
Abstract
Cognitive impairment and dementia are age-related major public health concerns in the elderly population. It is a major cause of disability, dependency, and poor quality of life. However, in Ethiopia, the magnitude of this cognitive impairment among the elderly community was not investigated. Hence, this study sought to determine the prevalence of cognitive impairment and associated factors among mature and older adults living in the community of Gondar town, Ethiopia, in 2020. A community-based cross-sectional study was conducted at Gondar town, from February 20 to April 30, 2020. Using a single-stage cluster sampling technique, 403 study participants were recruited. Data was collected by a pretested interviewer-administered structured questionnaire which consisting of sociodemographic variables, the Oslo Social Support Scale, and a Standardized Mini-mental State Examination (SMMSE) tool. Epi data version 3.0 was used to enter coded data and then exported into STATA 14 for analysis. Variables with a p-value < 0.25 in the bi-variable logistic regression were included in the multivariable regression. From multivariable logistic regression, variables having a p-value ≤ 0.05 were declared as statistically significant variables. In this study, a total of 403 study participants were involved, and 393 (97.5%) of them completed the survey. Among older participants screened for cognitive impairment, 43.8% was positive for cognitive impairment with a 95% CI (38.8–48.7%). The majority of the participants were (57.5%) male and (44.8%) aged over 60 years. After adjustment, the variables associated with cognitive impairment were age ≥ 75 years [odds ratio (OR) = 7.03, 95% CI 2.78–17.77] and between 61 and 74 years [OR = 3.18, 95% CI 1.81–5.59], and unable to read and write [OR = 5.05, 95% CI 2.04–12.50], low income level [OR = 2.60, 95% CI 1.26–5.20], being female [OR = 2.52, 95% CI 1.50–4.26], poor social support [OR = 2.50, 95% CI 1.30–4.81], and rural residence [OR = 2.39, 95% CI 1.26–4.51]. The prevalence of older participants who screened positively for cognitive impairment was high at Gondar town. The independent predictors of cognitive impairment among older individuals were older age, being unable to read and write, being female, low income, poor social support, and rural dwelling. Therefore, routine screening and social support, as well as free healthcare services for the mature and older community, are needed. Moreover, we strongly recommend the next researcher to use a diagnosis tool to estimate the actual prevalence of the problems among older people.
Similar content being viewed by others

Introduction
Cognitive impairment is defined as difficulty recalling, learning new things, focusing, or making decisions that affect one’s daily life1. It affects the orientation, attention, reasoning, memory, language, and executive functions of individuals2. Those affected elderly people had poor concentration, a short attention span, emotional disturbance3, and impairment of recent memory4,5.
Cognitive impairment and dementia are common age-related health problems among older people6. The proportion of older people is increasing in every country. By 2050, around two billion people worldwide will be aged 60 years or over7. Currently, around 50 million people live with a severe form of cognitive impairment worldwide, 60% of whom are from developing countries. Every year, around 10 million people are diagnosed with dementia8,9. The prevalence of severe cognitive impairment is expected to be 82 million in 2030 and 152 million by 20508,10. The problem is increasing worldwide and predicted to increase consistently more in developing countries11.
According to the 2007 census, 9% of the population in Ethiopia was aged ≥ 50 years, which is estimated to increase progressively12. Currently, family caregivers for elderly relatives in Ethiopia are generally poor13 and only half a million older people receive regular public sector pensions14.
The prevalence of cognitive impairment among older individuals was (42%) in French15, (28.5%) in Congo11, (37.9%) in the Central African Republic16, (20.9%) in Nigeria17, and (33.3%) in Cameroon6.
Cognitive impairments have health, psychological, social, and economic impacts. Its impact on health3,5,6 was increased rates of hospitalization, disability, and risk of falls. In addition, individuals with cognitive impairment have an increased risk of death, poor quality of life, worse quality of emotional well-being, and longer hospitalizations3,18,19. Severe cognitive impairment is now the seventh leading cause of death in all diseases20. Severe cognitive impairment deaths in Ethiopia reached 8316, or 1.36% of total deaths. The age-adjusted death rate is 24.48 per 100,000 population, which ranks Ethiopia 92th in the world21.
Stigma, dependency, and discrimination are also common psychological and social problems among people with severe cognitive impairment10,22. Severe cognitive impairments have an impact not only on the people living with severe cognitive impairment, but also on their caregivers, families, and society at large20. Informal caregivers, such as family members and friends, spend an average of five hours per day caring for people with dementia. These physical, emotional, and financial pressures can cause great stress to families and caregivers22.
According to the World Health Organization, the annual cost of caring for people with severe cognitive impairments will reach two trillion dollars by 20308,9,22.
Around 90% of people with severe cognitive impairment in low and middle-income countries do not obtain a diagnosis for this disorder9. In Ethiopia, cognitive impairment is expected to increase as the life expectancy of the population increases. Even though the burden of this health problem is huge, the prevalence and associated factors of cognitive impairment were not investigated among older communities in Ethiopia. Therefore, this study is aimed at investigating the prevalence of cognitive impairment and associated factors among mature and older adults living in the community of Gondar, Ethiopia, in 2020.
Methods and materials
Study area and period
A community-based cross-sectional study was conducted in Gondar town, from February 20 to April 30, 2020. Gondar town is located 750 km away from Addis Ababa (the capital city of Ethiopia) in the north-west direction. It is one of the ancient and densely populated towns in Ethiopia. According to a 2007 Ethiopian Central Statistical Agency office report, around 206,987 people are living in the town23.
Study population
All older people aged 50 years or above were included in this study.
Inclusion and exclusion criteria
All adults aged 50 years or older whose residence was in the selected kebeles were included in the study.
In this study, all elderly participants with hearing, visual, and speaking difficulties were excluded from the study.
Sample size determination
The sample size was estimated using a single population proportion formula by assuming a 50% prevalence of cognitive impairment, since there was no study conducted before in Ethiopia, a 95% confidence interval, and a 5% marginal error.
N = sample size, Zα/2 (1.96) = critical value at 95% confidence interval, p = expected estimates of prevalence value of cognitive impairment (50%), d = Margin of sampling error (5%). After adding 5% of the non-response rate, a total of 403 participants were selected.
Sampling procedures
A single-stage cluster sampling technique was employed to recruit the study participants. In Gondar town, there are 22 kebeles, which we considered as a cluster. From those 22 kebeles, (kebele 6, kebele 7, kebele 8, kebele 9, kebele 13, kebele 15, kebele 16, kebele 17, kebele 18, kebele 20) were randomly selected by using the lottery method. Then all adults with aged 50 years or above whose residences were in those selected kebeles were included in the study.
This study was conducted under the principle of the Helsinki Declaration. Ethical clearance was obtained from the Institutional Review Board of the University of Gondar. During the data collection period, the aim of the study was explained for each participant. Written informed consent was obtained from each study participant before we started the data collection process. The privacy and confidentiality of participant information were also kept properly.
Study variables
Dependent variable cognitive impairment (yes/no).
Independent variables;
Socio-demographic variables (age, sex, residence, social support, monthly income, marital status, and educational status).
Lifestyle and medical history related variables: substance use (khat chewing, cigarette smoking, and alcohol intake), overweight or underweight.
Operational definitions
In our study, mature and older adult was defined as being 50 years of age or above6.
Cognitive impairment
Using the Standardized Mini Mental State Examination (SMMSE) tool, participants with an educational level of ≤ grade 8 with scores of ≤ 22 and participants with an educational level of ≥ grade 9 with scores of ≤ 24 out of a total of 30 scores , had cognitive impairment24,25.
The stage of cognitive impairment was classified as a score of 20–24 as mild cognitive impairment, a score of 10–19 as moderate cognitive impairment, and a score of 0–9 as severe cognitive impairment for participants with ≥ 9 grade, and a score of 18–22 as mild, 8–17 as moderate, and 0–7 as severe cognitive impairment for participants with ≤ 8 grade24,25.
Social support
Using the Oslo Social Support Scale, participants who scored 3–8, 9–11, 12–14 points out of a total score had poor social support, moderate social support, and strong social support, respectively26.
Substance use
Khat chewers or cigarette smokers are those participants who had used khat or cigarettes in the previous month, while those individuals who had consumed alcohol that could cause intoxication in the previous month were alcohol drinkers27,28.
Body mass index (BMI)
Participants with BMI of < 18.5 kg/m2, (18.5–24.9 kg/m2), (25–29.9 kg/m2), ≥ 30 kg/m2 were classified as underweight, normal, overweight and obese, respectively27.
Data collection procedure and tools
An interviewer-administered structured questionnaire, which consists of socio-demographic variables, substance use, weight and height measurement, the Oslo Social Support Scale (OSSS), and a standardized mini mental state examination tool (SMMSE tool), was used to collect the data24,29. House to house survey was undertaken to collect the data. A SMMSE is a validated tool that is used for screening the cognitive status of the participants. The mean duration for assessments of the cognitive status of participants by SMMSE was 11 min. The tools consist of questions that evaluate orientation, attention, orientation, registration, calculation, recall, language, and praxis parts of cognition, which result in a total of 30 scores when summed. The total score for each participant was adjusted according to the educational level of the participants24. The inability to read and write was taken into account when scoring the test for those participants who had omitted items due to being unable to read and write. The score from this task was subtracted from the total score of 30 to give a new total. The person’s score was then adjusted to the new total score30.
The Oslo Social Support Scale (OSSS) tool was used to assess the social support level of study participants. It consists of three items scored out of 14; one item (4 points) and the remaining two items (5 points each)26.
Moreover, weight and height were measured using a weighing machine and a height-measuring stand to the nearest 0.1 cm and 0.1 kg, respectively. The scale was adjusted to a zero level between individual measurements.
Data processing and analysis
After the data have been checked for its completeness and coded, it is entered into Epi Data Version 3.0 and exported to STATA 14 for analysis. For categorical variables, descriptive statistics such as frequency, percentage, and bar graphs were used, whereas mean and standard deviation were used for continuous variables. Bi-variable and multivariable logistic regression analyses were done. In bi-variable logistic regression, variables associated with cognitive impairment at p-value < 0.25 were included in the multivariable regression model. Lastly, using a 95% confidence interval, variables having a p-value ≤ 0.05 in multivariable logistic regression were confirmed as significantly associated with cognitive impairment.
Model fitness was checked by the Hosmer and Lemeshow goodness of test (at p > 0.05) and multi-collinearity was also tested by variance inflation factor (VIF). Moreover, a commonly used cognitive impairment screening tool (SMMSE) was used to assess the cognitive status of the participants with a sensitivity and specificity of 81% and 94%, respectively31. The instrument's reliability was also established based on an internal consistency reliability assessment using Cronbach’s alpha (= 0.8), indicating that the tool is reliable.
Data quality assurance
To assure the quality of the data, training was given by the principal investigator to the data collectors with regard to the SMMSE tool and the procedure for height and weight measurement. For the consistency of the questionnaire, after it was translated to Amharic language by a language expert again retranslated back to English language by another expert. A pretest was conducted among 40 participants in Bahirdar town, then the questionnaire was amended accordingly. The supervisor and principal investigator supervised the data collectors during the data collection period. Protective materials and physical distance were applied by the data collectors during data collection for the prevention of COVID-19 transmission.
Results
Sociodemographic characteristics of study participants
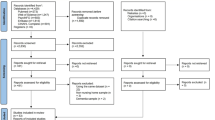
In this study, a total of 393 participants were involved, with a 97.5% response rate. The mean age of study participants was 63.6 years and 50 and 92 years were the minimum and maximum ages, respectively. Most of the study participants were male (66%), orthodox Christian followers (86.2%), attended primary school or less (42%), married (82%), and employed (34.9%). In this study, 5 (1.3%), 63 (16%), and 2 (0.5%) of the participants were khat chewers, alcohol users, and cigarette smokers, respectively. Those substance users used at least half a gram of khat and one stick of cigarate per month, and 2–3 L of alcohol per week (Table 1).
Prevalence of cognitive impairment among elderly community
The mean standardized mini-mental state examination score of the study participants was 23.3 (standard deviation ± 0.24).
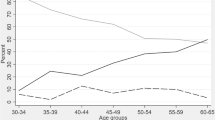
Among older participants screened for cognitive impairment, 43.8% was positive for cognitive impairment with a 95% CI (38.8–48.7%). Most of them, 21.9% had moderate cognitive impairment (Fig. 1).

Stage of cognitive impairment among mature and older adults living in the community of Gondar town, Ethiopia, 2020.
Factors associated with cognitive impairment in the elderly population
In binary logistic regression, age, sex, educational level, income level, social support, and body mass index were associated with cognitive impairment at a p-value < 0.25. However, in the multivariable logistic regression analysis, low educational level, female sex, poor social support, rural residence, low income, and older age were variables significantly associated with cognitive impairment at p-value ≤ 0.05. The odds of developing cognitive impairment among the elderly community with an age of ≥ 75 years was 7.03 times [AOR = 7.03, 95% CI 2.78–17.77] higher than those individuals with an age between 50–60 years. The odds of developing cognitive impairment among elderly females was 2.52 times [AOR = 2.52, 95% CI 1.5–4.26] higher than males. The odds of developing cognitive impairment among elderly individuals who had poor social support was 2.50 times [AOR = 2.50, 95% CI 1.30–4.80] higher than those individuals who had strong social support. The odds of developing cognitive impairment among rural residents was 2.4 times [AOR = 2.4, 95% CI 1.26–4.51] higher than those of urban residents. The odds of developing cognitive impairment among the elderly participants with an income level of ≤ 1500 ETB was 2.6 times [AOR = 2.6, 95% CI 1.26–5.20] higher than those participants with an income level of ≥ 3501 Ethiopian birr (Table 2).
Discussion
This research aimed to determine the magnitude of cognitive impairment and associated factors among mature and older adults living in the community of Gondar town.
Among mature and adult older participants screened for cognitive impairment, 43.8% was positive for cognitive impairment with a 95% CI (38.8–48.7%) which was higher than the studies done in Cameroon (33.3%)6, the Central Africa Republic (37.9%)16, Nigeria (19.7%)17, India (14%)32 and the Republic of Congo (28.5%)16. This variation might be due to the tool used to assess cognitive impairment. Community screening interview for dementia tool was used for Central Africa republic and Republic of Congo studies. In a study done in Nigeria, intervention for dementia in elderly Africans with cognition screening tools was used. It might also be due to the socio-demographic difference of study participants, in which in those studies, the participants had attained higher education.
As expected, different factors were capable of predicting cognitive impairment. In this study, getting older was associated with cognitive decline. This finding is in line with studies done in Cameroon6, Jamaica5, and Ethiopia27. The reason might be that as aging increase there is a decrement in neurotransmitters, gray matter volume, and neocortical synapses that result in cognitive impairment33,34,35. During aging the cerebrovascular reactivity is impaired, which result in brain hypoperfusion36. In addition to this, as age increases, there is deterioration in thinking, reasoning, and memory which is related to cognitive decline37,38.
Individuals who were unable to read and write were more likely to develop cognitive impairment than individuals attaining college and above, which is supported by other studies5,39,40. This might be due to education improving cognitive function through providing knowledge, understanding, skills, and experience39,40. It also promote cognitive function by increasing the number of synapse, vascularization, and promote neural development39,41.
In support of other studies6,41, low income level was significantly associated with cognitive impairment. It might be due to the inability to afford health care services for those participants with low income. Being female was associated with higher odds of developing cognitive impairment, which is similar to the finding of other studies6,11. This might be because of estrogen, progesterone, and testosterone hormones decline in women during menopause. Studies have shown that those hormones have a protective effect on the brain. They also reduce the level of amyloid beta peptide, which is negatively acting on the hippocampus6,42.
The odds of developing cognitive impairment among elderly individuals who had poor social support was higher than those individuals who had strong social support. This coincides with the studies conducted in Spain43 and Japan44. Social support influences both physical and mental health. Hence, those individuals with poor social support are more likely to develop cognitive impairment. It is hypothesized that poor social support associated with stress leads to corticosterone hypersecretion, which in turn leads to permanent loss of hippocampal neurons45.
Lastly, those individuals who are rural dwellers have a higher probability of developing cognitive impairment than elderly urban dwellers. This result is similar to studies conducted in China46 and India47. This might be due to an increase in educational and income levels among urban residents, which may lead to increased health-seeking behavior.
The findings of this research imply that cognitive impairment is becoming one of the health problems among adult and mature older community in Ethiopia.
Limitations of the study
A SMMSE is a screening tool that cannot be used for the diagnosis of the outcome variable. Therefore, those participants might need further evaluation to confirm the problem. Moreover, since this study used a cross-sectional study design, it doesn’t show a cause and effect relationship.
Conclusions
The prevalence of older participants who screened positively for cognitive impairment was high at Gondar town. The independent predictors of cognitive impairment among older individuals were older age, being unable to read and write, being female, low income, poor social support, and rural dwelling. Therefore, routine screening and social support, as well as free healthcare services for the mature and older community, are needed. Moreover, we strongly recommend the next researcher to use a diagnosis tool to estimate the actual prevalence of the problems among older people.
Data availability
The data will be available upon request from the corresponding author.
Abbreviations
- CI:
-
Confidence interval
- SMMSE:
-
Standardized Mini Mental State Examination
References
Putkonen, P. et al. Cognitive impairment. AIDS 6, 257–263 (2011).
Berger, I. et al. Cognition in chronic kidney disease: A systematic review and meta-analysis. BMC Med. 14, 1–10 (2016).
Johansson, M. Cognitive impairment and its consequences in everyday life. Neurology 9, 23–30 (2015).
Anderson, L. Cognitive Impairment: The Impact on Health in Florida (CDC, 2011).
Waldron, N. et al. The prevalence of cognitive impairment among older adults in Jamaica. WIMJ Open https://doi.org/10.7727/wimjopen.2014.003 (2015).
Tianyi, F. L., Agbor, V. N., Njamnshi, A. K. & Atashili, J. Factors associated with the prevalence of cognitive impairment in a rural elderly cameroonian population: A community-based study in sub-saharan Africa. Dement. Geriatr. Cogn. 47, 104–113 (2019).
WHO. Promoting Dementia-Inclusive Communities 1–50 (2020).
Guidelines, W. H. O. Risk Reduction of Cognitive Decline and Dementia. (2019).
WHO. Meeting on the Implementation of the Global Action Plan on the Public Health Response to Dementia 2017–2025 (WHO, 2018).
Towards a dementia-inclusive society towards a dementia inclusive society.
Angelique, M., Powell, J. & Thorogood, M. Prevalences of dementia and cognitive impairment among older people in sub-Saharan Africa: A systematic review. Bull World Health Organ 91, 773–783 (2013).
Ethiopian, P., From, D., Suite, S. & Models, O. F. Projecting Ethiopian demographics from 2012–2050 using the spectrum suite of models. (2014).
Bassah, N., Ubenoh, U. S. & Palle, J. N. An exploratory study of the knowledge and practices of family caregivers in the care of the elderly at home in the Buea Health District, Cameroon. J. Gerontol. Geriatr. Res. 07, 3–7 (2018).
Baleher, A. Regional Workshop on Ageing and Poverty E T H I O P I A Country position paper. (2003).
Artero, S. et al. Risk profiles for mild cognitive impairment and progression to dementia are gender specific. J. Neurol. Neurosurg. Psychiatry 79, 979–984 (2008).
Guerchet, M. et al. Prevalence of dementia in elderly living in two cities of central Africa: The EDAC survey. Dement. Geriatr. Cogn. Disord. 30, 261–268 (2010).
Adebiyi, A. O., Ogunniyi, A., Adediran, B. A., Olakehinde, O. O. & Siwoku, A. A. Cognitive impairment among the aging population in a community in southwest Nigeria. Health Educ. Behav. 43, 93S-99S (2015).
Plassman, B. L. et al. Prevalence of cognitive impairment without dementia in the United States. Ann. Intern. Med. 148, 427–434 (2008).
Sampson, E. L., Burns, A. & Richards, M. Improving end-of-life care for people with dementia. Br. J. Psychiatry 199, 357–359 (2011).
WHO. Global status response to public health report on the dementia. (2021).
Tolera, G. D. Psychology, autism and Alzheimer’s disease. J. Alzheimers Dis. Park. 3, 84 (2013).
WHO. A Handbook on How to Implement mDementia. (2021).
Statistical, C. 2007 Population and Housing Census of Ethiopia Administrative Report (Central Statistical Authority Addis Ababa, 2012).
Vertesi, A. et al. Standardized mini-mental state examination. Use and interpretation. Can. Fam. Physician 47, 2018–2023 (2001).
Gugssa, S. A. et al. Population norms for the mini-mental state examination in Ethiopia. Ethiop. Med. J. 49, 239–247 (2011).
Kocalevent, R. D. et al. Social support in the general population: Standardization of the Oslo social support scale (OSSS-3). BMC Psychol. 6, 4–11 (2018).
Gela, Y. Y. et al. Cognitive impairment and associated factors among chronic kidney disease patients: A comparative cross-sectional study. Neuropsychiatr. Dis. Treat. 17, 1483–1492 (2021).
Yeshaw, Y. & Mossie, A. Depression, anxiety, stress, and their associated factors among Jimma University staff, Jimma, Southwest Ethiopia, 2016: a cross-sectional study. Neuropsychiatr. Dis. Treat. 13, 2803–2812 (2017).
Molloy, D. D. W. & Clarnette, D. R. Standrdized Minimental State Examination (New Grange Press, 1999).
Molloy, D. W. Standardised mini-mental state examination (SMMSE)|IHPA. Am. J. Psychiatry 14, 102–105 (1991).
Sleutjes, D. K. L. et al. Validity of the mini-mental state examination-2 in diagnosing mild cognitive impairment and dementia in patients visiting an outpatient clinic in the Netherlands. Alzheimer Dis. Assoc. Disord. 34, 278–281 (2020).
Jadenur, S. S., Saroja, A. O., Kari, A. & Angolkar, M. Prevalence of cognitive impairment among people aged ≥ 50 years in rural population of Belagavi Taluka—A community based cross sectional study. Clin. Epidemiol. Glob. Health 13, 100940 (2022).
Legdeur, N. et al. Age dependency of risk factors for cognitive decline. BMC Geriatr. 18, 1–10 (2018).
Terry, R. D. & Katzman, R. Life span and synapses: Will there be a primary senile dementia?. Neurobiol. Aging 22, 347–348 (2001).
Harada, C. N., Natelson Love, M. C. & Triebel, K. L. Normal cognitive aging. Clin. Geriatr. Med. 29, 737–752 (2013).
Georgiadis, D. et al. Cerebrovascular reactivity is impaired in patients with cardiac failure. Eur. Heart J. 21, 407–413 (2000).
Deary, I. J. et al. Age-Associated Cognitive Decline. 135–152 (2009). https://doi.org/10.1093/bmb/ldp033
Habte, E. & Tekle, T. Cognitive functioning among elders with symptoms of depression: The case of two selected institutionalized care centers in Addis Ababa, Ethiopia. Health Sci. J. 12, 1–7 (2018).
Zahodne, L. B., Stern, Y. & Manly, J. J. Differing effects of education on cognitive decline in diverse elders with low versus high educational attainment. Neuropsychology 29, 649–657 (2015).
Parisi, J. M. et al. The role of education and intellectual activity on cognition. J. Aging Res. 2012, 20–24 (2012).
Lee, S., Buring, J. E., Cook, N. R. & Grodstein, F. The relation of education and income to cognitive function among professional women. Neuroepidemiology 26, 93–101 (2006).
Li, R. & Singh, M. Sex differences in cognitive impairment and Alzheimer’ s disease. Front. Neuroendocrinol. https://doi.org/10.1016/j.yfrne.2014.01.002 (2014).
Millán-Calenti, J. C., Sánchez, A., Lorenzo-López, L., Cao, R. & Maseda, A. Influence of social support on older adults with cognitive impairment, depressive symptoms, or both coexisting. Int. J. Aging Hum. Dev. 76, 199–214 (2013).
Murata, C., Saito, T., Saito, M. & Kondo, K. The association between social support and incident dementia: A 10-year follow-up study in Japan. Int. J. Environ. Res. Public Health 16, 239 (2019).
Rashid, A., Manan, A. A. & Rohana, S. The influence of social support on cognitive impairment in the elderly. Australas. Med. J. 9, 262–269 (2016).
Xu, H., Dupre, M. E., Gu, D. & Wu, B. The impact of residential status on cognitive decline among older adults in China: Results from a longitudinal study. BMC Geriatr. 17, 1–11 (2017).
Xu, H., Ostbye, T., Vorderstrasse, A. A., Dupre, M. E. & Wu, B. Place of residence and cognitive function among the adult population in India. Neuroepidemiology 50, 119–127 (2018).
Acknowledgements
The authors thank the University of Gondar for its support in conducting this study. We also acknowledged the data collector and the study participants for their enthusiasm and collaboration.
Author information
Authors and Affiliations
Contributions
Y.Y.G. made a significant contribution during conception, design of the work, methodology, analysis, data interpretation, and writing the final manuscript. S.A.F., Y.B., Y.A., B.D., M.G., M.A.S., and M.D. equally contributed to the analysis and interpretation of the data, drafted the manuscript, and substantively revised the work. All authors read and approved the final manuscript to be submitted to the current journal; and also agreed to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Gela, Y.Y., Fekadu, S.A., Belsti, Y. et al. Cognitive impairment and associated factors among mature and older adults living in the community of Gondar town, Ethiopia, 2020. Sci Rep 12, 7545 (2022). https://doi.org/10.1038/s41598-022-11735-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-11735-2
This article is cited by
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
