
Abstract
Aging not only affect biomarker-related processes, but it also affects the physiological processes of the human body. Of all the physiological processes, hearing and vision are of utmost importance to a human. Therefore, this study examines the prevalence and factors associated with hearing and vision difficulty and their sequential treatment among older adults in India. Utilizing data from Building a Knowledge Base on Population Aging in India, study used two sets of outcome variables; firstly, self-reported hearing and vision difficulty and secondly, treatment-seeking for hearing and vision difficulty. A total of 9541 older adults aged 60+ years from seven major regionally representative states were selected. Descriptive statistics were used to perform preliminary analysis. Additionally, the study employed the Heckprobit selection model. It is a two-equation model. This model is used in order to accommodate the heterogeneity (i.e., shared unobserved factors) among older adults and then address the endogeneity (between hearing and vision loss problems and their treatment-seeking behaviour) for older adults in India, the model offers a two-step analysis and deals with the zero-sample issue. Around 59% and 21% of older adults reported vision and hearing difficulty, respectively. Only 5% of older adults suffering from hearing difficulty reported utilizing hearing aids. Lifestyle factors (smoking tobacco and chewing tobacco) significantly affect hearing and vision difficulty; various chronic diseases were also found to be associated with high levels of hearing and vision difficulty among older adults. Results from Heckprobit model shows that older adults with 11+ years of education had higher probability to use visual [β = 0.54, 95% confidence interval (CI): 0.37, 0.70] and hearing aids [β = 0.6, 95% CI: 0.18, 1.02]. The use of hearing and vision aids was lower among poor older adults, older adults from Scheduled Caste, and older adults in rural areas. The study indicates that more than half of older adults face vision difficulty and almost one-fourth face hearing difficulty in rural India, education and lifestyle appear to be the main driver of health-seeking behaviour. Additional attention shall be given to understand the strategies that may advocate a higher use for hearing aids among older adults.
Similar content being viewed by others

Introduction
The etiology of the ageing process is a cumbersome process and is yet to be fully developed1. Various researcher have shared their views on the definition of ageing, and most of them agreed that ageing is the gradual accumulation of deleterious biological changes that are accompanied by a progressive loss of function2,3. The world is getting older faster than ever. With a decline in fertility and an increase in life expectancy around the globe, the ageing population is on the rise. This rise in ageing population is more worrisome in Europe and other western countries than anywhere else. In India, the ageing population has increased sharply during recent years4. The rise in ageing population is posing a challenge at the policy front. Researchers unanimously have associated aging with various degenerative problems4.
Aging not only affect biomarker related processes, but it also affects the physiological processes of the human body5. Hearing and vision difficulty are highly associated with ageing population across the populations6,7,8,9,10,11,12,13. Hearing and vision difficulty among older adults significantly affect their quality of life6,14. Hearing and vision difficulty is a common problem among older adults, and the impact of such loss may be profound15,16. The hearing and vision difficulty may have consequences for the social, functional, and psychological well-being of older adults12,15,16,17. Evidence from a large body of literature suggest a relationship of unhealthy behaviour such as smoking and drinking alcohol with the incidence of vision impairment19,20. A cohort study among the older adults conclude that participants with three unhealthy behaviour i.e., low die quality, heavy smoking and sedentary lifestyle increased the odds of vision impairment by threefold21. The biological mechanisms explain that smoking may reduce choroidal blood flow in the eye, and promote ischaemia, micro-infarctions, and hypoxia, all of which may increase the risk of vision impairment22,23. Also, there is a dirt of literatures on the direct relationship between smoking and hearing impairment. Only few studies acknowledge the causes of hearing loss due to cigarette smoking and alcohol drinking24,25,26,27. However, some studies failed to find any association between them28,29. Although the underlying mechanisms regarding the effect of smoking on auditory organ is unclear, studies pointed out the mechanisms including direct ototoxicity of nicotine, cochlear ischemia due to increased level of cardoxyhemoglobin, and smoking-mediated increased blood viscosity30. Moreover, evidence from many studies have acknowledge the association of increased risk of chronic condition among the vision and hearing impaired individual31,32. Of these chronic condition diabetes and hypertension which are the common degenerative diseases among the ageing population have been found to be closely link with ageing-related vision impairment and hearing loss33,34. Vision loss among diabetic patient is cause when high blood sugar damages the blood vessel in the retina. Damage blood vessels may leak and swell, resulting in blurry vision or stopping blood flow35. Hearing loss among the hypertensive is related to a microcirculatory insufficiency that occurs due to vascular occlusion caused by emboli, haemorrhage or vasospasm36. Studies have also found a link between socio-economic and demographic factors such as age, education, living arrangement, and marital status with vision and hearing impairment19,21,25,30.
Hearing difficulty is said to affect physical and social functioning, which may further have an impact on behavioural disorders, mood disturbances, and cognitive deficits13,17,18. Most of the hearing losses among older adults could be responsive to amplification37,38. Although hearing impairment among older adults can be treated using a hearing aid, accessibility and affordability to these aids becomes a challenge for the underprivileged older adults. In India, a considerable proportion of the population lives in rural areas without social and economic security and without access to proper medical care, which leaves them helpless in utilizing hearing aids39. Furthermore, various reasons are found to be associated with the under-utilization of hearing aids among older adults population40. Archana et al. noted attitude related factors and device-related factors to be most significant for non-use of hearing aids40. Vision difficulty is another common ailment among older adults in India. More than 50 million people in India were estimated to have low vision41. Uncorrected refractive errors and cataract are the two most significant factors of visual impairment among older adults41. Studies have noted a lower level of utilization of eye care services among older adults42. Various reasons were attributed to poor utilization of eye care services in India, no importance to eyes43, low education attainment, and low income44.
This study aimed to estimate the determinants of vision and hearing difficulty and decision to use vision and hearing aids. The analysis was performed under the assumptions that reporting vision and hearing difficulty and decision to use aids for the problem is a sequential decision making process. In our study about 40% and 80% of the older adults did not report any vision and hearing difficulty respectively, and for using vision and hearing aids (as a dependent variable) for them was zero. Thus, these zero observations result to sample selection biased leading to biased parameter estimation if the appropriate statistical model is not adopted. It is found that the two-stage regression model, Tobit model etc. are widely used methods to deal with this kind of data45. However, these model is acknowledging as restrictive because they are unable to provide a holistic picture that demonstrates an individual’s underlying sequential decision-making process: whether or not having vision or hearing difficulty (i.e., participant decision) leading to a decision of whether to seek treatment or not (i.e., treatment decision). The present study adopted the Heckman selection model to address the critical drawbacks of the other models46. The Heckman model adopted a two-step process that describes individual’s decision of using vision or hearing aids. According to this model, older adults report of having vision or hearing difficulty or not, and then decide whether to use vision or hearing aids or not. Further, to accommodate the heterogeneity (i.e., shared unobserved factors) among older adults and then address the endogeneity (between hearing and vision loss problems and its treatment seeking behaviour) for older adults in India, the model offers a two-step analysis and deals with the zero-sample issue47.
In this study we hypothesize that there is no relationship between having vision and hearing difficulty with decision making of using vision or hearing aid for the problem among older adults.
Data and methods
Data
The current study employed data from the Building a Knowledge Base on Population Aging in India (BKPAI) survey, which was conducted across seven Indian states in 2011. The survey collected data on several socioeconomic and health aspects of ageing in households with members aged 60 and up. The survey included seven large regionally representative states with higher populations of people aged 60 and up than the national average. The Primary Sampling Units (PSUs) were chosen using the probability proportional to population size (PPS) technique, and elderly households were picked using systematic sampling within each PSU. The northern section of the country is represented by Punjab and Himachal Pradesh, the southern part by Kerala and Tamil Nadu, the eastern part by Orissa and West Bengal, and the western part by Maharashtra. The states were chosen because they had a higher percentage of people aged 60 and up than the national average and represented all of the country's regions. As a result, the survey was deemed nationally representative.
Villages in rural regions and urban wards in urban areas were the primary sample units (PSUs). Each state had a set sample of 1280 elderly households. More information on the sampling technique and sample size may be found in BKPAI's national and state reports from 201148. The effective sample size for the current study was 9541 older individuals aged 60 and up from seven states. The research was carried out in conformity with all applicable laws and regulations. All the methods were applied as per relevant guidelines.
Outcome variables
There were two outcome variables used in the present study. Firstly, whether older adults were having any difficulty in vision (no or yes) and hearing (no or yes)? Secondly, whether older adults use any aids for self-reported vision and hearing impairment? Spectacles or lenses (no or yes) and hearing aid (no or yes).
Predictor variables
The predictor variables were categorized according to the previous literature. The predictor variables are as follows; Smoking tobacco (no or yes), chewing tobacco (no or yes), alcohol consumption (no or yes), diabetes (no or yes), hypertension (no or yes), stroke (no or yes), heart disease (no or yes), cataract (no or yes). Diabetes, hypertension, stroke, heart disease and cataract was assed using the question “has a doctor or nurse ever told you that you have Diabetes, hypertension, stroke, heart disease or cataract?”. Further variables were categorized into age (60–69, 70–79 and 80+), gender (men and women), marital status (not in a union and currently in a union), education (not educated, below five years, 6–10 years and 11+ years), working status (no, yes and retired), economic independence (independent, pension and dependent), living arrangement (alone, with the spouse, with children and others), wealth (poor, middle and rich). The wealth index drawn based on the BKPAI survey is based on the following 30 assets and housing characteristics: drinking water source; household electrification; type of toilet facility; cooking fuel; type of house; house ownership; ownership of a bank or post-office account; and ownership of a mattress, a pressure cooker, a chair, a cot/bed, a table, an electric fan, a radio/transistor, a colour television, a black and white television, a sewing machine, a mobile telephone, any landline phone, internet facility, a computer; a refrigerator, a watch or clock, a bicycle, an animal-drawn cart, a motorcycle or scooter, a car, a water pump, a thresher, and a tractor. Religion (Hindu, Muslim, Sikh, and others), caste (Scheduled Caste/Scheduled Tribe (SC/ST) and non-SC/ST), residence (rural and urban) and states (Himachal Pradesh, Punjab, West Bengal, Orrisa, Maharashtra, Kerala, and Tamil Nadu).
Statistical analysis
Preliminary analysis was carried out using descriptive statistics and bivariate analysis. The Heckprobit selection model, a two-equation model, was also used in the study49,50,51. First, there is a selection model (in this study, referring to “Do you have any of the following difficulties either vision or hearing? (yes or no)”). Secondly, there is an outcome model with a binary outcome (in this study refers to “Do you use any of the following aids either spectacles or lenses or a hearing aid? (yes or no)”). The model provides a two-step analysis and deals with the zero-sample issue, based on which it can accommodate the heterogeneity (i.e., shared unobserved factors) between older adults and then address the endogeneity (between difficulties in vision or hearing and opting for aid for the problem) for older adults in India. When the same independent variables from the selection equation occur in the result equation, the Heckman model is identified52,53,54. Because of the significant multicollinearity, this does not yield precise estimates in the outcome equation; it was advised that at least one independent variable must appear in the selection equation but not in the outcome equation. Statistical significance was defined as a p-value of less than 0.05.
The probit model with sample selection assumes that there exists an underlying relationship54:
such that we observe only the binary outcome54
The dependent variable, however, is not always observed. Rather, the dependent variable for observation j is observed if:
\({y}_{i}^{select}=\left({z}_{j}\gamma +{u}_{2j}\right)>0 \mathrm{selection\,\, equation}\)\(where\), \({u}_{1}\sim N (0, 1)\), \({u}_{2}\sim N (0, {\sigma }^{2})\), \(Corr \left({u}_{1},{u}_{2}\right)=\rho\).
When \(\rho\) ǂ 0, standard probit techniques applied to the first equation yield biased results. Heckprobit provides consistent, asymptotically efficient estimates for all the parameters in such models. The selection equation should have at least one variable that is not in the probit equation for the model to be well identified. The model is otherwise solely identified by its functional form, and the coefficients have no structural meaning.
Results
Figure 1 shows that more than half (59%) of the older adults reported vision problems and about 53.9% of them were using visual aids for the same (59% of the older adults in the sample). Moreover, one-fifth of older adults (20.5%) were suffering from hearing difficulty, and about 5% of them were using hearing aids (20.5% of the older adults in the sample). The hearing and vision loss are self-reported.

Percentage of older adults suffering from vision and hearing disability and their utilization of visual and hearing aids.
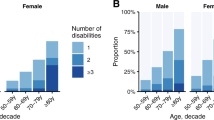
The socio-demographic profile of older adults was presented in Table 1. About fifteen percent of older adult’s smoke, 22% chewed tobacco, and another 8% consumed alcohol. Around 10%, 21%, 6%, and 13% of older adults were suffering from diabetes, hypertension, heart disease, and cataract, respectively. A majority of older adults belonged to 60–69 years’ age group, 53% were women, and three-fifths of the study population was currently in a union. About half of the older adults had no education and were dependent on pension, 67% were not working, and 70% were living with their children. One-fourth of the study population lived in urban areas.
Table 2 found that more than half of the older adults who reported the use of smoking (65%), chewing tobacco (69%), and alcohol consumption (62%) were suffering from a vision problem. Seven in every ten older adults suffering from diabetes (73%), hypertension (74%), stroke (74%), and heart diseases (74%) reported vision problems. Around 61% of women and 54% of working older adults reported a vision problem. Moreover, the use of visual aid was higher among men (57.7%), having 11+ education (84.4%), and rich older adults (76.1%). On the other hand, the hearing problem was more prevalent among older adults who smoke (21.5%), chew tobacco (24.5%), and were suffering from diabetes (21.2%), hypertension (23.6%), stroke (40.4%), and heart disease (26.5%) compared to their counterparts. Around 46 percent of the older adults aged 80+ were suffering from hearing problems. Interestingly, hearing problem (22%) was higher among women, but the use of hearing aid was higher in men (5.1%).
The results from the Heckprobit model for reporting of vision problems and sequential decision making for the use of visual aids are presented in Table 3. Results found that older adults who smoked [β = 0.24; CI: 0.15–0.33] and chewed tobacco [β = 0.14; CI: 0.07–0.21] had 0.24 and 0.14 times higher probability to have a vision problem, respectively. Furthermore, older adults who had diabetes [β = 0.25; CI: 0.16–0.34], hypertension [β = 0.31; CI: 0.24–0.38], and those who suffered from heart diseases [β = 0.22; CI: 0.10–0.33] had 0.25, 0.31, and 0.22 times more risk of vision problem, respectively. As expected, those suffering from cataract were highly susceptible to report vision problems. In the age group 70–79 years, the probability of having a vision problem was 0.30 times higher [β = 0.30; CI: 0.23–0.36], and in the age group 80 + years [β = 0.52; CI: 0.42–0.62], it was 0.52 times higher than the referenced category of age 60–69 years. Older adults with 11 + education had 0.18 times higher chances to report vision problems than older adults with no education [β = 0.18; CI: 0.06–0.31], and a similar result was found for using visual aids [β = 0.54; CI: 0.37–0.70]. Rich (0.52 times) older adults had higher probability to use vision aids compared to poor older adults [β = 0.52; CI: 0.42–0.63].
The results from the Heckprobit model for reporting of hearing problems and sequential decision making for the use of hearing aids are presented in Table 4. Older adults suffering from diabetes [β = 0.10; CI: 0.00–0.20] and heart diseases [β = 0.19; CI: 0.06–0.31] had 0.10 times and 0.19 times higher probability to report hearing problems, respectively, as compared to those who were not suffering from those diseases. Moreover, older adults currently in a union, having any level of education, and retired from work had lower probability to report hearing problems than their counterparts. On the other hand, older adults with 11 + education [β = 0.60; CI: 0.18–1.02] and living with children [β = 0.47; CI: 0.03–0.97] had 0.60 times and 0.47 times, respectively, higher probability to use hearing aids compared to older adults having no education and living alone.
Discussion
Vision and hearing disabilities are particularly prominent problems in the aging population. While vision difficulty harms a person’s physical senses of the surrounding world, hearing difficulty diminishes a person’s mode of social interactions and can lead to social isolation. Deteriorations in vision and hearing are associated with reduced quality of life, increased physical difficulty, imbalance, falls, hip fracture, and mortality55,56,57. A longitudinal study in UK provides evidence that hearing impairment among older adults is associated with loneliness, social isolation and the effect on cognitive function58. However, the rate of cognitive decline can be delayed or arrested if treatment is provided as earlier as possible with the help of hearing aid device17,58. The present study tries to address the issue of various factors associated with vision and hearing difficulty among older adults in India. The study reported that vision difficulty was a prominent difficulty among older adults than hearing difficulty. Various socio-economic, demographic, and behavioural risk factors were found to be associated with vision and hearing difficulty among older adults. We found a high proportion of older adults who reported having vision and hearing difficulty were also smoking, chewing tobacco, drinking alcohol, and suffering from chronic diseases. Also, the proportion of using vision and hearing aid among older adults varies by gender, level of education, and economic status.
Tobacco smoking has long been known as a significant risk factor for many chronic diseases; the effect of smoking on vision loss is not well recognized. Our results from the heckprobit model provide evidence that older adults who use smoked and chewed tobacco were more likely to report having vision difficulty, and the results are consistent with the previous results19. Previous literature has acknowledged that current smokers with cataract were more likely to suffer visual loss than non-smokers with cataracts20. Age-related macular degeneration (AMD) is the main cause of vision difficulty for older adults, although it does not cause complete blindness to a person, it can lead to loss of central vision, which happens very slowly in life. Epidemiological evidence suggests that smoking is a strong causality for age-related macular degeneration, that may promote ischemia, hypoxia, and micro-infractions and reduce choroidal blood flow in the eye, all of which could increase the predisposition of the macula to degenerative changes59,60. Our analysis also indicates that difficulty in vision was more likely to occur in older adults with a chronic disease like diabetes, hypertension, and heart disease compared with people without chronic disease, which is consistent with the previous studies conducted in Australia and America22,55. The possible explanation is that physical inactivity among individuals has been identified as the main factor attributed to the development of non-communicable disease32. Vision-impaired individuals are more likely to be physically inactive due to the fear of falls, which then puts them at a higher risk of developing chronic disease.61 Another reason may be related to eating unhealthy food as vision-impaired individuals may face difficulty in choosing healthy food if they cannot read the food nutrition labels properly62.
In terms of living arrangements, it was observed that older adults living alone were more likely to report having a vision difficulty as compare to those living with spouses or children. Previous literature suggests that older people living alone are considered as vulnerable as they were characterized by difficult living condition, lack of social support, high poverty, experience greater challenges in daily activities, and at greater risk of developing any chronic disease due to lifestyle factors63. Kharicha et al. mentioned that the difficulty with instrumental activities of daily living among older adults living alone might be related to the risk of chronic diseases like glaucoma, cataract, and arthritis64. Literate older adults from better household economic status were more likely to use visual aid as compared to those from poor economic status. Previous studies have acknowledged the use of visual aid, which includes spectacles increased with increasing socioeconomic status and possibly associated with the increased level of education65. However, use of spectacles in the rural areas remains low due to the cost of spectacles and low educational level in the rural areas66,67, users were found to be more common among the literates and employed people64,67.
Older adults with chronic diseases like diabetes and heart disease were found to be associated with having a hearing difficulty, which is consistent with our findings33,55. Study shows that peripheral nerve injury and presence of albuminuria among the patients with type 2 diabetes was associated with hearing loss33,68. Furthermore, older adults with higher levels of education and living with children were more likely to use a hearing aid. The possible explanation could be due to the indirect effect, as education is closely related to income, and the high cost was one of the key reasons for not using of hearing aid69,70, and on the other hand, older adults living with their children usually get their financial support and have access to better health care71.
The study had certain limitation. Firstly, the vision and hearing difficulty were self-reported in nature. Secondly, due to the binary response of hearing and visual difficulty, we cannot assess the types of hearing and visual difficulty which are the main contributors of these difficulty. However, apart from all these limitations the present paper presents the results which are quite important from policy point of view.
Conclusion
Our study has shown that a higher percentage of older adults have vision difficulty than hearing difficulty; moreover, the treatment-seeking for vision difficulty was much higher among older adults than treatment-seeking for hearing difficulty. Lifestyle factors (smoking tobacco and chewing tobacco) significantly affect hearing and vision difficulty; various chronic diseases were also found to be associated with high levels of hearing and vision difficulty among older adults. Hearing and vision difficulty, along with the sequential treatment for these ailments, were significantly affected by various socio-economic characteristics. The use of hearing and visual aids was lower among poor older adults, older adults from Scheduled Caste, and older adults in rural areas. It can be assumed that hearing and vision aids were significantly affected by their cost as the sequential treatment for hearing and vision difficulty was lower among poor older adults. Based on our findings, we recommend that additional attention shall be given to understand the strategies that may advocate a higher use for hearing aids among older adults. Although a well-planned health structure is in place in India, we suggest that this system of health structure shall be re-examined to establish and integrate the various needs of older adults. There is a need to integrate public health approaches into interventions for older adults with hearing and vision impairments.
References
López-Otín, C., Blasco, M. A., Partridge, L., Serrano, M. & Kroemer, G. The hallmarks of aging. Cell 153(6), 1194–1217. https://doi.org/10.1016/j.cell.2013.05.039 (2013).
Shpilka, T. & Haynes, C. M. The mitochondrial UPR: Mechanisms, physiological functions and implications in ageing. Nat. Rev. Mol. Cell Biol. 19(2), 109. https://doi.org/10.1038/nrm.2017.110 (2018).
Maklakov, A. A. & Chapman, T. Evolution of ageing as a tangle of trade-offs: Energy versus function. Proc. R. Soc. B. 2019(286), 20191604. https://doi.org/10.1098/rspb.2019.1604 (1911).
Patel, R., Chauhan, S., Chaurasiya, D., Kumar, S. & Paswan, B. Role and impact of social capital on health of older adult in India. Indian J. Soc. Res. 60(2), 279–305 (2019).
Cole, J. H., Marioni, R. E., Harris, S. E. & Deary, I. J. Brain age and other bodily ‘ages’: Implications for neuropsychiatry. Mol. Psychiatry 24(2), 266–281. https://doi.org/10.1038/s41380-018-0098-1 (2019).
Wang, B. et al. Burden of vision loss associated with eye disease in China 1990–2020: Findings from the Global Burden of Disease Study 2015. Br. J. Ophthalmol. 102(2), 220–224. https://doi.org/10.1136/bjophthalmol-2017-310333 (2018).
Davies-Kershaw, H. R. et al. Vision impairment and risk of dementia: findings from the English longitudinal study of ageing. J. Am. Geriatr. Soc. 66(9), 1823. https://doi.org/10.1111/jgs.15456 (2018).
McMullan, I. I., Bunting, B. P., Smith, L., Koyanagi, A. & Tully, M. A. Is there an association between self-reported physical activity and self-rated vision over time? Results from the Irish Longitudinal Study of Ageing. J. Aging Phys. Activity. 1, 1–8. https://doi.org/10.1123/japa.2019-0371 (2020).
Saftari, L. N. & Kwon, O. S. Ageing vision and falls: A review. J. Physiol. Anthropol. 37(1), 1–4. https://doi.org/10.1186/s40101-018-0170-1 (2018).
Maharani, A., Dawes, P., Nazroo, J., Tampubolon, G. & Pendleton, N. Sense-Cog WP1 group. Visual and hearing impairments are associated with cognitive decline in older people. Age Ageing. 47(4), 575–581. https://doi.org/10.1093/ageing/afy061 (2018).
Dawes, P., Wolski, L., Himmelsbach, I., Regan, J. & Leroi, I. Interventions for hearing and vision impairment to improve outcomes for people with dementia: A scoping review. Int. Psychogeriatr. 31(2), 203–221 (2019).
Yamada, Y. et al. Dual sensory impairment and cognitive decline: The results from the shelter study. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 71(1), 117–123. https://doi.org/10.1093/gerona/glv036 (2016).
Livingston, G. et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 396(10248), 413–446. https://doi.org/10.1016/S0140-6736(20)30367-6 (2020).
Ciorba, A., Bianchini, C., Pelucchi, S. & Pastore, A. The impact of hearing loss on the quality of life of elderly adults. Clin. Interv. Aging 7, 159. https://doi.org/10.1007/s00405-016-4222-z (2012).
Sabel, B. A., Wang, J., Cárdenas-Morales, L., Faiq, M. & Heim, C. Mental stress as consequence and cause of vision loss: The dawn of psychosomatic ophthalmology for preventive and personalized medicine. EPMA J. 9(2), 133–160. https://doi.org/10.1007/s13167-018-0136-8 (2018).
Picou, E. M. & Buono, G. H. Emotional responses to pleasant sounds are related to social disconnectedness and loneliness independent of hearing loss. Trends Hear. 22, 2331216518813243. https://doi.org/10.1177/2331216518813243 (2018).
Jayakody, D. M. et al. Hearing aids to support cognitive functions of older adults at risk of dementia: The HearCog trial-clinical protocols. BMC Geriatr. 20(1), 1–8 (2020).
Lin, F. R. et al. Hearing loss and cognitive decline in older adults. JAMA Intern. Med. 173(4), 293–299. https://doi.org/10.1001/jamainternmed.2013.1868 (2013).
Klein, R., Lee, K. E., Gangnon, R. E. & Klein, B. E. Relation of smoking, drinking, and physical activity to changes in vision over a 20-year period: the Beaver Dam Eye Study. Ophthalmology 121(6), 1220–1228. https://doi.org/10.1016/j.ophtha.2014.01.003 (2014).
Zhang, X., Kahende, J., Fan, A.Z., Li, Y., Barker, L., Thompson, T.J., Saaddine, J.B., & Mokdad, A.H. Peer reviewed: Smoking and visual impairment among older adults with age-related eye diseases. Prevent. Chronic Dis. 8(4). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3136979/ (2011).
Merle, B. M. J. et al. Unhealthy behaviours and risk of visual impairment: The CONSTANCES population-based cohort. Sci. Rep. 8, 6569 (2018).
Drinkwater, J. J., Davis, T. M. & Davis, W. A. Incidence and predictors of vision loss complicating type 2 diabetes: The Fremantle Diabetes Study Phase II. J. Diabetes Complic. 22, 107560. https://doi.org/10.1016/j.jdiacomp.2020.107560 (2020).
Klein, R., Peto, T., Bird, A. & Vannewkirk, M. R. The epidemiology of age-related macular degeneration. Am. J. Ophthalmol. 137(3), 486–495 (2004).
Ohgami, N., Kondo, T. & Kato, M. Effects of light smoking on extra-high-frequency auditory thresholds in young adults. Toxicol. Ind. Health 27(2), 143–147 (2011).
Nakanishi, N., Okamoto, M., Nakamura, K., Suzuki, K. & Tatara, K. Cigarette smoking and risk for hearing impairment: A longitudinal study in Japanese male office workers. J. Occup. Environ. Med. 1, 1045–1049 (2000).
de Oliveira, D. C. Low and high frequency tonal threshold audiometry: Comparing hearing thresholds between smokers and non-smokers. Braz. J. Otorhinolaryngol. 75(5), 738–744 (2009).
Gopinath, B. et al. The effects of smoking and alcohol consumption on age-related hearing loss: The Blue Mountains Hearing Study. Ear Hear. 31(2), 277–282 (2010).
Brandt, L. J. et al. Risk factors related to age-associated hearing loss in the speech frequencies. J. Am. Acad. Audiol. 7(3), 152–160 (1996).
Karlsmose, B., Lauritzen, T., Engberg, M. & Parving, A. A five-year longitudinal study of hearing in a Danish rural population aged 31–50 years. Br. J. Audiol. 34(1), 47–55 (2000).
Sumit, A. F. et al. Cigarette smoking causes hearing impairment among Bangladeshi population. PLoS ONE 10(3), e0118960 (2015).
Maroof, M., Ahmad, A., Khalique, N. & Ansari, M. A. Health problems among the aged: A community based study from urban Aligarh, Uttar Pradesh, India. Int. J. Commun. Med. Public Health 3, 944–947. https://doi.org/10.18203/2394-6040.ijcmph20160933 (2016).
Kohl, H. W. et al. Lancet Physical Activity Series Working Group. The pandemic of physical inactivity: global action for public health. Lancet 380(9838), 294–305. https://doi.org/10.1016/S0140-6736(12)60898-8 (2012).
Oh, I. H. et al. Hearing loss as a function of aging and diabetes mellitus: A cross sectional study. PLoS ONE 9(12), e116161 (2014).
Zhang, X. et al. Diabetes mellitus and visual impairment: National health and nutrition examination survey, 1999–2004. Arch. Ophthalmol. 126(10), 1421–1427 (2008).
CDC. Diabetes and Vision Loss. Centers for Disease Control and Prevention. https://www.cdc.gov/diabetes/managing/diabetes-vision-loss.html#:~:text=Thiscommoneyediseaseis,visionorstoppingbloodflow. (2021).
Agarwal, S., Mishra, A., Jagade, M., Kasbekar, V. & Nagle, S. K. Effects of hypertension on hearing. Indian J. Otolaryngol. Head Neck Surg. 65(3), 614–618 (2013).
Newman, C.W., & Sandridge, S.A. Hearing loss is often undiscovered, but screening is easy. Cleveland Clin. J. Med. 71(3), 225–232. https://mdedge-files-live.s3.us-east-2.amazonaws.com/files/s3fs-public/issues/articles/content_71_225.pdf (2004).
Jafari, Z., Kolb, B. E. & Mohajerani, M. H. Age-related hearing loss and tinnitus, dementia risk, and auditory amplification outcomes. Ageing Res. Rev. 1(56), 100963. https://doi.org/10.1016/j.arr.2019.100963 (2019).
Deepthi, R. & Kasthuri, A. Validation of the use of self-reported hearing loss and the Hearing Handicap Inventory for elderly among rural Indian elderly population. Arch. Gerontol. Geriatr. 55(3), 762–767. https://doi.org/10.1016/j.archger.2012.07.006 (2012).
Archana, G., Krishna, Y. & Shiny, R. Reasons for nonacceptance of hearing aid in older adults. Indian J. Otol. 22(1), 19. https://doi.org/10.4103/0971-7749.176513 (2016).
Pascolini, D. & Mariotti, S. P. Global estimates of visual impairment: 2010. Br. J. Ophthalmol. 96(5), 614–618. https://doi.org/10.1136/bjophthalmol-2011-300539 (2012).
Nirmalan, P. K. et al. Utilisation of eye care services in rural south India: The Aravind Comprehensive Eye Survey. Br. J. Ophthalmol. 88(10), 1237–1241. https://doi.org/10.1136/bjo.2004.042606 (2004).
Kumar, S. P. et al. Factors limiting the Northeast Indian elderly population from seeking cataract surgical treatment: Evidence from Kolasib district, Mizoram, India. Indian J. Ophthalmol. 66(7), 969. https://doi.org/10.4103/ijo.IJO_1184_17 (2018).
Lane, M. et al. Multiple deprivation, vision loss, and ophthalmic disease in adults: Global perspectives. Surv. Ophthalmol. 63(3), 406–436. https://doi.org/10.1016/j.survophthal.2017.10.009 (2018).
Tobin, J. Estimation of relationships for limited dependent variables. Econ. J. Econ. Soc. 1, 24–36 (1958).
Heckman, J. J. Sample selection bias as a specification error. Econ. J. Econ. Soc. 1, 153–161 (1979).
Srivastava, S., Sulaiman, K. M., Drishti, D. & Muhammad, T. Factors associated with psychiatric disorders and treatment seeking behaviour among older adults in India. Sci. Rep. 11(1), 1–3 (2021).
Building a Knowledge Base on Population Ageing in India (BKPAI). Report on the Status of Elderly in Select States of India. https://india.unfpa.org/sites/default/files/pub-pdf/AgeingReport_2012_F.pdf (2012).
Srivastava, S. & Gill, A. Untreated morbidity and treatment-seeking behaviour among the elderly in India: Analysis based on National Sample Survey 2004 and 2014. SSM-Popul. Health 1(10), 100557 (2020).
Rashid, M., Muhammad, T. & Srivastava, S. Back pain and treatment seeking among community-dwelling older adults: Findings from a population-based survey. Geriatr. Nurs. 42(6), 1446–1453 (2021).
Kumar, P. et al. Factors associated with gynaecological morbidities and treatment-seeking behaviour among adolescent girls residing in Bihar and Uttar Pradesh, India. PLoS ONE 16(6), e0252521 (2021).
Chiburis, R. & Lokshin, M. Maximum likelihood and two-step estimation of an ordered-probit selection model. Stand. Genomic Sci. 7(2), 167–182 (2007).
Miranda, A. & Rabe-Hesketh, S. Maximum likelihood estimation of endogenous switching and sample selection models for binary, ordinal, and count variables. Stand. Genomic Sci. 6(3), 285–308 (2006).
StataCorp. Stata Statistical Software: Release 16. https://www.stata.com/manuals13/rheckprobit.pdf (StataCorp LLC, 2019).
Crews, J. E. & Campbell, V. A. Vision impairment and hearing loss among community-dwelling older Americans: Implications for health and functioning. Am. J. Public Health 94(5), 823–829. https://doi.org/10.2105/AJPH.94.5.823 (2004).
Francesco, P. et al. Age-related hearing impairment—A risk factor and frailty marker dementia and AD. Nat. Rev. Neurol. 11(3), 157 (2015).
Kamil, R. J. et al. Association of hearing impairment with incident frailty and falls in older adults. J. Aging Health 28(4), 644–660 (2016).
Maharani, A., Pendleton, N. & Leroi, I. Hearing impairment, loneliness, social isolation, and cognitive function: Longitudinal analysis using English longitudinal study on ageing. Am. J. Geriatr. Psychiatry 27(12), 1348–1356 (2019).
Chakravarthy, U. et al. Clinical risk factors for age-related macular degeneration: A systematic review and meta-analysis. BMC Ophthalmol. 10(1), 31. https://doi.org/10.1186/1471-2415-10-31 (2010).
Thornton, J. et al. Smoking and age-related macular degeneration: A review of association. Eye 19(9), 935–944. https://doi.org/10.1038/sj.eye.6701978 (2005).
Ramulu, P. Y. et al. Fear of falling and visual field loss from glaucoma. Ophthalmology 119(7), 1352–1358. https://doi.org/10.1016/j.ophtha.2012.01.037 (2012).
Crews, J. E., Chou, C. F., Sekar, S. & Saaddine, J. B. The prevalence of chronic conditions and poor health among people with and without vision impairment, aged ≥ 65 years, 2010–2014. Am. J. Ophthalmol. 1(182), 18–30. https://doi.org/10.1016/j.ajo.2017.06.038 (2017).
Haslbeck, J. W., McCorkle, R. & Schaeffer, D. Chronic illness self-management while living alone in later life: A systematic integrative review. Res. Aging 34(5), 507–547. https://doi.org/10.1177/0164027511429808 (2012).
Kharicha, K., Iliffe, S., Harari, D., Swift, C., Gillmann, G., & Stuck, A.E. Health risk appraisal in older people 1: Are older people living alone an ‘at-risk’ group? Br. J. Gen. Pract. 57(537), 271–276. https://bjgp.org/content/57/537/271.short (2007).
Dandona R, Dandona L, Kovai V, Giridhar P, Prasad MN, Srinivas M. Population-based study of spectacles use in southern India. Indian J. Ophthalmol. 50(2), 145. http://www.ijo.in/text.asp?2002/50/2/145/14801 (2002).
Cherrier P, Jayanth B. Making eyeglasses accessible to the very poor: Creating a market in rural India. Field Actions Sci. Rep. J. Field Actions 3. https://journals.openedition.org/factsreports/355 (2009).
Raju Prema, R. G. et al. Comparison of refractive errors and factors associated with spectacle use in a rural and urban South Indian population. Indian J. Ophthalmol. 56(2), 139. https://doi.org/10.4103/0301-4738.39119 (2008).
Da Jung Jung, J. H., Kim, T., Kim, H. G., Lee, J. Y. & Lee, K. Y. Association between hearing impairment and albuminuria with or without diabetes mellitus. Clin. Exp. Otorhinolaryngol. 10(3), 221. https://doi.org/10.21053/ceo.2016.00787 (2017).
Gopinath, B. et al. Incidence and predictors of hearing aid use and ownership among older adults with hearing loss. Ann. Epidemiol. 21(7), 497–506. https://doi.org/10.1016/j.annepidem.2011.03.005 (2011).
Tahden, M. A., Gieseler, A., Meis, M., Wagener, K. C. & Colonius, H. What keeps older adults with hearing impairment from adopting hearing aids?. Trends Hear. https://doi.org/10.1177/2331216518809737 (2018).
Paul, A. & Verma, R. K. Does living arrangement affect work status, morbidity, and treatment seeking of the elderly population? A study of South Indian states. SAGE Open 6(3), 2158244016659528. https://doi.org/10.1177/2158244016659528 (2016).
Author information
Authors and Affiliations
Contributions
The concept was drafted by PK, SS, RP, SC, and SPM. PK and SS contributed to the analysis design. SC advised on the paper and assisted in paper conceptualization. SC, SPM, and RP contributed in the comprehensive writing of the article. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Marbaniang, S.P., Patel, R., Kumar, P. et al. Hearing and vision difficulty and sequential treatment among older adults in India. Sci Rep 12, 19056 (2022). https://doi.org/10.1038/s41598-022-21467-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-21467-y
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
