
Abstract
Enchondroma is the most common bone tumor in the hand. While standard surgical procedure is intra-lesional excision and bone grafting, there is a dispute between allogeneic bone, autogenous bone, and synthetic bone substitute grafting. Diverse adjuvant treatments have been introduced to reduce recurrence, but results are mixed with controversies. Meanwhile, whether existing descriptive classification could predict treatment outcome remains unclear. Thus, we reviewed patients with solitary enchondroma of the hand who underwent simple curettage followed by allogeneic cancellous bone chip impaction grafting. Eighty-eight patients with more than 5 years of follow-up were enrolled. Demographic data, local recurrence, and complications were reviewed. Duration of consolidation and the difference according to Takigawa classification were assessed. Range of motion (ROM), and functional scores were also evaluated. There were 51 women and 37 men, with a mean age of 37.9 years. Mean follow-up was 10.2 years. Recurrence occurred only in one patient. There was no complication. Mean postoperative total active motions of fingers and thumb were 239° and 132.9°. Mean modified Disabilities of the Arm, Shoulder, Hand score, and Musculoskeletal Tumor Society Score were 1.63, and 99.2 at the last follow-up. Consolidation, ROM, and functional scores according to Takigawa classification showed no significant differences. This study suggests that simple curettage with impaction grafting of allogeneic cancellous bone chip is a feasible method for treating solitary enchondromas involving short tubular bone of the hand with good long-term outcomes. Postoperative recurrence and complication rates were very low. Radiographic and clinical results were good regardless of the previous radiological classification.
Similar content being viewed by others


Introduction
Enchondroma is the most common benign bone tumor in the hand, with 40–47% of cases involving the hand1,2,3,4. Due to its slow growth, most cases are asymptomatic and incidentally detected. Symptomatic cases are usually in the setting of large lesions or pathologic fractures. Surgery is considered for both histopathologic confirmation and treatment or prevention of pathological fractures5. The standard surgical procedure most commonly used is intra-lesional excision combined with bone grafting6,7. Bone grafting is performed to promote bone regeneration and restore bone strength for skeletal defects following tumor excision4,8.
There is still a dispute between allogeneic bone, autogenous bone, and synthetic bone substitutes grafting. Advocates for allogeneic bone grafting assert that this surgical procedure is relatively straightforward with outcomes comparable to those of autogenous bone grafting9. However, there are still concerns about immune response, disease transmission, postoperative infection, and price associated with allogeneic bone grafting. Autogenous bone grafting has demonstrated excellent bone formation without these aforementioned complications. However, donor-site complications might occur7,10. Recently, good results of synthetic bone substitutes grafting have been reported11,12,13,14, but there are still concerns about foreign body reaction, long-term prognosis, and price. Therefore, which surgical method to use may depend on the surgeon’s preference.
Incidence of recurrence following resection and bone grafting is 2–15%4,15,16, which is similar between autogenous and allogeneic bone grafting16. While diverse adjuvant treatment methods in addition to curettage have been introduced to reduce recurrence, results are mixed with controversies. Therefore, such adjuvant treatments might not be helpful for treating solitary enchondroma of the hand.
In 1971, Takigawa first classified 110 cases of chondroma according to their shapes. Since then, the Takigawa classification has been often used in the literature. It divides chondromas into two types (monostotic and polycentric types) and five forms (central, eccentric, combined, polycentric and giant forms) based on simple radiographic findings17. In the literature, this system is mainly used for morphological classification. However, whether the descriptive classification could predict treatment outcome or prognosis remains unclear.
In this study, we aimed to address the following questions pertaining to the solitary enchondroma of the hand: (1) Can simple curettage without any adjuvant treatment prevent long-term recurrence? (2) Is allogeneic cancellous bone chip impaction grafting sufficient to promote bone regeneration with fewer complications? (3) What are clinical implications of conventional radiographic classification methods for solitary enchondroma of the hand?
Results
General patient information
Among 88 patients who were enrolled in this study, there were 51 women and 37 men. Their mean age was 37.9 years (range, 13–72 years). All lesions were confirmed as enchondroma by histologic examination. Symptoms included only pain, only deformity, and painful deformity and nineteen patients were diagnosed incidentally. The average duration of symptom before surgery was 3.3 months (range, 1 week–5 months). The mean amount of allogeneic cancellous bone used for surgery was 3 cc (range, 1.5–15 cc). The mean follow-up period after surgery was 10.2 years (range, 5.0–15.6 years). In the follow-up period, recurrence occurred only in one patient. This patient was a 16-year-old male with a lesion of 16.5 mm and type 1 in the proximal phalanx. A new cystic lesion was found at 26 months after the first operation after he reported recurred pain. Repeated curettage and allogeneic cancellous bone chip impaction grafting were performed. Pathology confirmed the enchondroma.
Radiographic results
Proximal phalanges were most frequently affected, followed by metacarpal bones, mid-phalanges, and distal phalanges. The most common affected sites among the fingers were the index finger and the little finger (Fig 1). Mean long axis of the lesion was 15 mm (range, 6–35 mm). The mean radiological consolidation period was 6 weeks (range, 4–12 weeks). There were 23 (26.1%) patients with Takigawa type A, 35 (39.8%) patients with type B, 21 (23.9%) patients with type C, and 9 (10.2%) patients with type D. The difference in time for radiological consolidation according to the Takigawa classification was not significant (p = 0.166) (Table 1) (Figs 2 and 3).

This figure shows locations of lesions. The most common affected sites among the fingers were the index and little fingers. Proximal phalanges were most frequently affected, followed by the metacarpal bones, middle phalanges, and distal phalanges among the bones.

A 13-year-old female with enchondroma of polycentric and giant form in the proximal phalanx of the right index finger. Simple radiographs taken before surgery (A), immediately (B), 1 month (C), 2 months (D), 1 year (E), and 9 years (F) after surgery.

A 18-year-old male with enchondroma of giant form in the fourth metacarpus of the Lt. hand. Simple radiographs taken before surgery (A), immediately (B), 1 month (C), 2 months (D), 1 year (E), and 6 years (F) after surgery.
Functional results
Postoperative range of motion (ROM) measurements at 6 months after surgery were reported in 85 out of 88 patients. Mean preoperative and postoperative total active motion (TAM) of fingers were 197.9° (range, 80°–250°) and 239.0° (range, 210°–250°), respectively. Mean preoperative and postoperative TAMs of thumb were 124.3° (range, 100°–140°) and 132.9° (range, 120°–140°), respectively. ROMs of fingers according to the Takigawa classification showed no significant difference (p = 0.131) (Table 1). Mean preoperative modified Disabilities of the Arm, Shoulder, and Hand (DASH) score and Musculoskeletal Tumor Society (MSTS) score were 2.07 (range, 1–9.1) and 84.7 (30–100), respectively. Mean modified DASH score and MSTS score at the last follow-up visit were 1.63 (range, 0–5), and 99.2 (range, 90.0–100), respectively. These two scores at the last follow-up according to the Takigawa classification showed no significant difference (p = 0.206, and p = 0.827) (Table 1).
Complications
After surgery, there was no complication associated with allogeneic bone grafting such as immune response, disease transmission, or postoperative infection until the final follow-up.
Discussion
There is debate about which surgical method is superior for treating solitary enchondroma of the hand. Whether curettage alone is sufficient and whether allogeneic or autogenous bone grafting is the optimal approach remains unclear. The classification suggested by Takigawa17 is commonly used for morphological descriptions. However, whether this classification system can predict treatment outcomes has not been demonstrated in large-scale case series. Our study analyzed long-term (> 5 years) clinical outcomes following simple curettage and allogeneic cancellous bone chip impaction grafting in 88 patients with a solitary enchondroma of the hand. In our experience, there was a good bone formation with only one documented recurrence. There were no complications associated with allogeneic cancellous bone chips. Our results also revealed no significant differences in duration of consolidation, ROM, or postoperative clinical scores according to the Takigawa classification.
Adjuvant treatments such as high-speed burring, alcohol soaking, CO2 laser ablation and bone cementation can be used to reduce risk of recurrence after curettage for endochondroma of the hand4,17,18,19. A previous study has reported that the difference in recurrence is not significant between case with alcohol treatment and those with high-speed burring20. Another research has revealed no treatment-related complications and recurrence when additional therapy with CO2 laser is performed after curettage19. In this study, recurrence developed only in one out of 88 patients even without adjuvant treatment after curettage using curettes. Considering surgical time and effort required for additional therapy, simple curettage is regarded a more efficient operational procedure than curettage followed by additional treatment.
While autogenous bone transplantation is still used to reconstruct a bone defect after curettage in the hand enchondroma, it might have donor site problems such as infection, hematoma, pain, and paresthesia10. In addition, operative time is prolonged10. Anterior iliac crest bone is preferred for autografting in enchondroma of the hand. Complications have been much reduced with the development of surgical instruments and techniques, but donor site morbidity was still reported as high as 7%21 after anterior iliac crest bone harvesting. It was reported that three patients complained of scar numbness among 37 with an average follow-up of 4.5 years22. In children who underwent iliac bone harvesting, school was resumed after an average of 12.6 days and sport activities after 1 month due to pain regardless of the used pain management protocol23. While bone can be harvested from the distal radius, there may still be donor site morbidity and harvest volume can be limited24. A study comparing curettage alone, autografting, bone substitute insertion, and cementation reported that the complication rate was 0.7, 3.5, 0, and 2.0%, respectively25. There is no significant difference in recurrence, but complications such as infection and donor site pain were prominent in case of autografting12. In that sense, the use of allogeneic bone or synthetic bone substitute grafting is increasing. Widely used synthetic bone substitutes are based on calcium phosphate, calcium sulphate, and the products are available in various forms such as granular and injectable ones12,25. They are convenient to use, however, possible disadvantages are foreign body reaction, delayed integration, insufficient defect consolidation, and lack of mechanical strength26. It was reported that one case of foreign body reaction among 11 patients with enchondroma who had synthetic bone substitute grafting12. Although allogeneic bone might potentially lead to immunological problems and disease morbidity, currently no such cases have been reported in previous studies7,27. Such complications did not occur in the present study, either.
As for consolidation period, autogenous bone grafting is the fastest, but allogeneic bone grafting is comparable. A study reported that the autografts took a mean of 38 days and allograft took a mean of 51 days for consolidation in 76 patients with 15-year follow-up period8. In the current study, the mean radiological consolidation period was 6 weeks (range, 4–12 weeks). There are still controversies on the timing of bone integration, and it can take 9 ~ 12 months in synthetic bone grafting12. While it took only 4 weeks to achieve radiologic consolidation in a case report11, but the outcome is difficult to be reliable due to the small number of cases.
Meanwhile, we should consider that early movement is important to prevent finger contracture in the treatment of hand enchondroma. Thinner cortical bone can increase the risk of fracture and prolong the immobilization period. Since contractures can occur with prolonged immobilization, it is necessary to have some stability after curettage. Therefore, augmentation after curettage might be needed. Bone cement such as PMMA, hydroxyapatite, Plaster of Paris can be used to fill the cavity for augmentation4,28,29. PMMA provides immediate mechanical strength to withstand weight bearing30. Cement injection after curettage has the advantage of enabling early joint motion. However, since the hand primarily does not bear a body weight, such immediate high mechanical strength is not required for finger motion. In addition, the incidence of infection and cellulitis caused by PMMA is higher than that by allogeneic bone30. We believe that impaction procedure could provide more structural stability in bone grafting31. It can also promote bone regeneration unlike other materials. Therefore, allogeneic cancellous bone chip impaction grafting is considered to be a safe and more efficient surgical technique for treatment of solitary enchondroma of the hand.
Since the first introduction of a morphological classification for hand enchondroma17, several studies have reported on its types and forms. While some reports7,12,16,17 showed that the central form was the most common one with the eccentric form being the second most common followed by the giant form which was the rarest, another study32 assessing isolated enchondroma of the hand reported that the eccentric form was the most common one. In the current study regarding the solitary enchondroma involving the short tubular bone of the hand, the most common form was the eccentric form, followed by the central form. There was no giant form. While studies on the treatment results according to classification are still lacking, there were no significant differences in consolidation period, ROM, or postoperative clinical scores according to the Takigawa classification in this study.
The current study had several limitations. First, this was a retrospective case series without a control group. We could not compare results of other surgical methods as the authors prefer this surgical method for solitary enchondroma of the hand and rarely use other surgical methods for a long time. In this study, 38 cases using other surgical methods were excluded. Although curettage followed by autogenous bone grafting has been considered the standard of surgical care, major complications might occur at the donor site33. To the best of our knowledge, we are the first to report long-term outcomes of allogeneic bone grafting with such a large number of cases. Considering previous reports on autografting, our method does not seem to be inferior as it has no donor site problems7,9. The second limitation was its retrospective study design. Therefore, some data were missing. Although the surgeon tried to follow up the patients at regular intervals, the consolidation period might not be accurate because it was evaluated at the time of the patient’s visit. Currently, the authors are conducting a prospective trial comparing autogenous and allogeneic bone grafting. Moreover, 93 patients with a follow-up of less than 5 years were excluded, which might have led to a selection bias. However, it is more common for patients with solitary enchondroma of the hand to fail to follow up when they are well without experiencing postoperative problems. Besides, local recurrence did not occur during their follow-up period in the 93 excluded patients. In this paper, only patients who were followed up for more than 5 years were included, demonstrating that the results of this surgical method were maintained well in the long term.
In conclusion, this study suggests that simple curettage with impaction grafting of allogeneic cancellous bone chip is a feasible surgical method for treating solitary enchondromas involving short tubular bone of the hand with good long-term outcomes. Postoperative recurrence and complication rates were very low. Radiographic and clinical results were good regardless of the radiological classification of lesions. Although previous classification is useful for explaining the lesion, but it may not affect treatment outcomes.
Methods
Study design and participants
In this retrospective, single-center study, chart review was performed to identify patients with histologically proven solitary enchondroma involving the short tubular bone of the hand who underwent simple curettage followed by allogeneic cancellous bone chip impaction grafting. The Catholic University of Korea St. Vincent’s Hospital Institutional Review Board approved this study (VC22RASI0161) and waived the need for informed consent as this retrospective medical record review was deemed a minimal risk study without collecting personal identifiable information. The research was carried out according to guidelines and regulations of the ethic committee.
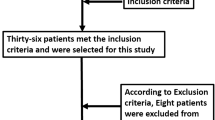
Inclusion criteria were patients (1) with histologically proven solitary enchondroma involving the short tubular bone of the hand, (2) without pathologic fractures, (3) who underwent simple curettage and allogeneic cancellous bone chip impaction grafting, and (4) with postoperative follow-up period longer than 5 years. Therefore, patients (1) with multiple lesions, (2) pathologic fractures and (3) follow-up period shorter than 5 years, and (4) who had autogenous bone grafting or any adjuvant treatment were excluded. From January 2006 to December 2016, 247 consecutive patients were diagnosed with enchondroma of the hand. Five patients with multiple enchondromas, and 23 patients with pathologic fractures were excluded. In addition, 93 patients who had insufficient follow-up period (< 5 years) and 38 patients who had autogenous bone grafting or any adjuvant treatment were excluded. Finally, a total of 88 patients who underwent simple curettage followed by allogeneic cancellous bone chip impaction grafting without any adjuvant treatment were enrolled in this study (Fig 4).

STROBE diagram demonstrates the patient selection process.
Surgical procedure
Simple curettage followed by allogeneic cancellous bone chip impaction grafting was performed. When the lesion was located on the phalanx, a dorsal or a lateral approach was used. A dorsal approach was used for metacarpal lesions. A large window was made in the cortical bone with a burr under fluoroscopy to confirm the extent of the lesion. Thorough curettage using curettes was performed to completely excise the lesion until cortical bone or normal cancellous bone was visible. The surgical specimen was sent to the hospital pathology department for histologic evaluation. After saline irrigation of the surgical site, allogeneic cancellous bone chip impaction grafting was performed using fluoroscopic guidance. After surgery, the hand was immobilized with short arm splint for approximately 2 weeks.
Radiographic evaluation
Patients were usually scheduled to have follow-up visits every 4 weeks during the first 3 months. Patients were then instructed to follow up every 3–6 months during the first year on a case-by-case basis. A yearly follow-up visit was then recommended. At each visit, patients underwent radiographic and clinical evaluations. Preoperative anteroposterior (AP), lateral, and oblique plain radiographs of the affected hand and postoperative radiographs obtained during follow-up period were evaluated. Preoperatively, the anatomical location of the lesion, size of the lesion, and Takigawa classification17 were assessed. Lesions were categorized into four types: central (type A), eccentric (type B), combined (type C), and polycentric or giant (type D).
Radiographic consolidation was defined by the presence of normal cortical bone and if the bone defect was less than 3 mm on plain radiographs after surgery. This finding corresponds to grade I of Tordai classification34 (grade I, normal cortical bone or a bone defect smaller than 3 mm in diameter; grade II, bone defects with a diameter 4 to 10 mm; grade III, bone defect larger than 10 mm with characteristics of enchondroma). We reviewed the duration of consolidation and analyzed the difference in duration according to the Takigawa classification of the lesion. Recurrent lesions were defined if the patient reported new pain or a new cystic change was noted on follow-up radiograph, and an enchondroma was histologically re-confirmed after re-operation.
Clinical evaluation
Age, sex, and preoperative symptom duration were reviewed. ROM was assessed using TAM of the affected digit. TAM was defined as the sum of active flexion and extension motion of metacarpophalangeal (MCP), proximal interphalangeal (PIP) and distal interphalangeal (DIP) arc of motion in degrees. Normal TAMs of the finger and thumb were reported as 260 and 140 degrees, respectively. We reviewed records of preoperative ROM and ROM at 6 months after surgery, as it was expected that there may be no significant changes in ROM after postoperative 6 months. Modified DASH score35 and MSTS score36 were evaluated. We analyzed the difference in ROM and the functional scores according to the Takigawa classification. Complications associated with allogeneic bone graft, including immune response, disease transmission, and postoperative infection, were reviewed.
Statistical analysis
Continuous variables are presented as means and ranges. Categorical variables are presented as numbers and percentages. One-way analysis of variance (ANOVA) was used to analyze the differences in postoperative consolidation period, ROM, modified DASH and MSTS scores according to the Takagawa classification. P value less than 0.05 was considered statistically significant.
Data availability
All data generated or analyzed during this study are included in this published article.
References
Payne, W. T. & Merrell, G. Benign bony and soft tissue tumors of the hand. J. Hand Surg. Am. 35(11), 1901–1910. https://doi.org/10.1016/j.jhsa.2010.08.015 (2010).
Jacobson, M. E. & Ruff, M. E. Solitary enchondroma of the phalanx. J. Hand Surg. Am. 36(11), 1845–1847. https://doi.org/10.1016/j.jhsa.2011.05.002 (2011).
Plate, A. M., Lee, S. J., Steiner, G. & Posner, M. A. Tumorlike lesions and benign tumors of the hand and wrist. J. Am. Acad. Orthop. Surg. 11(2), 129–141. https://doi.org/10.5435/00124635-200303000-00007 (2003).
Tang, C., Chan, M., Fok, M. & Fung, B. Current management of hand enchondroma: a review. Hand Surg. 20(1), 191–195. https://doi.org/10.1142/s0218810415300028 (2015).
Joosten, U., Joist, A., Frebel, T., Walter, M. & Langer, M. The use of an in situ curing hydroxyapatite cement as an alternative to bone graft following removal of enchondroma of the hand. J. Hand Surg. Br. 25(3), 288–291. https://doi.org/10.1054/jhsb.2000.0383 (2000).
Hasselgren, G., Forssblad, P. & Tornvall, A. Bone grafting unnecessary in the treatment of enchondromas in the hand. J. Hand Surg. Am. 16(1), 139–142 (1991).
Bauer, R. D., Lewis, M. M. & Posner, M. A. Treatment of enchondromas of the hand with allograft bone. J. Hand Surg. Am. 13(6), 908–916 (1988).
Yercan, H., Ozalp, T., Coskunol, E. & Ozdemir, O. Long-term results of autograft and allograft applications in hand enchondromas. Acta Orthop. Traumatol. Turc. 38(5), 337–342 (2004).
Jewusiak, E. M., Spence, K. F. & Sell, K. W. Solitary benign enchondroma of the long bones of the hand. J. Bone Joint Surg. Am. 53(8), 1587–1590 (1971).
Younger, E. M. & Chapman, M. W. Morbidity at bone graft donor sites. J. Orthop. Trauma 3(3), 192–195 (1989).
Raducu, L., Anghel, A., Vermesan, S. & Sinescu, R. D. Finger enchondroma treated with bone substituents - a case presentation. J. Med. Life 7(2), 223–225 (2014).
Hung, Y. W. et al. Local review of treatment of hand enchondroma (artificial bone substitute versus autologous bone graft) in a tertiary referral centre: 13 years’ experience. Hong Kong Med. J. 21(3), 217–223. https://doi.org/10.12809/hkmj144325 (2015).
Yasuda, M., Masada, K. & Takeuchi, E. Treatment of enchondroma of the hand with injectable calcium phosphate bone cement. J. Hand Surg. Am. 31(1), 98–102. https://doi.org/10.1016/j.jhsa.2005.08.017 (2006).
Ciobanu, P. et al. Treatment of Bone Defects Resulted after Excision of Enchondroma of the Hand in 15 Patients, Comparing the Techniques of Autologous Bone Graft, Injectable Bone Substitute and Spontaneous Healing. Appl. Sci. 12(3), 1300 (2022).
Gaulke, R. & Suppelna, G. Solitary enchondroma at the hand. Long-term follow-up study after operative treatment. J. Hand Surg. Br. 29(1), 64–66 (2004).
Sassoon, A. A., Fitz-Gibbon, P. D., Harmsen, W. S. & Moran, S. L. Enchondromas of the hand: factors affecting recurrence, healing, motion, and malignant transformation. J. Hand Surg. Am. 37(6), 1229–1234. https://doi.org/10.1016/j.jhsa.2012.03.019 (2012).
Takigawa, K. Chondroma of the bones of the hand. A review of 110 cases. J. Bone Joint Surg. Am. 53(8), 1591–1600 (1971).
Milgram, J. W. The origins of osteochondromas and enchondromas. A histopathologic study. Clin. Orthop. Relat. Res. 174, 264–284 (1983).
Giles, D. W., Miller, S. J. & Rayan, G. M. Adjunctive treatment of enchondromas with CO2 laser. Lasers Surg. Med. 24(3), 187–193 (1999).
Cha, S. M., Shin, H. D., Kim, K. C. & Park, I. Y. Extensive curettage using a high-speed burr versus dehydrated alcohol instillation for the treatment of enchondroma of the hand. J. Hand Surg. Eur. 40(4), 384–391. https://doi.org/10.1177/1753193413517204 (2015).
Huang, Y. C. et al. Comparing morbidities of bone graft harvesting from the anterior iliac crest and proximal tibia: a retrospective study. J. Orthop. Surg. Res. 13(1), 115. https://doi.org/10.1186/s13018-018-0820-3 (2018).
Shin, S. R. & Tornetta, P. 3rd. Donor site morbidity after anterior iliac bone graft harvesting. J. Orthop. Trauma 30(6), 340–343. https://doi.org/10.1097/BOT.0000000000000551 (2016).
Tache, A. & Mommaerts, M. Y. Pain management at iliac donor sites after grafting of alveolar clefts. System. Rev. Cleft Lip Palate 51(1), 62–69. https://doi.org/10.1016/j.ijom.2021.05.004 (2021).
Orman, O. et al. Comparison of distal radius autograft technique with iliac crest autograft technique in solitary finger enchondromas. Sisli Etfal Hastan Tip Bull. 56(3), 400–407. https://doi.org/10.14744/SEMB.2022.00483 (2022).
Bachoura, A., Rice, I. S., Lubahn, A. R. & Lubahn, J. D. The surgical management of hand enchondroma without postcurettage void augmentation: authors’ experience and a systematic review. Hand (N Y) 10(3), 461–471. https://doi.org/10.1007/s11552-015-9738-y (2015).
Shibuya, N. & Jupiter, D. C. Bone graft substitute: Allograft and xenograft. Clin. Podiatr. Med. Surg. 32(1), 21–34. https://doi.org/10.1016/j.cpm.2014.09.011 (2015).
Graham, S. M. et al. Biological therapy of bone defects: The immunology of bone allo-transplantation. Expert Opin. Biol. Ther. 10(6), 885–901. https://doi.org/10.1517/14712598.2010.481669 (2010).
Peltier, L. F. The use of plaster of Paris to fill large defects in bone: a preliminary report 1959. Clin. Orthop. Relat. Res. 382, 3–5. https://doi.org/10.1097/00003086-200101000-00002 (2001).
Schmitz, J. P., Hollinger, J. O. & Milam, S. B. Reconstruction of bone using calcium phosphate bone cements: A critical review. J. Oral Maxillofac. Surg. 57(9), 1122–1126 (1999).
Chen, C. J. & Brien, E. W. Early postoperative compilations of bone filling in curettage defects. J. Orthop. Surg. Res. 14(1), 261. https://doi.org/10.1186/s13018-019-1297-4 (2019).
Lunde, K. B., Foss, O. A., Fosse, L. & Skallerud, B. Constitutive models for constrained compression of unimpacted and impacted human morselized bone grafts. J. Biomech. Eng. 130(6), 061014. https://doi.org/10.1115/1.2979878 (2008).
Zarrate, J. S., Duque, G. R. & Ramírez, R. H. Isolated enchondroma of the hand. Long-term follow-up after surgical treatment. Rev. Assoc. Argent Ortop. Traumatol. 82(3), 189–194 (2017).
Lubahn, J. D. & Bachoura, A. Enchondroma of the hand: Evaluation and management. J. Am. Acad. Orthop. Surg. 24(9), 625–633. https://doi.org/10.5435/jaaos-d-15-00452 (2016).
Tordai, P., Hoglund, M. & Lugnegard, H. Is the treatment of enchondroma in the hand by simple curettage a rewarding method?. J. Hand Surg. Br. 15(3), 331–334 (1990).
Lee, J. Y., Lim, J. Y., Oh, J. H. & Ko, Y. M. Cross-cultural adaptation and clinical evaluation of a Korean version of the disabilities of arm, shoulder, and hand outcome questionnaire (K-DASH). J. Shoulder Elbow Surg. 17(4), 570–574. https://doi.org/10.1016/j.jse.2007.12.005 (2008).
Enneking, W. F., Dunham, W., Gebhardt, M. C., Malawar, M. & Pritchard, D. J. A system for the functional evaluation of reconstructive procedures after surgical treatment of tumors of the musculoskeletal system. Clin. Orthop. Relat. Res. 286, 241–246 (1993).
Acknowledgements
Authors thank Linda Lee, MD, Section of Cardiology, at the University of Chicago for providing assistance in editing this manuscript. The authors also wish to acknowledge the financial support of the Korean Musculoskeletal Tissue Transplantation Society research fund made in the program year of 2017 and the Catholic Medical Center Research Foundation made in the program year of 2018.
Author information
Authors and Affiliations
Contributions
H.Y.P. and M.W.J. conceptualized and designed the work. M.W.J., Y.H.C., and C.J.P. collected clinical data. Y.H.C. and C.J.P. developed the methodology and performed collection and analysis on radiologic data. H.Y.P., M.W.J., and Y.G.C. interpreted the data and drafted the work. M.W.J. reviewed and supervise the work. All the authors approved the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Park, H.Y., Joo, M.W., Choi, YH. et al. Simple curettage and allogeneic cancellous bone chip impaction grafting in solitary enchondroma of the short tubular bones of the hand. Sci Rep 13, 2081 (2023). https://doi.org/10.1038/s41598-023-29130-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-29130-w
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
