
Abstract
Although computer vision syndromes are becoming a major public health concern, less emphasis is given to them, particularly in developing countries. There are primary studies on different continents; however, there are inconsistent findings in prevalence among the primary studies. Therefore, this systematic review and meta-analysis aimed to estimate the pooled prevalence of computer vision syndrome. In this study, the review was developed using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. Online electronic databases, including PubMed/Medline, CINAHL, and Google Scholar, were used to retrieve published and unpublished studies. The study was conducted from December 1 to April 9/2022. Study selection, quality assessment, and data extraction were performed independently by two authors. Quality assessment of the studies was performed using the Joanna Briggs Institute Meta-Analysis of Statistics Assessment and Review Instrument tool. Heterogeneity was assessed using the statistical test I2. STATA 14 software was used for statistical analysis. A total of 7,35 studies were retrieved, and 45 studies were included in the final meta-analysis. The pooled prevalence of computer vision syndrome was 66% (95% CI: 59, 74). Subgroup analysis based on country was highest in Pakistan (97%, 95% CI: 96, 98) and lowest in Japan (12%, 95% CI: 9, 15). Subgroup analysis based on country showed that studies in Saudi Arabia (I2 = 99.41%, p value < 0.001), Ethiopia (I2 = 72.6%, p value < 0.001), and India (I2 = 98.04%, p value < 0.001) had significant heterogeneity. In the sensitivity analysis, no single study unduly influenced the overall effect estimate. Nearly two in three participants had computer vision syndrome. Thus, preventive practice strategic activities for computer vision syndrome are important interventions.
Similar content being viewed by others

Introduction
Computer vision syndrome (CVS) is defined as “a complex of eye and vision problems related to near work experienced during computer use”1. Visual fatigue (VF) and digital eye strain (DES) terms are also used for CVS, reflecting the different digital devices related to potential health problems2. Symptoms related to CVS can be classified as visual, ocular, and extraocular symptoms3. Visual symptoms include blurred vision, visual fatigue or discomfort, and diplopia4,5,6,7. Ocular symptoms include dry eye disease, redness, eye strain, and irritation1,8,9. Extraocular symptoms include headache and shoulder, neck, and back pain3,4,10,11,12,13,14.
Individuals spend more time on electronic devices such as computers, laptops, smartphones, tablets, and e-readers, which contribute to CVS15. Children are also affected in CVS, as they spend many hours using electronic devices for schoolwork, playing video games, and sending and receiving text messages15. However, the use of these devices even for 3 h/day can lead to the development of CVS3.
The massive growth of digital devices has become an integral part of daily life, and millions of individuals of all ages are at risk of CVS16,17,18. In developed nations, engagement with digital devices has increased substantially in recent years across all age groups19,20,21,22. Moreover, digital device use has increased in developing countries, resulting in a high burden of CVS due to low accessibility, low utilization of personal protective equipment, and limited break time while using electronic devices. CVS is a major public health problem leading to occupational hazard, an increased error rate, impaired visual abilities, reduced productivity, and low job satisfaction23,24.
A review of the literature showed that factors associated with CVS can be classified as personal factors, which include poor sitting position, inappropriate eye-to-screen distance, insufficient working procedures, improper viewing angle and distances, age, medical diseases, and long duration of computer usage. The environment and computer factors such as improper workstations, poor lighting, contrast, and resolution rooms, slow refresh rate, glare of the display, excessive screen brightness, and imbalance of light between the computer screen and surrounding working room5,10,25,26,27,28.
Modern digital technology markedly influences the daily activities and lifestyles of people4,7. CVS has an effect on reduced productivity and visual and musculoskeletal impairment and a negative impact on cadiac rhythms and sleep patterns4,7,13,29,30. Although CVS is becoming a major public health problem, less emphasis is given, particularly in developing countries. There are primary studies on different continents; however, there are inconsistent findings in prevalence among the primary studies. Therefore, this systematic review aimed to estimate the pooled prevalence of computer vision syndrome.
Methods
Protocol and registration
This systematic review and meta-analysis was registered on PROSPERO with registration number CRD42022325167. Available at: https://www.crd.york.ac.uk/prospero/#myprospero.
Search strategies
The systematic review was developed using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines31, and the review procedure was reported using the PRISMA-P 2009 checklist32 (supplementary file 1). Published and unpublished studies were searched in databases such as Medline/PubMed, CINAHL, and Google Scholar from December 1 to April 9/2022. MeSH terms and entry terms were used to search studies from databases, and modifications were made based on the type of database (supplementary file 2).
Eligibility criteria
Inclusion criteria
-
The following criteria were considered to include studies:
Study area.
-
Anywhere
Study scope.
-
Studies that report the prevalence of CVS and its associated factors
-
Studies that report the prevalence of CVS
-
“Both community- and facility-based studies”
-
Quantitative results, if the study reported both qualitative and quantitative results
Study design.
-
Observational study designs, including cross-sectional and cohort study designs
Language.
-
English
Population.
-
All population groups
Publication year.
-
No restriction
Exclusion criteria
Studies were excluded if:
-
Other than English
-
Studies that did not report specific outcomes (prevalence) of CVS
-
No full-text article following email contact to the corresponding authors
-
Qualitative studies
-
Letters, conference abstracts, case reports, and reviews,
CoCoPop/PEO
Condition: computer vision syndrome.
Context: worldwide.
Population: All population groups.
Outcome/context: The primary outcome of the study was the pooled prevalence of CVS. The prevalence of CVS was considered when the studies reported the overall prevalence of CVS or either of CVS syndromes (blurred vision, eye strain/fatigue, discomfort, diplopia, dry eye disease, redness, irritation, headache, shoulder, neck, and back pain) in the primary studies.
Study selection
Endnote reference manager software33 was used to organize and remove duplicates, irrelevant titles, and abstracts. Duplicate studies were removed. An assessment of studies using the title and abstract was performed, and irrelevant titles and abstracts were removed. Study selection was performed independently by two reviewers (EW and AK). The selection procedures of the studies were presented using a PRISMA diagram.
Quality assessment
A full-text review of studies was performed before the inclusion of studies in the final meta-analysis using “The Joanna Briggs Institute Meta-Analysis of Statistics Assessment and Review Instrument (JBI-MAStARI)”34 quality appraisal tool. The components of quality assessment include study setting, outcome and explanatory variable measurements, clear inclusion criteria, measurement criteria used, participants’ description, and valid statistical analysis. Independent quality assessment of the studies was reviewed by EW and AK, and studies with a quality score of 50% and above were included in the final systematic review and meta-analysis. Disagreement during quality assessment among reviewers was resolved with discussion. In addition, cross-referencing of the included articles was performed.
Data extraction
Independent data extraction was performed by the authors (EW and AK) using a pilot-tested data extraction Microsoft Office Excel sheet. The data extraction sheet elements included publication year, authors’ names, study design, country, sample size, response rate, prevalence and study subjects. Discrepancies were resolved by discussion between the authors (EW and AK). Contact with the corresponding authors of the studies was made for incomplete data, and the study was excluded if there was no response.
Data analysis
The extracted Excel data were imported into STATA version 14 for analysis. A narrative description and summary characteristics of the included studies were reported in tables and graphs. A random-effects model meta-analysis35 was used to estimate the overall effect size, and the results were presented using a forest plot.
The heterogeneity of studies was assessed by the I2 statistic36. I2 statistics of 25, 50 and 75% showed low, moderate and high heterogeneity, respectively, with p < 0.05. Publication bias was assessed using visual observation of the funnel plot37 and Egger’s test at p < 0.0538. To identify the sources of heterogeneity among the studies, subgroup analysis and meta-regression39 were performed based on country and sample size. Moreover, sensitivity analysis was performed to assess the effect of the study on the overall effect size.
Results
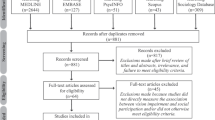
A total of 735 articles were retrieved using electronic database searches: PubMed, Google Scholar, and CINHAL. Seventy-seven articles were excluded due to duplication, and 559 articles were excluded because they were not related to the title and abstract. Ninety-nine full-text articles were assessed for quality eligibility, and 57 articles were excluded based on the quality appraisal tool because they were irrelevant, had no full text available, or were duplicates. Three articles were identified through a cross-reference search of the included studies. Finally, 45 articles were included in the systematic review and meta-analysis (Fig. 1).

PRISMA flow diagram studies screening, and selection on computer vision syndrome, 2022.
Characteristics of the included studies
A total of 45 cross-sectional studies with 17,526 sample sizes were included in this systematic review and meta-analysis: four studies in Saudi Arabia40,41,42,43, two studies in Nigeria44,45, three studies in Ghana46,47,48, four studies in Pakistan49,50,51,52, three studies in Spain53,54,55, seven studies in Ethiopia56,57,58,59,60,61,62, one study in Jordan63, two studies in China64,65, one study in Iran66, three studies in Egypt67,68,69, eight studies in India18,70,71,72,73,74,75,76, one study in Nepal77, one study in Sri Lanka29, two studies in Brazil78,79, one study in Beirut80, one study in Japan81, and one study in Thailand82. The sample size ranged from 74 in China64 to 2210 in Sri Lanka29 (Table 1).
Pooled prevalence of computer vision syndrome
The pooled prevalence of computer vision syndrome was 66% (95% CI: 59, 74). The lowest proportion included study was in Japan, 12% (95% CI: 9, 15)81, and the highest was in Pakistan, 99% (95% CI: 97, 100) 52. The I2 test showed that there was heterogeneity among the included studies (I2 = 99.42%, p value < 0.001) (Fig. 2).

Forest plot showing the pooled prevalence of computer vision syndrome, 2022.
Subgroup analysis by country
Subgroup analysis was performed based on country, and the prevalence of computer vision syndrome was highest in Pakistan (97%, 95% CI: 96, 98) and lowest in Japan (12%, 95% CI: 9, 15). The studies that showed significant heterogeneity were studies in Saudi Arabia (I2 = 99.41%, p value < 0.001), Ethiopia (I2 = 72.6%, p value < 0.001), Egypt (I2 = 80.06%, p value < 0.001), and India (I2 = 98.04%, p value < 0.001) (Table 2).
Meta regression
Meta-regression was performed to identify the source of heterogeneity across the studies by country and sample size. Meta-regression indicated that heterogeneity was not associated with country or sample size (p value > 0.05) (Supplementary file 3 Table S1).
Publication biases
Publication bias was checked using dot plots, and visual inspection suggested asymmetry (Supplementary file 4: Figure S1).Moreover, publication bias was not shown by Egger’s test (p = 0.21) (Supplementary file 5 Table S2).
Sensitivity analysis
The sensitivity analysis was performed, and no single study unduly influenced the overall effect estimate of CVS (Supplementary file 6 Table S3).
Discussion
This systematic review and meta-analysis aimed to assess the pooled prevalence of computer vision syndrome. Although there are primary studies conducted on CVS, there are inconsistent findings on prevalence results. Moreover, there are no systematic reviews and meta-analyses on the pooled prevalence of computer vision syndrome. Therefore, findings from this systematic review and meta-analysis will help policy-makers design appropriate strategies to reduce computer vision syndrome-related public health concerns.
The pooled prevalence of computer vision syndrome was 66% (95% CI: 59, 73). The pooled prevalence was in line with the study done in India COVID-19 pre lockdown, 64.3%86. However, the pooled prevalence was lower than that in studies performed in India during the COVID-19 lockdown, 87.3%86, Europe, 90%87, and Ethiopia, 73.21%88. The difference might be due to differences in study period, study setting, socioeconomic differences, awareness and behavioral change in the prevention of computer vision syndrome. Moreover, the precision of the diagnostic instruments used to record the prevalence of CVS may be the cause of a wide range of variations. Whether through direct or online surveys, the majority of papers used purely subjective questions. As most surveys rely solely on the existence of one or more CVS complaints to diagnose CVS without connecting these complaints to the time of screen use and the long-term frequency of these complaints for months, studies may exaggerate the true prevalence of CVS11,89. Additionally, the disparity may be caused by how people use screens, particularly smartphones, or screen abuse, such as poor lighting, uncomfortable seating positions, close eye-screen distance, improper visualization gaze, uncorrected refractive errors, prolonged continuous screen hours, a lack of breaks, viewing screens in the dark, and poor screen design.
This study has the following limitations: articles published only in English were included, and it was difficult to determine the cause-effect relationship, as all the studies were cross-sectional designs. Additional database searches, such as Science Direct, Web of Science, ProQuest, Scopus, EMBASE, etc., we’re not performed due to the lack of free access and we recommend funding to expand database searches. Moreover, this study was reported from 20 countries, which might lack representativeness.
Conclusion
Nearly two in three participants had computer vision syndrome. Thus, preventive practice strategic activities for computer vision syndrome are important interventions.
Data availability
All data are included in this manuscript and its supplementary information files.
References
Association, A. O. The Effects of Computer Use on Eye Health and Vision (American Optometric Association, 1997).
Rosenfield, M. Computer vision syndrome (aka digital eye strain). Optometry in practice 17(1), 1–10 (2016).
Association, AO, Guide to the clinical aspects of computer vision syndrome. St. Louis: American Optometric Association, 1995. 1.
Ahmed, S. F. et al. Visual function, digital behavior and the vision performance index. Clin. Ophthalmol. 12, 2553 (2018).
Klamm, J. & Tarnow, K. G. Computer vision syndrome: A review of literature. Medsurg Nurs. 24(2), 89 (2015).
Munshi, S. et al. Computer vision syndrome—A common cause of unexplained visual symptoms in the modern era. Int. J. Clin. Pract. 71(7), e12962 (2017).
Vaz, F. T. et al. Digital asthenopia: Portuguese group of ergophthalmology survey. Acta Med. Port. 32(4), 260–265 (2019).
Akkaya, S. et al. Effects of long-term computer use on eye dryness. North. Clin. Istanb. 5(4), 319 (2018).
Billones, R. K. C., Bedruz R. A. R., et al. Digital eye strain and fatigue recognition using electrooculogram signals and ultrasonic distance measurements. In 2018 IEEE 10th International conference on humanoid, nanotechnology, information technology, communication and control, environment and management (HNICEM). 2018. IEEE.
Chawla, A. et al. Computer vision syndrome: Darkness under the shadow of light. Can. Assoc. Radiol. J. 70(1), 5–9 (2019).
Iqbal, M. et al. Computer vision syndrome prevalence and ocular sequelae among medical students a university-wide study on a marginalized visual security issue. Open Ophthalmol. J. 15(1), 156–170 (2021).
Leung, T. W. et al. Blue-light filtering spectacle lenses: Optical and clinical performances. PLoS ONE 12(1), 0169114 (2017).
Stringham, J. M. et al. Macular carotenoid supplementation improves visual performance, sleep quality, and adverse physical symptoms in those with high screen time exposure. Foods 6(7), 47 (2017).
Touitou, Y. et al. Disruption of adolescents’ circadian clock: The vicious circle of media use, exposure to light at night, sleep loss and risk behaviors. J. Physiol.-Paris 110(4), 467–479 (2016).
Heiting, G, Wan, L, Computer vision syndrome and computer glasses: FAQ. All About Vision. 2017.
LAKACHEW, N, 2015 Prevalence and Associated Factors of Computer Vision Syndrome among Bank Workers in Gondar City, Northwest Ethiopia, 2015.
Mani, K, Ergonomics education for office computer workers: An evidence-based strategy. Anatomy, Posture, Prevalence, Pain, Treatment and Interventions of Musculoskeletal Disorders, 2018.
Singh, H. et al. Prevention of ocular morbidity among medical students by prevalence assessment of asthenopia and its risk factors. J. Evid. Based Med. Healthcare 3(15), 532–536 (2016).
Council, V, Eyes overexposed: The digital device dilemma. 2016.
Mastrota, K. M. As seen on TV: Doing harm, not help, to the ocular surface. Optometry Times 11(9), 30–32 (2019).
Palaiologou, I. Children under five and digital technologies: Implications for early years pedagogy. Eur. Early Child. Educ. Res. J. 24(1), 5–24 (2016).
Tadesse, S. et al. Utilization of personal protective equipment and associated factors among textile factory workers at Hawassa Town, Southern Ethiopia. J. Occup. Med. Toxicol. 11(1), 1–6 (2016).
Charpe, N. A. & Kaushik, V. Computer vision syndrome (CVS): Recognition and control in software professionals. J. Hum. Ecol. 28(1), 67–69 (2009).
Wimalasundera, S, Computer vision syndrome. Galle Med. J., 2009. 11(1).
Agarwal, S. et al. Evaluation of the factors which contribute to the ocular complaints in computer users. J. Clin. Diagnostic Res.: JCDR 7(2), 331 (2013).
Gowrisankaran, S. & Sheedy, J. E. Computer vision syndrome: A review. Work 52(2), 303–314 (2015).
Long, J. et al. Viewing distance and eyestrain symptoms with prolonged viewing of smartphones. Clin. Exp. Optom. 100(2), 133–137 (2017).
Millodot, M. Dictionary of Optometry and Visual Science E-Book (Elsevier Health Sciences, 2014).
Ranasinghe, P. et al. Computer vision syndrome among computer office workers in a developing country: An evaluation of prevalence and risk factors. BMC. Res. Notes 9(1), 1–9 (2016).
Shantakumari, N. et al. Computer use and vision. related problems among university students in Ajman, United Arab Emirate. Ann. Med. Health Sci. Res. 4(2), 258–263 (2014).
Page, M. J. et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 88, 105906 (2021).
Moher, D. et al. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 151(4), 264–269 (2009).
Agrawal, A. & Rasouli, M. Reference Management Software Programs. In EndNote 1-2-3 Easy! 7–18 (Springer, 2019).
Munn, Z. et al. JBI’s systematic reviews: Data extraction and synthesis. AJN Am. J. Nursing 114(7), 49–54 (2014).
Berkey, C. S. et al. A random-effects regression model for meta-analysis. Stat. Med. 14(4), 395–411 (1995).
Higgins, J. P. & Thompson, S. G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 21(11), 1539–1558 (2002).
Pustejovsky, J. E. & Rodgers, M. A. Testing for funnel plot asymmetry of standardized mean differences. Res. Synth. Methods 10(1), 57–71 (2019).
van Enst, W. A. et al. Investigation of publication bias in meta-analyses of diagnostic test accuracy: A meta-epidemiological study. BMC Med. Res. Methodol. 14(1), 1–11 (2014).
Spineli, L. M. & Pandis, N. Problems and pitfalls in subgroup analysis and meta-regression. Am. J. Orthod. Dentofac. Orthop. 158(6), 901–904 (2020).
Zalat, M. M. et al. Computer vision syndrome, visual ergonomics and amelioration among staff members in a Saudi medical college. Int. J. Occup. Saf. Ergon. 28, 1–9 (2021).
Abudawood, G. A. et al. Computer vision syndrome among undergraduate medical students in King Abdulaziz University, Jeddah, Saudi Arabia. J Ophthalmol https://doi.org/10.1155/2020/2789376 (2020).
Al Dandan, O. et al. Digital Eye strain among radiologists: A survey-based cross-sectional study. Acad. Radiol. 28(8), 1142–1148 (2021).
Al Subaie, M. et al. Computer vision syndrome among mobile phone users in Al-Ahsa, Kingdom of Saudi Arabia. Al-Basar Int. J. Ophthalmol. 4(4), 99 (2017).
Agbonlahor, O. Prevalence and knowledge of computer vision syndrome (CVS) among the working class adults in FCT Nigeria. J. Nigerian Optom. Assoc. 21(1), 49–60 (2019).
Nwankwo, B, Mumueh K, et al., Computer Vision Syndrome: Prevalence and Associated Risk Factors among Undergraduates in a Tertiary Institution in North western Nigeria. 2021.
Akowuah, PK, Nti AN, et al., Digital Device Use, Computer Vision Syndrome, and Sleep Quality among an African Undergraduate Population. Advances in Public Health, 2021. 2021.
Boadi-Kusi, SB, Abu SL, et al., Association between poor ergophthalmologic practices and computer vision syndrome among university administrative staff in Ghana. J. Environ. Public Health 2020. 2020.
Boadi-Kusi, SB, Adueming PO-W, et al., Computer vision syndrome and its associated ergonomic factors among bank workers. International Journal of Occupational Safety and Ergonomics, 2021: p. 1–8.
Arshad, S. et al. Computer vision syndrome: Prevalence and predictors among students. Ann. Psychophysiol 6(1), 15–22 (2019).
Mansoori, N. et al. Dry eye syndrome and associated risk factors among computer users in Karachi, Pakistan. ANNALS OF ABBASI SHAHEED HOSPITAL AND KARACHI MEDICAL & DENTAL COLLEGE 22(3), 165–170 (2017).
Noreen, K., Batool Z., et al., Prevalence of computer vision syndrome and its associated risk factors among under graduate medical students of urban karachi. Pakistan J. Ophthalmol., 2016. 32(3).
Noreen, K., Ali K., et al., Computer vision syndrome (CVS) and its associated risk factors among undergraduate medical students in midst of COVID-19. Pakistan J. Ophthalmol., 2021. 37(1).
Artime-Ríos, E. et al. Computer vision syndrome in healthcare workers using video display terminals: An exploration of the risk factors. J. Adv. Nurs. https://doi.org/10.1111/jan.15140 (2022).
Cantó-Sancho, N. et al. Computer vision syndrome prevalence according to individual and video display terminal exposure characteristics in Spanish university students. Int. J. Clin. Pract. 75(3), e13681 (2021).
Sánchez-Brau, M. et al. Prevalence of computer vision syndrome and its relationship with ergonomic and individual factors in presbyopic VDT workers using progressive addition lenses. Int. J. Environ. Res. Public Health 17(3), 1003 (2020).
Derbew, H. et al. Assessment of computer vision syndrome and personal risk factors among employees of commercial bank of Ethiopia in Addis Ababa, Ethiopia. J. Environ. Public Health https://doi.org/10.1155/2021/6636907 (2021).
Dessie, A. et al. Computer vision syndrome and associated factors among computer users in Debre Tabor Town Northwest Ethiopia. J. Environ. Public Health https://doi.org/10.1155/2018/4107590 (2018).
Gondol, B. N. et al. Prevalence of visual and posture related symptoms of computer vision syndrome among computer user workers of Ethiopian roads authority. J. Environ. Occup. Health 10(3), 73–78 (2020).
Assefa, N. L. 2015 Prevalence and associated factors of computer vision syndrome among bank workers in Gondar City, northwest Ethiopia. Clin. Optom. 9, 67 (2017).
Lemma, M. G. Computer vision syndrome and associated factors among secretaries working in ministry offices in Addis Ababa Ethiopia. Clin. Optom. 12, 213 (2020).
Lemma, M. T. et al. Computer vision syndrome and its predictors among secretary employees working in Jimma University, Southwest Ethiopia. J. Environ. Occup. Health 11(2), 27–36 (2021).
Zenbaba, D. et al. Prevalence of computer vision syndrome and associated factors among instructors in Ethiopian Universities: A web-based cross-sectional study. Sci. World J. https://doi.org/10.1155/2021/3384332 (2021).
Gammoh, Y. Digital eye strain and its risk factors among a university student population in jordan: A cross-sectional study. Cureus 13(2), e13575 (2021).
Wang, L. et al. Computer vision syndrome during SARS-CoV-2 outbreak in university students: A comparison between online courses and classroom lectures. Front. Public Health 9, 696036 (2021).
Han, C.-C. et al. Prevalence of asthenopia and its risk factors in Chinese college students. Int. J. Ophthalmol. 6(5), 718 (2013).
Hashemi, H., Khabazkhoob M., et al., The prevalence of asthenopia and its determinants among schoolchildren. J. Compr. Ped., 2017. 8(1).
Kamal, N.N., Abd El-Mageed A.S., Determinants of computer vision syndrome among bank employees in Minia City, Egypt. Egyptian J. Community Med., 2018. 36(4).
Nagwa, E. et al. Computer vision syndrome and associated factors among students of Faculty of Medicine, Cairo University. Med. J. Cairo Univ. 87, 4877–4881 (2019).
Zayed, H. A. M. et al. Digital eye strain: Prevalence and associated factors among information technology professionals Egypt. Environ. Sci. Pollut. Res. 28(20), 25187–25195 (2021).
Logaraj, M. et al. Computer vision syndrome and associated factors among medical and engineering students in Chennai. Ann. Med. Health Sci. Res. 4(2), 179–185 (2014).
Mohan, A. et al. Prevalence and risk factor assessment of digital eye strain among children using online e-learning during the COVID-19 pandemic: Digital eye strain among kids (DESK study-1). Indian J. Ophthalmol. 69(1), 140 (2021).
Rafeeq, U. et al. Computer vision syndrome among individuals using visual display terminals for more than two hours. Delta J. Ophthalmol. 21(3), 139 (2020).
Ranganatha, S. & Jailkhani, S. Prevalence and associated risk factors of computer vision syndrome among the computer science students of an engineering college of Bengaluru-a cross-sectional study. Galore Int. J. Health Sci. Res. 4(3), 10–15 (2019).
Rathore, D. A cross sectional study to assess prevalence of computer vision syndrome and vision related problems in computer users. J. Med. Sci. Clin. Res. 4, 11007–11012 (2016).
Tiwari, R. R. et al. Asthenopia (eyestrain) in working children of gem-polishing industries. Toxicol. Ind. Health 27(3), 243–247. https://doi.org/10.1177/0748233710386407 (2011).
Verma, S. et al. A cross-sectional study of the prevalence of computer vision syndrome and dry eye in computer operators. TNOA J. Ophthalmic Sci. Res. 59(2), 160 (2021).
Poudel, S. & Khanal, S. P. Magnitude and determinants of computer vision syndrome (CVS) among IT workers in Kathmandu Nepal. Nepalese J. Ophthalmol. 12(2), 245–251 (2020).
Sa, E. C. et al. Risk factors for computer visual syndrome (CVS) among operators of two call centers in São Paulo Brazil. Work 41(Suppl 1), 3568–3574. https://doi.org/10.3233/wor-2012-0636-3568 (2012).
Vilela, M. A. et al. Asthenopia in schoolchildren. Clin. Ophthalmol. 9, 1595–1603. https://doi.org/10.2147/opth.s84976 (2015).
Sawaya, R. I. T. et al. Asthenopia among university students: The eye of the digital generation. J. Family Med. Primary Care 9(8), 3921 (2020).
Uchino, M. et al. Prevalence of dry eye disease and its risk factors in visual display terminal users: the Osaka study. Am. J. Ophthalmol. 156(4), 759–766 (2013).
Wangsan, K. et al. Self-reported computer vision syndrome among Thai university students in virtual classrooms during the COVID-19 pandemic: Prevalence and associated factors. Int. J. Environ. Res. Public Health 19(7), 3996 (2022).
Akowuah, PK, Nti AN, et al., Research article digital device use, computer vision syndrome, and sleep quality among an African undergraduate population. 2021.
Arshad, S, Khan A, et al., Prevalence of asthenopia among computer operators in Central India and effectiveness of educational intervention. 2019.
Ranasinghe, P. et al. Computer vision syndrome among computer office workers in a developing country: An evaluation of prevalence and risk factors. BMC Res. Notes 9, 150. https://doi.org/10.1186/s13104-016-1962-1 (2016).
Khan, S, Khan S, et al., (2021) Comparison of prevalence data about digital eye strain (DES), pre-lockdown versus post-lockdown period in India a systematic review study. Children. 17: 18 74
Rosenfield, M. Computer vision syndrome: A review of ocular causes and potential treatments. Ophthalmic Physiol. Opt. 31(5), 502–515 (2011).
Adane, F. et al. Computer vision syndrome and predictors among computer users in Ethiopia: A systematic review and meta-analysis. Tropical Med. Health 50(1), 1–12 (2022).
Iqbal, M, Said O, et al., Visual sequelae of computer vision syndrome: A cross-sectional case-control study. J. Ophthalmol., 2021. 2021.
Acknowledgements
We would like to acknowledge Samara University for network and HINARY database website access.
Author information
Authors and Affiliations
Contributions
Conceptualization: A.K.L., Investigation: E.W.A., Methodology: A.K.L., E.W.A., Writing—original draft: E.W.A., Writing—review & editing: A.K.L., E.W.A.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Anbesu, E.W., Lema, A.K. Prevalence of computer vision syndrome: a systematic review and meta-analysis. Sci Rep 13, 1801 (2023). https://doi.org/10.1038/s41598-023-28750-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-28750-6
This article is cited by
-
Prevalence of computer vision syndrome during the COVID-19 pandemic: a systematic review and meta-analysis
BMC Public Health (2024)
-
Determinants of digital eye strain among university students in a district of India: a cross-sectional study
Journal of Public Health (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
