
Abstract
Strengthening tuberculosis diagnosis is an international priority and the advocacy for multi-disease testing devices raises the possibility of improving laboratory efficiency. However, the advantages of centralized platforms might not translate into real improvements under operational conditions. This study aimed to evaluate the field use of the Abbott RealTime MTB (RT-MTB) and Xpert MTB/RIF assays, in a large cohort of HIV-positive and TB presumptive cases in Southern Mozambique. Over a 6-month period, 255 HIV-positive TB presumptive cases were consecutively recruited in the high TB/HIV burden district of Manhiça. The diagnostic performance of both assays was evaluated against two different reference standards: a microbiological gold standard (MGS) and a composite reference standard (CRS). Results from the primary analysis (MGS) showed improved sensitivity (Se) and reduced specificity (Sp) for the Abbott RT-MTB assay compared to the Xpert MTB/RIF (RT-MTB Se: 0.92 (95% CI: 0.75;0.99) vs Xpert Se: 0.73 (95% CI: 0.52;0.88) p value = 0.06; RT-MTB Sp: 0.80 (0.72;0.86) vs Xpert Sp: 0.96 (0.92;0.99) p value < 0.001). The lower specificity may be due to cross-reactivity with non-tuberculous mycobacteria (NTMs), the detection of non-viable MTBC, or the identification of true TB cases missed by the gold standard.
Similar content being viewed by others


Introduction
Tuberculosis (TB) remains one of the leading causes of death and disease worldwide. The World Health Organization (WHO)'s End TB Strategy has set ambitious goals to be achieved by 2035: 90% reduction in TB incidence and 95% reduction in mortality compared with levels in 20151. In 2019, approximately 10 million people were estimated to be infected with TB and became ill1,2. Efforts to accelerate TB elimination rely on several factors, but efficient and timely diagnosis of the disease is of utmost importance3. In recent years, considerable progress has been made in improving global case detection rates, although the gap between the reported and estimated number of cases is still unacceptable. Around 3 million incident cases were not diagnosed in 2019 due to under-reporting and/or under-diagnosis1. Therefore, increasing case detection and strengthening the diagnostic cascade remains a priority. For that purpose, National Control Programmes need to foster laboratory networks by equipping them with rapid and accurate diagnostic technologies4,5.
In 2018, the WHO endorsed a list of essential novel tests for diagnosing TB6. Nucleic acid amplification tests (NAAT) have substantially advanced the investigation of Mycobacterium tuberculosis complex (MTBC) and have been recognized as promising tools in closing the gap between diagnosis and treatment. Not only are NAAT more sensitive and faster than traditional assays, they also allow more accurate and rapid resistance detection7,8,9. However, their application is limited due to lack of trained staff and availability of proper infrastructure in low resource settings8. In the last decade, the endorsement of the Xpert MTB/RIF (hereinafter Xpert) as an initial test for TB investigation has radically changed the landscape of TB diagnosis5. This cartridge-based molecular assay was designed for the Cepheid's GeneXpert System (module-based), which allows the rapid detection of the MTBC DNA and also detects more than 95% of mutations associated with rifampicin resistance10,11. Besides, this flexible and user-friendly platform, offers a complete range of tests for the diagnostic of many other infectious diseases12.
However, the molecular TB diagnostic pipeline is broader8,13. Recently, through the release of rapid communication, WHO made new recommendations on the use of molecular assays as initial tests for TB diagnosis (Xpert MTB/RIF, Xpert Ultra, and TrueNat MTB have shown to have good performance for the detection of TB and rifampicin resistance detection9). Additionally, in a Technical Expert Consultation Report, the WHO also evaluated the use of four centralized assays for similar purposes13.
The automated RealTime MTB assay has been developed by Abbott Molecular (Chicago, IL, USA; hereinafter RT-MTB) for the qualitative detection of MTB complex and genetic variants of rifampicin (RIF) and isoniazid (INH) resistance using the RT-MTB RIF/INH reflex option. The assay has been designed for testing on the Abbott m2000 System (m2000sp and m2000rt)14,15. These are high-throughput instruments, widely used for HIV-1 viral load monitoring, and a broad range of tests for other pathogens, including the recently discovered SARS-CoV-216. A major challenge for diagnostic laboratories is to enhance their operational productivity by integrating and simplifying laboratory techniques. The advocacy for high-capacity, multi-disease testing devices, mainly in settings with limited resources, provides the option of improving laboratory efficiency and cost-saving.
Early studies on the performance evaluation of the RT-MTB assay have shown varying results in both, clinical and in vitro analysis (Supplementary material, S1)14,17,18,19,20,21,22,23,24. While acceptable sensitivity and specificity values were achieved, few of these studies were conducted in high TB burden countries, and none of them were carried out on a large cohort of HIV-1 positive patients. People living with HIV (PLHIV) are one of the most vulnerable populations for TB disease, often paucibacillary and in whom other tests, such as Xpert, have shown lower sensitivity5. It is, therefore, crucial to use a diagnostic platform that will adequately identify MTB in individuals co-infected with HIV.
The aim of this study is to assess the diagnostic performance of the RT-MTB assay in a unique cohort of PLHIV in a high TB and HIV burden country25,26. To our knowledge, this is the first study that compares the performance analysis of RT-MTB and Xpert MTB/RIF in such a cohort using 2 different reference standards.
Materials and methods
Study design and setting
This is a prospective evaluation of the diagnostic performance of the Abbott RT-MTB and its RT-MTB RIF/INH assays. The study was conducted in the district of Manhiça, Maputo province, a rural area 80 km away from the capital with a population of approximately 190,000 inhabitants27. The HIV prevalence estimate in this district was 39.2% in 201228 and the latest published incidence rate of lab-confirmed TB among PLHIV (aged 18–47 years) is 847 per 100,000 population29.
Consecutive HIV-positive adults identified at the Manhiça District Hospital (HDM) were screened for any symptom compatible with TB, as recommended by WHO guidelines 30 between July to December 2016. Patients with at least one of the following symptoms: cough for any duration, hemoptysis, night sweats, fever or unintentional weight loss, were offered to participate in the study. Those who self-reported having received TB treatment within the previous 6 months were excluded. All samples were tested at the Centro de Investigação em Saúde de Manhiça (CISM) laboratory.
Study procedures
Participants were enrolled at the clinic of the National Tuberculosis Programme (NTP) in Manhiça village after informed consent and data were collected through specific questionnaires. Blood samples were obtained for viral load testing using the automated RealTime HIV-1 Assay (Abbott Molecular). If participants had no recent CD4 results (documented within the last 3 months), TruCount blood tubes (Becton Dickinson Biosciences, San Jose, CA) were also collected to determine T-cells counts by flow cytometry.
As part of the TB diagnostic workup, participants provided two sputum samples, which were received the day following enrolment at the CISM laboratory. Sputum induction was performed for individuals that were unable to provide sputum spontaneously. Clinically diagnosed or laboratory-confirmed TB patients were managed according to the National Tuberculosis Programme (NTP) guidelines and were started on TB treatment. In case of discordant results between RT-MTB (positive) and the standard of care (culture and Xpert negative), patients were contacted for re-evaluation and were requested to provide a third sputum sample to aid the decision of treatment iniciation. All participants were scheduled for a follow-up visit 2 months after enrolment. Those who did not attend the clinic on day 60 were contacted by telephone and interviewed.
Laboratory procedures
All diagnostic tests were performed in a TB Biosafety level 3 (BSL-3) laboratory, which is subject to external quality control and ISO certification.
Smear microscopy for both sputum specimens was performed by Ziehl Neelsen (ZN) staining. Results were reported as negative or on a scale of positive grades according to international standards. For each participant, specimens with the best quality were decontaminated using the Kubica method 31 and the resuspended pellet was used for all tests to compare diagnostic accuracy among homogeneous specimens (Fig. 1). For liquid cultures, 500 µl of the decontaminated pellet were inoculated into Mycobacterium Growth Indicator Tubes (MGIT) liquid medium and incubated in the Bactec MGIT 960 mycobacterial detection instrument (Becton Dickinson Microbiology System, USA) according to manufacturer´s instructions. Additionally, 200 µl were cultured in BD Lowenstein Jensen solid medium. After 42 days (for liquid culture) or 8 weeks (for solid culture) without growth, samples were classified as negative. In the case of positive results, MTBC was confirmed using ZN staining and BD TB Identification test (Becton Dickinson Microbiology System, USA). Phenotypic drug susceptibility tests (DST) were conducted on all positive cultures.

Laboratory flowchart. (*) The best quality sample was used to perform molecular tests.
Molecular assays were also performed according to the manufacturer´s instructions. Briefly, 500 µl of the sediment were processed by Xpert MTB/RIF after mixing with the specific Sample Reagent in a ratio of 1:3. Two milliliters of the mixture were transferred into the cartridge. Results were obtained in a maximum of 2 h. Similarly, for the RT-MTB assay, 500 µl of the decontaminated specimen were mixed with the specific inactivation reagent (LabMate, South Africa UK) in a ratio of 1:3 and were incubated for 1–48 h. Automated DNA extraction and sample preparation (addition of master mix) were performed on the m2000sp instrument followed by real-time PCR and automated result interpretation using the m2000rt instrument. Residual extracted nucleic acid aliquots from m2000sp deep well plates were stored at − 25 to − 15 °C for up to 90 days for drug susceptibility testing. Samples identified as MTBC positive by the RT-MTB were automatically selected by the “reflex” software on the m2000sp and tested for RIF and INH resistance using the RT-MTB RIF/INH assay32 Residual pellets were stored at − 25 to − 15 °C until the end of the study.
Statistical analysis
The statistical analysis was performed using R version 3.5.2 (The R Foundation for Statistical Computing Platform). Figures and tables were created using Excel Microsoft Office.
Baseline characteristics of individuals were reported using mean and standard deviation, proportions, or median and interquartile range, depending on the variable type. The diagnostic performance of the RT-MTB and Xpert MTB/RIF was assessed through calculation of sensitivity (Se) and specificity (Sp), negative and positive predictive values (NPV and PPV) of the tests (with binomial distribution 95% confidence intervals).
Two different cohorts were evaluated: the per-protocol cohort (those who completed the follow-up visit at month 2) and the intention-to-treat cohort (all patients initially enrolled irrespective of having follow-up visit). For the per-protocol cohort, we conducted a primary analysis using aggregated results on solid and liquid MTBC culture as a gold standard (hereinafter microbiological gold standard, MGS). Patients were classified as “microbiologically confirmed” if either liquid or solid culture was positive. If both cultures were contaminated, they were excluded from the analysis. Non-tuberculous mycobacteria (NTM) growths were considered negative for MTBC. Patients in whom culture or NAAT assays results were not available (contamination or invalid results) were excluded from the analysis. For a secondary diagnostic test evaluation, a composite reference standard (CRS) was made by combining culture results and clinical information on treatment initiation (blinded to RT-MTB results). Lastly, in our “intention to treat” cohort we compared results to the microbiological reference standard.
The McNemar’s test with continuity correction or the Exact nominal Symmetry Test when discordant cells had low counts, were used to evaluate a systematic difference between the performance of the Xpert and RT-MTB and against both reference standards.
Ethical considerations
This study was submitted to all relevant ethics boards. The protocol was approved by the CISM’s Internal Scientific Committee, the CISM’s Internal Bioethics Committee (CIBS – Comité Institucional de Bioética para a Saúde) and the National Bioethics Committee (CNBS—Comité Nacional de Bioética para a Saúde) with Ref Number 101/CNBS/2016. All individuals provided written informed consent to participate. The study methods were carried out under the relevant guidelines and regulations established by the National Bioethics Committee at the Ministry of Health.
Results
During the 6-month study period, 255 HIV-positive and TB presumptive individuals were enrolled following informed consent. Of these, only 227 patients provided sputum samples for TB investigation. Eleven participants were excluded due to the unavailability of test results and therefore, a total of 216 patients were included in the final analysis (Fig. 2).

Participant enrolment flowchart. *Participants tested negative for TB at the initial visit.
The sociodemographic and clinical characteristics of all participants were assessed (Table 1). The median age was calculated as 27 years [IQR 23;35], with 51.4% of them (111/216) identified as female and 58.3% (126/216) were on antiretroviral therapy (ART).
Per-protocol cohort
From 216 patients, 23.1% (50/216) did not attend the clinic for the 2-month follow-up visit and were excluded from the per-protocol analysis. All of them tested negative for TB at the initial visit, and based on NTP records, they did not start treatment during the study period. Of the final cohort of 166 patients, 15.6% (26/166) were TB positive by aggregated culture results, 8.4% (14/166) were smear positive, 11.4% (19/166) were positive by Xpert and 14.4% (24/166) by RT-MTB (Table 2).
Primary analysis, (MGS)
Table 3 provides comprehensive results on the performance of the Xpert and RT-MTB assays for both study cohorts using aggregated culture as the gold standard. Overall, Xpert sensitivity was lower than RT-MTB, (0.73 (95% CI: 0.52–0.88) vs 0.92 (95% CI: 0.75–0.99) p value = 0.06) respectively. In both tests, sensitivity decreased among smear negative patients, maintaining the improved but weak statistical evidence on the performance of RT-MTB over Xpert (p value = 0.063). Conversely, there was strong evidence of differences in specificity and PPV between Xpert and RT-MTB in all cases (i.e. overall Xpert Sp: 0.96 (0.92;0.99) vs RT-MTB Sp: 0.80 (0.72;0.86), p value < 0.001; overall PPV: 0.79 (0.58;0.93) vs 0.46 (0.32; 0.61)).
Secondary analysis, (CRS)
The diagnostic test values of the per-protocol cohort using the CRS are provided in Table 4. From Table 2, 27.7% (46/166) of participants were diagnosed with TB. Twenty-six of them tested positive for MTBC culture while the remaining twenty individuals started TB treatment per clinical criteria. The overall sensitivity of the three assays dropped when the results of the CRS and MGS were compared. As seen previously, RT-MTB and Xpert did not show systematic differences in sensitivity, except for smear negative patients (RT-MTB Se: 0.48 (0.30;0.67) vs Xpert Se: 0.29 (0.14;0.48) p value = 0.05).
The 22 RT-MTB false-positive subjects were further characterized. Based on culture results, 27.3% (6/22) were found to be positive for NTM. Three participants died after the 2-month study follow-up, four had been previously treated for TB and two of them had completed treatment only 1 year before enrolment. Follow-up results are provided in Supplementary material (S2). Additionally, cross-contamination into the Abbott m2000sp instrument was assessed. No amplification of MTBC was detected in surrounding samples of those theoretically considered false-positive.
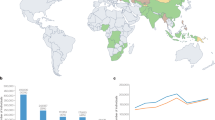
Figure 3 illustrates test values and 95%CI by test and reference standard. Figures 4 and 5 shows projections of positive predictive values (PPV) and negative predictive values (NPV) by pre-test probability.

Bar chart illustrating sensitivity and specificity values by reference standard. On the left-side overall values are displayed; on the right-side, test values among smear negative patients. Line chart represents 95% confidence intervals.

Xpert and RT-MTB PPVs and NPVs by pre-test probability. The prevalence applied has been calculated relying on the microbiological reference standard. NPV negative predicted value, PPV positive predicted value, Pre prevalence.

Xpert and RT-MTB PPVs and NPVs by pre-test probability. The prevalence applied has been calculated relying on the composite reference standard. NPV negative predicted value, PPV positive predicted value, Pre prevalence.
Intention-to-treat cohort
The overall test performance of the intention-to-treat cohort was found to be similar to the per-protocol cohort of patients, as shown in Table 3. Overall, we did not find systematic differences in sensitivity between assays although Xpert´s specificity was higher in all cases (overall Xpert Sp: 0.97 (0.94;0.99) vs RT-MTB: 0.80 (0.74;0.86) p value < 0.001). Findings were also stratified by smear microscopy and final data is detailed in Tables 2 and 3.
Threshold cycle number values for RT-MTB and RT-MTB RIF/INH results
Overall, the mean threshold cycle number (Cn) was 28.42 (SD 7.25), and 35.67 (SD 18.45) for false-positive samples. Concerning drug susceptibility, Xpert yielded 100% valid results (24 over 24 Xpert-positives results), compared to 34.6% (18 out of 52 positives by RT-MTB). Neither Xpert nor RT-MTB detected gene targets for rifampicin resistance, whereas markers for isoniazid monoresistance were identified in 2 patients by RT-MTB RIF/INH assay. From those samples without RT-MTB RIF/INH results (35/52), 21 of them proved below the limit of detection (LoD). When comparing with phenotypic DST, 57.7% (15/26) of culture positive cases got a resistance profile from RT-MTB RIF/INH assay. Fourteen of these results (14/15, 93.4%), agreed with the phenotypic DST. The only one discordant sample harbored a mutation related to low level of isoniazid resistance which did not translate into phenotypic resistance.
Operational characteristics and challenges
Our laboratory follows rigorous quality control procedures and instrument track records were registered and detailed in specific laboratory logbooks. For a head-to-head comparison of Xpert and RT-MTB assays, lab records were compared. The outcome indicated that the m2000 System required various interventions and repeated runs, as well as routine preventive maintenance. A list of technical interventions has been drawn up in Supplementary material (S3).
Discussion
This study aimed to evaluate the performance of the RT-MTB in a high TB and HIV burden region. To our knowledge, this is the largest study evaluating the RT-MTB diagnostic assay in clinical samples from a unique cohort of HIV-positive patients. We utilized the m2000 System for both HIV-1 viral load quantification and MTBC detection, with the purpose of adding evidence for the implementation of high-throughput and multi-disease testing on a single device.
Data on the clinical performance of the RT-MTB for the diagnosis of TB is limited and reported diagnostic values differ across studies (S1). In this clinical study, we compared both, RT-MTB and Xpert assays, to identify MTBC among PLHIV using two different reference standards. For the per-protocol cohort evaluation, the overall RT-MTB sensitivity on decontaminated samples was higher than Xpert. Our findings are in concordance with the study performed by Scott et al. 201722. Although they obtained higher sensitivity values for Xpert when testing concentrated samples, RT-MTB identified a substantially higher number of MTBC cases among smear negative patients (74.4% versus 25.7%). Similar trends were seen in our study, although there was limited statistical power to detect differences when using the composite reference standard (48% versus 29% p value = 0.05). Analysis of the intention-to-treat cohort did not improve on test parameters, however, RT-MTB showed better sensitivity than Xpert. These results are in line with several studies showing that molecular case-detection diminishes among smear negative patients5,33.
On the other hand, Xpert achieved markedly increased specificity and higher PPVs in all analyses. RT-MTB specificity and PPVs values remained lower and constant throughout. Additionally, using the CRS, the specificity of Xpert reached 100% among smear negatives although this could be biased (incorporation bias) by the fact that clinicians were not blinded to Xpert results. In order to get a better understanding of the lower specificity of RT-MTB and if it would be translated into false-positive test results, we evaluated the 22 discordant results among RT-MTB and culture. Six of these cultures were positive for NTM. Cross-reactivity has not been reported previously in similar studies19,24, although NTM cultures are often excluded from the analyses or considered as contamination, biasing the study findings17. Conversely, in vitro evaluation of RT-MTB showed 97% specificity due to cross-reactivity with two samples containing NTM, although Cn values were close to the established cut-off (Cn = 40)14. Importantly, our setting is associated with high NTM isolation in pediatric patients investigated for TB34. Our results could therefore indicate some degree of cross-reactivity with NTM. Of the remaining 16 discordant samples, 2 were collected from previous TB patients, 2 were from patients that had been treated recently, 4 were from patients that died after the follow-up period and no other relevant information was found on the remaining 8 discrepant cases. When RT-MTB Cns were compared, the Cn mean among those potential false-positives approached the cutoff of 40 established by the manufacturer. This could support the hypothesis of the detection of either low amounts of DNA in recently treated patients, or real false-positive results. Highly sensitive molecular tests deal with the identification of non-viable DNA35 or the detection of cross-contamination during test performance. In a recent meta-analysis to evaluate the laboratory cross-contamination of Mycobacterium tuberculosis, 2% of all positive results were found to be false-positives for this reason36. Our investigation did not suggest that intra-instrument carry-over was the cause of false positivity. Furthermore, our TB laboratory strictly follows Good Clinical and Laboratory Practice standards (GCLP); thus, cross-contamination of specimens due to material transfer during pre-analytic sample handling appears unlikely.
Since the evaluation of the molecular test performance relies on comparing results to a hypothetical error-free test, using culture as a gold standard brings limitations and possible detection bias37,38. Liquid and solid cultures have difficulties in identifying paucibacillary specimens, common in children and HIV patients. Whether positive molecular tests from culture negative samples are false-positives or misclassified real negatives are difficult to disentangle22. Therefore, we combined treatment initiation and positive cultures to better evaluate the accuracy of the molecular tests used in this study. The use of composite reference standards has been extensively used not only for tuberculosis39,40,41, but also for other infectious diseases when diagnosis accuracy evaluation might be compromised by weak reference standards38. Results on this approach led to improved specificity but lower sensitivity. Microbiological verification of TB cases is still challenging in the diagnostic workup and last year only 56% of cases were bacteriologically confirmed, therefore almost half of tuberculosis patients started treatment based on clinical observation1.
Lastly, on the importance of strengthening laboratory diagnosis in all dimension, the theoretical advantages of centralized platforms with greater capacity for testing might be translated into real improvements under operational conditions42. Although the Xpert´s PCR is performed in less than 2 hours12, just one cartridge can be tested per module, whereas up to 96 tests can be run simultaneously in the m2000sp platform. Nevertheless, these high-capacity devices, often result in longer turnaround time due to sample preparation and testing, thereby making them inferior in terms of throughput. In addition, they need suitable infrastructure, qualified personnel for the instrument´s set up and the capacity to perform adequate maintenance and handle any technical issues that may arise. The operational challenges (S3) we experienced with the m2000sp platform, raise awareness on the importance of strengthening diagnosis capacity, not only with regard to more accurate techniques but also on appropriate laboratory infrastructure, resources and trained personnel7.
Our study had further limitations. Firstly, we only tested the best quality specimen for liquid and solid culture because of budget concerns. Secondly, we could not assess the diagnostic accuracy of drug susceptibility testing due to a lack of phenotypic resistance strains. One of the advantages of the Abbott assay is its ability to identify rifampicin and isoniazid resistance mutations in the same DNA sample prepared to identify the presence of MTBC. However, we gained information on drug resistance in just 18 specimens with RT-MTB RIF/INH Resistance assay. Twenty-one samples were below the LoD, which is likely due to the lower LoD of the assay (17 CFU/mL) compared to that of the Resistance assay (60 CFU/mL). For the remaining samples, the system reported other test errors. Additionally, a number of technical issues were encountered related to the m2000sp instrument, leading to repeats and delaying the study. Lastly, the percentage of lost-to-follow-up was higher than expected and we could not characterize false-positive samples any further through other highly sensitive molecular assays or techniques, such as sequencing, in order to assess the true specificity of RT-MTB assay.
Conclusion
In this study, conducted among PLHIV in southern Mozambique, our results suggest better sensitivity and confirm lower specificity for the Abbott RT-MTB assay compared to the Xpert MTB/RIF. The RT-MTB assay may detect cases that may not otherwise be detected by culture, although this added yield might also be associated with some degree of cross-reactivity with NTMs, detection of non-viable mycobacteria (previously treated patients) or cross-contamination.
The considerable number of “false-positive” results calls for a profound case evaluation on an individual basis, involving trained personnel for the interpretation of molecular results and careful specimen handling to minimize the risk of potential cross-contaminations.
Data availability
The datasets generated during the current study are kept at the data center of CISM. An anonymized version of the dataset can be made available upon request to CISM’s Internal Scientific Committee (Email: cci@manhica.net).
References
World Health Organisation. Global Tuberculosis Report 2020. (2020). https://apps.who.int/iris/bitstream/handle/10665/336069/9789240013131-eng.pdf
Pan American Health Organization. Tuberculosis in the Americas 2018. (2018). https://iris.paho.org/handle/10665.2/49510
World Health Organization. The END TB Strategy, 2016–2035. https://www.who.int/tb/End_TB_brochure.pdf?ua=1
World Health Organization. Framework of indicators and targets for laboratory strengthening under The End TB Strategy. (2016). http://apps.who.int/iris/bitstream/handle/10665/250307/9789241511438-eng.pdf?sequence=1
World Health Organizaton. Automated Real-Time Nucleic Acid Amplification Technology for Rapid and Simultaneous Detection of Tuberculosis and Rifampicin Resistance: Xpert MTB/RIF Assay for the Diagnosis of Pulmonary and Extrapulmonary TB in Adults and Children: Policy update. https://apps.who.int/iris/handle/10665/112472
World Health Organization. World Health Organization Model List of Essential In Vitro Diagnostics. (2018). https://www.who.int/medical_devices/diagnostics/WHO_EDL_2018.pdf
World Health Organization. Regional Office for Europe. Algorithm for laboratory diagnosis and treatment-monitoring of pulmonary tuberculosis and drug-resistant tuberculosis using state-of-the-art rapid molecular diagnostic technologies. (2017). https://www.euro.who.int/en/publications/abstracts/algorithm-for-laboratory-diagnosis-and-treatment-monitoring-of-pulmonary-tuberculosis-and-drug-resistant-tuberculosis-using-state-of-the-art-rapid-molecular-diagnostic-technologies-2017
World Health Organization. Unitaid Tuberculosis Diagnostics Technology Landscape 5th Edition. https://unitaid.org/assets/2017-Unitaid-TB-Diagnostics-Technology-Landscape.pdf
World Health Organizaton. Rapid Communication: Molecular assays as initial tests for the diagnosis of tuberculosis and rifampicin resistance. (2020). https://www.who.int/tb/publications/2020/rapid-communications-molecular-assays/en/
Beynon, F. et al. Correlation of Xpert MTB/RIF with measures to assess mycobacterium tuberculosis bacillary burden in high HIV burden areas of Southern Africa. Sci. Rep. 8, 5201 (2018).
Maynard-Smith, L., Larke, N., Peters, J. A. & Lawn, S. D. Diagnostic accuracy of the Xpert MTB/RIF assay for extrapulmonary and pulmonary tuberculosis when testing non-respiratory samples: a systematic review. BMC Infect. Dis. 14, 709 (2014).
GeneXpert Systems Brochure. https://p.widencdn.net/bia0nv/Cepheid-GeneXpert-System-Brochure-CE-IVD-0309-English.
World Health Organization. Evaluation of centralized assays for TB detection and detection of resistance to rifampicin and isoniazid. WHO Technical Expert Consultation Report. (2019). https://apps.who.int/iris/handle/10665/329388
Tang, N. et al. Analytical and clinical performance of Abbott RealTime MTB, an assay for detection of Mycobacterium tuberculosis in pulmonary specimens. Tuberculosis 95, 613–619 (2015).
Kostera, J., Leckie, G., Abravaya, K. & Wang, H. Molecular, A. Performance of the Abbott RealTime MTB RIF/INH resistance assay when used to test Mycobacterium tuberculosis specimens from Bangladesh. Infect. Drug Resist. 11, 695–699 (2018).
Harrington, A. et al. Comparison of Abbott ID Now and Abbott m2000 methods for the detection of SARS-CoV-24 from nasopharyngeal and nasal swabs from symptomatic patients. J. Clin. Microbiol. 58(8), e00798-20 (2020).
Berhanu, R. H. et al. Performance of Xpert MTB/RIF, xpert ultra, and Abbott RealTime MTB for diagnosis of pulmonary tuberculosis in a high-HIV-burden setting. J. Clin. Microbiol. 56, e00560-e618 (2018).
Vinuesa, V., Navarro, D., Poujois, S., Zaragoza, S. & Borrás, R. Performance characteristics of the new Abbott Real Time MTB assay for detection of mycobacterium tuberculosis complex in respiratory specimens. Diagn. Microbiol. Infect. Dis. 84, 212–214 (2016).
Tam, K. K. et al. Direct detection of mycobacterium tuberculosis and drug resistance in respiratory specimen using Abbott Realtime MTB detection and RIF/INH resistance assay. Diagn. Microbiol. Infect. Dis. 89, 118–124 (2017).
Hinic, V. et al. Clinical evaluation of the Abbott RealTime MTB assay for direct detection of mycobacterium tuberculosis-complex from respiratory and non-respiratory samples. Tuberculosis 104, 65–69 (2017).
Hofmann-thiel, S., Molodtsov, N. & Antonenka, U. Evaluation of the Abbott RealTi m e MTB and RealTi m e MTB INH/RIF assays for direct detection of mycobacterium tuberculosis complex and resistance markers in respiratory and extrapulmonary specimens. J. Clin. Microbiol. 54, 3022–3027 (2016).
Scott, L. et al. Performance of the abbott realtime MTB and MTB RIF/INH assays in a setting of high tuberculosis and HIV coinfection in South Africa. J. Clin. Microbiol. 55, 2491–2501 (2017).
Wang, S. F. et al. The Abbott RealTime MTB assay and the Cepheid GeneXpert assay show comparable performance for the detection of mycobacterium tuberculosis in sputum specimens. Int. J. Infect. Dis. 45, 78–80 (2016).
Chen, J. H. et al. Performance of the new automated Abbott RealTime MTB assay for rapid detection of mycobacterium tuberculosis complex in respiratory specimens. Eur. J. Clin. Microbiol. Infect. Dis. 34(9), 1827–1832 (2015).
Garcia-Basteiro, A. L. et al. Unmasking the hidden tuberculosis mortality burden in a large post mortem study in Maputo Central Hospital, Mozambique. Eur. Respir. J. 54(3), 1900312 (2019)
García-Basteiro, A. L. et al. High tuberculosis burden among people living with HIV in southern Mozambique. Eur. Respir. J. 45, 547–549 (2015).
Nhacolo A. et al. Cohort profile update: Manhiça health and demographic surveillance system (HDSS) of the Manhiça health research centre (CISM). Int J Epidemiol. 2021 Jan 16:dyaa218.
González, R. et al. HIV incidence and spatial clustering in a rural area of Southern Mozambique. PLoS ONE 10, e0132053 (2015).
García-Basteiro, A. et al. Tuberculosis on the rise in southern Mozambique (1997–2012). Eur. Respir. J. 49, 1601683 (2017).
World Health Organizaton. Systematic screening for active tuberculosis. Principles and recommendations. http://apps.who.int/iris/bitstream/10665/84971/1/9789241548601_eng.pdf?ua=1&ua=1 (2013).
European Center for Diseases Prevention and Control. Handbook on tuberculosis laboratory diagnostic methods in the European Union. https://www.ecdc.europa.eu/sites/default/files/documents/TB-handbook-2018-final.pdf (2018) https://doi.org/10.2900/914169.
Kostera, J. et al. Analytical and clinical performance characteristics of the Abbott RealTime MTB RIF/INH resistance, an assay for the detection of rifampicin and isoniazid resistant Mycobacterium tuberculosis in pulmonary specimens. Tuberculosis 101, 137–143 (2016).
Kendall, E. A. et al. Empiric treatment of pulmonary TB in the Xpert era: Correspondence of sputum culture, Xpert MTB/RIF, and clinical diagnoses. PLoS ONE 14, 2e0220251 (2019).
López-Varela, E. et al. High rates of non-tuberculous mycobacteria isolation in Mozambican children with presumptive tuberculosis. PLoS ONE 12, e0169757 (2016).
World Health Organization. WHO Meeting Report of a Technical Expert Consultation: Non-inferiority analysis of Xpert MTB/RIF Ultra compared to Xpert MTB/RIF. https://apps.who.int/iris/handle/10665/254792.
Barac, A. et al. Laboratory cross-contamination of mycobacterium tuberculosis: a systematic review and meta-analysis. Lung 197, 651–661 (2019).
Saavedra, B. et al. Performance of Xpert MTB/RIF Ultra for tuberculosis diagnosis in the context of passive and active case finding. Eur. Respir. J. 58, 13993003 (2021).
Canchola, J. A., Tang, S., Hemyari, P. & Canchola, J. A. Composite reference standard in diagnostic research : a new approach to reduce bias in the presence of imperfect reference tests composite reference standard in diagnostic research : a new approach to reduce bias in the presence of imperfect reference test. Biometrics Rev. https://doi.org/10.13140/RG.2.1.2046.9844 (2015).
García-Basteiro, A. L. et al. The role of Xpert MTB/RIF in diagnosing pulmonary tuberculosis in post-mortem tissues. Sci. Rep. 6, 20703 (2016).
WHO/FIND. A multicentre non-inferiority diagnostic accuracy study of the Ultra assay compared to the Xpert MTB/RIF assay. https://www.finddx.org/wp-content/uploads/2019/12/Multicentre-noninferiority-study-Ultra-Xpert-FEB2017-FINAL.pdf
Vadwai, V. et al. Xpert MTB/RIF: a new pillar in diagnosis of extrapulmonary tuberculosis?. J. Clin. Microbiol. 49, 2540–2545 (2011).
World Health Organization. Considerations for adoption and use of multidisease testing devices in integrated laboratory networks. (2017). https://www.who.int/tb/publications/2017/considerations_multidisease_testing_devices_2017/en/
Acknowledgements
We want to thank all participants and their families for participating in the research project. We want to thank all the support received by the National TB Control Programme from Mozambique and Rifat Munir (NHLS, Johannesburg) for her comments to the manuscript. We acknowledge support from the Spanish Ministry of Science, Innovation and Universities through the “Centro de Excelencia Severo Ochoa 2019–2023” Program (CEX2018-000806-S), and support from the Generalitat de Catalunya through the CERCA Program.
Funding
B.S receives a pre-doctoral fellowship from the Secretariat of Universities and Research, Ministry of Enterprise and Knowledge of the Government of Catalonia and co-funded by European Social Fund (AGAUR). This research was supported by a grant from Abbott GmbH. Abbott GmbH was not involved in the data analysis or decision to submit this manuscript for publication.
Author information
Authors and Affiliations
Contributions
Study design (A.G.B. and L.S.); Enrolment and clinical work (L.F.); Study implementation (A.G.B., B.S.C., D.N. and E.M.); Laboratory work (B.S.C., E.M., R.M., F.M., A.C., N.G. and S.M.); Data analyses (B.S.C. and A.G.B.); Manuscript write-up (B.S.C.). All authors provided input for the final version of the manuscript and approved it as sent to the journal.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Saavedra, B., Mambuque, E., Gomes, N. et al. Diagnostic performance of the Abbott RealTime MTB assay for tuberculosis diagnosis in people living with HIV. Sci Rep 11, 19271 (2021). https://doi.org/10.1038/s41598-021-96922-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-96922-3
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
