
Abstract
Type 2 Diabetes Mellitus (T2DM) is a significant public health problem globally. The diagnosis and management of diabetes are critical to reduce the diabetes complications including cardiovascular disease and cancer. This study was designed to assess the potential association between T2DM and routinely measured hematological parameters. This study was a subsample of 9000 adults aged 35–65 years recruited as part of Mashhad stroke and heart atherosclerotic disorder (MASHAD) cohort study. Machine learning techniques including logistic regression (LR), decision tree (DT) and bootstrap forest (BF) algorithms were applied to analyze data. All data analyses were performed using SPSS version 22 and SAS JMP Pro version 13 at a significant level of 0.05. Based on the performance indices, the BF model gave high accuracy, precision, specificity, and AUC. Previous studies suggested the positive relationship of triglyceride-glucose (TyG) index with T2DM, so we considered the association of TyG index with hematological factors. We found this association was aligned with their results regarding T2DM, except MCHC. The most effective factors in the BF model were age and WBC (white blood cell). The BF model represented a better performance to predict T2DM. Our model provides valuable information to predict T2DM like age and WBC.
Similar content being viewed by others


Introduction
Diabetes is a metabolic disease that shows itself clinically as chronic hyperglycemia, blood lipid and protein abnormalities, and other symptoms that increase the risk of morbidity and mortality1. Diabetes is a significant public health issue in the U.S. and around the world; it has been categorized as type 1, type 2, and gestational diabetes2. Type 2 diabetes mellitus (T2DM) is rising is relation to urbanization, population aging, and related lifestyle changes, especially in people over 653. Adults with diabetes were anticipated to number 415 million worldwide in 2015, and by 2040, that number will increase to 642 million2,4. The national Coronary Artery Disease (CAD) risk factors monitoring report estimates that among Iranians aged 15–64, the prevalence of diabetes was 8.7% in overall, with nearly half (4.1%) of those patients were newly diagnosed cases5. Diabetes is a serious and chronic disorder that has a significant negative impact on people's lives, families, and societies all over the world. Uncontrolled diabetes also increases the risk of metabolic, cellular, and blood disturbances leading to vascular complications, cancer, and all-cause death. According to estimates, it was one of the top 10 causes of mortality for adults and resulted in 4 million deaths worldwide in 20172,4. Despite the lack of the typical hematologic pathologic features associated with T2DM, several hematologic abnormalities have been identified in patients with this illness. It has been demonstrated that T2DM is closely related with several hematological abnormalities affecting platelets (PLTs), white blood cells (WBCs), red blood cells (RBCs), and the coagulation systems6,7.
Recent studies have indicated a correlation between some hematological parameters and diabetes, such as a reduction in RBC count in developing T2DM, and an increase in total WBC and PLT count in type 2 diabetic patients7,8,9. However, previous studies identified no relationship between T2DM and the other hematological parameters. Although a cross-sectional study has shown the association between the hematological parameters and T2DM in adult patients, its sample size was meaningfully lower than the current study7.
An early diagnosis and management of diabetes are crucial to reducing the risks of cardiovascular disease, cancer, and mortality due to the rising prevalence of diabetes and its relation to these diseases. The objective of this present study was to determine the association between diabetes and hematological factors.
Methods
Participants
The participants were recruited from the baseline of the Mashhad Stroke and Heart Atherosclerotic Disorders (MASHAD) study, Mashhad, north-eastern Iran, following a similar research protocol10. Nine thousand seven hundred four (9704) individuals aged 35–65 years were enrolled regarding their T2DM status were studied from the baseline of this cohort. T2DM was defined as a fasting blood glucose (FBG) ≥ 126 mg/dl or being treated with available oral hypoglycemic medications or insulin. Also, we consider triglyceride-glucose (TyG) index for the diagnosis of T2DM that defined as follows11:
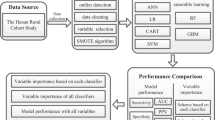
Also, we categorize the TyG index by using the median of our data. The median of TyG index in our data is 8.831. The inclusion criteria were males and females between the age of 35 and 65 years. We are dealing with data that is unbalanced (Diabetic vs. Non-Diabetic) in this investigation. One of the approaches that can be used for solving this problem is Synthetic Minority Oversampling Technique (SMOTE)12. The SMOTE algorithm is one of the most widely used under sampling and over sampling methods that create synthetic minority class samples. Therefore, in this study, the SMOTE algorithm was used to balance the classes. The observations were then analyzed on a balanced data set and after cleaning the data in each of the measured variables, finally with 9000 observations. After the cleaning data, we used the data from 9000 individuals in this study (Fig. 1).

Flow chart of this study.
At the beginning of this study, we measured the demographic characteristics (including gender and age) and hematological information including HGB (Hemoglobin), HCT (Hematocrit), MCH (Mean Corpuscular Hemoglobin), PLT (Platelet count), LYM (Lymphocyte Count), MXD (Mixed Cell Count), NEUT (Neutrophil Count), RDW (Red cell Distribution Width), PDW (Platelet Distribution Width), MPV (Mean Platelet Volume), RBC (Red Blood Cell), MCV (Mean Corpuscular Volume), MCHC (Mean Corpuscular Hemoglobin Concentration), and WBC (White Blood Cell).
Blood sampling
According to a standard protocol, all blood samples were taken from an antecubital vein of all participants who were in a sitting position, between 8–10 am, after 14 h of fasting. The samples were collected in 20 ml vacuum tubes and centrifuged for 30–45 min to separate the serum and plasma, and later sent to Bu Ali Research Institute, Mashhad, for laboratory examinations. Aliquots of serum were also kept frozen at -80 C for future analysis. The details of laboratory measurements and cut-offs are explained in the baseline report of the MASHAD cohort study10.
Statistical analysis and model building
To describe the quantitative and qualitative variables, mean ± SD and frequency (%) were reported, respectively. Chi-square and Fisher’s exact tests were applied to measure the association between categorical variables. Also, the mean of quantitative variables between the two groups were compared by independent T test. In addition, machine learning techniques such as logistic regression (LR) and decision tree (DT) algorithms have been used to analyze data. In fact, we applied these algorithms to deduce the association between T2DM and hematological factors. We considered two models for the prediction of T2DM. Model I investigated the association of T2DM with hematological factors and Model II investigated the association of the TyG index with hematological factors. All analysis were performed using SPSS version 22 (Armonk, NY: IBM Corp.) and SAS JMP Pro (SAS Institute Inc., Cary, NC) at the significant level of 0.05.
Logistic regression (LR) modeling
Logistic Regression is a popular model to evaluate the relationship between various predictor variables (either categorical or continuous) and binary outcomes in medicine, public health, etc.13.
Let \({Y}_{i}\) denotes the response variable and takes the values of 0 or 1 depending on whether response occurs or not. Also, \({\varvec{X}}\) be vectors of covariates associated with response variable, \({\varvec{\beta}}\) is the corresponding vectors of regression coefficients. So, the association between the covariates and binary response variable can be investigated as follows:
Decision tree (DT) modelling
Machine learning is one of the artificial intelligence analyses that emerged in the late twentieth century14,15. In other words, machine learning is a process for extracting hidden knowledge in large data sets. One of the important problems for researchers in this process is data classification16. There are different techniques for classification problems16. DT can be applied in various applications in the medical field17,18,19. Due to the simplicity in understanding and clarity and extracting simple and understandable rules, it is widely applied and studied in these fields16. The DT consists of components, nodes, and branches. So that, there are three types of nodes: (1) a root node represents the result of subdividing all records into two or more exclusive subsets. (2) The internal nodes represent a possible point in the tree structure connected to the root node from the top and the leaf nodes from the bottom. (3) Leaf nodes that show the tree’s final results in dividing records into target groups. Branches in the tree indicate the chance of placing records in target groups that emanate from the root node and the internal nodes14,15. DT algorithm uses the Gini impurity index for selecting the best variable.
where \({P}_{i}\) is the probability that a record in D belongs to the class \({C}_{i}\) and is estimated by |\({C}_{i}\),D|/|D. Logistic regression or LR is a statistical model applied to modeling dichotomous targets and investigating the effect of explanatory variables on the dichotomous target variable. In LR, the probability of placing each of the records in the target groups is also presented20,21. The main advantage of using the LR is that it can provide a good direct or inverse relationship between the inputs or explanatory variables and the target. It is also a flexible method22.
Bootstrap forest (BF) modeling
BF platform fits an ensemble model by averaging several decision trees, each of which is fit to a bootstrap sample of the training data. Each split in each tree shows a random subset of the predictors. In this way, many weak models are combined to produce a stronger model. The final prediction for an observation is the average of the predicted values for that observation over all the decision trees. In fact, the BF determines the significant factors associated with diabetes.
Receiver operating characteristic (ROC) curves were used to evaluate the accuracy, precision, and specificity for all three algorithms. Also, the confusion matrix of the three algorithms were given.
Ethics approval
All the participants consented to take part in the study by signing written informed consent. The study protocol was reviewed and all methods are approved by the Ethics Committee of Mashhad University of Medical Sciences with approval number IR.MUMS.REC.1399.660. All methods were carried out in accordance with relevant guidelines and regulations.
Results
A total of 9000 complete datasets of participant were analyzed in this cohort study (N = 4500 with Diabetes [female 62.77% vs male 37.22%], N = 4500 without Diabetes [female 59.15% vs male 40.84%]). The main baseline characteristics of the study population are summarized in Table 1. All the variables were significantly different between the two groups, including age, WBC, PDW, RDW, RBC, sex, PLT, MCHC, and HCT (P < 0.05). According to previous studies on the positive relationship of the TyG index with the presence of T2DM, we also considered the association of the TyG index with the hematological factors11,23,24.
Three machine learning techniques were used to investigate the relationship between hematological predictors and binary response variables (diabetic, and non-diabetic). So, the main objective of this study was to anticipate diabetes using the LR, DT, and BF models and to determine their associated factors, especially hematological markers. For this purpose, the dataset was randomly split into two parts: training data, and test data (75% vs 25%). The training dataset was utilized to develop the DT and BF models, which was then validated using test data (25%) that hadn't been used during training.
LR model
Results from the multiple LR model revealed that all variables were significantly associated with having of diabetes (P < 0.05). In other words, our findings after adjusting the effect of other variables in the Model I presented that the odds of having diabetes in males is 0.69 times than of females (P < 0.05). Also, after adjusting the effect of other variables for each increasing in age, the odds of having diabetes raises by 8 percent (P 0.05). Among the analyzed hematological variables, age (OR = 1.08, 95%CI = (1.07,1.08)), WBC (OR = 1.29, 95%CI = (1.24,1.33)), and PDW (OR = 1.11, 95%CI = (1.08,1.14)), had the greatest associations with having of diabetes, especially WBC because for each unit increase in WBC, the odds of having diabetes increases by 29 percent (P < 0.001) (Table 2 Model I). Also, our findings after adjusting the effect of other variables in the Model II presented that the odds of having high TyG index in males is 0.66 times than of females (P < 0.05). Also, after adjusting the effect of other variables for each increasing in age, the odds of having high TyG index raises by 7 percent (P < 0.05). Among the analyzed hematological variables, age (OR = 1.07, 95%CI = (1.06, 1.08)), RBC (OR = 1.74, 95%CI = (1.36, 1.38)), WBC (OR = 1.33, 95%CI = (1.28,1.38)), and PDW (OR = 1.08, 95%CI = (1.05,1.12)), had the greatest associations with having high TyG index, especially WBC because for each unit increase in WBC, the odds of having high TyG index increases by 33 percent (P < 0.001) (Table 2 Model II).
For comparison models the confusion matrices of the models I and II are given in Table 4. Moreover, Fig. 2 (a) and (b) depicts the ROC curves of the models I and II.

ROC curves for LR, DT, and BF algorithms for models I and II. Figures (a, c and e) show the ROC curves for LR, DT, and BF algorithms in model I. Also, figures (b, d and f) show the ROC curves for LR, DT, and BF algorithms in model II.
DT model
Figures S1 and S2 in Supplementary Information file illustrates the outcomes of the DT training for hematological factors. The DT algorithm determined the various diabetes risk factors and categorized them into 5 layers. According to the DT model, the first variable (root) is of the utmost significance for classifying data, with the subsequent variables having the subsequent levels of significance25. Figures S1 and S2 in Supplementary Information file illustrates that WBC, followed by age and RDW, has the greatest impact on the diabetes presence risk for models I and II.
In Model I participants with age < 47, WBC < 5.9, and RDW ≥ 41.2 had lower diabetes, according to the DT model, than those with higher WBC and RDW levels and older ages (0.8793 vs. 0.1207 incident rate). Eighty percent of patients had diabetes in the subgroup with older age (> = 47), low RDW (41.7), and high WBC (> = 6.8). More diabetes cases were represented by older age, higher WBC, and lower RDW levels than their corresponding opposite groupings. Table 3 (Model I) illustrates the specific diabetic rules developed by the DT model. The important variables in Table 2 (Model I) are used as input for this model. Age and WBC were thus determined to be the most crucial variables in the DT model and in the diagnosis of diabetes. In Model II participants with age < 47, WBC < 6.1, and RDW ≥ 39.4 had lower TyG index, according to the DT model, than those with higher WBC and RDW levels and older ages (0.8341 vs. 0.1659 incident rate). Eighty three percent of patients had high TyG index in the subgroup with older age (> = 47), high WBC (> = 6.3), and low RDW (< 41.7). Cases with high TyG index were represented by older age, higher WBC, and lower RDW levels than their corresponding opposite groupings. Table 3 (Model II) illustrates the specific rules developed by the DT model. The important variables in Table 2 (Model II) are used as input for this model. Age and WBC were thus determined to be the most crucial variables in the DT model and in the diagnosis of diabetes. For evaluation, the confusion matrices of the models I and II are given in Table 4. Moreover, Fig. 2(c) and (d) depicts the ROC curves of the models I and II.
BF model
Finally, for another analysis we used BF for classification the data based on diabetes. The factors included in this BF algorithm are 9 hematological factors for model I and 10 hematological factors for model II used in previous models. Also, in this case, we set the following specifications: Number of Trees in the Forest: 43, Number of Terms Sampled per Split: 2, Training Rows: 6750 for model I and 6734 for model II, Test Rows: 2250 for model I and 2244 for model II, Minimum Splits per Tree: 10, Minimum Size Split: 9. Again for comparison, the confusion matrices of the models I and II are given in Table 4. Moreover, Fig. 2 (e) and (f) show the ROC curves of the models I and II. As shown in Table 4 the accuracy of the models I and II are 83.33 and 97.43 percent. Furthermore, the important variables associated with T2DM based on BF algorithm are given as: Age, WBC, PLT, RBC, RDW, PDW, HCT, MCHC, and Sex in model I and Age, WBC, RBC, HGB, RDW, PDW, PLT, HCT, MCHC, and Sex in model II. As one can observe Age, and WBC were the most significant factors which equal to the obtained results from LR and DT models. We summarize this study in a graphical abstract in Fig. 3.

Graphical Abstract.
Discussion
In this study, a large number of biological and hematological factors like age, WBC, PDW, RDW, RBC, Sex, PLT, MCHC, and HCT had a significant relationship with T2DM. As we mentioned previously, we considered the association of the TyG index with hematological factors because of its positive relationship with T2DM presence. We found that the association of hematological factors with the TyG index was aligned with their results regarding T2DM, except MCHC. Therefore, we will continue the discussion based on the results of the T2DM and hematological factors. The most important and effective factors associated with T2DM presence were found to be age (as the most important and significant factors in the first line of DT) and WBC (as the second factor).
We found that in people over age of 47, the risk of diabetes increased dramatically. In line with our study, one study conducted in western Algeria on a sample of 1852 subjects, get these results with age 5025. In another study, the researchers indirectly found that the prevalence of T2DM was higher in middle-aged patients than in younger patients26. Contrary to our findings, a study on 307 diabetics showed that age had no significant relationship with the incidence or prevalence of diabetes1.
Our findings show that the WBC may be associated with the presence of T2DM. In people with a WBC ≥ 5.4, the prevalence of diabetics was 4 times more than of non-diabetics. Similarly, Lindsay et al. found that high WBC has the protentional to be considered as T2DM after adjusting for age and sex31. Another study conducted in 2018 showed that high WBC count, a marker of subclinical inflammation, can be used as an indicator of T2DM due to obesity32.
One of the most important difficulties for diabetics is the increased risk of thrombotic events and coagulation problems33. Platelets, are the main cellular element of coagulation, and play an important role in this process, and disruption in their number, shape, and activation pathways (measured by PT and MPV criteria) can lead to coagulation problems. The results of our study indicated a direct association between PLT count and the risk of diabetes. Conversely to our findings, the results obtained from a study of 1852 Algerian subjects with 1059 type 2 diabetic patients showed negative effect of PLT on the onset of T2DM25 and Some studies just showed that PLT levels are not involved in the development of diabetes pathology34,35. The association between PLT and MPV and their effects on each other has been investigated and confirmed in other studies, but surprisingly we could not find any significant association between MPV and the incidence of diabetes. Similarly, a number of studies could not find any association36,35,36,39, but some have found conflicting results with showing positive effects40,39,42.
The association of RDW and diabetes are stated in different studies. G. Smith and et al. found that Low RDW is associated with increased incidence of T2DM43 .Nevertheless, a study conducted in China in 2018 shows a direct link between RDW and the incidence of diabetes44.
We also found that HCT was negatively associated with the presence of diabetes, and a 2020 study in Northwest Ethiopia confirmed this inverse relationship45. But in another study, they could not find a significant link between HCT and diabetes46.
We also found that like high WBC, high RBC and MCHC can also increase the risk of diabetes. As shown in the decision tree, it can be inferred that a decrease in RBC, lower than 4.73, can greatly decrease the risk of diabetes.
Similar to our results, a study of 87 bangal T2DM showed a correlation between high MCHC and RDW with T2DM47. However, the study carried out in Saudi Arabia on a population with T2DM showed a negative association between diabetes and MCHC48. And so, this factor needs to be further investigated to determine its exact link to diabetes.
According to the results of the study, we obtained that for each unit increase in RBC, the odds of having diabetes 1.64 times which indicates a strong effect of red blood cell count on the risk of T2DM. However, very few studies in the world have linked this factor, and most studies have only reported the effect of T2DM on changes in the appearance and properties of red blood cells49,48,51. Even a 2013 study by Zhan-Sheng Wang and Zhan-Chun Song, which examined the relationship between red blood cell count and its effect on microvascular complications in Chinese patients with T2DM, yielded conflicting results. It was found that the proportion of patients with microvascular complications increases with decreasing red blood cell count (p value below 0.001)52. Another study in India in 2019 examined the association and role of hematological factors in diabetes mellitus reported that poorly controlled diabetics were more likely to develop anemia53.
One of the most important strengths of our study is the large sample size used. The second strength is the wide age range used in the study, which easily includes the three age groups of young, middle-aged, and elderly, and examines this relationship in them. Also, in this study we examined a relatively large number of hematological factors and for some of these factors not many studies have been done globally yet.
One of the limitations of this study is that we did not measure HbA1c in participants of the MASHAD cohort study. Moreover, it would have been much better if we could have enriched the target community in terms of cultural diversity because our study population was adults in the Mashhad cohort who all live in a common geographical area with relatively similar customs and lifestyles. This makes it impossible to generalize the results of this study to the other countries or even the total population of Iran.
The results of this study can help health authorities in early diagnosis and prevention of diabetes by examining only a few simple hematological criteria.
Conclusion
Our study showed that the BF model showed a better performance for the prediction of T2DM than the DT and LR models. According to our results, it may be concluded that some of the hematological factors could be valuable tool in the prediction of T2DM such as WBC, PDW, RDW, RBC, PLT, MCHC, and HCT. Among these hematological factors, WBC had the most significant role in the prediction of T2DM. Our findings indicates that hematological factors can be of value for using in the health care setting to predict the T2DM, as they are cost-effective, accessible, and simple markers.
Data availability
Data sharing is not applicable to this article as no new data were created in this study. Further enquiries can be directed to the corresponding author.
References
Demirtas, L. et al. Association of hematological indicies with diabetes, impaired glucose regulation and microvascular complications of diabetes. Int. J. Clin. Exp. Med. 8(7), 11420 (2015).
Xu, G. et al. Prevalence of diagnosed type 1 and type 2 diabetes among US adults in 2016 and 2017: Population based study. BMJ 362, k1497 (2018).
LeRoith, D. et al. Treatment of diabetes in older adults: An endocrine society* clinical practice guideline. J. Clin. Endocrinol. Metab. 104(5), 1520–1574 (2019).
Saeedi, P. et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the international diabetes federation diabetes atlas. Diabetes Res. Clin. Pract. 157, 107843 (2019).
Najafipour, H., Farjami, M., Sanjari, M., Amirzadeh, R., Shadkam Farokhi, M., Mirzazadeh, A. Prevalence and incidence rate of diabetes, pre-diabetes, uncontrolled diabetes, and their predictors in the adult population in southeastern Iran: Findings From KERCADR Study. Front. Public Health.9 (2021).
Jones, R. L. & Peterson, C. M. Hematologic alterations in diabetes mellitus. Am. J. Med. 70(2), 339–352 (1981).
Arkew, M., Yemane, T., Mengistu, Y., Gemechu, K. & Tesfaye, G. Hematological parameters of type 2 diabetic adult patients at debre berhan referral hospital, Northeast Ethiopia: A comparative cross-sectional study. PLoS ONE 16(6), e0253286 (2021).
Engström, G. et al. Red cell distribution width, haemoglobin A1c and incidence of diabetes mellitus. J. Intern. Med. 276(2), 174–183 (2014).
Milosevic, D. & Panin, V. L. Relationship between hematological parameters and glycemic control in type 2 diabetes mellitus patients. J. Med. Biochem. 38(2), 164–171 (2019).
Ghayour-Mobarhan, M. et al. Mashhad stroke and heart atherosclerotic disorder (MASHAD) study: Design, baseline characteristics and 10-year cardiovascular risk estimation. Int. J. Public Health 60(5), 561–572 (2015).
Hameed, E. K. TyG index a promising biomarker for glycemic control in type 2 diabetes mellitus. Diabetes Metab Syndr. 13(1), 560–563 (2019).
Lusa, L. Improved shrunken centroid classifiers for high-dimensional class-imbalanced data. BMC bioinformatics 14(1), 1–3 (2013).
David W. Hosmer Jr. SL, Rodney X. Sturdivant. Applied Logistic Regression. 3rd, editor. Hoboken, New Jersey: John Wiley & Sons Inc. (2013).
Saberi-Karimian, M. et al. Potential value and impact of data mining and machine learning in clinical diagnostics. Crit. Rev. Clin. Lab. Sci. 58(4), 275–296 (2021).
Mohammadi, M. & Mansoori, A. A projection neural network for identifying copy number variants. IEEE J. Biomed. Health Inform. 23(5), 2182–2188 (2018).
Zhong, Y., editor The analysis of cases based on decision tree.In 2016 7th IEEE international conference on software engineering and service science (ICSESS) IEEE (2016).
Aghasizadeh M, Samadi S, Sahebkar A, Miri‐Moghaddam E, Esmaily H, Souktanloo M, et al. Serum HDL cholesterol uptake capacity in subjects from the MASHAD cohort study: Its value in determining the risk of cardiovascular endpoints. J. Clin. Lab. Anal.:e23770 (2021).
Saberi‐Karimian, M., Safarian‐Bana, H., Mohammadzadeh, E., Kazemi, T., Mansoori, A., Ghazizadeh, H., et al. A pilot study of the effects of crocin on high‐density lipoprotein cholesterol uptake capacity in patients with metabolic syndrome: A randomized clinical trial. BioFactors. (2021).
Saberi-Karimian, M. et al. Data mining approaches for type 2 diabetes mellitus prediction using anthropometric measurements. J. Clin. Lab. Anal. 37(1), e24798. https://doi.org/10.1002/jcla.24798 (2023).
Hooley, J. M. & Teasdale, J. D. Predictors of relapse in unipolar depressives: Expressed emotion, marital distress, and perceived criticism. J. Abnorm. Psychol. 98(3), 229 (1989).
Mohammadi, F., Pourzamani, H., Karimi, H., Mohammadi, M., Mohammadi, M., Ardalan, N., et al. Artificial neural network and logistic regression modelling to characterize COVID-19 infected patients in local areas of Iran. Biomed. J. (2021).
Al-Azzam, N., Elsalem, L. & Gombedza, F. A cross-sectional study to determine factors affecting dental and medical students’ preference for virtual learning during the COVID-19 outbreak. Heliyon 6(12), e05704 (2020).
Chamroonkiadtikun, P., Ananchaisarp, T. & Wanichanon, W. The triglyceride-glucose index, a predictor of type 2 diabetes development: A retrospective cohort study. Prim. Care Diabetes 14(2), 161–167 (2020).
Park, B., Lee, H. S. & Lee, Y.-J. Triglyceride glucose (TyG) index as a predictor of incident type 2 diabetes among nonobese adults: A 12-year longitudinal study of the korean genome and epidemiology study cohort. Transl. Res. 228, 42–51 (2021).
Kachekouche, Y., Dali-Sahi, M., Benmansour, D. & Dennouni-Medjati, N. Hematological profile associated with type 2 diabetes mellitus. Diabetes Metab. Syndr. 12(3), 309–312 (2018).
Feldman-Billard, S., Sedira, N., Boelle, P.-Y., Poisson, F. & Héron, E. High prevalence of undiagnosed diabetes and high risk for diabetes using HbA1c criteria in middle-aged patients undergoing cataract surgery. Diabetes Metab. 39(3), 271–275 (2013).
Lee, J.-W., Lim, N.-K. & Park, H.-Y. The product of fasting plasma glucose and triglycerides improves risk prediction of type 2 diabetes in middle-aged Koreans. BMC Endocr. Disord. 18(1), 1–10 (2018).
Navarro-González, D., Sánchez-Íñigo, L., Pastrana-Delgado, J., Fernández-Montero, A. & Martinez, J. A. Triglyceride–glucose index (TyG index) in comparison with fasting plasma glucose improved diabetes prediction in patients with normal fasting glucose: The vascular-metabolic CUN cohort. Prev. Med. 86, 99–105 (2016).
Bennett, C., Guo, M. & Dharmage, S. HbA1c as a screening tool for detection of type 2 diabetes: A systematic review. Diabet. Med. 24(4), 333–343 (2007).
Selvi, N. M. K. et al. Association of triglyceride-glucose index (TyG index) with HbA1c and insulin resistance in type 2 diabetes mellitus. Maedica 16(3), 375 (2021).
Lindsay, R. High white blood cell count is associated with a worsening of insulin sensitivity and predicts the development o. Diabetes 51, 455 (2002).
Gu, Y. et al. White blood cells count as an indicator to identify whether obesity leads to increased risk of type 2 diabetes. Diabetes Res. Clin. Pract. 141, 140–147 (2018).
Kim, J. H., Bae, H. Y. & Kim, S. Y. Clinical marker of platelet hyperreactivity in diabetes mellitus. Diabetes Metab. J. 37(6), 423–428 (2013).
Kodiatte, T. A. et al. Mean platelet volume in type 2 diabetes mellitus. J. Lab. Physicians. 4(01), 005–009 (2012).
Zhang, M., Zhang, Y., Li, C. & He, L. Association between red blood cell distribution and renal function in patients with untreated type 2 diabetes mellitus. Ren. Fail. 37(4), 659–663 (2015).
Ozder, A. & Eker, H. H. Investigation of mean platelet volume in patients with type 2 diabetes mellitus and in subjects with impaired fasting glucose: A cost-effective tool in primary health care?. Int. J. Clin. Exp. Med. 7(8), 2292 (2014).
Jabeen, F., Fawwad, A., Rizvi, H. A. & Alvi, F. Role of platelet indices, glycemic control and hs-CRP in pathogenesis of vascular complications in type-2 diabetic patients. Pak. J. Med. Sci. 29(1), 152 (2013).
Zaccardi, F. et al. Platelet mean volume, distribution width, and count in type 2 diabetes, impaired fasting glucose, and metabolic syndrome: A meta-analysis. Diabetes Metab. Res. Rev. 31(4), 402–410 (2015).
Erdoğan, S. et al. Liver enzymes, mean platelet volume, and red cell distribution width in gestational diabetes. Turkish J. Med. Sci. 44(1), 121–5 (2014).
Lippi, G. et al. The mean platelet volume is significantly associated with higher glycated hemoglobin in a large population of unselected outpatients. Prim. Care Diabetes 9(3), 226–230 (2015).
Akinsegun, A., Olusola, D.A., Sarah, J.-O., Olajumoke, O., Adewumi, A., Majeed, O., et al. Mean platelet volume and platelet counts in type 2 diabetes: mellitus on treatment and non-diabetic mellitus controls in Lagos, Nigeria. Pan Afr. Med. J. 18 (2014).
Hekimsoy, Z., Payzin, B., Örnek, T. & Kandoğan, G. Mean platelet volume in Type 2 diabetic patients. J. Diabetes Complicat. 18(3), 173–176 (2004).
Engström, G. et al. Red cell distribution width, haemoglobin A 1c and incidence of diabetes mellitus. J. Intern. Med. 276(2), 174–183 (2014).
Zhang, J. et al. The association between the red cell distribution width and diabetic nephropathy in patients with type-2 diabetes mellitus. Ren. Fail. 40(1), 590–596 (2018).
Adane, T., Getaneh, Z. & Asrie, F. Red blood cell parameters and their correlation with renal function tests among diabetes mellitus patients: A comparative cross-sectional study. Diabetes Metab. Syndr. Obes. Targets Ther. 13, 3937 (2020).
Berria, R. et al. Reduction in hematocrit and hemoglobin following pioglitazone treatment is not hemodilutional in type II diabetes mellitus. Clin. Pharmacol. Ther. 82(3), 275–281 (2007).
Jaman, M. S. et al. Diabetes and red blood cell parameters. Ann. Clin. Endocrinol. Metabol. 2, 001–009 (2018).
Waggiallah, H. & Alzohairy, M. The effect of oxidative stress on human red cells glutathione peroxidase, glutathione reductase level, and prevalence of anemia among diabetics. N. Am. J. Med. Sci. 3(7), 344 (2011).
Rand, P. W. et al. Effects of diabetes mellitus on red cell properties. Clin. Hemorheol. Microcirc. 1(4), 373–384 (1981).
Moon, J. et al. Impaired RBC deformability is associated with diabetic retinopathy in patients with type 2 diabetes. Diabetes Metab. 42(6), 448–452 (2016).
Vahalkar, G. S. & Haldankar, V. A. RBC membrane composition in insulin dependent diabetes mellitus in context of oxidative stress. Indian J. Clin. Biochem. 23(3), 223–226 (2008).
Wang, Z.-S. et al. Red blood cell count as an indicator of microvascular complications in Chinese patients with type 2 diabetes mellitus. Vasc. Health Risk Manag. 9, 237 (2013).
Farooqui, R., Afsar, N. & Afroze, I. A. Role and significance of hematological parameters in diabetes mellitus. Annal. Pathol. Lab. Med. 6(3), 158–162 (2019).
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
A.M.: conception, data analyzing. T.S.: conception, interpretation of data. Z.S.H.: drafting the article. S.S.S.: conception, interpretation of data. N.E.: drafting the article. E.N.: data analyzing. M.G.: revising the article. Z.K.: drafting the article. S.E.: revising the article. M.G.: formal analysis. G.F.: revising the article. H.E.: corresponding author. M.G.M.: corresponding author.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Mansoori, A., Sahranavard, T., Hosseini, Z.S. et al. Prediction of type 2 diabetes mellitus using hematological factors based on machine learning approaches: a cohort study analysis. Sci Rep 13, 663 (2023). https://doi.org/10.1038/s41598-022-27340-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-27340-2
This article is cited by
-
White blood cell and platelet distribution widths are associated with hypertension: data mining approaches
Hypertension Research (2024)
-
Unpacking Occupational Health Data in the Service Sector: From Bayesian Networking and Spatial Clustering to Policy-Making
Mathematical Geosciences (2024)
-
A Comprehensive Survey on Diabetes Type-2 (T2D) Forecast Using Machine Learning
Archives of Computational Methods in Engineering (2024)
-
Uric acid is associated with type 2 diabetes: data mining approaches
Diabetology International (2024)
-
iDP: ML-driven diabetes prediction framework using deep-ensemble modeling
Neural Computing and Applications (2024)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
