
Abstract
Risk factors for long-term non-motor symptoms and quality of life following subthalamic nucleus deep brain stimulation (STN DBS) have not yet been fully identified. In the present study, we investigated the impact of motor symptom asymmetry in Parkinson’s disease. Data were extracted for 52 patients with Parkinson’s disease (half with predominantly left-sided motor symptoms and half with predominantly right-sided ones) who underwent bilateral STN and a matched healthy control group. Performances for cognitive tests, apathy and depression symptoms, as well as quality-of-life questionnaires at 12 months post-DBS were compared with a pre-DBS baseline. Results indicated a deterioration in cognitive performance post-DBS in patients with predominantly left-sided motor symptoms. Performances of patients with predominantly right-sided motor symptoms were maintained, except for a verbal executive task. These differential effects had an impact on patients’ quality of life. The results highlight the existence of two distinct cognitive profiles of Parkinson’s disease, depending on motor symptom asymmetry. This asymmetry is a potential risk factor for non-motor adverse effects following STN DBS.
Similar content being viewed by others

Introduction
Although subthalamic nucleus deep brain stimulation (STN DBS) generally results in positive motor outcomes for patients with Parkinson’s disease (PD), the literature contains equivocal findings regarding its impact on cognition, with studies indicating negative effects1,2, although some have shown positive effects3,4,5. Studies of the neuropsychiatric effects of STN DBS6,7 are also far from unanimous, as some have reported a positive effect of STN DBS on neuropsychiatric symptoms5, while others have shown negative effects for apathy8, depressive symptoms and anxiety9, and emotion processing (for review see,10). As a consequence of these mixed results, current findings on quality of life in patients post-DBS are heterogeneous (for review see6,11).
One possible explanation for conflicting reports about the nature of STN DBS effects on cognitive performance, neuropsychiatric status, and quality-of-life measures is the heterogeneity of patients included in the studies. Recent studies in PD have focused on the impact of motor asymmetry on both cognition (for review see12) and social perceptual functions13 in pre-DBS conditions. They have highlighted different cognitive profiles for patients with PD who exhibit predominantly left-sided motor symptoms (LPD) versus those who exhibit predominantly right-sided motor symptoms (RPD), suggesting that LPD patients perform more poorly on tasks in the visuospatial modality, whereas RPD patients perform more poorly on tasks in the verbal modality or involving emotion processing12. A magnetic resonance imaging study also highlighted hemispheric differences in cortical degeneration in PD characterized by early left cortical atrophy, independent of motor symptom asymmetry14. Despite these indications of laterality effects in pre-DBS conditions, little research has been done on the non-motor impact of motor symptom asymmetry in patients post-DBS. In one recent study15, the authors found that LPD patients had impaired vocal emotion recognition for neutral, angry, happy, and sad voices before DBS that normalized after DBS, whereas RPD patients performed comparably to controls before DBS, but differed significantly on fear recognition after DBS. Although no significant difference was found between the RPD and LPD subgroups on any of the neuropsychological background tests in either the pre- or postoperative conditions, comparisons with healthy controls (HCs) suggested a potentially greater post-DBS deterioration in cognitive performance in LPD patients than in RPD patients. Regarding neuropsychiatric status, RPD patients scored higher on anxiety than did LPD patients in the preoperative condition, but no significant difference was found in the postoperative condition. In addition, RPD patients were more depressed than HCs in both the pre- and postoperative conditions, whereas LPD patients showed no depressive symptoms at any point. Finally, no effect was reported for apathy. These results suggest that neuropsychiatric profiles differ according to motor symptom asymmetry, with greater vulnerability of RPD patients but also a beneficial effect of DBS on anxiety in this subgroup. Given STN functional anatomy, these results suggest that DBS has a dissociative effect in the cognitive and affective domains, depending on motor symptom lateralization. Based on the integrative model of STN function put forward by Péron, et al.10, the study by Voruz, et al.15 supports the notion that although STN DBS typically restores motor functions, the surgery/stimulation can unintentionally impair non-motor functions. In this study, RPD patients (with inferred left cerebral pathology) did not exhibit any emotional impairment prior to surgery (probably owing to right hemispheric specialization of the basal ganglia for vocal emotion processing16), but developed emotional impairment in the wake of DBS. In contrast, LPD patients did display vocal emotional impairment prior to surgery (in line with the study by Stirnimann, et al.16), but this deficit normalized post-DBS. A recent study that used intracranial recordings corroborated this notion by showing that STN oscillations during emotion processing vary according to PD motor asymmetry17. From a clinical perspective, this could be crucial for patient management, as it points to a dissociative effect across the cognitive, neuropsychiatric, and motor domains post-DBS according to motor symptom asymmetry. To our knowledge, however, this has not yet been studied in a larger cohort in a pre- versus post-DBS condition, as in Voruz, et al.15 study.
In this context, our primary objective in the present study was to investigate changes in cognitive symptoms 12 months after DBS surgery in a cohort of 52 patients in comparison with the results of a baseline assessment conducted 3 months pre-DBS and the performances of an HC group. Patients were classified according to the lateralization of their motor symptoms (LPD vs. RPD). Our secondary objective was to measure the influence of motor symptom asymmetry and DBS on neuropsychiatric characteristics and physical and mental quality of life.
From overall findings in the literature, we made several predictions about the expected effects of motor symptom asymmetry on cognition, apathy and depression symptoms, and quality of life following DBS. First, on the basis of Voruz, et al.15 results in the neuropsychological domain, we expected to observe poorer performance on cognitive function tests post-DBS, but only for the LPD subgroup, with performance levels unchanged in the RPD subgroup. Second, we predicted that RPD patients would exhibit greater vulnerability to apathy and depression symptoms than would LPD patients and that DBS would have a beneficial effect on these symptoms in the RPD subgroup15. Third, from the results of Drapier, et al.7, we predicted that DBS would bring about an improvement in quality of life and that this improvement would be driven by the physical quality-of-life subscore. This improvement would be significant only in RPD patients, driven by a significant improvement in their motor symptoms, as observed by Voruz, et al.15.
Methods
Participants
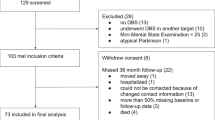
As described elsewhere18, we extracted data from the Rennes Hospital database for 52 patients with PD (26 RPD and 26 LPD patients) who had undergone bilateral STN DBS between 2004 and 2015, matched on age, sex, handedness, socio-education level, and disease duration. All patients met the criteria of the Parkinson’s UK Brain Bank for idiopathic PD19. Selection criteria for STN DBS followed international recommendations published in 199920 that include disabling levodopa (DOPA)-induced symptoms refractory to medical treatment (motor fluctuations and dyskinesias), disease > 5 years, and age < 70 years. All patients were implanted bilaterally in the STN with quadripolar DBS electrodes (monopolar stimulation). The locations of the electrodes were determined by using stereotactic coordinates derived from a three-dimensional computed tomography scan (coordinate of active electrode in Table 1). General information regarding STN DBS parameters are available in Table 1. Motor symptoms were assessed by using Part III of the Unified Parkinson’s Disease Rating Scale (UPDRS)21, the Hoehn and Yahr Scale (H&Y;22), the Schwab and England Scale (S&E;23), and the Activities of Daily Living scale24 in on- and off-DOPA conditions. The total levodopa-equivalent daily dose (LEDD) was calculated in accordance with Lozano, et al.25. The asymmetry of motor symptoms prior to DBS was retrospectively calculated on the lateralized items (items 20–26) of the UPDRS III21. Patients with a negative score were considered to be LPD patients and those with a positive score were considered to be RPD patients. None of the participants exhibited cognitive decline as measured with the Mattis Dementia Rating Scale26 (MDRS > 130), major executive decline, or DOPA-resistant axial motor signs.
Patients completed a clinical assessment (motor, cognitive, apathy, depression, and quality-of-life batteries) 3 months before the operation (on DOPA medication) and 12 months after it (on DOPA medication and on stimulation). Patient subgroups were compared with 25 HCs matched for age, sex, and sociocultural level (see Table 1), who had no history of neurological disease, head injury, or alcohol abuse and who displayed no signs of dementia.
The study was approved by the ethics committee of Rennes University Hospital and conducted in accordance with the Declaration of Helsinki. All patients gave their written informed consent before taking part.
Cognitive, apathy, depression, and quality-of-life assessments
Cognitive, apathy, depression, and quality-of-life assessments were administered to all patients included in the Rennes University Hospital cohort.
The cognitive battery included the MDRS26 and a series of tests that assessed frontal executive functions: the Modified Wisconsin Card Sorting Test (MCST,27, the Trail Making Test (TMT,28, the Categorical and Literal Fluency Test (2’)29, and the Stroop test30.
The assessment for depression and apathy symptoms included the Montgomery-Åsberg Depression Rating Scale (MADRS,31), chosen because of the predominance of psychological items over somatic items, thus limiting interference with PD symptoms, and the Apathy Evaluation Scale (AES,32), which yields a general apathy score, as well as subscores for emotional (AES-E), social (AES-S), and other (AES-O) apathy.
Finally, quality of life was assessed by using the Short Form 36-item Health Survey (SF-36,33, which yields separate mental and physical quality-of-life scores.
Statistical analysis
To compare the effects of DBS at different time points among LPD and RPD patients, as well as the differences between patients and HC, we ran one-tailed independent-sample t tests for intergroup comparisons and one-tailed dependent-sample t tests for intragroup comparisons on the normally distributed variables. For those variables with non-normal distributions (i.e., DBS parameters, MDRS, MCST), we performed a Kruskal–Wallis nonparametric one-way analysis of variance on ranks for intergroup comparisons between more than two groups (LPD patients 3 months pre-DBS; LPD patients 12 months post-DBS; RPD patients 3 months pre-DBS; RPD patients 12 months post-DBS; and HC group) and Mann–Whitney U tests if there was a significant group effect. For the nonparametric intragroup comparisons, we performed Wilcoxon matched pairs tests. All significant results (p < 0.05) are indicated in the tables according to the conditions being compared. Because we performed planned comparisons on the basis of operational hypotheses on a few sensible features and we report the results of all analyses and given the descriptive and advisory nature of this study, corrections for multiple comparisons were not performed. Nevertheless, to avoid an effect of inter-collinearity in a second step, we performed a false discovery rate (FDR) correction at each time point (pre- and post-DBS condition) and for each domain of results (motor, cognition, apathy/depression, and quality of life).
To quantify the relationships between the cognitive variables, sociodemographic factors, stimulation parameters, motor symptoms, neuropsychiatric variables, and quality-of-life data, we ran linear multiple regression forward stepwise analyses on ∆ scores (12-month post-DBS score—3-month pre-DBS score) for all variables. To reduce the likelihood of Type I errors, only variables that were found to differ significantly in intra- or intergroup comparisons were included in the models.
Analyses were performed with Statistica version 13.5.0.
Results
Stimulation parameters and electrode location
Interestingly, we observed a significant difference in voltage parameters between RPD and LPD subgroups (Table 1). LPD patients had a higher voltage than RPD patients did in the right STN (z = − 2.21, p = 0.02), and RPD patients tended to have a higher voltage than LPD patients did in the left STN (z = 1.73, p = 0.08). No other significant difference was found in stimulation parameters between LPD and RPD subgroups. No significant difference was found for electrode location, although it should be noted that data concerning electrode contact coordinates were missing for 21 patients.
DOPA therapy and motor effects of STN DBS (Tables 1 and 2)
A significant decrease in LEDD was observed in the postoperative condition in comparison with the preoperative condition within the two subgroups, whereas no significant difference was observed in intergroup comparisons.
There was a significant intragroup difference for RPD and LPD patients who were on medication and on stimulation regarding the UPDRS III score between the pre-DBS and the 12-month post-DBS conditions (Supplementary Table 1). Interestingly, intergroup analyses revealed a significant difference between the two subgroups on the S&E score in the off-DOPA condition at 12 months post-DBS (t = 2.57, p = 0.013, significant after FDR correction), with a higher score for LPD patients (Supplementary Table 2. All other results were nonsignificant.
Effects of STN DBS on cognition, apathy, depression, and quality of life
Cognition (Table 2 and Fig. 1)
In the pre-DBS condition, results revealed a significant difference between the LPD subgroup and the HCs on categorical verbal fluency (t = 2.04, p = 0.047).
In the post-DBS condition, results revealed no significant difference in cognitive performance between the RPD subgroup and the HC group at 12 months, except for categorical verbal fluency at 12 months post-DBS (t = 2.51, p = 0.015). However, there was a negative effect of DBS on the cognitive performance of the LPD subgroup, compared with the HC group, at 12 months. More specifically, this effect was observed for TMT B-A performance at 12 months post-DBS (t = − 2.11, p = 0.040) and MCST—Number of categories 12 months post-DBS (z = 2.26, p = 0.024).
After FDR correction, only the significant difference between RPD and HC for categorical verbal fluency at 12 months post-DBS and between LPD and HC for MCST—Number of categories at 12 months post-DBS survived. All other results were nonsignificant after FDR correction.
Apathy and depression (Supplementary Table 3)
Apathy. Intergroup analyses revealed a significant difference in the pre-DBS condition between RPD and LPD patients on the AES-O (t =− 2.12, p = 0.039) and AES-E (t = − 2.41, p = 0.020) subscales, suggesting greater other and emotional apathy in RPD patients (Supplementary Table 3, but only the AES-E result survived to FDR correction. Interestingly, no significant difference was observed between these two groups at 12 months post-DBS on the AES-O (t = − 1.18, p = 0.244) and AES-E (t =− 2.02, p = 0.052) subscales.
Depression. Analysis also revealed a significant difference in the pre-DBS condition between RPD and LPD subgroups and the HC group on the depression scale. Both patient subgroups had higher ratings than the HC group in the preoperative condition (LPD vs. HC: z = − 2.97, p = 0.003; RPD vs. HC: z = − 2.95, p = 0.003) and in the 12-month postoperative condition. All results survived to FDR correction (Supplementary Table 3).
All other results were nonsignificant.
Quality of life (Supplementary Table 4)
The intragroup analyses of scores on the two quality-of-life questionnaires indicated significant improvements in the SF-36 total score at 12 months and mainly on the subscales for the RPD subgroup (Supplementary Table 4). The SF-36 total (t = − 2.26, p = 0.033), global health (t = − 3.18, p = 0.004), physical role (t = − 2.30, p = 0.031), physical score (t = − 2.90, p = 0.008), and social function (t = − 3.34, p = 0.003) scores improved significantly at 12 months for RPD patients. After FDR correction, for the RPD subgroup, global health, physical score, and social function were still significant, whereas a significant improvement in LPD patients was reported for only the global health (t = − 2.40, p = 0.025) and physical pain (t = − 2.52, p = 0.019) scores and both results for LPD survived to FDR correction. All other results for SF-36 were nonsignificant.
Relationships among variables that distinguished between LPD and RPD patients and secondary measures
Significant differences were observed for the following variables of interest: on-DOPA on-stimulation UPDRS III, off-DOPA S&E, TMT B-A, categorical verbal fluency, phonemic verbal fluency, AES-E, AES-O, and SF-36 global health scores. Regression models were fitted for each variable to explore which additional measures best explained the observed group differences.
For the on-DOPA on-stimulation UPDRS III score, the best fit was achieved by using the SF-36 physical role score (R2 = 0.12, p = 0.043).
For the off-DOPA S&E score, the best fit was achieved by using the SF-36 physical function (R2 = 0.30, p = 0.002), off-DOPA H&Y (R2 = 0.10, p = 0.041), Stroop interference (R2 = 0.12, p = 0.016), AES-O (R2 = 0.08, p = 0.037), SF-36 physical function (R2 = 0.08, p = 0.022), AES-B (R2 = 0.05, p = 0.043), and MDRS total (R2 = 0.05, p = 0.031) scores.
For the TMT B-A score, the best fit was achieved by using the off-DOPA off-stimulation UPDRS III (R2 = 0.13, p = 0.037), off-DOPA H&Y (R2 = 0.10, p = 0.035), and SF-36 physical pain (R2 = 0.04, p = 0.018) scores.
For categorical verbal fluency, the best fit was achieved by using the LEDD (R2 = 0.14, p = 0.041) and SF-36 vitality (R2 = 0.18, p = 0.008) scores.
For phonemic verbal fluency, the best fit was achieved by using the SF-36 vitality (R2 = 0.28, p = 0.003), SF-36 physical (R2 = 0.15, p = 0.009), Stroop interference (R2 = 0.09, p = 0.028), SF-36 emotional role (R2 = 0.09, p = 0.016), and AES-E (R2 = 0.06, p = 0.024) scores.
For the AES-E score, the best fit was achieved by using the AES-B (R2 = 0.57, p < 0.001), SF-36 mental health (R2 = 0.08, p = 0.018), AES-Total (R2 = 0.06, p = 0.001), and SF-36 mental (R2 = 0.01, p = 0.040) scores.
For the AES-O score, the best fit was achieved by using the AES-Total (R2 = 0.52, p < 0.001), off-DOPA on-stimulation UPDRS III (R2 = 0.08, p = 0.026), and SF-36 physical (R2 = 0.10, p = 0.035) scores.
For the SF36 global health score, the best fit was achieved by using the off-DOPA H&Y (R2 = 0.19, p = 0.015), on-DOPA on-stimulation UPDRS III (R2 = 0.12, p = 0.035), AES-E (R2 = 0.10, p = 0.021), and TMT (R2 = 0.10, p = 0.003) scores.
Discussion
The aim of the present study was to investigate the cognitive, neuropsychiatric (apathy and depression), and quality-of-life profiles of patients with PD 12 months after STN DBS as a function of motor symptom asymmetry. According to recent research15, motor symptom asymmetry could be a meaningful predictor of non-motor performance following surgery. The present results seem to indicate that, at 12 months, DBS does not have a detrimental effect on cognitive measures for RPD patients (with inferred left cerebral pathology), whereas we did observe a harmful effect for LPD patients compared with HCs. In addition, whereas apathy seemed to be reduced for RPD patients, there were no changes in the severity of neuropsychiatric symptoms (i.e., apathy and depression scores) for LPD patients. As a consequence, DBS primarily had a beneficial effect on quality of life for RPD patients. These findings indicate that PD motor symptom asymmetry is a risk factor in the non-motor impact of STN DBS.
Before taking the interpretation any further, several main limitations need to be considered. First, the retrospective nature of the study, as well as the small size of the sample, represent limitations to the inferences that can be made from the present results. Second, the contacts used for chronic stimulation, according to the coordinates X, Y, Z, which were calculated with respect to the inter-commissural (anterior commissure-posterior commissure) line, did not allow precise localization of the stimulation contacts within the STN. The unavailability of contact coordinates for 21 subjects did not allow specific speculation about the direct effects of stimulation as a function of laterality of motor symptoms, and so these effects remain to be explored in future studies. Third, in our patient groups, we had two left-handed patients in each group. Although our groups were counterbalanced, the presence of patients with reverse brain asymmetry may have influenced the results. Fourth, one can argue that dopaminergic treatment may underlie the post-DBS effects, notably on apathy found in RPD patients. That being said, we failed to observe a significant difference between RPD and LPD patients for LEDD in both the pre- and postoperative conditions, or to find a significant correlation between LEDD and AES in the multiple regression analyses. Fifth and finally, we chose to discuss all our results for multiple comparisons, despite the fact that the majority of our results were still significant after FDR correction. We realize that the significance level of 0.05 was not maintained for all hypotheses combined. Nevertheless, our choice to discuss all of our results can be explained by the descriptive and advisory nature of this study, which would have excluded relevant data for the interpretation of the results, as well as by the fact that we had previously chosen to analyze only a limited number of features related to our hypotheses in order to present all the results and that we did not carry out a post hoc analysis afterwards.
Analysis of cognitive measures revealed differential effects of DBS as a function of motor symptom asymmetry. As predicted, cognitive performances were mostly preserved in RPD patients compared with those in HCs at 12 months post-DBS, the exception being scores on the executive verbal task, where performance worsened post-DBS. In contrast, at 12 months, the performances of LPD patients worsened on nonverbal executive functions compared with those in HCs. This pattern of results corroborates the post-DBS results reported by Hershey, et al.34, as well as those observed by Voruz, et al.35. A first interpretation of these results may be that they represent an overload effect of the DBS in the cerebral hemisphere ipsilateral to motor symptoms. Indeed, as postulated by Péron, et al.36, DBS would induce a desynchronizing effect on this ipsilateral associative loop through possible interconnectivity between the motor and associative areas of the STN37, or by a direct effect of the DBS on the associative loop38, while restoring the synchronization of the contralateral loops. That said, how can we explain that this effect would be more prominent for LPD than for RPD patients? A more critical and complex role of the left STN may be suspected, despite interhemispheric interaction between the large-scale networks involving the two STNs17. In the case of LPD patients, as suggested by our results, dynamics and connectivity between the basal ganglia and other cortical regions involving fine executive processing would be altered. The LPD subgroup’s poorer performance on the TMT B-A (not significant after FDR correction), the number of categories on the MCST (still significant after FDR correction), and verbal fluency (not significant after FDR correction) could be explained by an alteration of processes of connectivity involving the prefrontal, frontal, and basal ganglia regions of the left hemisphere39,40,41. A similar phenomenon could be hypothesized for the RPD subgroup, with a potential overload effect of the DBS on the right STN, but because tasks that investigate visuo-spatial performance are lacking, these phenomena could not be observed during our study. In the future, it would be interesting to perform wider neuropsychological testing (including exhaustive memory and visuo-spatial tests) post-DBS. Finally, in the very long term, we predict that LPD patients would be able to compensate for the detrimental effect of DBS and would deteriorate less cognitively. RPD patients, on the other hand, would remain stable in the first month post-DBS (except for visuo-spatial performances for the reasons evoked earlier), but are expected to exhibit major cognitive impairment in the very long term because of the well-known vulnerability of the left hemisphere to neurodegeneration, which was illustrated in our results by the worsening of verbal executive tasks in these patients42,43,44.
Analysis revealed no significant differences between the PD subgroups for depression symptoms. However, there were significant differences between LPD and RPD patients on the AES-E and AES-O subscores (only AES-E score survived to FDR correction). At the pre-DBS assessment, RPD patients scored higher than LPD patients on these two subscales, indicating greater apathy in RPD than in LPD patients. Interestingly, at 12 months post-DBS, LPD and RPD patients no longer differed significantly on the AES-O and AES-E subscales. Although we failed to observe intragroup effects, intergroup effects suggest a differential modification in post-DBS apathy as a function of motor asymmetry. These findings may suggest greater vulnerability of RPD patients for developing apathy symptoms in the natural evolution of the disease and that DBS has the potential to restore mood disorders in this patient subtype. Previous results that showed an increase in apathy may have been biased by the presence of unequal proportions of LPD and RPD patients45. Future empirical and meta-analytic studies are needed, considering the motor symptom asymmetry.
Finally, in line with our predictions, results for quality of life also differed according to motor symptom asymmetry. Notably, RPD patients exhibited post-DBS improvement in their quality of life across all domains (overall, global health, social function, physical role, and physical function scores) at 12 months post-DBS, whereas LPD patients did not display an improvement in the overall and physical scores or in the social function score. These results are in line with the literature suggesting an improvement in quality of life post-DBS in whole PD studies6; in addition, they demonstrate a weaker effect in LPD patients. These results may suggest that the improvement of quality of life observed in whole PD groups may have been driven by the RPD subgroup of patients, but this issue remains to be explored in future studies. Moreover, as expected, motor scores significantly predicted improvement in global health but, interestingly, the apathy (AES-E) and cognitive (TMT) scores were also significant predictors and may explain why quality of life is significantly less increased for the LPD subgroup, in whom cognitive performances decrease in postoperative conditions.
Conclusion
The current findings support the existence of two profiles of PD based on motor symptom asymmetry at disease onset that differ in terms of the impact of STN DBS on patients’ cognitive performance, apathy and depression symptoms, and mental and physical quality of life. It would therefore be useful to include asymmetry as a variable in future studies in order to better characterize these profiles and the effect of DBS on each, as well as to build better predictions of disease progression. Our results open a new avenue for research in the field of personalized medicine. An individualized approach could increase the efficacy of PD treatments, as well as prompt early recourse to cognitive-behavioral therapy in certain populations in order to limit cognitive decline.

Neuropsychological and cognitive performances of the LPD and RPD subgroups of patients with PD before (preoperative condition, baseline) and after (postoperative condition, M + 12) STN DBS and of the HC group. (A) For mental flexibility (TMT B-A score), LPD performed significantly worse than healthy controls in the post-DBS condition, whereas no significant differences were observed in the pre-DBS condition, as well as between RPD and healthy controls for the pre- and post-DBS condition. (B) For MCST—Number of categories, LPD performed significantly worse than healthy controls in the post-DBS condition, whereas no significant differences were observed in the pre-DBS condition, as well as between RPD and healthy controls for the pre- and post-DBS condition. DBS deep brain stimulation, LPD: predominantly left-motor symptoms, MCST modified Wisconsin card sorting test, RPD predominantly right-motor symptoms, TMT trail making test. *p < .050. **Significant after FDR correction.
Abbreviations
- AES:
-
Apathy evaluation scale
- DBS:
-
Deep brain stimulation
- DOPA:
-
Levodopa
- HC:
-
Healthy control
- H and Y:
-
Hoehn and Yahr scale
- LEDD:
-
Levodopa-equivalent daily dose
- LPD:
-
Patients with Parkinson’s disease exhibiting predominantly left-sided motor symptoms
- MCST:
-
Modified Wisconsin card sorting test
- MDRS:
-
Mattis dementia rating scale
- PD:
-
Parkinson’s disease
- RPD:
-
Patients with Parkinson’s disease exhibiting predominantly right-sided motor symptoms
- S and E:
-
Schwab and England scale
- SF-36:
-
Short form 36-item health survey
- STN:
-
Subthalamic nucleus
- TMT:
-
Trail making test
- UPDRS:
-
Unified Parkinson’s disease rating scale
References
Saint-Cyr, J. A., Trépanier, L. L., Kumar, R., Lozano, A. M. & Lang, A. J. B. Neuropsychological consequences of chronic bilateral stimulation of the subthalamic nucleus in Parkinson’s disease. Brain 123, 2091–2108 (2000).
Alegret, M. et al. Effects of bilateral subthalamic stimulation on cognitive function in Parkinson disease. Arch. Neurol. 58, 1223–1227 (2001).
Daniele, A. et al. Cognitive and behavioural effects of chronic stimulation of the subthalamic nucleus in patients with Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 74, 175–182 (2003).
Bove, F. et al. Dementia and subthalamic deep brain stimulation in Parkinson disease: A long-term overview. Neurology 95, e384–e392 (2020).
Appleby, B. S., Duggan, P. S., Regenberg, A. & Rabins, P. V. Psychiatric and neuropsychiatric adverse events associated with deep brain stimulation: A meta-analysis of ten years’ experience. Mov. Disord: Off J. Mov. Disord. Soc. 22, 1722–1728 (2007).
Geraedts, V., Feleus, S., Marinus, J., van Hilten, J. & Contarino, M. What predicts quality of life after subthalamic deep brain stimulation in Parkinson’s disease? A systematic review. Eur. J. Neurol. 27, 419–428 (2020).
Drapier, S. et al. Only physical aspects of quality of life are significantly improved by bilateral subthalamic stimulation in Parkinson’s disease. J. Neurol. 252, 583–588 (2005).
Drapier, D. et al. Does subthalamic nucleus stimulation induce apathy in Parkinson’s disease?. J. Neurol. 253, 1083 (2006).
Aarsland, D., Marsh, L. & Schrag, A. Neuropsychiatric symptoms in Parkinson’s disease. Mov. Disord.: Off. J. Mov. Disord. Soc. 24, 2175–2186 (2009).
Péron, J., Frühholz, S., Vérin, M. & Grandjean, D. Subthalamic nucleus: A key structure for emotional component synchronization in humans. Neurosci. Biobehav. Rev. 37, 358–373 (2013).
Daniels, C. et al. Is improvement in the quality of life after subthalamic nucleus stimulation in Parkinson’s disease predictable?. Mov. Disord. 26, 2516–2521 (2011).
Verreyt, N., Nys, G. M., Santens, P. & Vingerhoets, G. Cognitive differences between patients with left-sided and right-sided Parkinson’s disease. A Rev. Neuropsychol. Rev. 21, 405–424 (2011).
Coundouris, S. P., Adams, A. G., Grainger, S. A. & Henry, J. D. Social perceptual function in Parkinson’s disease: A meta-analysis. Neurosci. Biobehav. Rev. 104, 255–267 (2019).
Claassen, D. O. et al. Cortical asymmetry in Parkinson’s disease: early susceptibility of the left hemisphere. Brain Behav. 6, e00573 (2016).
Voruz, P. et al. Motor symptom asymmetry in Parkinson’s disease predicts emotional outcome following subthalamic nucleus deep brain stimulation. Neuropsychologia 144, 107494 (2020).
Stirnimann, N. et al. Hemispheric specialization of the basal ganglia during vocal emotion decoding: Evidence from asymmetric Parkinson’s disease and (18)FDG PET. Neuropsychologia 119, 1–11. https://doi.org/10.1016/j.neuropsychologia.2018.07.023 (2018).
Benis, D. et al. Subthalamic nucleus oscillations during vocal emotion processing are dependent of the motor asymmetry of Parkinson’s disease. NeuroImage 222, 117215 (2020).
Ahrweiller, K. et al. Postural instability and gait disorders after subthalamic nucleus deep brain stimulation in Parkinson’s disease: A PET study. J. Neurol. 266, 2764–2771 (2019).
Daniel, S. & Lees, A. Parkinson’s disease society brain bank, London: overview and research. J. Neural Transm. Suppl. 39, 165–172 (1993).
Defer, G. L., Widner, H., Marié, R. M., Rémy, P. & Levivier, M. Core assessment program for surgical interventional therapies in Parkinson’s disease (CAPSIT-PD). Mov. Disord.: Off. J. Mov. Disord. Soc. 14, 572–584 (1999).
Fahn, S. & Elton, R. UPDRS program members. Unified Parkinson’s disease rating scale. Recent Develop. Parkinson’s Dis. 2, 153–163 (1987).
Hoehn, M. & Yahr, M. Parkinsonism: Onset, progression and mortality. Neurology 50, 318–318 (1967).
Schwab, R. S. in Third symposium on Parkinson's disease. 152-157 (E&S Livingstone).
Schwab, R. S., England, A. C., Poskanzer, D. C. & Young, R. R. Amantadine in the treatment of Parkinson’s disease. JAMA 208, 1168–1170 (1969).
Lozano, A. M. et al. Effect of GPi pallidotomy on motor function in Parkinson’s disease. The Lancet 346, 1383–1387 (1995).
Mattis, S. Dementia Rating Scale: Professional Manual. (Psychological Assessment Resources, Incorporated, 1988).
Nelson, H. E. A modified card sorting test sensitive to frontal lobe defects. Cortex 12, 313–324 (1976).
Reitan, R. M. Validity of the trail making test as an indicator of organic brain damage. Percept. Mot. Skills 8, 271–276 (1958).
Cardebat, D., Doyon, B., Puel, M., Goulet, P. & Joanette, Y. Formal and semantic lexical evocation in normal subjects. Performance and dynamics of production as a function of sex, age and educational level. Acta neurologica belgica 90, 207–217 (1990).
Stroop, J. R. Studies of interference in serial verbal reactions. J. Exp. Psychol. 18, 643 (1935).
Montgomery, S. & Asberg, M. MADRS scale. Brit. J. Psychiatr. 134, 382–389 (1979).
Marin, R. S., Biedrzycki, R. C. & Firinciogullari, S. Reliability and validity of the apathy evaluation scale. Psychiatr. Res. 38, 143–162 (1991).
Ware, J. E. Jr. & Sherbourne, C. D. The MOS 36-item short-form health survey (SF-36): I. Conceptual framework and item selection. Med. Care 30(6), 473–483 (1992).
Hershey, T. et al. Unilateral versus bilateral STN DBS effects on working memory and motor function in Parkinson disease. Exp. Neurol. 210, 402–408 (2008).
Voruz, P. et al. Motor symptom asymmetry in Parkinson’s disease predicts emotional outcome following subthalamic nucleus deep brain stimulation. Neuropsychologia 144, 107494 (2020).
Péron, J., Frühholz, S., Vérin, M. & Grandjean, D. Subthalamic nucleus: A key structure for emotional component synchronization in humans. Neurosci. Biobehav. Rev. 37, 358–373 (2013).
Arnold, A. S. et al. Resting-State functional connectivity of the subthalamic nucleus to limbic, associative, and motor networks. Brain Connect. 8, 22–32 (2018).
Jeune, Le. et al. Subthalamic nucleus stimulation affects limbic and associative circuits: A PET study. Eur. J. Nucl. Med. Mol. Imag. 37, 1512–1520 (2010).
Zakzanis, K. K., Mraz, R. & Graham, S. J. An fMRI study of the trail making test. Neuropsychologia 43, 1878–1886 (2005).
Jodzio, K. & Biechowska, D. Wisconsin card sorting test as a measure of executive function impairments in stroke patients. Appl. Neuropsychol. 17, 267–277 (2010).
Chouiter, L. et al. Partly segregated cortico-subcortical pathways support phonologic and semantic verbal fluency: A lesion study. Neuroscience 329, 275–283 (2016).
Donix, M. et al. APOE associated hemispheric asymmetry of entorhinal cortical thickness in aging and Alzheimer’s disease. Psychiatr. Res.: Neuroimag. 214, 212–220 (2013).
Whitwell, J. L. et al. Frontal asymmetry in behavioral variant frontotemporal dementia: Clinicoimaging and pathogenetic correlates. Neurobiol. Aging 34, 636–639 (2013).
Beste, C. et al. Alterations in voluntary movement execution in Huntington’s disease are related to the dominant motor system: Evidence from event-related potentials. Exp. Neurol. 216, 148–157 (2009).
Boon, L. I. et al. Structural and functional correlates of subthalamic deep brain stimulation-induced apathy in Parkinson’s disease. Brain Stimul. 14, 192–201 (2021).
Funding
The present study was performed at the Neurology Department of Rennes University Hospital, France (Prof. Vérin). The first author was funded by Swiss National Foundation grant no. 105314_182221 (PI: Dr Julie Péron). The funders had no role in data collection, discussion of content, preparation of the manuscript, or decision to publish. The authors report no conflicts of interest.
Author information
Authors and Affiliations
Contributions
(1) Research project: A. Conception, B. Organization, C. Execution; (2) Statistical Analysis: A. Design, B. Execution, C. Review and Critique; (3) Manuscript: A. Writing of the first draft, B. Review and Critique. P.V.: 1A, 3C, 2A, 2B, 3A, 3B J.P.: 2C, 3B K.A.: 1C, 2A, 3B C.H.: 1C, 3B P.S.: 1C, 3B S.D.: 1C, 3B D.D.: 1C, 3B M.V.: 1A, 1B, 1C, 2C, 3B J.A.P.: 1A, 1B, 1C, 2B, 2C, 3A, 3B.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Voruz, P., Pierce, J., Ahrweiller, K. et al. Motor symptom asymmetry predicts non-motor outcome and quality of life following STN DBS in Parkinson's disease. Sci Rep 12, 3007 (2022). https://doi.org/10.1038/s41598-022-07026-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-07026-5
This article is cited by
-
Moderating effects of uric acid and sex on cognition and psychiatric symptoms in asymmetric Parkinson’s disease
Biology of Sex Differences (2023)
-
Study of the relationship between onset lateralization and hemispheric white matter asymmetry in Parkinson's disease
Journal of Neurology (2023)
-
Imbalanced motivated behaviors according to motor sign asymmetry in drug-naïve Parkinson’s disease
Scientific Reports (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
