
Abstract
Acute lymphoblastic leukemia (ALL) is the most common type of childhood cancer. Treatments of ALL predispose survivors to obesity, which increases the risk of cardiovascular disease and diabetes. The hallmark of obesity is excess fat mass, and adiposity is a superior predictor of cardiometabolic risk when compared to Body Mass Index (BMI), yet clinical measures of adiposity in children are lacking. The Tri-Ponderal Mass Index (TMI) (kg/m3) is a more accurate adiposity measure compared to BMI z-score in the general pediatric population. This cross-sectional study aimed to validate TMI as an adiposity measure against DEXA scan-derived adiposity, and to compare it to BMI z-score, in pediatric ALL survivors. This study was a retrospective chart review of pediatric ALL survivors diagnosed between 2004 and 2015 at McMaster Children’s Hospital, a tertiary pediatric center in Ontario, Canada. One hundred and thirteen patients (Female n = 55, 48.70%) were included, and adiposity was measured using DEXA scans. Exploratory partial correlations and linear regression analyses were adjusted for age, sex, ethnicity, and ALL risk status. Both TMI and BMI z-score correlated with the DEXA-measured fat mass percentage (FM%) (partial correlation TMI versus FM% r = 0.56; p value < 0.0001; BMI z-score versus FM% r = 0.55; p value < 0.0001). In regression analyses, the association of TMI was not inferior to BMI z-score in assessing adiposity (TMI versus FM% estimated unstandardized B 0.80, 95% CI 0.56, 1.02; p value < 0.0001; BMI z-score versus FM% (unstandardized B 0.37, 95% CI 0.26, 0.49; p value < 0.0001). The TMI is a useful clinical adiposity-specific measure in survivors of pediatric ALL.
Similar content being viewed by others

Introduction
Acute Lymphoblastic Leukemia (ALL) accounts for 25% of all childhood cancers, making it the most common pediatric malignancy with a worldwide incidence of 1–4.75/100,0001,2.
These children undergo 2–3 years of multimodal chemotherapy, including treatment with corticosteroids3. Some children with the high-risk disease would also receive craniospinal irradiation or hematopoietic stem cell transplantation4,5,6. Survival of children with ALL has reached around 90% in some high-income countries7,8,9. However, these survivors are at risk of developing cardiometabolic disorders including obesity, metabolic syndrome, type 2 diabetes mellitus, and cardiovascular diseases. Obesity is one of the significant drivers of adverse outcomes and, together with cardiometabolic disorders, can impact the quality of life and life expectancy of these survivors1,10,11,12,13,14,15,16,17.
The causes of obesity in this population are multifactorial and include steroids and radiotherapy, obesity at diagnosis, and sedentary lifestyle. Obesity can be associated with metabolic abnormalities including dyslipidemia and dysglycemia12,13,18,19. While weight management interventions have been attempted during and after therapy, they have had a limited success20.
The expansion of the adipose tissue compartment is the hallmark of obesity; epidemiological evidence suggests that adiposity is a robust predictor of cardiovascular diseases and type 2 diabetes mellitus risk markers in children compared to the most common clinical diagnostic measure of obesity, the Body Mass Index (BMI)21,22.
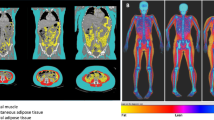
The protocols used for treating children with ALL recommend regular assessments of bone health using Dual-Energy X-ray Absorptiometry (DEXA) as the gold standard17,23,24. While DEXA scans measure the bone mass, they also incorporate measurements of the adipose tissue mass. As adiposity is an essential driver of cardiometabolic risk, adipose tissue assessment may help predict future cardiometabolic risk and is an attractive approach to identify at-risk survivors.
However, DEXA scans are expensive, require designated space for the specialized equipment, and need trained personnel to use the machinery and interpret the scans25,26,27,28. Defining clinical adiposity measures can help measure fat mass changes during and post-treatment. It may also help evaluate the response to future adiposity management interventions in survivors, as these interventions are currently lacking20.
The Tri-Ponderal Mass Index (TMI) was recently validated as a more accurate measure of adiposity than Body Mass Index (BMI) and BMI z-score in the general pediatric population and survivors of childhood brain tumors29,30. Importantly, the TMI utilizes the height and weight measurements recorded in routine clinical settings and considers childrens’ growth patterns by adjusting weight to height cubed (kg/m3) versus the conventional use of height squared in BMI-based calculations (kg/m2)29.
The aim of this study was to validate TMI as a clinical measure of adiposity against DEXA compared to the BMI z-score in childhood ALL survivors.
Results
Population characteristics
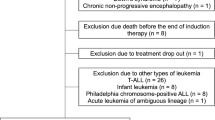
The details of participants are reported in Table 1. Of the 113 participants included in this study, 55 (48.70%) were female. Both males and females had similar age at diagnosis (male 6.20 ± 5.10 years; female 5.10 ± 3.50 years) and at the first DEXA scan post-therapy (male 10.40 ± 5.60 years; female 9.90 ± 4.90 years). The majority of participants were Caucasian (n = 97, 85.80%; female n = 47, 85.50%).
The anthropometric data and DEXA scan measures of body composition are reported in Table 2. Males were taller and had a higher weight when compared to females (height: male SDS 0.10 ± 1.10, female SDS -0.07 ± 1.10; weight: male SDS 0.17 ± 1.20, female SDS − 0.10 ± 0.90). While BMI percentiles were similar between males and females (male 66.50 ± 32.80; female 63.20 ± 34.70), the BMI z-scores were higher in male participants when compared to females (male 0.70 ± 1.40; female 0.60 ± 1.30). The TMI measures were similar in both sexes (male 14.90 ± 3.00; female 14.80 ± 3.00).
Eight females (14.50%) and eight males (13.80%) had a TMI > 85th percentile signifying excess adiposity. The female TMI cut-off was 17.20 kg/m3 (range 17.20–26.50) and male TMI cut-off was 17.70 kg/m3 (range 17.70–26.40).
ALL treatments
The details of the ALL subtypes, risk status, and treatment protocols are reported in Table 3. B-cell ALL was the most common subtype (n = 102, 90.20%). Most ALL cases were in the standard risk category (n = 78, 69.00%), while 32 (28.30%) were in the high-risk category. All 113 patients were treated with Dana-Farber Cancer Institute (DFCI) protocols between 2004 and 201531,32,33,34. The majority of patients were treated according to DFCI ALL Consortium Protocol 05–001 (DFCI 05–001) approved and activated in 2005 (n = 77, 68.20%)31,32,33,34. Steroid regimens in the treatment protocols are reported in Supplementary Table S1. Five patients received craniospinal irradiation (male n = 3, 1650.00 ± 653.80 cGy; female n = 2, 1500.00 ± 424.30 cGy).
Associations of TMI and BMI z-score with DEXA-based adiposity measures
Spearman’s correlation analyses were conducted to assess the correlation between body mass and adiposity measures and unadjusted and age, sex, ethnicity, and ALL risk status-adjusted partial correlations are reported in Table 4. The TMI correlated strongly with BMI z-score (r = 0.81; p value < 0.0001) and both TMI and BMI z-score demonstrated a positive correlations with DEXA-derived FM% (TMI r = 0.56, p value < 0.0001; BMI z-score r = 0.55, p value < 0.0001).
To further assess TMI associations with DEXA-based adiposity, multivariable regression analysis with adjustments for age, sex, ethnicity, and ALL risk status was conducted (Table 5). The TMI was associated with the DEXA-based fat mass percentage (FM%; unstandardized B 0.80; 95% CI 0.56, 1.02; p value < 0.0001). A similar regression analysis was repeated with the BMI z-scores and demonstrated its association with the FM% (unstandardized B 0.37; 95% CI 0.26, 0.49; p value < 0.0001).
To further compare the associations of the TMI and BMI z-scores with DEXA-based adiposity, we generated the Receiver Operating Characteristic (ROC) curve (Fig. 1) and calculated the Area Under the Curve (AUC). The analysis demonstrated that both TMI and BMI z-score were excellent tests to predict the DEXA-based adiposity (TMI: AUC 0.81, 95% CI 0.71–0.91, p value < 0.0001; BMI z-score: AUC 0.86, 95% CI 0.76–0.97, p value < 0.0001).

The ROC curve for the TMI and BMI z-score association with the DEXA-based fat mass percentage (FM%).
Furthermore, the TMI was associated with the BMI z-score (unstandardized B 1.80, 95% CI 1.65, 2.05; p value < 0.0001).
Taken together, TMI and BMI z-score is associated with DEXA-based total adiposity measures in pediatric survivors of ALL.
Discussion
The advent of novel ALL therapies has transformed the life expectancy of children with ALL over the past few decades35. With the reduction in premature mortality, there has been a widened focus on mitigating the burden of morbidities of ALL and its treatment20.
Some of the most significant morbidities reported in survivors include adverse cardiometabolic health outcomes such as type 2 diabetes and cardiovascular diseases17,36. As adiposity is a predictor of adverse cardiovascular and metabolic outcomes, reliable biological and clinical markers of adiposity are urgently needed to identify and target survivors with interventions that mitigate cardiometabolic risk. This study demonstrated that TMI, similar to BMI z-score, is significantly associated with DEXA-based total adiposity measures in pediatric ALL survivors. However, as an adiposity-specific measure, TMI has several important advantages when compared to BMI-based measures to estimate adipose tissue mass.
TMI has a stronger association with total adiposity in the general pediatric population compared to BMI z-score, the latter being inaccurate in estimating adiposity and misclassifying physically advanced children as being overweight or obese29,37,38,39,40.
Also, TMI is associated with central adiposity measures, especially waist-to-height ratio, in the general pediatric population and survivors of childhood brain tumors30,41,42. While our data demonstrate that TMI and BMI z-scores are comparable in their association with total adiposity, TMI is a more specific measure of total adiposity. This specificity may offer an added advantage in the childhood ALL survivors when estimating the adipose mass. The adipose tissue-specific nature of TMI, along with it being sex-specific and age- and puberty-independent offers a useful clinical tool that can be tracked longitudinally to assess changes in adiposity in survivors. Importantly, it can also be used to track responses to interventions to manage adiposity in this population.
An important question is whether TMI can predict cardiometabolic outcomes across the lifespan. While TMI is inferior or equal to BMI z-scores in detecting insulin resistance, it is a better predictor of metabolic syndrome in children than BMI43,44,45, and is positively associated with systolic and diastolic blood pressure in obese youth, although the latter association has not been consistently reported46,47,48,49.
Also, childhood BMI and TMI can predict adult obesity, type 2 diabetes, increased carotid intima-media thickness, and elevations in Low-Density Lipoprotein in the general population43. However, the use of TMI as a tool to predict long-term cardiometabolic outcomes in ALL survivors needs further characterization, as there are likely differences between ALL patients and the general population regarding the mechanisms driving adiposity in these groups.
Pediatric ALL patients are exposed to corticosteroids throughout their treatment32,33,34, which leads to excess adiposity, increased appetite, weight gain, and decreased bone mineral density17,50,51,52. Importantly, steroid treatment leads to the expansion of the total fat mass and is not associated with the redistribution of fat from the limbs to the trunk53, This makes TMI a valid tool to assess adiposity in survivors, as most of the steroid-driven weight gain is related to adipose tissue expansion rather than generalized growth, including muscle and bone compartments pattern seen with exogenous obesity53.
One of the strengths of this study is that we report on the association of TMI with total adiposity in ALL survivors, a population that has not been previously studied. We have also validated the TMI against DEXA, the gold standard in adiposity measurement.
One of the study's limitations is that no central adiposity measures were included in the analysis, and this should be the goal of future studies. The correlation of TMI with waist-to-height ratio and a lesser extent waist-to-hip ratio, as central adiposity measures have been documented30, and would be quite essential to replicate in the ALL population that is already at higher risk of adverse cardiometabolic disorders when compared to the general population. The study's cross-sectional nature is another limitation, as the evolution of TMI measures over time would be essential to assess. The inclusion of pubertal staging and its correlation with TMI in ALL survivors is important, as adiposity increases throughout puberty, particularly in females39.
Conclusion
In conclusion, this study reports the association of TMI and BMI z-score with DEXA measures of adiposity in survivors of ALL. This study's findings provide further evidence that TMI is an accurate and feasible clinical marker of adiposity in this population that is at high risk of cardiometabolic disorders. Also, the TMI is advantageous as an age-independent and sex-specific measure of adiposity than BMI z-scores. This allows the use of constant cut-offs to determine adiposity in different pediatric populations, including childhood ALL survivors. There is a need to validate TMI use in ALL survivors to decide whether it can predict long-term cardiometabolic outcomes.
Methods
Participants
This study was a cross-sectional study of pediatric ALL survivors who were diagnosed between August 2004-June 2015 at McMaster Children’s Hospital, a tertiary pediatric academic center in Hamilton, Ontario, Canada. One hundred and thirteen patients (n = 55 female, 48.70%) had DEXA data available for analysis. The study was a retrospective chart review approved by the Hamilton Integrated Research Ethics Board that exempted the study from consent requirements, as the retrospective chart review design involved the deidentification of the data after collection. The study procedures were performed following the relevant guidelines and legal regulations.
Data were obtained from patient charts through electronic medical record systems. The anonymized data were collected at the end of treatment for each patient, including age, age at diagnosis, sex, ethnicity, ALL subtype, ALL risk status, and treatment data. Anthropometric measures, including height and weight, were collected, with the height measured to the closest 0.1 cm and weight measured to the nearest 0.1 kg. For the DEXA scan data bone mineral content, bone density, bone mineral apparent density, total fat (kg), fat mass percentage (FM%), and lean body mass were retrieved from the patient’s first available DEXA scan post completion of therapy. The mean duration between the completion of treatment and the DEXA scan was 22.30 ± 29.70 months.
BMI and TMI calculations
The BMI and TMI were calculated using height and weight measurements. BMI was calculated as the weight (kg) divided by the height squared in meters (m2)29, while TMI was calculated as the weight (kg) divided by height cubed in meters (m3)29. BMI percentiles were calculated using the World Health Organization Growth Charts for Canada54 and BMI z-scores were calculated using the Calculator from the Centres for Disease Control and Prevention anthropometric Z-scores calculator55. Fat Mass Percentage (FM%) were obtained from DEXA scans (Hologic densitometer (Discovery A; Hologic, Inc, Bedford, Massachusetts). Puberty data were unavailable.
Statistical analyses
Statistical analyses were performed using SPSS Version 25.0 for Macintosh56. Data are presented as frequencies (%) for categorical variables and means (SD) for continuous variables. Box plots and visual inspections were used to identify outliers for removal from the analysis. Data distribution was assessed for normality using the Shapiro–Wilk and Kolmogorov–Smirnov tests57. The age, BMI z-score, TMI, and FM% variables were log-transformed to account for non-normal distributions.
Unadjusted as well as partial correlations of the associations between TMI, BMI, and DEXA-based adiposity measures were performed that were adjusted for age, sex, ethnicity, and ALL risk status. Multivariable linear regression analyses were conducted to assess the associations of total body mass and adiposity with TMI. The dependent variable was the FM% or BMI z-score, and the independent variables were TMI, age, sex, ethnicity, and ALL risk status. Results were reported as standardized and unstandardized beta coefficients with 95% confidence intervals and associated p values with statistical significance set at α of 0.05. The ROC curve and AUC calculations were used to further examine the association of TMI with DEXA-based adiposity58.
Data availability
The data for the current study used for statistical analysis are available from the corresponding author upon reasonable justification.
References
Pui, C.-H., Robison, L. L. & Look, A. T. Acute lymphoblastic leukaemia. Lancet 371, 1030–1043. https://doi.org/10.1016/s0140-6736(08)60457-2 (2008).
Redaelli, A., Laskin, B. L., Stephens, J. M., Botteman, M. F. & Pashos, C. L. A systematic literature review of the clinical and epidemiological burden of acute lymphoblastic leukaemia (ALL). Eur. J. Cancer Care 14, 53–62 (2005).
Stanulla, M. & Schrappe, M. Treatment of childhood acute lymphoblastic leukemia. Semin. Hematol. 46, 52–63. https://doi.org/10.1053/j.seminhematol.2008.09.007 (2009).
Pui, C. H. et al. Treating childhood acute lymphoblastic leukemia without cranial irradiation. N Engl. J. Med. 360, 2730–2741. https://doi.org/10.1056/NEJMoa0900386 (2009).
Hill, F. G. H. et al. Successful treatment without cranial radiotherapy of children receiving intensified chemotherapy for acute lymphoblastic leukaemia: results of the risk-stratified randomized central nervous system treatment trial MRC UKALL XI (ISRC TN 16757172). British Journal of Haematology 33, 33–46 (2004).
Janiszewski, P. M. et al. Abdominal obesity, liver fat, and muscle composition in survivors of childhood acute lymphoblastic leukemia. J. Clin. Endocrinol. Metab. 92, 3816–3821. https://doi.org/10.1210/jc.2006-2178 (2007).
Hunger, S. P. et al. Improved survival for children and adolescents with acute lymphoblastic leukemia between 1990 and 2005: a report from the children’s oncology group. J. Clin. Oncol. 30, 1663–1669. https://doi.org/10.1200/JCO.2011.37.8018 (2012).
Salzer, W. L. et al. Long-term results of the pediatric oncology group studies for childhood acute lymphoblastic leukemia 1984–2001: a report from the children’s oncology group. Leukemia 24, 355–370. https://doi.org/10.1038/leu.2009.261 (2010).
Bartram, J. et al. Excellent outcome of minimal residual disease-defined low-risk patients is sustained with more than 10 years follow-up: results of UK paediatric acute lymphoblastic leukaemia trials 1997–2003. Arch. Dis. Child. 101, 449–454. https://doi.org/10.1136/archdischild-2015-309617 (2016).
Chow, E. J., Pihoker, C., Hunt, K., Wilkinson, K. & Friedman, D. L. Obesity and hypertension among children after treatment for acute lymphoblastic leukemia. Cancer 110, 2313–2320. https://doi.org/10.1002/cncr.23050 (2007).
Veringa, S. J., van Dulmen-den Broeder, E., Kaspers, G. J. & Veening, M. A. Blood pressure and body composition in long-term survivors of childhood acute lymphoblastic leukemia. Pediatr. Blood Cancer 58, 278–282. https://doi.org/10.1002/pbc.23251 (2012).
Garmey, E. G. et al. Longitudinal changes in obesity and body mass index among adult survivors of childhood acute lymphoblastic leukemia: a report from the Childhood Cancer Survivor Study. J. Clin. Oncol. 26, 4639–4645. https://doi.org/10.1200/JCO.2008.16.3527 (2008).
Asner, S., Ammann, R. A., Ozsahin, H., Beck-Popovic, M. & von der Weid, N. X. Obesity in long-term survivors of childhood acute lymphoblastic leukemia. Pediatr. Blood Cancer 51, 118–122. https://doi.org/10.1002/pbc.21496 (2008).
Nuver, J., Smit, A. J., Postma, A., Sleijfer, D. T. & Gietema, J. A. The metabolic syndrome in long-term cancer survivors, and important target for secondary preventive measures. Cancer Treat. Rev. 28, 195–214. https://doi.org/10.1016/s0305-7372(02)00038-5 (2002).
Rosen, G. P., Nguyen, H. T. & Shaibi, G. Q. Metabolic syndrome in pediatric cancer survivors: a mechanistic review. Pediatr. Blood Cancer 60, 1922–1928. https://doi.org/10.1002/pbc.24703 (2013).
Razzouk, B. I. et al. Obesity in survivors of childhood acute lymphoblastic leukemia and lymphoma. J. Clin. Oncol. 25, 1183–1189. https://doi.org/10.1200/JCO.2006.07.8709 (2007).
Browne, E. K. et al. Changes in body mass index, height, and weight in children during and after therapy for acute lymphoblastic leukemia. Cancer 124, 4248–4259. https://doi.org/10.1002/cncr.31736 (2018).
Oeffinger, K. C. et al. Cardiovascular risk factors in young adult survivors of childhood acute lymphoblastic leukemia. J. Pediatr. Hematol. Oncol. 23, 424–430 (2001).
Tonorezos, E. S. et al. Contribution of diet and physical activity to metabolic parameters among survivors of childhood leukemia. Cancer Causes Control 24, 313–321. https://doi.org/10.1007/s10552-012-0116-6 (2013).
Wang, K. W. et al. Bariatric interventions in obesity treatment and prevention in pediatric acute lymphoblastic leukemia: a systematic review and meta-analysis. Cancer Metastasis Rev. 39, 79–90. https://doi.org/10.1007/s10555-020-09849-y (2020).
Koning, L., Denhoff, E., Kellogg, M. D. & Ferranti, S. D. Associations of total and abdominal adiposity with risk marker patterns in children at high-risk for cardiovascular disease. BMC Obes. https://doi.org/10.1186/s40608-015-0043-7 (2015).
Freedman, D. S., Mei, Z., Srinivasan, S. R., Berenson, G. S. & Dietz, W. H. Cardiovascular risk factors and excess adiposity among overweight children and adolescents: the Bogalusa Heart Study. J. Pediatr. 150, 12-17 e12. https://doi.org/10.1016/j.jpeds.2006.08.042 (2007).
Pietrobelli, A., Peroni, D. G. & Faith, M. S. Pediatric body composition in clinical studies: which methods in which situations?. Acta Diabetol. 40(Suppl 1), S270-273. https://doi.org/10.1007/s00592-003-0084-0 (2003).
Pietrobelli, A. & Tatò, L. Body composition measurements: From the past to the future. Acta Paediatr. 94, 8–13. https://doi.org/10.1080/08035320510035221 (2005).
Blijdorp, K. et al. Obesity is underestimated using body mass index and waist-hip ratio in long-term adult survivors of childhood cancer. PLoS ONE 7, e43269. https://doi.org/10.1371/journal.pone.0043269 (2012).
Gonzalez-Ruiz, K. et al. Comparison of bioelectrical impedance analysis, slaughter skinfold-thickness equations, and dual-energy X-ray absorptiometry for estimating body fat percentage in colombian children and adolescents with excess of adiposity. Nutrients https://doi.org/10.3390/nu10081086 (2018).
Huang, T. T. K., Watkins, M. P. & Goran, M. I. Predicting total body fat from anthropometry in latino children. Obes. Res. 11, 1192–1199. https://doi.org/10.1038/oby.2003.164 (2003).
Glickman, S. G., Marn, C. S., Suppiano, M. A. & Dengel, D. R. Validity and reliability of dual-energy X-ray absorptiometry for the assessment of abdominal adiposity. J. Appl. Physiol. 97, 509–514. https://doi.org/10.1152/japplphysiol.01234.2003 (2004).
Peterson, C. M. et al. Tri-ponderal mass index vs body mass index in estimating body fat during adolescence. JAMA Pediatr. 171, 629–636. https://doi.org/10.1001/jamapediatrics.2017.0460 (2017).
Sims, E. D. et al. Tri-ponderal mass index in survivors of childhood brain tumors: a cross-sectional study. Sci. Rep. 8, 16336. https://doi.org/10.1038/s41598-018-34602-5 (2018).
Angiolillo, A. L. AALL0932: Treatment of Patients with Newly Diagnosed Standard Risk B-Lymphoblastic Leukemia (B-ALL) or Localized B-lineage Lymphoblastic Lymphoma (B-LLy) A Groupwide Phase III Study. Children’s Oncology Group 5 (2010).
Silverman, L. B. Randomized Study of Intravenous Calaspargase Pegol (SC-PEG asparaginase) and Intravenous Oncaspar in Children and Adolescents with Acute Lymphoblastic Leukemia or Lymphoblastic Lymphoma. Dana-Farber Cancer Institute (2012).
Silverman, L. B. DFCI ALL Consortium Protocol 05–01: Treatment of Acute Lymphoblastic Leukemia in Children. Dana-Farber Cancer Institute (2007).
Silverman, L. B. Treatment of Acute Lymphoblastic Leukemia in Children and Adults Dana Farber Cancer Institute (DFCI) Consortium Protocol 2000–01. Dana Farber Cancer Institute (2000).
Yeh, J. M. et al. Life expectancy of adult survivors of childhood cancer over 3 decades. JAMA Oncol. https://doi.org/10.1001/jamaoncol.2019.5582 (2020).
Wilson, C. L. et al. Decline in physical activity level in the childhood cancer survivor study cohort. Cancer Epidemiol. Biomark. Prev. 23, 1619–1627. https://doi.org/10.1158/1055-9965.Epi-14-0213 (2014).
Maynard, L. M. et al. Childhood body composition in relation to body mass index. Pediatrics 107, 344–350. https://doi.org/10.1542/peds.107.2.344 (2001).
Neovius, M. & Rasmussen, F. Evaluation of BMI-based classification of adolescent overweight and obesity: choice of percentage body fat cutoffs exerts a large influence. The COMPASS study. Eur. J. Clin. Nutr. 62, 1201–1207. https://doi.org/10.1038/sj.ejcn.1602846 (2008).
Kaplowitz, P. B. Link between body fat and the timing of puberty. Pediatrics 121(Suppl 3), S208-217. https://doi.org/10.1542/peds.2007-1813F (2008).
Kaplowitz, P. B., Slora, E. J., Wasserman, R. C., Pedlow, S. E. & Herman-Giddens, M. E. Earlier onset of puberty in girls: relation to increased body mass index and race. Pediatrics 108, 347–353. https://doi.org/10.1542/peds.108.2.347 (2001).
Ibrahim, M. M. Subcutaneous and visceral adipose tissue: structural and functional differences. Obes. Rev. 11, 11–18. https://doi.org/10.1111/j.1467-789X.2009.00623.x (2010).
Nascimento, V. G., Bertoli, C. J., Gallo, P. R., Abreu, L. C. & Leone, C. Tri-ponderal mass index: a screening tool for risk of central fat accumulation in Brazilian preschool children. Medicina (Kaunas) https://doi.org/10.3390/medicina55090577 (2019).
Wu, F. et al. Association of youth triponderal mass index vs body mass index with obesity-related outcomes in adulthood. JAMA Pediatr. 172, 1192–1195. https://doi.org/10.1001/jamapediatrics.2018.3034 (2018).
Neves, F. S. et al. Tri-ponderal mass index is useful for screening children and adolescents with insulin resistance. Rev. Paul Pediatr. 38, e2019066. https://doi.org/10.1590/1984-0462/2020/38/2019066 (2020).
Matsuo, A. R. et al. Tri-ponderal mass index as a tool for insulin resistance prediction in overweight adolescents: A cross-sectional study. Nutrition 74, 110744. https://doi.org/10.1016/j.nut.2020.110744 (2020).
Ramírez-Vélez, R. et al. Tri-ponderal mass index vs. fat mass/height3 as a screening tool for metabolic syndrome prediction in colombian children and young people. Nutrients https://doi.org/10.3390/nu10040412 (2018).
Shim, Y. S. The relationship between tri-ponderal mass index and metabolic syndrome and its components in youth aged 10–20 years. Sci. Rep. 9, 14462. https://doi.org/10.1038/s41598-019-50987-3 (2019).
Park, H. K. & Shim, Y. S. Distribution of tri-ponderal mass index and its relation to body mass index in children and adolescents aged 10 to 20 years. J. Clin. Endocrinol. Metab. 105, e826-834. https://doi.org/10.1210/clinem/dgaa030 (2020).
Alfaraidi, H. et al. The Tri-ponderal Mass Index is associated with adiposity in adolescent type 2 diabetes mellitus: a cross-sectional analysis. Sci. Rep. 11, 9111. https://doi.org/10.1038/s41598-021-88705-7 (2021).
Iughetti, L., Bruzzi, P., Predieri, B. & Paolucci, P. Obesity in patients with acute lymphoblastic leukemia in childhood.pdf. Ital. J. Pediatr. https://doi.org/10.1186/1824-7288-38-4 (2012).
Winter, C., Muller, C., Hoffmann, C., Boos, J. & Rosenbaum, D. Physical activity and childhood cancer. Pediatr. Blood Cancer 54, 501–510. https://doi.org/10.1002/pbc.22271 (2010).
Hartman, A. et al. A randomized trial investigating an exercise program to prevent reduction of bone mineral density and impairment of motor performance during treatment for childhood acute lymphoblastic leukemia. Pediatr. Blood Cancer 53, 64–71. https://doi.org/10.1002/pbc.21942 (2009).
Konijn, N. P. et al. The short-term effects of two high-dose, step-down prednisolone regimens on body composition in early rheumatoid arthritis. Rheumatology 55, 1615–1622. https://doi.org/10.1093/rheumatology/kew221 (2016).
Dieticians of Canada. WHO Growth Charts for Canada, <https://www.dietitians.ca/Advocacy/Interprofessional-Collaborations-(1)/WHO-Growth-Charts> (2014).
Canadian Pediatric Endocrine Group. Calculator: CDC anthropometric Z-scores 0–20y, <https://apps.cpeg-gcep.net/quickZ_CDC/> (2016).
IBM SPSS Statistics for Macintosh, Version 25 (IBM Corp., Armonk, NY, 2017).
Razali, N. M. & Wah, Y. B. Power comparisons of Shapiro-Wilk, Kolmogorov-Smirnov, Lilliefors and Anderson-darling tests. J. Stat. Model. Anal. 2, 21–33 (2011).
Mandrekar, J. N. Receiver operating characteristic curve in diagnostic test assessment. J. Thorac. Oncol. 5, 1315–1316. https://doi.org/10.1097/JTO.0b013e3181ec173d (2010).
Author information
Authors and Affiliations
Contributions
A.W.Z, C.P, L.T, J.T.W, and M.C.S. conceived the study question. A.W.Z., C.P., and J.T.W. performed and facilitated data abstraction. A.W.Z, C.P, L.T, J.T.W, and M.C.S. performed the data analysis. A.W.Z. and M.C.S. drafted the manuscript and all authors reviewed and approved the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Zhang, A.W., Wiernikowski, J.T., Portwine, C. et al. The triponderal mass index as a measure of adiposity in pediatric survivors of acute lymphoblastic leukemia: a cross-sectional study. Sci Rep 12, 1404 (2022). https://doi.org/10.1038/s41598-022-05236-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-05236-5
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
