecision, inconsistency, indirectness, and publication bias), with a modification of adding “coherence” to judge the difference between direct and indirect evidence (i.e., transitivity) obtained from the network analysis. The quality of evidence was evaluated for both the mixed and indirect evidence, to assess the overall level of evidence from this study64. The tables of the quality of evidence from all possible comparisons under each outcome were generated using the CINeMA software65.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
Kumbargere Nagraj, S. et al. Interventions for treating post-extraction bleeding. Cochrane Database Syst. Rev. 3, CD011930. https://doi.org/10.1002/14651858.CD011930.pub3 (2018).
Lee, J. S., Kim, M. K. & Kang, S. H. Effect of warfarin discontinuation on the incidence of postoperative bleeding in tooth extraction. J. Korean Assoc. Oral Maxillofac. Surg. 46, 228–234. https://doi.org/10.5125/jkaoms.2020.46.4.228 (2020).
Bouloux, G. F., Steed, M. B. & Perciaccante, V. J. Complications of third molar surgery. Oral Maxillofac. Surg. Clin. N. Am. 19, 117–128. https://doi.org/10.1016/j.coms.2006.11.013 (2007).
Martinowitz, U. et al. Dental extraction for patients on oral anticoagulant therapy. Oral Surg. Oral Med. Oral Pathol. 70, 274–277. https://doi.org/10.1016/0030-4220(90)90139-j (1990).
Gupta, A., Epstein, J. B. & Cabay, R. J. Bleeding disorders of importance in dental care and related patient management. J. Can. Dent. Assoc. 73, 77–83 (2007).
Brancaccio, Y. et al. Evaluation of local hemostatic efficacy after dental extractions in patients taking antiplatelet drugs: A randomized clinical trial. Clin. Oral Investig. 25, 1159–1167. https://doi.org/10.1007/s00784-020-03420-3 (2021).
da Silva, R. V., Gadelha, T. B., Luiz, R. R. & Torres, S. R. Intra-alveolar epsilon-aminocaproic acid for the control of post-extraction bleeding in anticoagulated patients: Randomized clinical trial. Int. J. Oral Maxillofac. Surg. 47, 1138–1144. https://doi.org/10.1016/j.ijom.2018.02.013 (2018).
Bajkin, B. V., Vujkov, S. B., Milekic, B. R. & Vuckovic, B. A. Risk factors for bleeding after oral surgery in patients who continued using oral anticoagulant therapy. J. Am. Dent. Assoc. 146, 375–381. https://doi.org/10.1016/j.adaj.2015.01.017 (2015).
Pippi, R., Scorsolini, M. G., Luigetti, L., Pietrantoni, A. & Cafolla, A. Tooth extraction without discontinuation of oral antithrombotic treatment: A prospective study. Oral Dis. 27, 1300–1312. https://doi.org/10.1111/odi.13641 (2021).
Medeiros, F. B. et al. Bleeding evaluation during single tooth extraction in patients with coronary artery disease and acetylsalicylic acid therapy suspension: A prospective, double-blinded, and randomized study. J. Oral Maxillofac. Surg. 69, 2949–2955. https://doi.org/10.1016/j.joms.2011.02.139 (2011).
Al-Mubarak, S. et al. Evaluation of dental extractions, suturing and INR on postoperative bleeding of patients maintained on oral anticoagulant therapy. Br. Dent. J. 203, E15. https://doi.org/10.1038/bdj.2007.725 (2007).
Caliskan, M., Tükel, H. C., Benlidayi, M. E. & Deniz, A. Is it necessary to alter anticoagulation therapy for tooth extraction in patients taking direct oral anticoagulants? Med. Oral Patol. Oral Cir. Bucal. 22, e767–e773. https://doi.org/10.4317/medoral.21942 (2017).
Ruangchainicom, N., Mahardawi, B. & Sakdejayont, W. Topical hemostatic agents from an oral-surgery perspective. J. Oral Maxillofac. Surg. Med. Pathol. 33, 249–255. https://doi.org/10.1016/j.ajoms.2020.11.007 (2021).
Ockerman, A. et al. Local haemostatic measures after tooth removal in patients on antithrombotic therapy: A systematic review. Clin. Oral Investig. 23, 1695–1708. https://doi.org/10.1007/s00784-018-2576-x (2019).
Mahardawi, B. et al. The role of hemostatic agents after tooth extractions: A systematic review and meta-analysis. JADA 154, 3. https://doi.org/10.1016/j.adaj.2023.05.003 (2023).
Cipriani, A., Higgins, J. P., Geddes, J. R. & Salanti, G. Conceptual and technical challenges in network meta-analysis. Ann. Intern. Med. 159, 130–137. https://doi.org/10.7326/0003-4819-159-2-201307160-00008 (2013).
Moreno-Drada, J. A. et al. Effectiveness of local hemostatic to prevent bleeding in dental patients on anticoagulation: A systematic review and network meta-analysis. J. Craniomaxillofac. Surg. 49, 570–583. https://doi.org/10.1016/j.jcms.2021.04.014 (2021).
Puia, S. A., Hilber, E. M. & Garcia-Blanco, M. Randomized clinical trial comparing three local hemostatic agents for dental extractions in patients under chronic anticoagulant therapy—A comparative study. Ann. Maxillofac. Surg. 10, 292–296. https://doi.org/10.4103/ams.ams_276_20 (2020).
Ragab, H. R. & Melek, L. N. Comparison of two hemostatic agents in patients receiving anticoagulants without altering medication dosage. Egypt. Dent. J. 65, 3315–3321. https://doi.org/10.21608/edj.2019.74763 (2019).
Rai, S. & Rattan, V. Efficacy of feracrylum as topical hemostatic agent in therapeutically anticoagulated patients undergoing dental extraction: A comparative study. J. Maxillofac. Oral Surg. 18, 579–583. https://doi.org/10.1007/s12663-018-1156-6 (2019).
Queiroz, S. et al. Tranexamic acid as a local hemostasis method after dental extraction in patients on warfarin: A randomized controlled clinical study. Clin. Oral Investig. 22, 2281–2289. https://doi.org/10.1007/s00784-017-2327-4 (2018).
Muralidharan, G. Evaluation of Post Extraction Hemostasis in Cardiac Patients with Gelatamp Dental Dressing Without Stopping Aspirin and Clopidogrel Therapy (Best Dental Science College, 2017).
Bajkin, B. V. et al. Comparison of efficacy of local hemostatic modalities in anticoagulated patients undergoing tooth extractions. Vojnosanit Pregl. 71, 1097–1101. https://doi.org/10.2298/vsp1412097b (2014).
Ripollés-de Ramón, J., Muñoz-Corcuera, M., Bravo-Llatas, C. & Bascones-Martínez, A. Tranexamic acid gel in patients treated with oral anticoagulants. Med. Clin. (Barc.) 143, 484–488. https://doi.org/10.1016/j.medcli.2013.07.028 (2014).
Çakarer, S. et al. Evaluation of the hemostatic effects of Ankaferd blood stopper during dental extractions in patients on antithrombotic therapy. Clin. Appl. Thromb. Hemost. 19, 96–99. https://doi.org/10.1177/1076029611435836 (2013).
Al-Belasy, F. A. & Amer, M. Z. Hemostatic effect of n-butyl-2-cyanoacrylate (histoacryl) glue in warfarin-treated patients undergoing oral surgery. J. Oral Maxillofac. Surg. 61, 1405–1409. https://doi.org/10.1016/j.joms.2002.12.001 (2003).
Halfpenny, W., Fraser, J. S. & Adlam, D. M. Comparison of 2 hemostatic agents for the prevention of postextraction hemorrhage in patients on anticoagulants. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 92, 257–259. https://doi.org/10.1067/moe.2001.115463 (2001).
Ockerman, A. et al. Tranexamic acid and bleeding in patients treated with non-vitamin K oral anticoagulants undergoing dental extraction: The EXTRACT-NOAC randomized clinical trial. PLoS Med. 18, e1003601. https://doi.org/10.1371/journal.pmed.1003601 (2021).
Souto, J. C., Oliver, A., Zuazu-Jausoro, I., Vives, A. & Fontcuberta, J. Oral surgery in anticoagulated patients without reducing the dose of oral anticoagulant: A prospective randomized study. J. Oral Maxillofac. Surg. 54, 27–32. https://doi.org/10.1016/s0278-2391(96)90297-9 (1996).
Radhakrishna, S., Shukla, V. & Shetty, S. K. Is chitosan dental dressing better than cotton gauze in achieving hemostasis in patients on antithrombotics? J. Oral Maxillofac. Surg. 81, 224–231. https://doi.org/10.1016/j.joms.2022.10.011 (2023).
Redwan, H. Evaluating chitosan effectiveness as hemostatic agent on patients on antiplatelet Th. Int. J. Dent Oral Sci. 7, 164. https://doi.org/10.19070/2377-8075-20000164 (2020).
Giudice, A. et al. Dental extractions for patients on oral antiplatelet: A within-person randomised controlled trial comparing haemostatic plugs, advanced-platelet-rich fibrin (A-PRF+) plugs, leukocyte- and platelet-rich fibrin (L-PRF) plugs and suturing alone. Int. J. Oral Implantol. (Berl.) 12, 77–87 (2019).
Seethamsetty, S. et al. A comparative evaluation of the effectiveness of chitosan-based dressing and conventional method of hemostasis in patients on oral antithrombotic therapy without therapy interruption. J. Pharm. Bioallied Sci. 11, S18–S23. https://doi.org/10.4103/jpbs.JPBS_229_18 (2019).
Pippi, R., Santoro, M. & Cafolla, A. The use of a chitosan-derived hemostatic agent for postextraction bleeding control in patients on antiplatelet treatment. J. Oral Maxillofac. Surg. 75, 1118–1123. https://doi.org/10.1016/j.joms.2017.01.005 (2017).
Sharma, S., Kale, T. P., Balihallimath, L. J. & Motimath, A. Evaluating effectiveness of axiostat hemostatic material in achieving hemostasis and healing of extraction wounds in patients on oral antiplatelet drugs. J. Contemp. Dent. Pract. 18, 802–806. https://doi.org/10.5005/jp-journals-10024-2130 (2017).
Kumar, K. R., Kumar, J., Sarvagna, J., Gadde, P. & Chikkaboriah, S. Hemostasis and post-operative care of oral surgical wounds by hemcon dental dressing in patients on oral anticoagulant therapy: A split mouth randomized controlled clinical trial. J. Clin. Diagn. Res. 10, 37–40. https://doi.org/10.7860/jcdr/2016/17275.8462 (2016).
Pippi, R., Santoro, M. & Cafolla, A. The effectiveness of a new method using an extra-alveolar hemostatic agent after dental extractions in older patients on oral anticoagulation treatment: An intrapatient study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 120, 15–21. https://doi.org/10.1016/j.oooo.2015.02.482 (2015).
Soares, E. C. et al. Postoperative hemostatic efficacy of gauze soaked in tranexamic acid, fibrin sponge, and dry gauze compression following dental extractions in anticoagulated patients with cardiovascular disease: A prospective, randomized study. Oral Maxillofac. Surg. 19, 209–216. https://doi.org/10.1007/s10006-014-0479-9 (2015).
Giray, C. B., Sungur, A., Atasever, A. & Araz, K. Comparison of silk sutures and n-butyl-2-cyanoacrylate on the healing of skin wounds. A pilot study. Aust. Dent. J. 40, 43–45. https://doi.org/10.1111/j.1834-7819.1995.tb05613.x (1995).
Suthar, P. et al. Comparing intra-oral wound healing after alveoloplasty using silk sutures and n-butyl-2-cyanoacrylate. J. Korean Assoc. Oral Maxillofac. Surg. 46, 28–35. https://doi.org/10.5125/jkaoms.2020.46.1.28 (2020).
Giray, C. B., Atasever, A., Durgun, B. & Araz, K. Clinical and electron microscope comparison of silk sutures and n-butyl-2-cyanoacrylate in human mucosa. Aust. Dent. J. 42, 255–258. https://doi.org/10.1111/j.1834-7819.1997.tb00130.x (1997).
Javelet, J., Torabinejad, M. & Danforth, R. Isobutyl cyanoacrylate: A clinical and histologic comparison with sutures in closing mucosal incisions in monkeys. Oral Surg. Oral Med. Oral Pathol. 59, 91–94. https://doi.org/10.1016/0030-4220(85)90123-9 (1985).
Oladega, A. A., James, O. & Adeyemo, W. L. Cyanoacrylate tissue adhesive or silk suture for closure of surgical wound following removal of an impacted mandibular third molar: A randomized controlled study. J. Craniomaxillofac. Surg. 47, 93–98. https://doi.org/10.1016/j.jcms.2018.10.018 (2019).
Setiya, S., Halli, R., Shah, A., Chhabaria, G. & Singh, T. Comparative evaluation of efficacy of tissue glue and sutures after surgical removal of impacted mandibular third molars—A prospective controlled clinical study. J. Oral Maxillofac. Surg. Med. Pathol. 27, 183–188. https://doi.org/10.1016/j.ajoms.2014.06.007 (2015).
Rewainy, M., Osman, S. & El-prince, N. The use of n-butyl cyanoacrylate adhesive in the closure of mucoperiosteal flap after the surgical extraction of impacted mandibular third molar. Alex. Dent. J. 40, 152–159. https://doi.org/10.21608/adjalexu.2015.59139 (2015).
Tengborn, L., Blombäck, M. & Berntorp, E. Tranexamic acid—An old drug still going strong and making a revival. Thromb. Res. 135, 231–242. https://doi.org/10.1016/j.thromres.2014.11.012 (2015).
Ker, K., Beecher, D. & Roberts, I. Topical application of tranexamic acid for the reduction of bleeding. Cochrane Database Syst. Rev. https://doi.org/10.1002/14651858.CD010562.pub2 (2013).
de Vasconcellos, S. J. et al. Topical application of tranexamic acid in anticoagulated patients undergoing minor oral surgery: A systematic review and meta-analysis of randomized clinical trials. J. Craniomaxillofac. Surg. 45, 20–26. https://doi.org/10.1016/j.jcms.2016.10.001 (2017).
Shen, E. C. et al. Releasing growth factors from activated human platelets after chitosan stimulation: A possible bio-material for platelet-rich plasma preparation. Clin. Oral Implants Res. 17, 572–578. https://doi.org/10.1111/j.1600-0501.2004.01241.x (2006).
Burkatovskaya, M. et al. Use of chitosan bandage to prevent fatal infections developing from highly contaminated wounds in mice. Biomaterials 27, 4157–4164. https://doi.org/10.1016/j.biomaterials.2006.03.028 (2006).
Elangwe, C. N. et al. A review on chitosan and cellulose hydrogels for wound dressings. Polymers 14, 5163. https://doi.org/10.3390/polym14235163 (2022).
Zhang, S. et al. Application status and technical analysis of chitosan-based medical dressings: A review. RSC Adv. 10, 34308–34322. https://doi.org/10.1039/d0ra05692h (2020).
Guo, Y. et al. Advances in the development and optimization strategies of the hemostatic biomaterials. Front. Bioeng. Biotechnol. 10, 1062676. https://doi.org/10.3389/fbioe.2022.1062676 (2022).
Seyednejad, H., Imani, M., Jamieson, T. & Seifalian, A. M. Topical haemostatic agents. Br. J. Surg. 95, 1197–1225. https://doi.org/10.1002/bjs.6357 (2008).
Achneck, H. E. et al. A comprehensive review of topical hemostatic agents: Efficacy and recommendations for use. Ann. Surg. 251, 217–228. https://doi.org/10.1097/SLA.0b013e3181c3bcca (2010).
Sundaram, C. P. & Keenan, A. C. Evolution of hemostatic agents in surgical practice. Indian J. Urol. 26, 374–378. https://doi.org/10.4103/0970-1591.70574 (2010).
Hutton, B. et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: Checklist and explanations. Ann. Intern. Med. 162, 777–784. https://doi.org/10.7326/m14-2385 (2015).
Ouzzani, M., Hammady, H., Fedorowicz, Z. & Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 5, 4. https://doi.org/10.1186/s13643-016-0384-4 (2016).
Sterne, J. A. C. et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 366, l4898. https://doi.org/10.1136/bmj.l4898 (2019).
Higgins, J. P., Thompson, S. G., Deeks, J. J. & Altman, D. G. Measuring inconsistency in meta-analyses. BMJ 327, 557–560. https://doi.org/10.1136/bmj.327.7414.557 (2003).
Krahn, U., Binder, H. & König, J. A graphical tool for locating inconsistency in network meta-analyses. BMC Med. Res. Methodol. 13, 35. https://doi.org/10.1186/1471-2288-13-35 (2013).
Rücker, G. & Schwarzer, G. Ranking treatments in frequentist network meta-analysis works without resampling methods. BMC Med. Res. Methodol. 15, 58. https://doi.org/10.1186/s12874-015-0060-8 (2015).
Guyatt, G. H. et al. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 336, 924–926. https://doi.org/10.1136/bmj.39489.470347.AD (2008).
Salanti, G., Del Giovane, C., Chaimani, A., Caldwell, D. M. & Higgins, J. P. Evaluating the quality of evidence from a network meta-analysis. PLoS ONE 9, e99682. https://doi.org/10.1371/journal.pone.0099682 (2014).
Nikolakopoulou, A. et al. CINeMA: An approach for assessing confidence in the results of a network meta-analysis. PLoS Med. 17, e1003082. https://doi.org/10.1371/journal.pmed.1003082 (2020).
Acknowledgements
This research project is supported by the Second Century Fund (C2F), Chulalongkorn University.
Author information
Authors and Affiliations
Contributions
Conceptualization and Methodology: B.M.; Formal analysis and investigation: B.M., S.J., and A.S.; Writing—original draft preparation: B.M. and K.T.; Writing—review and editing: K.T.; Project Supervision: A.P. All authors read and approved the final version of this submission.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Mahardawi, B., Jiaranuchart, S., Arunjaroensuk, S. et al. The effect of different hemostatic agents following dental extraction in patients under oral antithrombotic therapy: a network meta-analysis. Sci Rep 13, 12519 (2023). https://doi.org/10.1038/s41598-023-39023-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-39023-7
This article is cited by
-
Cyanoacrylate tissue adhesive versus silk sutures for mandibular third molar surgery: a systematic review and meta-analysis
Clinical Oral Investigations (2024)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
