
Abstract
Females are known to have a better survival rate than males in the general population, but previous studies have shown that this superior survival is diminished in patients on dialysis. This study aimed to investigate the risk of mortality in relation to sex among Korean patients undergoing hemodialysis (HD) or peritoneal dialysis (PD). A total of 4994 patients with kidney failure who were receiving dialysis were included for a prospective nationwide cohort study. Cox multivariate proportional hazard models were used to determine the association between sex and the risk of cause-specific mortality according to dialysis modality. During a median follow-up of 5.8 years, the death rate per 100 person-years was 6.4 and 8.3 in females and males, respectively. The female-to-male mortality rate in patients on dialysis was 0.77, compared to 0.85 in the general population. In adjusted analyses, the risk of all-cause mortality was significantly lower for females than males in the entire population (hazard ratio [HR] 0.79, 95% confidence interval [CI] 0.71–0.87, P < 0.001). No significant differences in the risk of cardiovascular and infection-related deaths were observed according to sex. The risk of mortality due to sudden death, cancer, other, or unknown causes was significantly lower for females than males in the entire population (HR 0.66, 95% CI 0.56–0.78, P < 0.001), in patients on HD (HR 0.75, 95% CI 0.62–0.90, P = 0.003), and in patients on PD (HR 0.49, 95% CI 0.34–0.70, P < 0.001). The survival advantage of females in the general population was maintained in Korean dialysis patients, which was attributed to a lower risk of noncardiovascular and noninfectious death.
Trial registration: ClinicalTrials.gov Identifier: NCT00931970.
Similar content being viewed by others

Introduction
Females have a higher survival rate than males in the general population1, which may be related to a lower prevalence of cardiovascular risk factors and cardiovascular disease in females2,3. As differences in male and female physiology have been recognized, sex-specific distinctions have been widely reported for many diseases, including type 2 diabetes mellitus, cardiovascular disease, depression, acute kidney injury, chronic kidney disease, and kidney failure treated by dialysis4,5,6,7,8,9,10,11,12,13,14,15.
Previous analyses13,14,15,16, including studies from the Dialysis Outcomes and Practice Patterns Study (DOPPS) and the Austrian Dialysis Registry, have shown that the superior survival rate of females compared to males in the general population is not maintained in the dialysis population. This cancellation of the survival advantage for females was largely independent of differences in comorbidities or smoking status, and the reasons for this finding have not been fully understood. Considering that ethnicity, practice patterns, and accessibility to medical care could affect dialysis outcomes, it is important to investigate sex disparities in the survival of Asian patients on dialysis across countries.
This nationwide prospective cohort study in Korea aimed to investigate whether the survival benefit of females compared to males in the general population persist in the kidney failure population and to determine the association between sex and the risk of cause-specific mortality.
Results
Patient characteristics
Figure 1 shows the patient inclusion process. Among a total of 5244 incident and prevalent patients receiving dialysis, 63 patients who died within 90 days of dialysis initiation, 7 patients undergoing both HD and PD, and 180 patients with inadequate information for analysis were excluded from this study. Thus, a total of 3284 patients on HD and 1710 patients on PD were included in this study.

Flow chart of participant inclusion. Among a total of 5244 incident and prevalent patients receiving dialysis, 63 patients who died within 90 days of dialysis initiation, 7 patients undergoing both hemodialysis (HD) and peritoneal dialysis (PD), and 180 patients with inadequate information for analysis were excluded. Thus, a total of 3284 patients on HD and 1710 patients on PD were included in this study.
Baseline characteristics are provided in Table 1. In the entire study population, females had lower body mass index (BMI), a lower proportion of diabetes as the primary kidney disease, and fewer comorbidities than males. The proportion of incident patients was significantly higher among male patients than female patients and, accordingly, the dialysis vintage was significantly shorter in male patients than female patients. The rate of transition to transplantation did not differ between the two groups.
Causes of death
During the median follow-up of 5.8 (IQR 3.6–7.4) years, 678 (32.9%) and 1163 deaths (39.7%) occurred in females and males, respectively. The rate of death per 100 person-years was 6.4 in females and 8.3 in males in the entire population. The female-to-male mortality rate in patients on dialysis was 0.77, which was comparable to the 0.85 female-to-male mortality rate in the general population17. The rate of death per 100 person-years in the HD population was 6.9 in females and 8.2 in males. In the PD population, the rates were 5.4 in females and 8.6 in males (Fig. 2). Cardiovascular death was the most common cause of death in both dialysis modalities (Table 2).

Death event rates per 100 person-years in male and female patients according to dialysis modality. The rate was 6.4 in females and 8.3 in males in the entire population, 6.9 in females and 8.2 in males in the hemodialysis (HD) population, and 5.4 in females and 8.6 in males in the peritoneal dialysis (PD) population.
Risk of mortality by sex
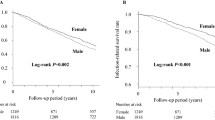
In the cumulative incidence curve, males had significantly more all-cause death events and noncardiovascular and noninfectious death events than females in the entire population, the HD population, and the PD population (Fig. 3).

Cumulative incidence curve for deaths in male and female patients according to dialysis modality. (A–C) Male patients had significantly more all-cause death events and (D–F) noncardiovascular and noninfectious death events than female patients in the entire population, hemodialysis (HD) population, and peritoneal dialysis (PD) population.
Cox multivariate proportional hazard models (Table 3) demonstrated that females had a significantly lower risk of all-cause death than males in the entire population (hazard ratio [HR] 0.79, 95% confidence interval [CI] 0.71–0.87, P < 0.001). The risk of mortality due to sudden death, cancer, other, or unknown causes was significantly lower for females than males in the entire population (HR 0.66, 95% CI 0.56–0.78, P < 0.001), in patients on HD (HR 0.75, 95% CI 0.62–0.90, P = 0.003), and in patients on PD (HR 0.49, 95% CI 0.34–0.70, P < 0.001) (Table 4). Multivariable regression analysis of the association between sex and mortality according to the type of population (incident or prevalent) showed consistent results (Supplementary Table S1). No significant differences in the risk of cardiovascular and infection-related deaths were observed according to sex.
Sex-specific factors for death and interaction analyses
Table 5 shows factors associated with all-cause mortality according to sex in the multivariate regression analysis. Older age at the time of dialysis initiation, the presence of diabetes, cardiovascular comorbidities, moderate to severe chronic liver disease, and lower level of serum albumin were independent risk factors for all-cause mortality in both females and males. Mild to severe malnutrition (adjusted HR 1.27, 95% CI 1.10–1.46, P = 0.001) was an independent risk factor for mortality in males, but not in females.
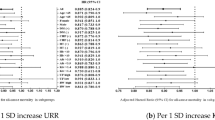
Interaction analyses (Fig. 4) showed that the risk of all-cause death (interaction P = 0.033) and noncardiovascular and noninfectious death (interaction P = 0.045) associated with diabetes was higher in female patients on PD than in male patients on PD. In addition, the risk of all-cause death associated with BMI was lower in male patients on HD than in female patients on HD (interaction P = 0.008).

(A) Analysis of sex interaction in the associations between patient characteristics and all-cause or (B) noncardiovascular and noninfectious death. The risk of all-cause mortality associated with diabetes was higher in female patients on peritoneal dialysis (PD) than male patients on PD (interaction P = 0.033). The risk of noncardiovascular and noninfectious death associated with diabetes was higher in female patients on PD than in male patients on PD (interaction P = 0.045).
Discussion
In this nationwide prospective cohort study, females with kidney failure receiving HD or PD exhibited a lower risk of death than males during a median follow-up of 6.3 years after extensive adjustment for demographic factors, cardiovascular and noncardiovascular comorbidities, laboratory findings, and nutritional status. The survival benefit of females on dialysis was mainly attributed to a lower risk of noncardiovascular and noninfectious death. Furthermore, factors associated with all-cause death differed in males and females with kidney failure. Mild to severe malnutrition and lower BMI were independent risk factors for mortality in males but not in females.
In contrast to the results from this Korean nationwide cohort study, previous studies13,14,15,16, including international dialysis cohort studies, have reported that the survival advantage of females compared to males in the general population is diminished in the HD population. Though the mortality of males surpassed that of females in the general population in all DOPPS countries, with male-to-female mortality rate ratios > 2 in certain countries, mortality rates were very similar for males and females in the HD population, with male-to-female mortality rate ratios close to 1 in all DOPPS countries except Japan14. The varying results may be explained by ethnicity, different practice patterns, differences in access to health care due to different insurance systems between countries, and various unadjusted biases. Previous studies explained that similar survival rates by sex in HD patients may be due to the mortality risk associated with diabetes, coronary artery disease, and cardiovascular disease14, or that non-cardiovascular disease18 was higher among adult females than male HD patients. Moreover, higher BMI, which is well known to be associated with better survival in HD patients19,20, was reported to be slightly less protective among females than males14. Cardiovascular mortality between male and female dialysis patients in our study was similar to previous studies. However, the risk of noncardiovascular and noninfectious death was significantly lower in females than males on both HD and PD. Although the exact mechanism of this result may be uncertain, it provides important information that care for cardiovascular infectious complications, as well as other medical conditions, including respiratory, liver, gastro-intestinal, and endocrine or hematological diseases may be more necessary, especially in male dialysis patients.
This current study found that factors associated with death differed between males and females with kidney failure. Mild to severe malnutrition was an independent risk factors for mortality in male, but not female, patients on dialysis. In this study, analysis of the sex interaction showed that the risk of all-cause death associated with BMI was lower in male patients on HD than in female patients on HD. Previous studies from the present Korean kidney failure cohort have reported that BMI or subjective global assessment (SGA) could be useful for predicting mortality in male patients on HD but not in female patients on HD21,22. A greater protective effect of higher BMI on survival in male patients on dialysis than female patients on dialysis could be explained by higher skeletal muscle mass and reduced fat mass associated with sex hormones in males23 and a sex-specific association of skeletal muscles mass and arterial stiffness in dialysis patients24. Although the exact mechanism of death being less influenced by nutritional status in female patients on dialysis than male patients on dialysis is unclear, the possibility of other complementary factors associated with reduced vulnerability to malnutrition in females compared to males cannot be completely excluded.
In previous studies including the general population, the negative effect of diabetes on cardiovascular death was greater in females than in males25,26. In this study, analysis of the sex interaction showed that the risk of all-cause and noncardiovascular and noninfectious death associated with diabetes was significantly higher in females on PD than in males on PD. Similarly, the European Renal Association European Dialysis and Transplant Association Registry demonstrated that females with diabetes on PD have a higher mortality risk than males on PD27. Considering that the impact of diabetes on death differed according to dialysis modality and sex, individualized advice according to sex may be required in determining the dialysis modality, and tailored care according to sex may also be required in the management of dialysis patients.
This present study has some limitations. First, although we tried to adjust for significant confounding factors, unadjusted variables may have persisted. Second, misclassification of the cause of death cannot be completely excluded because the cause of death coding did not undergo an external audit. Third, the results from the present study showed only a significant association between mortality and sex in dialysis patients, not causation. Fourth, as the baseline information was obtained at the time of enrollment and some information, such as BMI, comorbidities, laboratory data, and SGA scores, can change over time, the information at the time of dialysis initiation may be reflected in incident patients, but not prevalent patients. Finally, sex was determined based on medical records and no information was available on transgender or nonbinary patients. Nevertheless, this study has several strengths. First, though previous international cohort studies have reported sex-specific differences in HD patients, this study provided results from both HD and PD patients, which can have different clinical outcomes. Second, this study is the first prospective cohort including an Asian population with relatively long follow-up period.
In conclusion, female Korean incident and prevalent dialysis patients on HD and PD had a survival benefit compared to male patients during a median follow-up period of 6.3 years, mainly due to a lower risk of noncardiovascular and noninfectious death. This suggests that monitoring and management for cardiovascular or infectious complications, as well as other causes of death from cancer, pulmonary, hepatic, gastro-intestinal disease, endocrine or hematological disease, and suicide, may be necessary, especially in male dialysis patients.
Methods
Study population
A nationwide prospective observational cohort study was conducted in Korean patients with kidney failure (NCT00931970). Patients who were at least 19 years old and who had initiated maintenance dialysis due to kidney failure within 3 months or received dialysis due to kidney failure for more than 3 months were eligible for the study. Patients scheduled for a kidney transplantation within 3 months were excluded from the study.
Follow-up and outcomes
Incident or prevalent dialysis patients were enrolled from September 2008 to December 2013 and followed for the occurrence of death until December 2017. Patients were censored at the time of kidney transplantation. Cause of death was classified as all-cause, cardiovascular, or infection-related mortality, sudden death, cancer, other, or unknown. Cardiovascular death was defined as death from myocardial infarction, heart failure, arrhythmia, or stroke. Other causes of death included chronic obstructive lung disease, liver disease, gastro-intestinal disease, endocrine or hematological disease, and suicide.
Other variables
Baseline information at the time of enrollment included age, sex, dialysis modality, dialysis vintage, BMI, SGA scores, comorbidities, and laboratory data. Comorbid conditions included a history of diabetes, coronary artery disease, cerebrovascular disease, congestive heart failure, peripheral vascular disease, arrhythmia, hypertension, chronic lung disease, moderate-to-severe chronic liver disease, and malignancy. Laboratory data included hemoglobin, albumin, calcium, and phosphorus. Dialysis modality was defined as the modality 90 days after the first dialysis.
Statistical analysis
Data were expressed as mean ± standard deviation or median and interquartile range (IQR). Differences between groups were tested by independent sample t-tests and chi-squared tests as appropriate.
The Cox proportional hazard model adjusted for confounding factors was used to analyze the association between sex and mortality. Adjusted confounding factors included age, BMI, diabetes as the primary kidney disease, coronary artery disease, cerebrovascular disease, congestive heart failure, peripheral vascular disease, arrhythmia, hypertension, chronic lung disease, moderate-to-severe chronic liver disease, malignancy, hemoglobin, albumin, calcium, phosphorus, and SGA scores. Multivariable regression analysis was used to investigate the factors associated with all-cause mortality according to sex. The sex interaction in the association between patient characteristics and mortality was also analyzed.
Statistical analyses were performed using the SAS system for Windows, version 9.4 (SAS Institute Inc., Cary, NC) and R (R Foundation for Statistical Computing, Vienna, Austria; www.r-project.org). Significance was set at P < 0.05.
Ethics approval and consent to participate
All patients provided written informed consent before inclusion, and the Institutional Review Board of each center approved the study protocol (in alphabetical order: The Catholic University of Korea, Bucheon St. Mary’s Hospital; The Catholic University of Korea, Incheon St. Mary’s Hospital; The Catholic University of Korea, Seoul St. Mary’s Hospital; The Catholic University of Korea, St. Mary’s Hospital; The Catholic University of Korea, St. Vincent’s Hospital; The Catholic University of Korea, Uijeongbu St. Mary’s Hospital; Cheju Halla General Hospital; Chonbuk National University Hospital; Chonnam National University Hospital; Chung-Ang University Medical Center; Chungbuk National University Hospital; Chungnam National University Hospital; Dong-A University Medical Center; Ehwa Womans University Medical Center; Fatima Hospital, Daegu; Gachon University Gil Medical Center; Inje University Pusan Paik Hospital; Kyungpook National University Hospital; Kwandong University College of Medicine, Myongji Hospital; National Health Insurance Corporation Ilsan Hospital; National Medical Center; Pusan National University Hospital; Samsung Medical Center, Seoul; Seoul Metropolitan Governmalet, Seoul National University, Boramae Medical Center; Seoul National University Hospital; Seoul National University, Bundang Hospital; Yeungnam University Medical Center; Yonsei University, Severance Hospital; Yonsei University, Gangnam Severance Hospital; Ulsan University Hospital; Wonju Christian Hospital). All clinical investigations were conducted in accordance with the guidelines of the Declaration of Helsinki and the Good Clinical Practice guidelines.
Data availability
Data supporting the findings of the current study are available from the corresponding author upon reasonable request.
References
Murray, C. J. & Lopez, A. D. Mortality by cause for eight regions of the world: Global Burden of Disease Study. Lancet 349(9061), 1269–1276 (1997).
Isles, C. G., Hole, D. J., Hawthorne, V. M. & Lever, A. F. Relation between coronary risk and coronary mortality in women of the renfrew and paisley survey—comparison with men. Lancet 339(8795), 702–706 (1992).
Kardys, I., Vliegenthart, R., Oudkerk, M., Hofman, A. & Witteman, J. C. The female advantage in cardiovascular disease: Do vascular beds contribute equally?. Am. J. Epidemiol. 166(4), 403–412 (2007).
Meisinger, C. et al. Sex differences in risk factors for incident type 2 diabetes mellitus: The MONICA Augsburg cohort study. Arch. Intern. Med. 162(1), 82–89 (2002).
Perreault, L. et al. Sex differences in diabetes risk and the effect of intensive lifestyle modification in the Diabetes Prevention Program. Diabetes Care 31(7), 1416–1421 (2008).
Huxley, V. H. Sex and the cardiovascular system: The intriguing tale of how women and men regulate cardiovascular function differently. Adv. Physiol. Educ. 31(1), 17–22 (2007).
Safford, M. M. et al. Association of race and sex with risk of incident acute coronary heart disease events. JAMA 308(17), 1768–1774 (2012).
Piccinelli, M. & Wilkinson, G. Gender differences in depression. Crit. Rev. Br. J. Psychiatry. 177, 486–492 (2000).
Neugarten, J., Golestaneh, L. & Kolhe, N. V. Sex differences in acute kidney injury requiring dialysis. BMC Nephrol. 19(1), 131 (2018).
O’Brien, Z. et al. Sex and mortality in septic severe acute kidney injury. J Crit Care. 49, 70–76 (2019).
Carrero, J. J. Gender differences in chronic kidney disease: Underpinnings and therapeutic implications. Kidney Blood Press Res. 33(5), 383–392 (2010).
Carrero, J. J., Hecking, M., Chesnaye, N. C. & Jager, K. J. Sex and gender disparities in the epidemiology and outcomes of chronic kidney disease. Nat. Rev. Nephrol. 14(3), 151–164 (2018).
Carrero, J. J. et al. Sex differences in the impact of diabetes on mortality in chronic dialysis patients. Nephrol. Dial. Transplant. 26(1), 270–276 (2011).
Hecking, M. et al. Sex-specific differences in hemodialysis prevalence and practices and the male-to-female mortality rate: The dialysis outcomes and practice patterns study (DOPPS). PLoS Med. 11(10), e1001750 (2014).
Kainz, A. et al. Sex-specific analysis of haemodialysis prevalence, practices and mortality over time: The Austrian Dialysis Registry from 1965 to 2014. Nephrol. Dial. Transplant. 34(6), 1026–1035 (2019).
Villar, E., Remontet, L., Labeeuw, M. & Ecochard, R. Effect of age, gender, and diabetes on excess death in end-stage renal failure. J. Am. Soc. Nephrol. 18(7), 2125–2134 (2007).
Causes of Death Statistics in 2017 - Statistics Korea. https://kostat.go.kr/portal/korea/kor_nw/1/6/2/index.board. Accessed on November 18, 2021.
Carrero, J. J. et al. Cardiovascular and noncardiovascular mortality among men and women starting dialysis. Clin. J. Am. Soc. Nephro. 6(7), 1722–1730 (2011).
Leavey, S. F. et al. Body mass index and mortality in “healthier” as compared with “sicker” haemodialysis patients: Results from the Dialysis Outcomes and Practice Patterns Study (DOPPS). Nephrol. Dial. Transplant. 16(12), 2386–2394 (2001).
Kalantar-Zadeh, K., Abbott, K. C., Salahudeen, A. K., Kilpatrick, R. D. & Horwich, T. B. Survival advantages of obesity in dialysis patients. Am. J. Clin. Nutr. 81(3), 543–554 (2005).
Park, J. M. et al. Survival in patients on hemodialysis: Effect of gender according to body mass index and creatinine. PLoS ONE 13(5), e0196550 (2018).
Ko, Y. E. et al. Gender-specific discrepancy in subjective global assessment for mortality in hemodialysis patients. Sci. Rep. 8(1), 17846 (2018).
Kelly, D. M. & Jones, T. H. Testosterone and obesity. Obes. Rev. 16(7), 581–606 (2015).
Liu, X. et al. Gender-specific associations of skeletal muscle mass and arterial stiffness among peritoneal dialysis patients. Sci. Rep. 8(1), 1351 (2018).
Lee, W. L., Cheung, A. M., Cape, D. & Zinman, B. Impact of diabetes on coronary artery disease in women and men: A meta-analysis of prospective studies. Diabetes Care 23(7), 962–968 (2000).
Juutilainen, A. et al. Gender difference in the impact of type 2 diabetes on coronary heart disease risk. Diabetes Care 27(12), 2898–2904 (2004).
van de Luijtgaarden, M. W. et al. Effects of comorbid and demographic factors on dialysis modality choice and related patient survival in Europe. Nephrol. Dial. Transplant. 26(9), 2940–2947 (2011).
Acknowledgements
We would like to express our gratitude to the investigators of the Clinical Research Center for End Stage Renal Disease (CRC for ESRD) in Korea.
Funding
This research was supported by a grant from the Korea Health Technology R&D Project through the Korea Health Industry Development Institute, which is funded by the Ministry of Health and Welfare, Republic of Korea (HC15C1129, HI15C0001). The funder had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
Conceptualization, H.Y.J. and Y.L.K.; methodology, H.Y.J., Y.J., and Y.L.K.; formal analysis, H.Y.J., Y.J., and Y.L.K.; investigation, H.Y.J., Y.S.K., S.W.K., C.W.Y., N.H.K., H.W.N., S.J.J., J.H.L., J.Y.C., J.H.C., S.H.P., C.D.K., and Y.L.K.; data curation, H.Y.J., Y.S.K., S.W.K., C.W.Y., N.H.K., J.H.C., S.H.P., C.D.K., and Y.L.K.; funding acquisition, Y.L.K.; writing—original draft preparation, H.Y.J.; writing—review and editing, H.Y.J. and Y.L.K.; approval of final manuscript: all authors.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Jung, HY., Jeon, Y., Kim, Y.S. et al. Sex disparities in mortality among patients with kidney failure receiving dialysis. Sci Rep 12, 18555 (2022). https://doi.org/10.1038/s41598-022-16163-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-16163-w
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
