
Abstract
Handgrip strength is a predictor of functional impairment and presence of morbimortality in older adults. However, appropriate reference values and cutoff points are required for its optimal use. This study describes handgrip characteristics in the older adult population of Antioquia-Colombia and compares the dynapenia handgrip cutoffs proposed for Colombians with international criteria. A cross-sectional study including 1592 older adults was done. Dynapenia prevalence by handgrip was analyzed using the following cutoffs: European Consensus of Sarcopenia (2018), Asian Working Group for Sarcopenia (2019), Chilean (2018), and Colombian (2019). Handgrip strength significantly decreased with aging, showing a positive and strong association with functional and health parameters. The highest prevalence of dynapenia was found with the Asian Consensus cutoffs (26.1%) and the lowest with the Colombian cutoffs (0.8%). Low agreement was found between the Colombian cutoffs with the European Consensus (kappa = 0.059; p < 0.001), the Asian Consensus (kappa = 0.039; p < 0.001) and the Chilean proposal (kappa = 0.053; p < 0.001). Dynapenia using the Chilean, European, and Asian cutoffs was associated with physical inactivity, presence of multimorbidity, slow gait speed, nutritional risk, and low calf circumference. Meanwhile, the Colombian cutoffs was only associated with slow gait speed and low calf circumference. The handgrip cutoffs proposed for Colombians seems to underestimate the dynapenia prevalence in older people from Antioquia. Furthermore, these cutoff points did not show associations with relevant functional and health parameters. The handgrip cutoffs proposed for Colombians should be used with caution.
Similar content being viewed by others

Introduction
Worldwide older adult population has significantly increased in recent years and is expected to continue growing. In 2019, one of nine people in the world was 65 years or older. This proportion is projected to increase to be one out of six by 20501. In 2015, the World Health Organization (WHO) highlighted the need to promote and maintain older adults’ physical and mental capacities2. For achieving this goal, health professionals require simple evaluation methods to measure and monitor the medical-nutritional status of geriatric population. The assessment of muscle strength using manual dynamometry, or handgrip, has a predictive power for cognitive impairment, slow mobility, low functional condition, and mortality in older adults3,4. Likewise, handgrip is used in diagnosing sarcopenia, frailty, and malnutrition5,6,7. For these reasons, manual dynamometry is proposed as a clinical indicator that should be included in medical and nutritional status assessments8,9.
The optimal use of handgrip as a health indicator requires appropriate reference values and cutoff points to classify low grip strength (dynapenia), and it is recommended that these parameters are derived from the very population to be evaluated5,10. The European Consensus for the Definition and Diagnosis of Sarcopenia (EWSOP2) has updated dynapenia cutoffs in 20185. The Asian Working Group for Sarcopenia defined cutoffs for this population group in 201911. In North America, reference values and cutoffs were developed from the National Nutrition and Health Study in 201612. In South America, countries like Chile (2018) and Brazil (2020) have also published reference values13,14. Multicentric studies, including data from Colombia, have proposed cutoffs for older people15,16. Noteworthy is the fact that cutoffs proposed for Colombian population in 2019 are the first borderline values developed using a nationally representative sample with data from the SABE study (Survey on Health, Well-Being, and Aging in Latin America and the Caribbean)17. However, these Colombian cutoffs are twenty percent lower, or even more, than those recommended in Europe5, Asia11, and Chile13. Their application could underestimate the prevalence of sarcopenia since low handgrip strength, according to EWSOP25 is one the first criteria in the diagnostic of this syndrome. The reasons for the low Colombians cutoffs remain unclear, although they may seem to be related with the characteristics of the reference population conditions (e.g., ethnic, social, cultural, or lifestyle) and the statistical method applied for derivation.
Therefore, it is necessary to evaluate the cutoffs proposed for Colombians in 2019 and their association with indicators of multimorbidity and functionality in a Colombian population sample different from the SABE study. Accordingly, the first objective of this study is to describe the handgrip characteristics in older population from Antioquia, Colombia. The second objective is to compare the dynapenia prevalence in this population using the international cutoffs with those originally proposed for Colombians in 201917 and alternative Colombian borderline values corresponding to the 25th percentile of the population described by Ramirez et al.17. The third objective is to analyze the variations in the dynapenia associations with functional and health parameters after applying the above-mentioned cutoffs.
Results
Characteristics of the study population
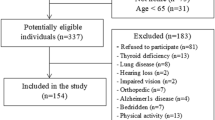
Out of the 1592 older adults evaluated, 59.0% (n = 913) were women. The mean age was 70.1 ± 7.7 years, 70.5 ± 7.8 years in men, and 69.8 ± 7.7 years in women. 89% percent of the participants had up to primary school studies as their maximum educational level (Table 1). The median for body weight was 63.7 kg (IQR: 55.6–72.2), for height 154.5 cms (IQR: 148.6–161.4), for calf circumference 34.6 cms (IQR: 32.5–37.1), and for BMI 26.2 kg/m2 (IQR: 23.4–29.6). Comparatively, men were heavier (men: 66.8 kg, IQR: 59.6–76.4; women: 62.9 IQR: 53.6–71.2; p < 0.001), taller (men:163.0 cms, IQR: 158.3–168.6; women 150.2 cms, IQR: 144.7–154.6; p < 0.001), and had lower body mass index (BMI) (men: 25.4 kg/m2, IQR: 23.1–28.5; women: 27.9 kg/m2, IQR:24.6–31.3; p < 0.001). Men and women presented similar calf circumference median values (34.6 cm for men and 34.5 cm for women; p = 0.046). In women, physical inactivity, multimorbidity, slow gait speed, risk of malnutrition, low calf circumference classification, and excess body weight shown higher percentage (Table 1).
Handgrip and health/functional parameters
Handgrip was higher in apparently healthier older adults (Table 1). Handgrip was higher (p < 0.05) among active people, with gait speed ≥ 0.8 m/s, calf circumference ≥ 31 cms, adequate BMI, and without multimorbidities or nutritional risk. These results were similar in men and women, except for the BMI classification in men, in which those with excess body weight showed the highest handgrip value (Table 1).
Differences in dynapenia prevalence were found using the cutoff points of interest (Table 2). The highest prevalence was found with the Asian Consensus (26.1%) and the lowest prevalence with the original Colombian cutoffs (0.8%). Tables 2 and 3 show the associations between health status, functionality parameters, and anthropometric characteristics with dynapenia classifications. Dynapenia classifications using the Chilean, the European, the Asian and the 25th percentile as alternative Colombian borderline cutoffs showed associations with physical inactivity, presence of multimorbidity, slow gait speed, nutritional risk, and low calf circumference. Meanwhile, dynapenia classification with the original Colombian cutoffs was associated with slow gait speed and low calf circumference variables.
Concordance and agreement of handgrip cutoff points
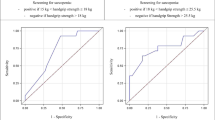
The concordance and agreement between cutoffs for dynapenia classification are shown in Table 4 and Fig. 1. The highest concordance was found between the European Consensus and the Chilean proposal (k = 0.943; p < 0.001); the black squares fill almost the entire area of the diagonal rectangles (Fig. 1a). The diagonal line crossing smoothly through the vertex of the rectangles (Fig. 1a) evinces symmetry (minimal bias) between dynapenia classifications using the European Consensus and the Chilean proposal. When dynapenia classification was done using the 25th percentile for alternative borderline values, fair agreements were found with the European Consensus (k = 0.382; p < 0.001), the Asian Consensus (k = 0.268; p < 0.001) and the Chilean proposal (k = 0.348; p < 0.001). The black squares fill a halfway area of the diagonal rectangles (Fig. 1d–f). Slight agreements were found between the original Colombian cutoffs with the European Consensus (k = 0.059; p < 0.001), the Asian Consensus (k = 0.039; p < 0.001) and the Chilean proposal (k = 0.053; p < 0.001); the black squares fill a small area of the agreement cell for dynapenia (upright diagonal rectangles in Fig. 1g–i). Sex disaggregated analysis showed kappa results similar to those using the aggregate population (Supplementary Table S1 online).

Agreement plot of dynapenia between different cutoff points. European consensus EWGSOP2 2018: European Working Group on Sarcopenia in Older People update in 20185. Asian consensus 201911. Chileans 2018: Reference values of handgrip dynamometry in older Chileans13. Original Colombian cutoffs 2019: reference cutoffs for handgrip strength among older adults17. Alternative Colombian borderlines2019 (< p25): values lower than the 25-percentile taken from Ramirez-Velez et al.17. K: Cohen’s Kappa Coefficient. McNemar: McNemar test. < p25: Values below 25 percentile.
Discussion
The first objective of this study was to describe handgrip characteristics in the older population from Antioquia, Colombia. In this population, handgrip strength significantly decreases with aging, in both men and women. Handgrip strength has shown a positive and strong association with functional and health parameters. These findings corroborate the potential value of manual dynamometry in medical and nutritional assessments of older population. In relation to the second objective, dynapenia prevalence was below 1% when applying the original Colombian cutoffs17. The prevalence increased up to 5.5% using the alternative Colombian borderline values. While applying the international criteria, prevalence was around 20%. Regarding the third objective, dynapenia classification using the cutoffs proposed for Colombians did not show any significant association with physical inactivity, presence of multimorbidity, or malnutrition risk. This suggests that the handgrip cutoff points proposed for Colombians seems to underestimate the prevalence of dynapenia in the older population of Antioquia.
Handgrip strength was higher in subjects that were physically active, morbidity free, and free of malnutrition risk, which is in line with previous studies18,19,20,21. Likewise, older adults with adequate handgrip strength showed normal gait speed, thus supporting this measurement's utility to identify older people with locomotion impairments22,23. These results endorse handgrip strength as a screening and monitoring tool for nutrition and health status in older population3,4,8.
Using the original cutoff points proposed for Colombians, the prevalence of dynapenia in the older population of Antioquia was rather low (0.8%); this percentage shows a slight agreement with the international criteria (kappa < 0.06). Probably, the prevalence of dynapenia is higher in Antioquia´s population, as it is suggested by the international cutoff points (between 18.4 and 26.1%) and the health conditions found of multimorbidity (45.9%), risk of malnutrition (36.2%), physical inactivity (36.7%) and slow gait speed (45.0%). Accordingly, the application of the original Colombian cutoffs seem to underestimate the prevalence of sarcopenia, frailty, and malnutrition in this population, which may delay the treatments of these conditions, and then affecting the general wellbeing of the older adult Colombian population.
The low performance of the original handgrip cutoffs proposed for Colombians is probably due to several factors. One factor might relate to the sociodemographic characteristics of the population used for deriving the cutoff points. However, the Colombian older population was similar in terms of age, gender, and educational levels as to the population from Chile, and other developing countries of South America wherein cutoffs were higher13,14. Therefore, the methodology used to derive the cutoffs may have played a major role. The proposed handgrip cutoff points were derived from the SABE-Colombia study, which included population aged between 60 and 10817. Since handgrip strength decreases with aging and its reduction is related to functional impairment, considering older adults as reference population to derive cutoff points may be inappropriate. EWGSOP2 cutoffs for dynapenia, proposed in 2019 (< 27 kg for men and < 16 kg for women), were derived from British adult population5. These cutoff points correspond to a < 2.5 T-score value of the maximum handgrip strength found in adult men (29–39 years old) and women (26–42 years old)5. Cutoff points for the older population developed in adults have shown to be helpful in monitoring health parameters like bone mass density24.
Using values below one standard deviation for establishing cutoff points could be another factor that contributed to the low performance of the original handgrip thresholds proposed for Colombians. One standard deviation is close to 15th and 16th percentiles on a normal sample distribution, and this could be a low value for handgrip cutoff points in older people. Lera et al.13, using a sample of older adult Chilean population, established handgrip cutoffs using the 25th percentile. Lera’s thresholds seem to be more appropriate for the older population of Antioquia, as shown in the results of this study. Similarly, the Asian handgrip cutoff points11, developed with older population using the 20th percentile, showed results in accordance with the multimorbidity states and functionality status found in the population of Antioquia.
The alternative Colombian borderlines yielded higher dynapenia prevalence (5.5%) than the cutoffs originally proposed for Colombians in 2019 (0.8%). Dynapenia classification with the alternative Colombian borderlines showed additional associations with physical inactivity, presence of multimorbidity, and nutritional risk evaluated by MNA; such associations were missing when the cutoff points proposed for Colombians were used. From a clinical viewpoint, the application of the alternative Colombian borderlines appears to be more reasonable for diagnosing dynapenia in older people from Antioquia. However, these borderline values generate lower dynapenia prevalence than the international criteria. Therefore, it seems reasonable to continue using the international handgrip cutoff points, especially when using manual dynamometry in health promotion and disease prevention among older population of Antioquia.
A strength of this study was its representative sample of older people from Antioquia, which included people from urban and rural areas. Moreover, this study used a handgrip device and measurement protocol resembling the Colombian SABE survey. One limitation of this study is its cross-sectional design that limits establishing causal conclusions. However, the analysis in this study does not claim this type of association. Rather, the analysis focuses on reporting the characteristics of handgrip strength and the concordance between the different classifications for dynapenia.
Conclusions
Handgrip strength was higher in men than women, in youngest-old people (60–64 years), in those with normal nutritional status, lacking multimorbidity, and presenting optimal functional indicators. This study found low concordance between the original handgrip cutoffs proposed for Colombians regarding other international criteria. Moreover, the Colombian thresholds did not show any significant associations with physical inactivity, presence of multimorbidity or malnutrition risk. The handgrip cutoffs proposed for Colombians should be used with caution.
Methods
This is a cross-sectional study derived from the survey Food and Nutritional Profile of Households in Antioquia, 2019 (which stands in Spanish for “Perfil Alimentario y Nutricional de los Hogares de Antioquia, 2019”). Antioquia is the second largest department in Colombia and has over six million inhabitants. The Government of Antioquia and the School of Nutrition and Dietetics from the University of Antioquia carried out the survey with strict quality control processes for data collection25. Households were selected using a probabilistic, stratified, and multi-stage sampling design. All adults 60 years and older dwelling in the selected households were included in the study. A total of 1592 older people participated in the study, making up a representative sample for residential area (urban–rural). People with physical or mental limitations were excluded from the analysis due to limitations to collect anthropometric and handgrip measurements. The study followed the Helsinki Declaration guidelines. The measurement protocols were approved by the Ethics Committee from Universidad de Antioquia’s Faculty of Medicine (Act number 12, August 23, 2018). Participants voluntarily manifested their consent to participate in the study and signed an informed consent letter.
Trained and standardized health staff performed anthropometric and physical activity measurements. Body weight was measured with an electronic scale (Seca 878, California, United States of America), height with a portable stadiometer (Seca 213, California, United States of America), and calf circumference with a metal tape (Lufkin W6006ME, Texas, United States of America). Each measurement was made twice. A third measurement was done when a difference between measurements was greater than 0.1 kg in body weight, 0.5 cm (cms) in height, or 0.2 cms in calf. Calf circumference values below 31.0 cms were considered low26. Handgrip strength was measured twice in each hand using a digital dynamometer (Takei 5401, Tokyo, Japan). A third measurement was performed when a difference ≥ 10% was found between the first and the second measurements. The highest measurement of both hands was used as the maximum handgrip since this value is probably less affected by the number of trials than the average of the measurements27.
National and international handgrip cutoffs were used to classify dynapenia (Table 5). The analysis included the cutoffs of the European consensus EWGSOP2 20185, the Asian 2019 consensus11, the Chilean 2018 proposal13, the Original Colombian 2019 cutoffs17 and alternative Colombian borderline values corresponding to the 25th percentile of the population described by Ramirez et al.17. This analysis was included by the authors while reviewing alternative borderline values in contrast to the original proposed for Colombians.
Gait speed was assessed in a five-meter walk on a flat surface. In the first meter, the participants assessed were allowed to reach a regular walking pace, and in the last meter, the participants were allowed to slow down. The walking time from the beginning of the second meter up to the end of the fourth meter was recorded with a digital stopwatch28,29. When the speed was below 0.8 m per second, the participant was classified with a slow gait speed30.
Face-to-face interviews were used to collect data on sociodemographic variables, health conditions, and physical activity. The Advanced Activities of Daily Living scale by Reuben et al. was used to classify people as active and inactive31. The Mini Nutritional Assessment was applied to classify people with malnutrition (< 17 points), at risk of malnutrition (17–23.5 points), or under normal nutritional status (≥ 24 points)26. Risk of malnutrition and malnutrition categories were combined due to the low frequency of malnutrition (n = 34). Likewise, BMI was calculated, and the older people were classified using the Pan American Health Organization cutoffs for underweight, normal weight, overweight, and obesity32. Information about the participants’ diagnostic diseases was obtained by a physician and registered using the most prevalent list. Suffering two or more medical conditions/diseases was classified as multimorbidity, following the WHO guidelines33.
The statistical analysis was done using SPSS software version 25 (Chicago: SPSS Inc.; Ill). The quantitative variables were checked for normal distribution using the Kolmogorov–Smirnov test. These variables are described with median and interquartile range (IQR). According to the data distribution, the Mann–Whitney U or Kruskal–Wallis tests were used for comparing handgrip values with demographic, anthropometric, physical activity, and health status variables. Multiple comparisons among groups were done using Dunn´s post-hoc test. Categorical variables are presented as frequencies and percentages. The maximum likelihood test was used to determine their association with the dynapenia classifications. McNemar’s test was used to compare the results of the dynapenia classifications. Cohen’s Kappa coefficient was used to assess concordance between them. Kappa coefficients were interpreted using Landis and Koch; κ values (a) above 0.80 indicated an almost perfect agreement, (b) from 0.61 up to 0.80 indicated substantial agreement, (c) from 0.41 up to 0.60 indicated moderate agreement, (d) from 0.21 up to 0.40 indicated fair agreement, and (e) between 0.00 and 0.20 indicated a slight agreement34. Bangdiwala charts were built to visualize agreement analysis of the dynapenia classifications using a vcd package in R35. A perfect agreement is determined when the black squares and the rectangular boxes of the diagonal chart have the same size. The disagreement increases as the black square's size decreases compared to the cells' rectangular area. Bias increases positively or negatively in accordance with the vertex line connecting the rectangles, when pointing up or down the diagonal. A full explanation of Bangdiwala’s agreement chart can be found somewhere else36. P-values < 0.05 were considered as significant.
Data availability
The data that support the findings of this study are available from Gobernación de Antioquia-Colombia (Gerencia de Seguridad Alimentaria y Nutricional office), but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of Gobernación de Antioquia-Colombia (Gerencia de Seguridad Alimentaria y Nutricional office).
References
United Nations, Department of Economic and Social Affairs, Population Division (2019). World Population Ageing 2019: Highlights (ST/ESA/SER.A/430).
World Health Organization. World report on ageing and health. World Health Organization. https://apps.who.int/iris/handle/10665/186463.
Rijk, J. M., Roos, P. R., Deckx, L., van den Akker, M. & Buntinx, F. Prognostic value of handgrip strength in people aged 60 years and older: A systematic review and meta-analysis. Geriatr. Gerontol. Int. 16(1), 5–20. https://doi.org/10.1111/ggi.12508 (2016).
Bohannon, R. W. Grip strength: An indispensable biomarker for older adults. Clin. Interv. Aging 14, 1681–1691. https://doi.org/10.2147/CIA.S194543 (2019).
Cruz-Jentoft, A. J. et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Age. 48(1), 16–31. https://doi.org/10.1093/ageing/afy169 (2019).
Jensen, G. L. et al. GLIM criteria for the diagnosis of malnutrition: A consensus report from the global clinical nutrition community. JPEN J. Parenter Enteral. Nutr. 43(1), 32–40. https://doi.org/10.1002/jpen.1440 (2019).
Fried, L. P. et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. Ser A 56(3), M146–M157. https://doi.org/10.1093/gerona/56.3.M146 (2001).
Susan, J. W. et al. Hand grip strength as a potential nutritional assessment tool in long-term care homes. J. Aging Res. Healthc. 1(2), 1–11. https://doi.org/10.14302/issn.2474-7785.jarh-16-1177 (2016).
Bohannon, R. W. Muscle strength: Clinical and prognostic value of handgrip dynamometry. Curr. Opin. Clin. Nutr. Metab. Care 18(5), 465–470 (2015).
Dodds, R. M. et al. Global variation in grip strength: A systematic review and meta-analysis of normative data. Age Age. 45(2), 209–216. https://doi.org/10.1093/ageing/afv192 (2016).
Chen, L. K. et al. Asian working Group for Sarcopenia: 2019 consensus update on Sarcopenia diagnosis and treatment. J. Am. Med. Dir. Assoc. 21(3), 300-307.e2. https://doi.org/10.1016/j.jamda.2019.12.012 (2020).
Perna, F. M. et al. Muscular grip strength estimates of the U.S. population from the national health and nutrition examination survey 2011–2012. J. Strength Cond. Res. 30(3), 867 (2016).
Lera, L. et al. Reference values of handgrip dynamometry and the relationship between low strength and mortality in older Chileans. Clin. Interv. Aging. 13, 317–324. https://doi.org/10.2147/cia.s152946 (2018).
Fernandes, S. G. G. et al. Cut-off points to screening for sarcopenia in community-dwelling older people residents in Brazil. PeerJ 9, 12038. https://doi.org/10.7717/peerj.12038 (2021).
de Souza Barbosa, J. F. et al. Clinically relevant weakness in diverse populations of older adults participating in the International Mobility in Aging Study. Age (Dordr). 38(1), 25. https://doi.org/10.1007/s11357-016-9888-z (2016).
Leong, D. P. et al. Reference ranges of handgrip strength from 125,462 healthy adults in 21 countries: a prospective urban rural epidemiologic (PURE) study. J. Cachexia Sarcopenia Muscle. 7(5), 535–546. https://doi.org/10.1002/jcsm.12112 (2016).
Ramírez-Vélez, R., Correa-Bautista, J. E., García-Hermoso, A., Cano, C. A. & Izquierdo, M. Reference values for handgrip strength and their association with intrinsic capacity domains among older adults. J. Cachexia Sarcopenia Muscle. 10(2), 278–286. https://doi.org/10.1002/jcsm.12373 (2019).
Bilajac, L. et al. The influence of physical Activity on handgrip strength of elderly. Arch. Gerontol. Geriatr. Res. 4(1), 020–024. https://doi.org/10.17352/aggr.000011 (2019).
Montes, M. C. et al. Strength and multimorbidity among community-dwelling elderly from southern Brazil. Nutrition 71, 110636. https://doi.org/10.1016/j.nut.2019.110636 (2020).
Volaklis, K. A. et al. Handgrip strength is inversely and independently associated with multimorbidity among older women: Results from the KORA-Age study. Eur. J. Intern. Med. 31, 35–40. https://doi.org/10.1016/j.ejim.2016.04.001 (2016).
Akbar, F. & Setiati, S. Correlation between hand grip strength and nutritional status in elderly patients. J. Phys. Conf. Ser. 1073, 042032 (2018).
Lin, Y.-H., Chen, H.-C., Hsu, N.-W. & Chou, P. Using hand grip strength to detect slow walking speed in older adults: the Yilan study. BMC Geriatr. 21(1), 428. https://doi.org/10.1186/s12877-021-02361-0 (2021).
Arokiasamy, P., Selvamani, Y., Jotheeswaran, A. T. & Sadana, R. Socioeconomic differences in handgrip strength and its association with measures of intrinsic capacity among older adults in six middle-income countries. Sci. Rep. 11(1), 19494. https://doi.org/10.1038/s41598-021-99047-9 (2021).
Kanis, J. A. et al. A reference standard for the description of osteoporosis. Bone 42(3), 467–475. https://doi.org/10.1016/j.bone.2007.11.001 (2008).
PANA: Perfil Alimentario y Nutricional de de los Hogares de Antioquia 2019 [Internet]. Medellin, Colombia: Escuela de Nutricion y Dietetica, Universidad de Antioquia. Gobernacion de Antioquia. [cited 2020 April 12]. http://cia.corantioquia.gov.co/cgi-bin/koha/opac-detail.pl?biblionumber=11112.
Vellas, B. et al. The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients. Nutrition 15(2), 116–122. https://doi.org/10.1016/s0899-9007(98)00171-3 (1999).
Roberts, H. C. et al. A review of the measurement of grip strength in clinical and epidemiological studies: Towards a standardised approach. Age Age. 40(4), 423–429. https://doi.org/10.1093/ageing/afr051 (2011).
Ávila-Funes, J. A., Gray-Donald, K. & Payette, H. Medición de las capacidades físicas de adultos mayores de Quebec: Un análisis secundario del estudio NuAge. Salud Pública de México 48, 446–454 (2006).
Guralnik, J. M. et al. A short physical performance battery assessing lower extremity function: Association with self-reported disability and prediction of mortality and nursing home admission. J. Gerontol. 49(2), M85-94. https://doi.org/10.1093/geronj/49.2.m85 (1994).
Cruz-Jentoft, A. J. et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Age. 39(4), 412–423. https://doi.org/10.1093/ageing/afq034 (2010).
Reuben, D. B., Laliberte, L., Hiris, J. & Mor, V. A hierarchical exercise scale to measure function at the Advanced Activities of Daily Living (AADL) level. J. Am. Geriatr. Soc. 38(8), 855–861. https://doi.org/10.1111/j.1532-5415.1990.tb05699.x (1990).
Organización Panamericana de la Salud; Guía Clínica para Atención Primaria a las Personas Adultas Mayores. Módulo 5. Valoración Nutricional del Adulto Mayor. Washington, D.C: OPS; 2002.
Multimorbidity: Technical Series on Safer Primary Care. Geneva: World Health Organization; 2016. Licence: CC BY-NC-SA 3.0 IGO.
Landis, J. R. & Koch, G. G. The measurement of observer agreement for categorical data. Biometrics 33(1), 159–174 (1977).
Meyer D, Zeileis A, Hornik K. vcd: Visualizing Categorical Data: R package version 1.4–4; 2017.
Bangdiwala, S. I. & Shankar, V. The agreement chart. BMC Med. Res. Methodol. 13(1), 97. https://doi.org/10.1186/1471-2288-13-97 (2013).
Acknowledgements
The authors thank the participants and their families for providing information to the survey Food and Nutritional Profile of Households in Antioquia, 2019. We also thank the School of Nutrition and Dietetics from Universidad de Antioquia and the Office of Food and Nutrition Security (in Spanish: Gerencia de Seguridad Alimentaria y Nutricional: MANÁ) from Gobernación de Antioquia.
Funding
This study was funded by The Office of Food and Nutrition Security (in Spanish: Gerencia de Seguridad Alimentaria y Nutricional: MANÁ) from Gobernación de Antioquia, and the School of Nutrition and Dietetics from Universidad de Antioquia.
Author information
Authors and Affiliations
Contributions
F.A.P., A.E.R., and J.A. contributed equally to this work.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Patiño-Villada, F.A., Estrada-Restrepo, A. & Aristizábal, J. Handgrip strength in older adults from Antioquia-Colombia and comparison of cutoff points for dynapenia. Sci Rep 13, 1718 (2023). https://doi.org/10.1038/s41598-023-28898-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-28898-1
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
