
Abstract
Inhaled corticosteroids (ICS) have been associated with increased risk of pneumonia. Their impact on respiratory virus infections is unclear. We performed a post-hoc analysis of the FLUVAC cohort, a multicenter prospective cohort study of adults hospitalized with influenza-like illness (ILI) during six consecutive influenza seasons (2012–2018). All patients were tested for respiratory virus infection by multiplex PCR on nasopharyngeal swabs and/or bronchoalveolar lavage. Risk factors were identified by logistic regression analysis. Among the 2658 patients included, 537 (20.2%) were treated with ICS before admission, of whom 282 (52.5%, 282/537) tested positive for at least one respiratory virus. Patients on ICS were more likely to test positive for non-influenza respiratory viruses (25.1% vs. 19.5%, P = 0.004), especially for adenovirus (aOR 2.36, 95% CI 1.18–4.58), and respiratory syncytial virus (aOR 2.08, 95% CI 1.39–3.09). Complications were reported in 55.9% of patients on ICS (300/537), primarily pneumonia (171/535, 32%). Among patients on chronic ICS who tested positive for respiratory virus, 14.2% (40/282) were admitted to intensive care unit, and in-hospital mortality rate was 2.8% (8/282). Chronic use of ICS is associated with an increased risk of adenovirus or RSV infections in patients admitted for ILI.
Similar content being viewed by others
Introduction
Inhaled corticosteroids (ICS) are commonly used for the treatment of various chronic respiratory diseases, including asthma, and chronic obstructive pulmonary diseases (COPD)1. In 2018, the number of patients with COPD or asthma was estimated at 600 million worldwide2,3,4. A recent study showed an association between chronic respiratory diseases, and the risk of non-influenza respiratory virus (NIRV) infections, but did not address ICS use5. Several randomized studies demonstrated that appropriate use of ICS improves respiratory function and quality of life, and reduces the risk of exacerbations6. However, chronic use of ICS has been associated with an increased risk of pneumonia7,8,9,10,11. Few studies evaluated the risk of viral infections in patients with chronic use of ICS. A landmark study demonstrated that ICS inhibit antiviral activity in situ, leading to delayed virus clearance and increased bacterial load during COPD exacerbations12. However, clinical data on the potential association between chronic use of ICS, and the risk of respiratory virus infections, are scarce. We aimed to compare the characteristics and outcome of respiratory virus infections in adults hospitalized for influenza-like illness (ILI) with, or without, chronic use of ICS.
Materials and methods
Study design
We performed a post-hoc analysis of the FLUVAC study, a multicenter prospective cohort of adult patients admitted for influenza-like illness in six French university hospitals13: Cochin Hospital, Paris; Bichat Hospital, Paris; Pontchaillou Hospital, Rennes; Dupuytren Hospital, Limoges; Montpellier University Hospital; Edouard Herriot Hospital, Lyon. During the study period, all adults hospitalized for at least 24 h with ILI during the influenza season in France (December-March), with symptoms onset < 7 days before screening, were invited to participate. ILI was defined as a combination of two criteria: (i) at least one of the following symptoms: fever (≥ 38 °C), headache, myalgia or malaise, and (ii) at least one of the following respiratory symptoms: cough, sore throat, or shortness of breath (dyspnea). The characteristics and outcome of patients with influenza, respiratory syncytial virus (RSV), and other NIRV in this cohort have been previously reported5,13,14,15. Data on demographic characteristics, comorbidities, treatment before admission (including ICS), clinical presentation, testing for respiratory viruses, hospitalization, treatment, and outcome, were prospectively collected on a standardized questionnaire, from medical charts, and through face-to-face interviews with patients.
For the study reported herein, we included all patients enrolled during the first six FLUVAC seasons (2012/13, 2013/14, 2014/15, 2015/16, 2016/17, and 2017/18). Patients with missing data about ICS use, or testing for respiratory viruses, were excluded.
Virological data
All patients were tested for a panel of respiratory viruses, mostly by nasopharyngeal swabs, and in some cases by bronchoalveolar lavage, if clinically indicated. Respiratory samples were initially tested in the virology units of the participating hospitals by in-house real-time influenza A & B PCR after manual nucleic acid extraction. Amplification was performed with ABI 7500 thermocycler. All samples were then sent to the French National Reference Center for respiratory viruses (CNR-Lyon) for confirmation by RT-PCR. Samples were also screened for a panel of NIRV: adenovirus (52 serotypes), human bocaviruses 1–4, human coronaviruses 229E, NL63, OC43, and HKU1, human metapneumoviruses A1, A2, B1 and B2, parainfluenza viruses 1–4, picornavirus, and respiratory syncytial virus (RSV), by real-time PCR, using the Respiratory Multiwell System (MWS) r-gene assay (bioMérieux S.A., Marcy l’Etoile, France) on an ABI 7300 analyzer.
Ethics
The FLUVAC study (clinicaltrials.gov NCT02027233) was performed in accordance with the principles of Good Epidemiological and Clinical Practices in clinical research and the Declaration of Helsinki, and the study protocol was approved by regional ethics committees (Comité de Protection des Personnes ‘Ile-de-France IV’). This ancillary study was approved by the institutional review board of I-REIVAC (Innovative Clinical Research Network in Vaccinology, France). All the study participants provided written informed consent for respiratory virus testing and data collection before inclusion.
Statistical analysis
We performed a descriptive analysis of the total population and of the population of patients positive for at least one respiratory virus, according to chronic use of ICS. Results were expressed as mean and standard deviation (SD), or median and interquartile range (IQR) for quantitative variables, and n (%) for qualitative variables. The Student test or Fisher’s exact test was used, as appropriate, for univariate comparisons. Missing data for each variable were excluded from the denominator.
To evaluate a potential association between ICS and respiratory virus infections, we performed a multivariate analysis, using a backward logistic regression model for each virus associated with ICS in univariate analysis. In each virus model, associated factors with a P-value < 0.2 in univariate analysis were included in the multivariate analysis. The multivariate analysis for each virus was also adjusted for age and sex. We performed a Bonferroni correction in order to maintain a global alpha risk at 5%. A P-value of 0.05 or less was considered statistically significant. Variables with > 10% missing values were excluded from multivariate analyses with one exception for ‘chronic pulmonary disease’ (27% missing values) which is known to be a major risk factor for viral infections. Collinearity was assessed using the variance inflation factor (VIF) < 5.
Finally, we performed multivariate analyses using a backward stepwise logistic regression model using intensive care unit (ICU) admission as the dependent variable and including covariates with a P-value < 0.2 in univariate analysis, namely age (continuous variable), influenza vaccine, systemic corticosteroids, ICS, empirical antiviral treatment, RSV infection, and influenza virus infection. The model was adjusted for other covariates known to influence ICU admission: chronic heart disease, chronic heart failure, immunosuppressive treatment and malignancy.
Results from both regressions were expressed as odds ratios (OR) and adjusted odds ratios (aOR) with their 95% confidence intervals (95% CI). All analyses were performed using R-Studio (Integrated Development for R. RStudio, Inc., Boston, USA).
Results
Patients characteristics and virus distribution
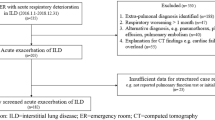
Of the 3156 patients included in the FLUVAC study, 2658 (84.2%, 95% CI 49–53) had complete data on chronic use of ICS, and results of respiratory viruses testing (Fig. 1). The median age was 71 years [IQR 56–83], 53.7% were men, 81.6% had at least one chronic underlying disease, 45.7% had been hospitalized in the previous 12 months, and 46.9% had been vaccinated against influenza during the last 6 months. At least one respiratory virus was found in 52.2%, mostly influenza (64.4% of all respiratory viruses, 895/1389), picornavirus (11.2%, 156/1389), RSV (9.2%, 128/1389), coronavirus (8.6%, 120/1389), human metapneumovirus (6.8%, 94/1389), adenovirus (2.7%, 38/1389), bocavirus (1.7%, 23/1389), and parainfluenza virus (1.2%, 16/1389). At least 2 respiratory viruses were identified in 84 patients (6%).

Study flow chart. ILI influenza-like illness, ICS inhaled corticosteroids.
Characteristics of patients with chronic use of inhaled corticosteroids
Of the 2,658 patients enrolled, 537 patients (20.2%) were chronic users of ICS (Supplementary Table S1). These patients had a median age of 70 years [IQR 58–81], and 283 (52.7%) were men. The main comorbidities in patients on chronic use of ICS was chronic respiratory disease (89.3%), chronic heart disease (42.2%), diabetes (22%), haematological or solid malignancy (16.3%), and chronic kidney disease (13.2%). Of note, 19.4% of patients on chronic use of ICS were also taking systemic corticosteroids. However, in all analyses performed, there was no collinearity between ICS and systemic corticosteroids. Main symptoms were dyspnea (89.6%), fever (84.5%), cough (76%), and myalgia (22%). Median duration of ILI symptoms before admission was 2 days [1–3]. The median length of hospital stay was 7 days [IQR 4–7]. A total of 300 patients presented at least one complication (55.9%) during their hospital stay, including respiratory failure (37.8%), pneumonia (32%), mechanical ventilation (14.8%), heart failure (14%), renal failure (11.8%), acute respiratory distress syndrome (9%), and shock (1.7%). ICU admission occurred in 67 patients (12.5%). In-hospital mortality was 3.2%.
As compared to patients not on ICS, patients with chronic use of ICS were more likely to receive systemic corticosteroids (19.4% vs. 9.6%, P < 0.001), and to have received an influenza vaccine during the last 6 months (59.6% vs. 43.7%, P < 0.001). Dyspnea was more frequent on admission in patients with chronic use of ICS (86.7% vs. 73.1%, P < 0.001).
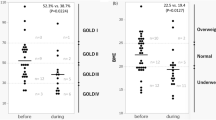
In univariate analysis, chronic use of ICS was associated with higher risk of respiratory failure (37.8% vs. 27.2%, P < 0.001), and ICU admission (12.5% vs. 8.4%, P = 0.01). After adjustment for age, sex, comorbidities, empirical antiviral treatment and respiratory virus, these associations between ICS use and ICU admission or respiratory failure were no longer present (Supplementary Table S2). In-hospital mortality was 3.2% (17/537) in patients with chronic use of ICS, and 4.5% (96/2121) in patients with no use of ICS (P = 0.18).
Patients with respiratory virus infections: comparison of patients with or without chronic use of inhaled corticosteroids (Tables 1, 2)
The proportion of documented respiratory virus infections was similar between patients with, or without, ICS (282/537, 52.5% vs. 1107/2121, 52.2%; P = 0.92). However, patients on ICS were more likely to test positive for NIRV (135/537, 25.1% vs. 413/2121, 19.5%, P = 0.004), and less likely to test positive for influenza virus (159/282, 56.4% vs. 736/1107, 66.5%, P = 0.002). Proportion of A/B influenza viruses was similar in patients with, or without ICS. Patients on ICS were more likely to test positive for adenovirus (14/282, 5% vs. 24/1107, 2.2%, P = 0.013), and RSV (41/282, 14.5% vs. 87/1104, 7.9%, P = 0.001). At least 2 viruses were documented in 22 patients (7.8%) in the ICS group, and 62 patients (5.6%) in the group without ICS. On multivariate analysis, ICS use was significantly associated with adenovirus (aOR 2.36, 95% CI 1.18–4.58), and RSV (aOR 2.08, 95%CI 1.39–3.09), but not with influenza (aOR 0.86, 95% CI 0.6–1.24) (Supplementary Table S3).
Discussion
In this post-hoc analysis of 2,658 adult patients hospitalized for community-acquired ILI and tested for respiratory virus infections by multiplex PCR, we found that chronic use of ICS was associated with increased risk of NIRV infections, particularly adenovirus and RSV. Although patients on ICS were more likely to be transferred in ICU, in-hospital mortality rates were similar in patients with, or without, ICS, and chronic use of ICS was not associated with ICU admission on multivariate analysis.
Only few studies have evaluated the impact of chronic use of ICS on the characteristics and outcomes of respiratory virus infections. ICS have been associated with higher bacterial load in sputum16, and increased risk of pneumonia10,11,17,18. In the latter studies, the diagnosis of pneumonia was based on radio-clinical criteria, with no or limited microbiological documentation. Two recent meta-analyses7,8, and one narrative review9, confirmed that chronic use of ICS is associated with increased risk of pneumonia overall, but could not specify whether this applies for virus as well as for bacteria. Of note, chronic use of ICS has been convincingly associated with a higher risk of non-tuberculous mycobacterial infections19,20,21.
Singanayagam et al. showed that ICS impair innate and acquired antiviral immune responses, through an alteration of interferon production, and antimicrobial peptides deficiency, leading to delayed virus clearance12. At least one respiratory virus has been documented in up to 45% of COPD exacerbations in patients treated by ICS, primarily rhinovirus, adenovirus, and influenza16. A retrospective multicenter study reported 15 consecutives cases of severe pneumonia due to adenovirus in immunocompetent patients, of whom 14 were on ICS22. Of note, human adenoviruses are commonly associated with severe respiratory infections, even lethal, in immunocompromised but also in immunocompetent patients23,24.
To the best of our knowledge, no clinical study found an increased risk of RSV in patients on chronic use of ICS. However, this association is biologically plausible, as human cathelicidin LL-37, which inhibits RSV in vitro and in vivo25, is suppressed by ICS26. The increased risk of RSV infections in patients with malignancy, immunosuppression and/or chronic pulmonary disease, as pointed out by our multivariate analysis, has been documented by others14,27,28. Although influenza was more rarely identified in patients treated by ICS (56.4% vs. 66.5%, P = 0.002), this association was no longer significant in multivariate analysis, and could be explained by the higher influenza vaccination coverage in patients on ICS. Indeed, yearly vaccination against seasonal influenza is recommended in most patients with chronic use of ICS, as these treatments are primarily prescribed in patients with chronic pulmonary diseases.
We found no differences in the occurrence of coronaviruses infections between patients treated by ICS and those who had not. Our data were from before the COVID-19 pandemic and we only studied human coronaviruses 229E, NL63, OC43, and HKU1. These results could be different with SARS-CoV-2 because it was recently demonstrated that ICS downregulated the bronchial epithelial expression SARS-CoV-2 related genes, especially ACE2 that encodes the SARS-CoV-2 human receptor29. To date, studies that have evaluated the impact of ICS on COVID-19 clinical outcomes found discrepant results30,31,32.
This study has limitations. First, given that the analysis of ICS impact was not the primary objective of the FLUVAC prospective cohort study, treatment by ICS was only collected as a dichotomic variable (yes/no), with no information on dose, duration, and comedication. Hence, we were unable to analyze a potential dose–response effect, as documented for the association between ICS and pneumonia11. Likewise, we could not compare the impact of different ICS, while fluticasone has been associated with higher risk of pneumonia than budesonide8,11. Second, data on underlying respiratory diseases have not been collected as well, so that we could not compare respiratory virus distribution, and its association with ICS, in patients with COPD, or asthma, the main indications for ICS. Third, the study design did not allow us to measure prevalence or incidence rate in population treated by ICS. Fourth, our study was performed in a single country in Western Europe, so that our findings may not apply to other countries with different epidemiology of respiratory viruses, or other practices regarding ICS use and influenza vaccination policies. Also, there are discrepancies between the ECDC, WHO and CDC definitions of ILI, which could restrict the generalization of our results. Of note, our findings could be seasonally biased, especially for picornaviruses (enteroviruses and rhinovirus) which may circulate anytime during the year, while our study was restricted to influenza seasons. Fifth, we have no robust data to support causality between respiratory virus detection and ILI in the patients enrolled. However, our study has strengths, including its prospective, multicenter design and standardization of viral test for all patients included, during six consecutive years.
In conclusion, this study suggests a potential link between chronic use of ICS, and respiratory virus infections. To our knowledge, no previous study identified ICS as a risk factor for adenovirus and RSV infections. Further studies are needed to evaluate the role of ICS on viral immunity and their impact on respiratory infections.
Abbreviations
- ARDS:
-
Acute respiratory distress syndrome
- BMI:
-
Body mass index
- COPD:
-
Chronic obstructive pulmonary disease
- ICS:
-
Inhaled corticosteroids
- ICU:
-
Intensive care unit
- ILI:
-
Influenza-like illness
- IQR:
-
Interquartile range
- NIRV:
-
Non-influenza respiratory viruses
- RSV:
-
Respiratory syncytial virus
- SD:
-
Standard deviation
References
Husta, B. C., Raoof, S., Erzurum, S. & Mehta, A. C. Tracheobronchopathy from inhaled corticosteroids. Chest 152, 1296–1305 (2017).
Fergeson, J. E., Patel, S. S. & Lockey, R. F. Acute asthma, prognosis, and treatment. J. Allergy Clin. Immunol. 139, 438–447 (2017).
Quaderi, S. A. & Hurst, J. R. The unmet global burden of COPD. Glob. Health Epidemiol. Genomics. https://doi.org/10.1017/gheg.2018.1 (2018).
Varmaghani, M. et al. Global prevalence of chronic obstructive pulmonary disease: Systematic review and meta-analysis. East. Mediterr. Health J. 25, 47–57 (2019).
The FLUVAC Study Group. Non-influenza respiratory viruses in adult patients admitted with influenza-like illness: A 3-year prospective multicenter study. Infection. https://doi.org/10.1007/s15010-019-01388-1 (2020).
Tashkin, D. P. & Strange, C. Inhaled corticosteroids for chronic obstructive pulmonary disease: What is their role in therapy? Int. J. Chron. Obstruct. Pulmon. Dis. 13, 2587–2601 (2018).
Festic, E., Bansal, V., Gupta, E. & Scanlon, P. D. Association of inhaled corticosteroids with incident pneumonia and mortality in COPD patients; systematic review and meta-analysis. J. Chronic Obstruct. Pulm. Dis. 13, 312–326 (2016).
Yang, M. et al. Inhaled corticosteroids and risk of upper respiratory tract infection in patients with asthma: Meta-analysis. Infection 47, 377–385 (2019).
Singanayagam, A., Chalmers, J. D. & Hill, A. T. Inhaled corticosteroids and risk of pneumonia: Evidence for and against the proposed association. QJM 103, 379–385 (2010).
Calverley, P. M. A. & Jones, P. W. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N. Engl. J. Med. 356, 775 (2007).
Suissa, S., Patenaude, V., Lapi, F. & Ernst, P. Inhaled corticosteroids in COPD and the risk of serious pneumonia. Thorax 68, 1029–1036 (2013).
Singanayagam, A. et al. Corticosteroid suppression of antiviral immunity increases bacterial loads and mucus production in COPD exacerbations. Nat. Commun. https://doi.org/10.1038/s41467-018-04574-1 (2018).
Loubet, P. et al. Factors associated with poor outcomes among adults hospitalized for influenza in France: A three-year prospective multicenter study. J. Clin. Virol. 79, 68–73 (2016).
Loubet, P. et al. Clinical characteristics and outcome of respiratory syncytial virus infection among adults hospitalized with influenza-like illness in France. Clin. Microbiol. Infect. 23, 253–259 (2017).
Loubet, P. et al. Characteristics of human metapneumovirus infection in adults hospitalized for community-acquired influenza-like illness in France, 2012–2018: A retrospective observational study. Clin. Microbiol. Infect. 27, e1–e6 (2021).
Contoli, M. et al. Long-term effects of inhaled corticosteroids on sputum bacterial and viral loads in COPD. Eur. Respir. J. 50, 1700451 (2017).
Wedzicha, J. A. et al. The prevention of chronic obstructive pulmonary disease exacerbations by salmeterol/fluticasone propionate or tiotropium bromide. Am. J. Respir. Crit. Care Med. 177, 19–26 (2008).
Kardos, P., Wencker, M., Glaab, T. & Vogelmeier, C. Impact of salmeterol/fluticasone propionate versus salmeterol on exacerbations in severe chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 175, 144–149 (2007).
Hojo, M. et al. Increased risk of nontuberculous mycobacterial infection in asthmatic patients using long-term inhaled corticosteroid therapy: NTM infections in asthmatics using ICS. Respirology 17, 185–190 (2012).
Andréjak, C. et al. Chronic respiratory disease, inhaled corticosteroids and risk of non-tuberculous mycobacteriosis. Thorax 68, 256–262 (2013).
Brode, S. K. et al. The risk of mycobacterial infections associated with inhaled corticosteroid use. Eur. Respir. J. 50, 1700037 (2017).
Tan, D. et al. Severe community-acquired pneumonia caused by human adenovirus in immunocompetent adults: A multicenter case series. PLoS ONE 11, e0151199 (2016).
Kujawski, S. A. et al. Outbreaks of adenovirus-associated respiratory illness on 5 college campuses in the United States, 2018–2019. Clin. Infect. Dis. 72, 1992–1999 (2021).
Scott, M. K. et al. Human adenovirus associated with severe respiratory infection, Oregon, USA, 2013–2014. Emerg. Infect. Dis. 22, 1044–1051 (2016).
Currie, S. M. et al. Cathelicidins have direct antiviral activity against respiratory syncytial virus in vitro and protective function in vivo in mice and humans. J. Immunol. 196, 2699–2710 (2016).
Singanayagam, A. et al. Inhaled corticosteroid suppression of cathelicidin drives dysbiosis and bacterial infection in chronic obstructive pulmonary disease. Sci. Transl. Med. 11, 3879 (2019).
Walsh, E. E., Peterson, D. R. & Falsey, A. R. Risk factors for severe respiratory syncytial virus infection in elderly persons. J. Infect. Dis. 189, 233–238 (2004).
Nam, H. H. & Ison, M. G. Respiratory syncytial virus infection in adults. BMJ 366, l5021 (2019).
Milne, S. et al. Inhaled corticosteroids downregulate SARS-CoV-2-related genes in COPD: Results from a RCT. Eur. Respir. J. https://doi.org/10.1183/13993003.00130-2021 (2021).
Ramakrishnan, S. et al. Inhaled budesonide in the treatment of early COVID-19 (STOIC): A phase 2, open-label, randomised controlled trial. Lancet Respir. Med. 9, 763–772 (2021).
Aveyard, P. et al. Association between pre-existing respiratory disease and its treatment, and severe COVID-19: A population cohort study. Lancet Respir. Med. https://doi.org/10.1016/S2213-2600(21)00095-3 (2021).
Sen, P., Majumdar, U., Zein, J., Hatipoğlu, U. & Attaway, A. H. Inhaled corticosteroids do not adversely impact outcomes in COVID-19 positive patients with COPD: An analysis of Cleveland Clinic’s COVID-19 registry. PLoS ONE 16, e0252576 (2021).
Acknowledgements
We are very grateful to all persons and institutions who contributed to the FLUVAC study.
Funding
This work was not funded. The study sites received funding from Sanofi Pasteur and MSD for the FLUVAC study. Vaccine producers had no role in the study design, data analysis, decision to publish or preparation of the manuscript.
Author information
Authors and Affiliations
Consortia
Contributions
D.L.P. had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. D.L.P. and P.L. did the analysis. D.L.P., P.T., P.L. and S.J. co-wrote the original draft. F.B., V.T., F.L., P.V., S.A., B.L., X.D., A.S.L., N.F., C.V., S.A., F.G., V.F., G.L., V.F., G.L., N.L., Z.L., O.L. contributed substantially to the investigation and data collection, as well to reviewing and editing the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors reported no conflict of interest related to this work. DLP, PT, FB, VT, FL, PV, SA, BL, XD, ASL, NF, CV, SA, FG, VF, GL, VF, GL, NL, ZL have nothing to disclose. PL reports personal fees and non-financial support from Pfizer, personal fees and non-financial support from Sanofi Pasteur, outside the submitted work. OL reports personal fees and non-financial support from Janssen, personal fees and non-financial support from MSD, personal fees and non-financial support from Sanofi Pasteur, personal fees and non-financial support from GSK, personal fees and non-financial support from Pfizer, outside the submitted work. SJ reports personal fees from Actelion, personal fees from AIRB, personal fees from AstraZeneca, personal fees from Bristol-Myers Squibb, personal fees from Boehringer Ingelheim, personal fees from Chiesi, personal fees from Galecto, personal fees from Gilead, personal fees from GlaxoSmithKline, personal fees from LVL, personal fees from Mundipharma, personal fees from Novartis, personal fees from Pfizer, personal fees from Roche, personal fees from Savara-Serendex, outside the submitted work.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Luque-Paz, D., Tattevin, P., Loubet, P. et al. Chronic use of inhaled corticosteroids in patients admitted for respiratory virus infections: a 6-year prospective multicenter study. Sci Rep 12, 4199 (2022). https://doi.org/10.1038/s41598-022-08089-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-08089-0
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
