
Abstract
Craniospinal irradiation using helical tomotherapy (HT-CSI) has advantages in aspects of homogeneous dose distribution. Physicians, however, still have concerns of pulmonary toxicity due to HT-CSI’s relatively large, low-dose irradiated volume from continuous and 360° rotation delivery. In this study, we investigated the pulmonary toxicity of HT-CSI. We retrospectively reviewed 105 patients who received HT-CSI between January 2014 and December 2019. Grade 2 + pulmonary toxicities were evaluated. Intensive systemic treatment was defined as systemic treatment administration before, during, and after HT-CSI. VX Gy was defined as % volume receiving ≥ X Gy. Thirteen patients (12.4%) presented with grade 2 + pulmonary toxicities after HT-CSI. Of these patients, only one experienced grade 2 radiation pneumonitis combined with pembrolizumab-induced pneumonitis. Conversely, pneumonia was observed in 12 patients. Intensive systemic treatment (p = 0.004), immunosuppressive drugs (p = 0.031), and bilateral lung V5 Gy ≥ 65% (p = 0.031) were identified as independent risk factors for pneumonia. The risk factor for pneumonia in pediatric patients were immunosuppressive drugs (p = 0.035) and bilateral lung V5 Gy ≥ 65% (p = 0.047). HT-CSI can be a safe treatment modality with tolerable pulmonary toxicities. Intensive systemic treatment, immunosuppressive drugs, and bilateral lung V5 Gy ≥ 65% were significantly associated with pneumonia. In these patients, close follow-up should be considered for proper management of pneumonia.
Similar content being viewed by others


Introduction
Craniospinal irradiation (CSI) is necessary for preventing the spread of central nervous system tumors via cerebrospinal fluid, or for palliative purposes when leptomeningeal seeding of solid cancers causes neurologic symptoms1,2,3.
Yonsei Cancer Center has conducted CSI using two-dimensional radiotherapy (RT) from 1992 and three-dimensional conformal RT (3D-CRT) from 2000. However, due to the low conformity of the 3D-CRT itself, it has the disadvantage of releasing unnecessary doses to the normal tissue and organs around the target4,5. This is especially highlighted in children. The main patients receiving CSI are children, and they are known to have more serious side effects: endocrine system disorders, growth disorders, and secondary malignancy after RT6,7.
Since 2012, our institution has compensated for this disadvantage of 3D-CRT by setting up CSI using helical tomotherapy (HT-CSI), and helical tomotherapy (HT) is still used as the main modality of CSI. HT-CSI generally gives a more conformal dose distribution than 3D-CRT. Thus, unnecessary doses irradiated to normal tissues or organs near the target can be reduced, thereby reducing side effects8,9. However, HT-CSI has potential limits. It is characterized by a full 360-degree delivery, which is continuously irradiated in all directions. It has a wider low dose distribution than that in 3D-CRT for CSI (see Supplementary Fig. S1 online). For this reason, there is a concern about pulmonary toxicity caused by HT-CSI10,11.
In this study, we analyzed the prevalence and risk factors for pulmonary toxicity in patients receiving HT-CSI and ultimately investigated the safety and feasibility of HT-CSI. In addition, we tried to determine whether a difference exists between pediatric and adult patients with pulmonary toxicity due to HT-CSI.
Results
Patient, treatment, and dosimetric characteristics
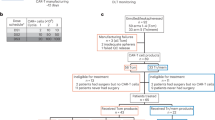
The baseline characteristics of patients are summarized in Table 1. There were 51 pediatric (48.6%) and 54 adult patients (51.4%). The median age at CSI was 21 years (range 2–74). The most common disease was germ cell tumor in pediatric (22/51, 43.1%) and glioblastoma in adult (14/54, 25.9%) patients, respectively.
Treatment details are listed in Table 2. Total CSI dose for all patients was median 36.0 Gy (range 12.0–45.0) with a fractional dose of median 1.5 Gy (range 1.2–3.0); 23 patients (21.9%) with < 20 Gy, 27 (25.7%) with 20–36 Gy, and 55 (52.4%) with ≥ 36 Gy, respectively. The total CSI dose for 51 pediatric patients was median 23.4 Gy; 20 (39.2%) with < 20 Gy, 17 (33.3%) with 20–36 Gy, and 14 (27.5%) with ≥ 36 Gy, respectively. The total CSI dose for 54 adult patients was median 36.0 Gy; 3 (5.6%) with < 20 Gy, 10 (18.5%) with 20–36 Gy, and 41 (75.9%) with ≥ 36 Gy, respectively. Boost RT was administered to 85 patients (81.0%), 13 (12.4%) of them on T spine level. Systemic treatment was given to 70 patients (66.7%). Forty-six patients (43.8%) received systemic treatment before HT-CSI, 43 (41.0%) after HT-CSI, and 36 (34.3%) during HT-CSI. Intensive systemic treatment, which involved systemic treatment before, during, and after HT-CSI, was given to 15 patients (14.3%); 14 pediatric (27.5%), and one adult patient (1.9%). Sixty-two patients (59.0%) were hospitalized during HT-CSI for median 38 days. During HT-CSI, 29 patients (27.6%) received immunosuppressive drugs; 18 of whom received dexamethasone and 11, prednisolone. Nine pediatric (17.6%) and 20 adult patients (37.0%) were administered immunosuppressive drugs.
Pulmonary toxicity
Over a median follow-up duration of 10.5 months (range 0.7–62.1 months), there were 16 patients (15.2%) who presented with pulmonary toxicities after HT-CSI; grade 1 in 3, grade 2 in 11, and grade 3 in 2 patients. None of them experienced grade 4 or 5 toxicity. Of the 13 grade 2 + pulmonary toxicities, one was diagnosed with radiation pneumonitis and 12 with pneumonia. Dosimetric characteristics of patients according to the presence of grade 2 + pulmonary toxicities are shown in Supplementary Table S1 online. Each dosimetric parameter showed no statistical difference depending on whether the patient had grade 2 + pulmonary toxicities, and the bilateral lung V5 Gy showed a high tendency in the group of patients with grade 2 + pulmonary toxicities (not statistically significant). VX Gy was defined as the volume of organs at risk of receiving at least X Gy.
The characteristics of the patients who had grade 2 + pulmonary toxicities are summarized in Table 3. Radiation pneumonitis was diagnosed in a total of 4 patients, 3 had grade 1 and 1 patient, grade 2. Of the 12 patients diagnosed with pneumonia, seven were diagnosed with pneumocystis pneumonia and 5 with bacterial pneumonia.
The patient diagnosed with grade 2 radiation pneumonitis was a 52-year-old man who underwent HT-CSI for leptomeningeal seeding of malignant melanoma. Radiation pneumonitis occurred 2.7 months after the start of HT-CSI. Bilateral lung V5 Gy, V10 Gy, V20 Gy, and V30 Gy of this patient were 61.5%, 31.4%, 13.0%, 6.0%, and 1.0%, respectively. During and after HT-CSI, he received pembrolizumab. Therefore, it was determined that radiation pneumonitis and pembrolizumab-induced pneumonitis occur together. This patient's dose distribution for HT-CSI and computed tomography (CT) images at the time of diagnosis of radiation pneumonitis are shown in Fig. 1.

A 52-year-old man in whom grade 2 radiation pneumonitis developed 82 days after initiation of radiotherapy for leptomeningeal carcinomatosis of malignant melanoma. (A, C) Dose distribution for craniospinal irradiation and (B, D) radiation pneumonitis in computed tomographic image.
Pneumonia occurred median 2.3 months after the start of HT-CSI. In multivariate analysis, intensive systemic treatment (odds ratio (OR) 9.63, 95% confidence interval (CI) 2.07–44.76, p = 0.004), immunosuppressive drugs (OR 4.68, 95% CI 1.15–19.0, p = 0.031) and bilateral lung V5 Gy ≥ 65% (OR 4.90, 95% CI 1.16–20.77, p = 0.031) were identified as independent risk factors for pneumonia (Table 4). Five (5/7, 71.4%) patients diagnosed with pneumocystis pneumonia received intensive systemic treatment, while none of the patients with bacterial pneumonia received intensive systemic treatment. Five (5/7, 71.4%) patients diagnosed with pneumocystis pneumonia and 1 (1/5, 20.0%) with bacterial pneumonia were administered immunosuppressive drugs.
Subgroup analysis by age
Mean bilateral lung dose (pediatric vs. adult; median 6.7 Gy vs. 8.1 Gy, p = 0.036), bilateral lung V5 Gy (median 48.2% vs. 64.0%, p = 0.012), V10 Gy (median 16.3% vs. 24.8%, p = 0.032), mean bone marrow dose (median 14.4 Gy vs. 17.7 Gy, p = 0.001), bone marrow V20 Gy (median 40.0% vs. 43.0%, p = 0.004) and mean heart dose (median 7.4 Gy vs. 8.5 Gy, p = 0.001) were significantly higher in adult patients than those in pediatric patients. The beam-on time was significantly longer for adult patients than for pediatric patients (median 518.0 s vs. 616.3 s, p = 0.004). A comparison of dosimetric characteristics between pediatric and adult patients is shown in Table 5.
Of the 12 patients diagnosed with pneumonia, 7 (7/51, 13.7%) were pediatric and 5 (5/54, 9.3%) were adult patients. Of the 7 pediatric patients, 4 were diagnosed with pneumocystis pneumonia and 3 were diagnosed with bacterial pneumonia. Of the 5 adult patients, 3 were diagnosed with pneumocystis pneumonia and 2 with bacterial pneumonia. In multivariate analysis for risk factors of pneumonia in pediatric patients, immunosuppressive drugs (OR 13.03, 95% CI 1.20–141.93, p = 0.035) and bilateral lung V5 Gy ≥ 65% (OR 10.17, 95% CI 1.04–99.79, p = 0.047) were identified as independent risk factors (Table 4). Univariate and multivariate analyses in adult patients showed no independent risk factors associated with pneumonia (see Supplementary Table S2 online).
Discussion
The results of this study showed that the incidence of grade 2 + pulmonary toxicity was 12.4%, of which 92.3% were in the form of pneumonia. The risk of developing pneumonia increased as immunosuppressive drugs were used, the longer the systemic treatment was received, and the wider the lung was irradiated with low doses.
HT can solve the complex junction problem, which was pointed out as a disadvantage of 3D-CRT and create a homogenous dose distribution by delivering image-modulated beam helically during CSI, which requires treatment of extended volume in the cranio-caudal direction12. In addition, HT is more comfortable (both prone or supine) for the patient during treatment and allows for daily verification using megavoltage CT (MVCT) at each fraction13.
However, helical delivery of beams can cause the disadvantage of low dose exposure to a wide range of normal tissues. Due to the nature of HT, there have been concerns about lung toxicity caused by low doses, and several related studies have been published. Of these, the largest number of studies were conducted on patients who received RT to the lung lesions directly. In these studies, 27–70% of patients who received RT using HT for lung cancer were diagnosed with grade 2 + pulmonary toxicity, and bilateral lung V5 Gy was found to be a significant predictive factor of pulmonary toxicity, similar to our findings14,15,16. In particular, most of these pulmonary toxicity-related studies set the cut-off value of lung V5 Gy at 65–67.5%, and our findings also showed a significant difference in pulmonary toxicity based on 65% of lung V5 Gy. There is also a concern that secondary malignancy may appear more than other RT-induced side effects owing to the widely irradiated low dose. However, there is no study showing clear evidence for secondary malignancy in HT, and although a small number of patients were examined, there were also results that HT did not induce the greater likelihood of secondary malignancy17,18.
Another disadvantage of HT is the long beam-on time. According to dosimetric comparative studies between volumetric modulated arc therapy (VMAT) and HT, the beam-on time was approximately two times longer in HT than in VMAT19. Especially, HT-CSI has a longer beam-on time because of its wider treatment range than that for other treatment sites; thus, intrafractional movement is likely to occur.
In addition, studies on the feasibility of CSI using VMAT have been recently published20,21,22. As a result of dosimetric comparison, HT was superior to VMAT in planning target volume (PTV) conformity and homogeneity and in organs at risk sparing. Further, lung V5 Gy had a median value of 60–70%, and it was higher than the 55.2% of our study. The main toxicity in CSI using VMAT was hematologic toxicity and showed an incidence rate similar to 3D-CRT. Further studies are needed because studies on CSI using VMAT have relatively fewer patients and a shorter follow-up period than HT-CSI studies.
Some studies analyzed the pulmonary toxicity in patients who received HT-CSI, one of which reported that none of 18 pediatric patients who received HT-CSI were diagnosed with symptomatic acute radiation pneumonitis23. Öztunali et al. reported that 2 out of 43 patients aged 7 on average (range 1–56) who received HT-CSI for medulloblastoma were diagnosed with grade 1 pneumonitis and 1 was diagnosed with grade 3 pneumonitis24. As these studies showed, all pulmonary toxicity studies in patients who received CSI were mostly conducted on pediatric patients. In both studies, the incidence of radiation pneumonitis was lower than that of the study directly treating lung lesions. The incidence of grade 2 + pulmonary toxicity in our study was 12.4%, but among them, pure radiation pneumonitis comprised one case, with the rest being pneumonia.
One patient with radiation pneumonitis in this study had received pembrolizumab during and after HT-CSI. The relationship between immune checkpoint inhibitor (ICI) and pneumonitis has been reported in several studies, with an incidence rate of 3–5%25,26. There is some overlap between the toxicity associated with RT and the toxicity associated with an ICI. One study showed an increase in the incidence of immune-related adverse events of any grade, if the dose is more than 2 Gy per fraction27. In the development of pneumonitis, the relationship between low-dose irradiation to the lungs and pembrolizumab is yet to be identified, only relevant case reports exist28, and further investigation is needed.
Of the types of pneumonia, cryptogenic organizing pneumonia and pneumocystis pneumonia are particularly associated with RT29,30,31. Cryptogenic organizing pneumonia is a form of idiopathic interstitial pneumonia, and inflammation of the bronchioles (bronchiolitis) and surrounding tissue in the lungs32. Cryptogenic organizing pneumonia was known to be caused by interactions between the infection, RT, and immune systems29. Among the several factors, RT was thought to play a vital role in the development of cryptogenic organizing pneumonia by causing indirect lung injury by the autoimmune process rather than by direct lung injury30. In our study, there were 5 patients with bacterial pneumonia, which is believed to have occurred in the same mechanism as cryptogenic organizing pneumonia. Unlike RT, the relationship between chemotherapy and cryptogenic organizing pneumonia is rarely known, and only case reports have been published33. None of the patients diagnosed with bacterial pneumonia in our study received intensive systemic treatment, and 3 (60%) patients did not receive chemotherapy, or received chemotherapy for less than two months; therefore, the connection between bacterial pneumonia and chemotherapy is expected to be low.
Pneumocystis pneumonia is an opportunistic infection caused by a fungus called Pneumocystis jirovecii. Its development should be considered in not only immunocompromised patients, but also in patients undergoing intensive chemotherapies and immunotherapies, organ transplantation, or corticosteroid treatment34,35,36. No research has so far shown that RT is an independent risk factor for pneumocystis pneumonia, but studies have shown that there is a risk of opportunistic infection due to lymphopenia, which occurs when RT is combined with chemotherapy or steroid31. Lee et al. also reported that prolonged high-dose steroid therapy and concurrent chemoradiotherapy were risk factors for pneumocystis pneumonia development among patients with lung cancer37. Of the patients diagnosed with pneumocystis pneumonia in our study, 71.4% received intensive systemic treatment and immunosuppressive drugs, respectively, and all 7 patients diagnosed with pneumocystis pneumonia received either intensive systemic treatment or immunosuppressive drugs.
In both types of pneumonia, RT can be a risk factor, and our study showed a relationship between pneumonia and bilateral lung V5 Gy. However, no previous literature has found a direct link between low dose exposure to lung and pneumonia, so further research is needed.
We divided patients into pediatrics and adults, and performed subgroup analysis for each group, with significantly higher dosimetric parameters including bilateral lung V5 Gy in adult patients. This is estimated to be due to a relatively higher prescription dose for CSI in adult patients than in pediatric patients (median 36.0 Gy vs. 23.4 Gy). Subgroup analysis of pediatric patients found that immunosuppressive drugs and bilateral lung V5 Gy were risk factors associated with pneumonia. Immunocompromised children are at risk of pneumonia due to opportunistic pathogens, especially prolonged corticosteroid therapy was found to be a risk factor in pneumocystis pneumonia in pediatric patients38. Chemotherapy, which causes bone marrow insufficiency, is also a principal factor in causing pneumonia in pediatric patients39. In our study, intensive systemic treatment was not found to be statistically related to pneumonia in pediatric patients, but all pediatric patients diagnosed with pneumonia had received systemic treatment for more than 2 months. Finally, as in the case of overall patients, there was no related literature that revealed the association between pneumonia and bilateral lung V5 Gy in pediatric patients.
One of the limitations of this study was that due to its retrospective nature, there was uncertainty in assessing subjective symptoms that may result in an underestimation of symptomatic pulmonary toxicity. In addition, since all patients who received HT-CSI were analyzed, tumor and treatment characteristics are heterogeneous. Moreover, although the pathophysiology of bacterial pneumonia and pneumocystis pneumonia differ, two types of pneumonia were grouped and analyzed at once. Lastly, since pneumonia is caused by relatively various factors compared to radiation pneumonitis, and the patient to be analyzed also has various treatment and clinical-related factors that can cause pneumonia, there may be confounding factors. Nevertheless, the strength of this study is that among the studies that tried to analyze toxicity in HT-CSI, ours had a large amount of patient data, including 50 or more pediatric and adult patients, respectively. In addition, this is the first study to analyze pulmonary toxicity by subdividing it into radiation pneumonitis and pneumonia, and to suggest the relationship between a low dose irradiated to the lungs and pneumonia. Finally, this study tried to apply the dosimetric factor to the clinical field by analyzing the differences in dosimetric characteristics according to grade 2 + pulmonary toxicity or pediatric/adult.
In conclusion, the findings of this study suggest that HT could be a safe treatment modality with tolerable pulmonary toxicities in terms of CSI. The incidence rate of grade 2 + radiation pneumonitis was 1.0%, and 11.4% of total patients were diagnosed with pneumonia caused by multiple factors. Intensive systemic treatment, immunosuppressive drugs, and bilateral lung V5 Gy ≥ 65% were significantly associated with pneumonia. In pediatric patients, immunosuppressive drugs, and bilateral lung V5 Gy had a greater effect. If any of the above risk factors are present among patients receiving HT-CSI, close follow-up should be considered for proper management of pneumonia. In addition, when planning HT-CSI, it is recommended that the low dose irradiated to the lung be as low as possible, especially V5 Gy should be the most concerned.
Materials and methods
Patient selection
HT-CSI (Accuray, Sunnyvale, CA, USA) has been utilized in our institution since 2014. Patients who received HT-CSI between January 2014 and December 2019 were screened (n = 106). Additionally, our institution has also utilized one of the newest generation of tomotherapy delivery systems (Radixact™: Accuray, Sunnyvale, CA, USA) for CSI since November 2018. Patients who received CSI using Radixact™ between November 2018 and December 2019 were also screened (n = 17). Patients who received CSI combined with 3D-CRT (n = 5) or could not complete RT (n = 13) were excluded. Finally, 105 patients were included in our cohort.
This study was approved by the Severance Hospital institutional review board (No. 4–2021-0555). The requirement for informed consent was also waived by the Severance Hospital institutional review board because of the retrospective nature of this study. This study was conducted in accordance with the 1964 Declaration of Helsinki and its later amendments. All methods were carried out in accordance with relevant guidelines and regulations.
Radiotherapy
All patients underwent simulation CT with 3- or 5-mm slice thickness and intravenous contrast. Thermoplastic masks and Vac-Lok cushion (Blue BAG, Elekta, Stockholm, Sweden) were used for immobilization. Clinical target volume (CTV), PTV, and organs at risk were contoured on simulation CT images using MIM software (MIM Software Inc., Cleveland, OH, USA). CTV for the whole brain and spinal canal plus 3-mm margin were contoured. PTV was generated by expanding the CTV by 3-mm margin at the brain, 5-mm margin at C1-T7 spine level, 7-mm margin at T8-T12 spine level, and 10-mm margin at L1 spine-sacral level. The whole brain, spinal canal, and organs at risk are contoured according to the European Society for Paediatric Oncology (SIOPE) guidelines40. TomoTherapy (Accuray, Sunnyvale, CA, USA) or Precision (Accuray, Sunnyvale, CA, USA) software were used for intensity-modulated RT (IMRT) plans. The medical dosimetrists set the following three major parameters: a field width of 2.5–5.0 cm, a pitch of 0.29–0.45, and a modulation factor of 1.4–2.7. PTV coverage was evaluated using the percentage of PTV covered by ≥ 95% of the prescribed dose, with a goal of ≥ 95%. The dose constraints for organs at risk followed the criteria presented in the Quantitative Analysis of Normal Tissue Effects in the Clinic: lung mean dose ≤ 20 Gy, V20 Gy ≤ 30%, and heart mean dose ≤ 26 Gy41.
For daily treatment, the patient’s posture was fixed with thermoplastic masks and the Vac-Lok cushion was used when simulation CT was performed42. MVCT obtained from the zygomatic arch to the level of the C4 spine was automatically registered in the simulation CT image. After automatic registration, if necessary, the couch was moved to the correct setting in the X, Y, and Z directions at the discretion of the radiation therapist. Post-treatment MVCT ranging from the levels of T12 to L4 was obtained after each fractional treatment was delivered. Because MVCT was acquired at the C spine and L spine levels, no imaging dose was added to the lungs, and only a therapeutic dose could be given.
Follow-up and assessment of pulmonary toxicity
After RT, patients were followed up by surgeons, oncologists, and radiation oncologists, once monthly then every 3 months for the first 2 years, every 6 months for 1 year, then yearly thereafter. Pulmonary toxicity was diagnosed based on the patient's subjective symptoms and imaging findings. Any grade 2 + pulmonary toxicities (radiation pneumonitis or pneumonia) were evaluated based on the Common Terminology Criteria for Adverse Events version 5.0. Grade 2 pulmonary toxicity was defined by symptomatic aspects, as limiting instrumental activities of daily living, and it required medical intervention.
Statistical analysis
To analyze factors related to grade 2 + pulmonary toxicities, logistic regression analysis was used. The following variables were used: age (pediatric, adult), sex (male, female), total CSI dose group (< 20 Gy, 20–36 Gy, ≥ 36 Gy), dose per fraction for CSI, intensive systemic treatment, immunosuppressive drugs, admission during CSI, and dosimetric factors (bilateral lung V5 Gy, bone marrow V5 Gy). Adult and pediatric patients were defined as patients above and below the age of 20 years, respectively. Intensive systemic treatment was defined as systemic treatment administration before, during, and after HT-CSI.
An independent t-test was used to compare the doses irradiated to organs at risks in pediatric and adult patients, and to examine the relationship of dose difference in both groups, and the incidence of pulmonary toxicity.
For multivariate analysis, a backward stepwise selection procedure was adopted. P-values lower than 0.05 were considered statistically significant. Statistical analysis was performed using IBM SPSS, version 25.0 (IBM Corp., Armonk, NY, USA).
Data availability
There are no restrictions on the availability of materials or information. The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Maity, A. et al. Craniospinal radiation in the treatment of biopsy-proven intracranial germinomas: Twenty-five years’ experience in a single center. Int. J. Radiat. Oncol. Biol. Phys. 58, 1165–1170. https://doi.org/10.1016/j.ijrobp.2003.08.028 (2004).
Navajas, A. & Giralt, J. Evidence in medulloblastomas. Clin. Transl. Oncol. 12, 271–277. https://doi.org/10.1007/s12094-010-0503-y (2010).
Buszek, S. M. & Chung, C. Radiotherapy in leptomeningeal disease: A systematic review of randomized and non-randomized trials. Front. Oncol. 9, 1224. https://doi.org/10.3389/fonc.2019.01224 (2019).
Seravalli, E. et al. Dosimetric comparison of five different techniques for craniospinal irradiation across 15 European centers: Analysis on behalf of the SIOP-E-BTG (radiotherapy working group). Acta Oncol. 57, 1240–1249. https://doi.org/10.1080/0284186x.2018.1465588 (2018).
St Clair, W. H. et al. Advantage of protons compared to conventional X-ray or IMRT in the treatment of a pediatric patient with medulloblastoma. Int. J. Radiat. Oncol. Biol. Phys. 58, 727–734. https://doi.org/10.1016/s0360-3016(03)01574-8 (2004).
Chang, E. L. et al. Acute toxicity and treatment interruption related to electron and photon craniospinal irradiation in pediatric patients treated at the University of Texas M. D. Anderson Cancer Center. Int. J. Radiat. Oncol. Biol. Phys. 52, 1008–1016. https://doi.org/10.1016/s0360-3016(01)02717-1 (2002).
Mu, X. et al. Does electron and proton therapy reduce the risk of radiation induced cancer after spinal irradiation for childhood medulloblastoma? A comparative treatment planning study. Acta Oncol. 44, 554–562. https://doi.org/10.1080/02841860500218819 (2005).
Sterzing, F. et al. Helical tomotherapy. Experiences of the first 150 patients in Heidelberg. Strahlenther Onkol. 184, 8–14. https://doi.org/10.1007/s00066-008-1778-6 (2008).
Schiopu, S. R. et al. Craniospinal irradiation using helical tomotherapy for central nervous system tumors. J. Radiat. Res. 58, 238–246. https://doi.org/10.1093/jrr/rrw095 (2017).
Ramsey, C., Seibert, R., Mahan, S. L., Desai, D. & Chase, D. Out-of-field dosimetry measurements for a helical tomotherapy system. J. Appl. Clin. Med. Phys. 7, 1–11. https://doi.org/10.1120/jacmp.v7i3.2212 (2006).
Hijal, T. et al. Simultaneous integrated boost in breast conserving treatment of breast cancer: A dosimetric comparison of helical tomotherapy and three-dimensional conformal radiotherapy. Radiother. Oncol. 94, 300–306. https://doi.org/10.1016/j.radonc.2009.12.043 (2010).
Peñagarícano, J. A., Papanikolaou, N., Yan, Y., Youssef, E. & Ratanatharathorn, V. Feasibility of cranio-spinal axis radiation with the Hi-Art tomotherapy system. Radiother. Oncol. 76, 72–78. https://doi.org/10.1016/j.radonc.2005.06.013 (2005).
Sterzing, F. et al. Megavoltage CT in helical tomotherapy—Clinical advantages and limitations of special physical characteristics. Technol. Cancer Res. Treat. 8, 343–352. https://doi.org/10.1177/153303460900800504 (2009).
Song, C. H. et al. Treatment-related pneumonitis and acute esophagitis in non-small-cell lung cancer patients treated with chemotherapy and helical tomotherapy. Int. J. Radiat. Oncol. Biol. Phys. 78, 651–658. https://doi.org/10.1016/j.ijrobp.2009.08.068 (2010).
Kim, Y., Hong, S. E., Kong, M. & Choi, J. Predictive factors for radiation pneumonitis in lung cancer treated with helical tomotherapy. Cancer Res. Treat. 45, 295–302. https://doi.org/10.4143/crt.2013.45.4.295 (2013).
Jo, I. Y. et al. Significance of low-dose radiation distribution in development of radiation pneumonitis after helical-tomotherapy-based hypofractionated radiotherapy for pulmonary metastases. J. Radiat. Res. 55, 105–112. https://doi.org/10.1093/jrr/rrt080 (2014).
Han, E. Y. et al. Estimation of the risk of secondary malignancy arising from whole-breast irradiation: Comparison of five radiotherapy modalities, including TomoHDA. Oncotarget 7, 22960–22969. https://doi.org/10.18632/oncotarget.8392 (2016).
Kim, D. W. et al. Risk of second cancer from scattered radiation of intensity-modulated radiotherapies with lung cancer. Radiat. Oncol. (London, England) 8, 47. https://doi.org/10.1186/1748-717x-8-47 (2013).
Müdder, T. et al. Dosimetric comparison between helical tomotherapy and volumetric modulated arc therapy in patients with malignant pleural mesothelioma. Clin. Oncol. (Royal College of Radiologists (Great Britain) https://doi.org/10.1016/j.clon.2021.08.005 (2021).
Sun, Y. et al. Dosimetric comparisons of craniospinal axis irradiation using helical tomotherapy, volume-modulated arc therapy and intensity-modulated radiotherapy for medulloblastoma. Transl. Cancer Res. 8, 191–202. https://doi.org/10.21037/tcr.2019.01.30 (2019).
Lőcsei, Z. et al. Assessment of the results and hematological side effects of 3D conformal and IMRT/ARC therapies delivered during craniospinal irradiation of childhood tumors with a follow-up period of five years. BMC Cancer 20, 702. https://doi.org/10.1186/s12885-020-07168-7 (2020).
Wong, K. K. et al. Acute toxicity of craniospinal irradiation with volumetric-modulated arc therapy in children with solid tumors. Pediatr. Blood Cancer 65, e27050. https://doi.org/10.1002/pbc.27050 (2018).
Peñagarícano, J., Moros, E., Corry, P., Saylors, R. & Ratanatharathorn, V. Pediatric craniospinal axis irradiation with helical tomotherapy: Patient outcome and lack of acute pulmonary toxicity. Int. J. Radiat. Oncol. Biol. Phys. 75, 1155–1161. https://doi.org/10.1016/j.ijrobp.2008.12.083 (2009).
Öztunali, A. et al. Toxicity reduction after craniospinal irradiation via helical tomotherapy in patients with medulloblastoma: A unicentric retrospective analysis. Cancers (Basel) https://doi.org/10.3390/cancers13030501 (2021).
Reck, M. et al. Pembrolizumab versus chemotherapy for PD-L1-positive non-small-cell lung cancer. N. Engl. J. Med. 375, 1823–1833. https://doi.org/10.1056/NEJMoa1606774 (2016).
Nishino, M., Giobbie-Hurder, A., Hatabu, H., Ramaiya, N. H. & Hodi, F. S. Incidence of programmed cell death 1 inhibitor-related pneumonitis in patients with advanced cancer: A systematic review and meta-analysis. JAMA Oncol. 2, 1607–1616. https://doi.org/10.1001/jamaoncol.2016.2453 (2016).
Hwang, W. L., Pike, L. R. G., Royce, T. J., Mahal, B. A. & Loeffler, J. S. Safety of combining radiotherapy with immune-checkpoint inhibition. Nat. Rev. Clin. Oncol. 15, 477–494. https://doi.org/10.1038/s41571-018-0046-7 (2018).
Nakajima, S. et al. Pneumonitis following Pembrolizumab and radiation therapy in a patient with lung cancer and rib metastasis: A case report. Med. Case Rep. Study Protoc. 1, e0004. https://doi.org/10.1097/md9.0000000000000004 (2020).
Ogo, E. et al. A survey of radiation-induced bronchiolitis obliterans organizing pneumonia syndrome after breast-conserving therapy in Japan. Int. J. Radiat. Oncol. Biol. Phys. 71, 123–131. https://doi.org/10.1016/j.ijrobp.2007.09.003 (2008).
Crestani, B. et al. Bronchiolitis obliterans organizing pneumonia syndrome primed by radiation therapy to the breast. The Groupe d’Etudes et de Recherche sur les Maladies Orphelines Pulmonaires (GERM"O"P). Am. J. Respir. Crit. Care Med. 158, 1929–1935. https://doi.org/10.1164/ajrccm.158.6.9711036 (1998).
Hughes, M. A., Parisi, M., Grossman, S. & Kleinberg, L. Primary brain tumors treated with steroids and radiotherapy: Low CD4 counts and risk of infection. Int. J. Radiat. Oncol. Biol. Phys. 62, 1423–1426. https://doi.org/10.1016/j.ijrobp.2004.12.085 (2005).
Cordier, J.-F. Cryptogenic organising pneumonia. Eur. Respir. J. 28, 422–446. https://doi.org/10.1183/09031936.06.00013505 (2006).
Lee, E. J., Lee, S. Y., In, K. H., Kim, C. H. & Park, S. Organizing pneumonia associated with oxaliplatin-combined chemotherapy: A case report. Med. Princ. Pract. 21, 89–92. https://doi.org/10.1159/000331898 (2012).
Barbounis, V. et al. Pneumocystis carinii pneumonia in patients with solid tumors and lymphomas: Predisposing factors and outcome. Anticancer Res. 25, 651–655 (2005).
Takeuchi, K. & Yakushijin, Y. Pneumocystis jirovecii pneumonia prophylaxis for cancer patients during chemotherapy. Pathogens https://doi.org/10.3390/pathogens10020237 (2021).
Sepkowitz, K. A., Brown, A. E., Telzak, E. E., Gottlieb, S. & Armstrong, D. Pneumocystis carinii pneumonia among patients without AIDS at a cancer hospital. JAMA 267, 832–837 (1992).
Lee, E. H. et al. Risk factors and clinical characteristics of Pneumocystis jirovecii pneumonia in lung cancer. Sci. Rep. 9, 2094. https://doi.org/10.1038/s41598-019-38618-3 (2019).
Shankar, S. M. & Nania, J. J. Management of Pneumocystis jiroveci pneumonia in children receiving chemotherapy. Paediatr. Drugs 9, 301–309. https://doi.org/10.2165/00148581-200709050-00003 (2007).
Voulgaridou, A., Athanasiadou, K. I., Athanasiadou, E., Roilides, E. & Papakonstantinou, E. Pulmonary infectious complications in children with hematologic malignancies and chemotherapy-induced neutropenia. Diseases https://doi.org/10.3390/diseases8030032 (2020).
Ajithkumar, T. et al. SIOPE-Brain tumor group consensus guideline on craniospinal target volume delineation for high-precision radiotherapy. Radiother. Oncol. J. Eur. Soc. Therap. Radiol. Oncol. 128, 192–197. https://doi.org/10.1016/j.radonc.2018.04.016 (2018).
Marks, L. B. et al. Use of normal tissue complication probability models in the clinic. Int. J. Radiat. Oncol. Biol. Phys. 76, S10-19. https://doi.org/10.1016/j.ijrobp.2009.07.1754 (2010).
Lee, J. et al. Practical aspects of the application of helical tomotherapy for craniospinal irradiation. Sci. Rep. 11, 6120. https://doi.org/10.1038/s41598-021-85574-y (2021).
Acknowledgements
This work was supported by the National Research Foundation of Korea (NRF). We received funding from the Basic Science Research Program through the NRF funded by the Ministry of Education; Grant No: NRF-2018R1D1A1B07049228.
Author information
Authors and Affiliations
Contributions
H.Y. and Y.C. conceived and designed the study. J.L. performed the study. E.K., N.K. and J.L. analyzed the data. H.Y. and C.S. contributed materials and analysis tools. J.L. and Y.C. prepared all figures and tables, and composed the main manuscript. All authors reviewed the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Lee, J., Kim, E., Kim, N. et al. Pulmonary toxicity of craniospinal irradiation using helical tomotherapy. Sci Rep 12, 3221 (2022). https://doi.org/10.1038/s41598-022-07224-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-07224-1
This article is cited by
-
Impact of delivery time factor on treatment time and plan quality in tomotherapy
Scientific Reports (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
