
Abstract
Stroke is a significant cause of death and disability. In Thailand, it imposes a major health burden, and the prevalence of stroke is increasing, particularly in patients with hypertension (HT), diabetes mellitus (DM), and dyslipidemia (DLP). We aimed to determine the trends in the prevalence of stroke and the associated factors among Thai patients with HT. Nationwide cross-sectional studies were conducted annually in 2014, 2015 and 2018 based on data obtained from the Thailand DM/HT study. Nationally, representative patients with HT in Thailand were sampled with stratified one-stage cluster sampling. A total of 104,028 participants were included in this study. The prevalence of stroke remained constant, with prevalence rates of 4.0%, 3.8%, and 3.9% in 2014, 2015 and 2018, respectively (p for trend = 0.221). Our findings suggested that the management of stroke patients who are covered by the universal coverage scheme should be evaluated. Effective interventions, including promoting smoking cessation, attenuating cholesterol levels, and controlling blood pressure should be provided to hypertensive patients to prevent ischemic stroke. Young adults with HT should be more concerned about the possibility of stroke. The use of prophylactic low-dose aspirin should be carefully monitored to prevent hemorrhagic stroke.
Similar content being viewed by others


Introduction
Worldwide, stroke is one of the leading causes of death and long-term disability1. Based on data from the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 20172, the age-standardized incidence of patients with stroke declined by 11% (from 0.17 to 0.15%) worldwide from 1990 to 20173. This decline may have resulted from more aggressive control of the risk factors through the adoption of preventive measures. Similarly, the global age-standardized stroke mortality rate decreased by 33.4% (from 0.12 to 0.08%), and the disability-adjusted life years lost decreased by 31% (from 2.39 to 1.66%) from 1990 to 2017. In contrast, the global age-standardized prevalence of stroke has increased by 3.1% (from 1.26 to 1.30%). However, from 1990 to 2017, the prevalence increased only in upper-middle-income countries, with an average growth rate of 11% (from 1.40 to 1.55%), whereas it decreased by 3% (from 1.03 to 1.00%) and 8% (from 1.26 to 1.16%) in low- and high-income countries, respectively, and remained unchanged (1.08%) in lower-middle-income countries.
Thailand is an upper-middle-income country located in Southeast Asia. Over the past few decades, Thailand has gradually transformed from an agricultural to an industrialized nation. The economic and health transitions in addition to urbanization have modified many aspects of the lifestyles of the Thai people, including the introduction of unhealthy diets and reductions in the level of physical activity4,5. As a consequence, the prevalence of metabolic syndrome and cardiovascular diseases, including stroke, has increased. Stroke has become a major health burden and the leading cause of death in Thailand, with a higher prevalence in males5. The mean age of patients at the onset of ischemic stroke is approximately 65 years6. From 1994 to 1996, the prevalence of stroke in Thailand was 1.12%, with the highest prevalence found in the central region7. A study conducted over the period from 2004 to 2006 demonstrated that the prevalence of stroke was approximately 1.88% among Thai individuals aged 45 years and older5,8. In 2014, it was reported that the prevalence of stroke in Thailand was 1.3%9.
Many risk factors for stroke are modifiable. Among these, hypertension (HT) is an important risk factor for stroke10,11,12,13. Other risk factors include diabetes mellitus (DM), dyslipidemia (DLP), and overweight10,14. Lifestyle modifications, including smoking cessation, physical activity participation, healthy diet consumption and body weight control, can reduce mortality from stroke15. However, information on the distribution of the prevalence of stroke according to geographic region, hospital level, or health coverage scheme in Thailand is limited. In this study, we aimed to determine the prevalence of stroke in Thai patients with HT visiting the Ministry of Public Health and Bangkok Metropolitan Administration Hospitals from 2014 to 2018 based on information from the Thailand Diabetes Mellitus/Hypertension (DM/HT) database and identify the associated factors. The outcomes of this study potentially support the development of preventive strategies and promote the capacity of healthcare professionals to counsel patients with stroke in Thailand.
Methods
Study designs and subjects
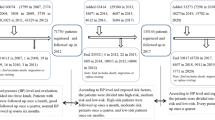
Cross-sectional surveys were conducted once per year in 2014, 2015 and 2018. After receiving permission from the National Health Security Office (NHSO) and Medical Research Network of the Consortium of Thai Medical School (MedResNet), the database “An Assessment on Quality of Care among Patients Diagnosed with Type 2 Diabetes and Hypertension Visiting the Ministry of Public Health and Bangkok Metropolitan Administration Hospitals in Thailand” (Thailand DM/HT) was accessed, and the relevant data were retrieved16. Patients visiting subdistrict (health-promoting), district (community), provincial (general) and regional hospitals nationwide were included in the Thailand DM/HT study, with the aim of encompassing all hospital levels under the Ministry of Public Health. Among the 1,098 hospitals, a total of 28 regional hospitals, 80 general hospitals, 883 community hospitals and 107 health-promoting hospitals participated. In this study, the inclusion criteria were HT, age of 18 years or older, and medical treatment in the abovementioned hospitals during the previous 12 months. Patients who had participated in a clinical trial were excluded. Nationally and provincially, representatives of patients with HT in Thailand were sampled proportional to the population size with a stratified one-stage cluster sampling method.
Data collection
At each clinic, health care personnel invited patients with a pre-existing diagnosis of HT to participate in the study. The patients were asked to sign a consent form to allow the investigators to review and abstract their medical records. A standardized case report form (CRF) was used for medical record abstractions. The CRF was completed by a well-trained registered nurse using a standard protocol and was sent to the MedResNet central data management unit in Nonthaburi, Thailand. To transfer the CRF to the electronic dataset, an automated scan-to-database software solution was used to extract data and convert them to database records16. The collected data comprised demographics, weight, height, body mass index (BMI), smoking status, systolic blood pressure (SBP), diastolic blood pressure (DBP), stroke history, stroke subtypes, stroke comorbidities, including DLP, DM, gout, renal insufficiency, atrial fibrillation (AF), and history of low-dose aspirin use. In this study, the database from the Thailand DM/HT study was used for analysis. Based on secondary data, stroke was determined according to the International Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10) codes17 I60-I64 for overall stroke, I63 for ischemic stroke, and I60-I62 for hemorrhagic stroke recorded by clinicians. Similarly, stroke comorbidities were determined according to the ICD-10 codes17 E78 for DLP, E11 for DM, M10 for gout, N18-N19 for renal insufficiency, and I48 for AF. Current smokers were defined as those who had smoked within the previous 12 months. Nonsmokers were patients who had never smoked or had smoked fewer than 100 cigarettes18 in their lifetime. Ex-smokers were defined as those who had smoked at least 100 cigarettes in their lifetime but had quit smoking for at least 12 months. BMI was calculated as the body weight in kilograms divided by the height in meters squared [weight (kg)/height (m)2].
Statistical analysis
The data were analyzed using Stata Statistical Software: Release 17 (StataCorp LLC., College Station, TX, USA). Demographic characteristics were analyzed with descriptive statistics. The outcomes are presented as numbers and percentages for categorical data and as the means and standard deviations (SDs) for continuous data. The prevalence of stroke was assessed using descriptive statistics and is reported as the percentage with the associated 95% confidence interval (95% CI). The p for trend was calculated using the chi-square test for trend. The chi-square test and Student’s t-test were used to compare categorical and continuous variables, respectively. Univariate and multivariate logistic regression analyses were performed to determine the associated factors for stroke. Sex, age, geographic region, hospital level, healthcare coverage scheme, smoking, DM, DLP, renal insufficiency, AF, BMI, and uncontrolled HT were included in the multivariate logistic regression analyses of the factors associated with ischemic stroke. Sex, age, geographic region, hospital level, healthcare coverage scheme, smoking, DLP, renal insufficiency, BMI, and the use of prophylactic low-dose aspirin were adjusted in the final model to determine the factors associated with hemorrhagic stroke. The magnitudes of the associations obtained from univariate and multivariate analyses are represented as crude odds ratios (ORs) and adjusted odds ratios (AORs), respectively, with the corresponding 95% CIs. The level of statistical significance was set at p < 0.05.
Ethical considerations
The Thailand DM/HT study was approved by the Thai National Health Security Office Institutional Review Board. This study was reviewed and approved by the Institutional Review Board, Royal Thai Army Medical Department (approval number S086h/63). This study was conducted in accordance with the principles of the Declaration of Helsinki. Informed consent was obtained from all individual participants included in the study.
Results
Demographic characteristics
A total of 104,028 Thai patients with HT were included in the study, with 33,227 (31.9%) in 2014, 32,440 (31.2%) in 2015 and 38,361 (36.9%) in 2018. Females accounted for 62.1% of all participants. The average ages of the participants were 63.8 ± 11.7, 63.9 ± 11.8 and 64.6 ± 11.8 years, and the average durations of HT since diagnosis were 6.4 ± 4.0, 6.7 ± 4.2 and 6.8 ± 4.5 years in 2014, 2015, and 2018, respectively. The majority of participants were patients visiting community hospitals (72.6%). Most of the patients were covered under the universal coverage scheme (74.2%). The demographic characteristics of the study participants by year are presented in Table 1.
Trends in the prevalence of stroke among Thai patients with hypertension
Table 2 illustrates the trends in the prevalence of stroke by sex, age group, and geographic region. From 2014 to 2018, the overall prevalence of stroke among Thai patients with HT remained unchanged. The prevalences were 4.0%, 3.8%, and 3.9% for overall stroke (p for trend = 0.221); 3.6%, 3.4%, and 3.5% for ischemic stroke (p for trend = 0.517); and 0.5%, 0.4% and 0.4% for hemorrhagic stroke (p for trend = 0.033) in 2014, 2015, and 2018, respectively. Overall, although the prevalence of stroke remained constant over the 5 years in both males (p for trend = 0.15) and females (p for trend = 0.686), the prevalence was higher in males. From 2014 to 2018, the prevalence of overall stroke was approximately 5.6% to 6.0% in males, while it was approximately 2.7% to 2.8% in females. Strikingly, a significant increasing trend in the prevalence of overall stroke was found in patients under the age of 40 years, with prevalence rates of 0.9%, 1.3%, and 2.6% (p for trend = 0.02) in 2014, 2015, and 2018, respectively. In contrast, in patients aged between 50 and 59 years, the prevalence of overall stroke significantly decreased from 3.5% in 2014 to 3.4% in 2015 and further decreased to 2.8% in 2018 (p for trend = 0.007). This pattern was also seen in ischemic stroke. With regard to the geographic distribution of the prevalence of stroke, the prevalence of overall stroke significantly increased from 3.0% in 2014 to 3.6% in 2018 (p for trend < 0.005) in patients living in the northeastern part of Thailand. In contrast, among patients residing in the central part of Thailand, the prevalence of overall stroke significantly declined from 4.4% in 2014 to 3.7% in 2018 (p for trend = 0.005). Again, it was observed that this pattern only existed in ischemic stroke. The prevalence of hemorrhagic stroke significantly decreased from 0.7% in 2014 to 0.4% in 2018 (p for trend = 0.001) among patients living in the northern part of Thailand.
Associated factors of stroke among Thai patients with hypertension
Univariate and multivariate regression analyses were performed to identify the independent factors for ischemic stroke and hemorrhagic stroke among Thai patients with HT from 2014 to 2018. After adjusting for potential confounders, factors associated with ischemic stroke were male sex, older age, geographic region, hospital level, healthcare coverage schemes, smoking, comorbid DLP, AF, low BMI, and uncontrolled HT (Table 3). For hemorrhagic stroke, the independent associated factors were male sex, younger age, geographic region, hospital level, healthcare coverage schemes, low BMI, and the use of prophylactic low-dose aspirin (Table 4).
Discussion
To the best of our knowledge, this is the first and largest epidemiological study in Southeast Asia to focus on stroke and its associated factors among Thai patients with HT. These results revealed the constant trends in the prevalence of stroke among Thai patients with HT from 2014 to 2018. The prevalence of overall stroke in this population ranged from 3.8 to 4.0% (Table 2). Unsurprisingly, the prevalence of ischemic stroke was higher than that of hemorrhagic stroke. In patients with HT, the prevalence of stroke was 5.1% in Madrid, Spain19, and 11.6% in Southern Piauí, Brazil20. In Thailand, the prevalence of overall stroke in patients with HT was relatively low. This may be the result of improvements in the stroke management system. Indeed, in Thailand, a stroke fast track system was initiated and has been improved over the past two decades21. As a consequence, more acute stroke patients are treated within the golden period.
Previously, the central part of Thailand was reported to have the highest prevalence of stroke, followed by the southern, northern, and northeastern regions; the northeastern region has been reported to have the lowest prevalence of stroke in Thailand8. In this study, however, the geographic distribution of the prevalence of stroke in patients with HT was slightly different. We found that ischemic stroke was most prevalent in the southern part of Thailand, whereas the northeastern region still had the lowest stroke prevalence (Table 2). However, there was a significant increasing trend in the prevalence of ischemic stroke in patients with HT residing in the northeastern part of Thailand from 2014 to 2018. With regard to hemorrhagic stroke, the prevalence was also lowest in the northeastern region (Table 2), and the risk of stroke nearly doubled in patients with HT residing in other regions of the country (Table 4). The most plausible explanation of the lowest prevalence of both ischemic and hemorrhagic strokes being found in the northeastern part of Thailand is that agriculture is the main occupation of people residing in this area with a lower rate of industrialization. Their lifestyles are still conservative; for example, healthy diets consisting of mainly rice and vegetables and regular physical activity related to their occupation may lower the risk of stroke. However, further investigation is required to identify the associated factors contributing to a significant increasing trend in the prevalence of ischemic stroke in this area and the change from the central to the southern region where the highest prevalence of ischemic stroke was observed.
Interestingly, in Thai patients with HT, we found that the prevalence of both ischemic (Table 3) and hemorrhagic strokes (Table 4) was higher in patients who were admitted to regional and provincial hospitals than in those admitted to community hospitals. This can be explained by the fact that stroke patients are likely to be referred to tertiary care centers. Specialists and essential medical facilities are not available in health-promoting and community hospitals; as a result, patients with stroke in such hospitals may have limited access to neurologists. At present, Thailand has fewer than 400 active neurologists. More than two-thirds of this specialized group lives in Bangkok and the surrounding provinces5. The concentration of neurologists in Bangkok results in a shortage of neurologists across the country, particularly in rural areas. In addition, we found that the highest prevalence of both ischemic (Table 3) and hemorrhagic strokes (Table 4) was observed in hypertensive patients who were under the universal health coverage scheme, which is the major healthcare coverage scheme in Thailand. The most plausible explanation is that there are imbalances between the demand and supply of treatment for stroke that affect the management system within the universal health coverage scheme. The need for longitudinal studies on the outcomes of stroke at different hospital levels and the impact of universal health coverage schemes on the outcome of stroke is suggested. Collectively, these findings indicated that stroke should be a focus in regional and provincial hospitals and that opportunities to prevent stroke should be considered by providing more intensive preventive strategies to hypertensive patients, especially those who are under the universal health coverage scheme.
The present study revealed that male sex was a risk factor for both ischemic (Table 3) and hemorrhagic strokes (Table 4) in Thai patients with HT. These results were consistent with previous studies performed in southwestern China10 and in Thailand, particularly in patients older than 35 years old22. An analysis of 471,971 participants from the UK Biobank cohort study demonstrated that the incidence of stroke was higher among males23. However, this remains controversial, as opposite results have been reported. In the USA, the incidence and prevalence of stroke were higher in females24,25. It was reported that estrogen was a protective factor against the development of ischemic stroke26. Therefore, the higher prevalence of stroke in males may be related to a lower level of female hormones. However, menopausal and postmenopausal females may lose this protective effect, which results in an increased susceptibility to ischemic brain changes26.
Although stroke can occur at any age, it is mainly a disease of the elderly population. We found that the risk of ischemic stroke increased with increasing age group among Thai patients with HT in a dose–response relationship (Table 3). The average age of patients at the onset of ischemic stroke in Thailand, according to the Thai Stroke Registry, is approximately 65 years6. This age is consistent with the average age of onset of ischemic stroke reported in other developing countries27,28,29. Nevertheless, from 2014 to 2018, the prevalence of overall and ischemic strokes continuously increased in patients with HT who were younger than 40 years (Table 2). In addition, the present study also found an inverse dose–response relationship between age and the risk of hemorrhagic stroke (Table 4). These results indicated that young Thai people with HT should be more concerned about the possibility of stroke. Interestingly, in Western countries, the proportion of patients with hemorrhagic stroke is dramatically higher in the young adult subpopulation: 15–20% of the general stroke population has hemorrhagic stroke, while 40–55% of young adult diagnosed with stroke has hemorrhagic stroke30,31,32,33. In a large American study, fivefold and 2.33-fold increased risks of hemorrhagic stroke were observed in young adults who abused amphetamine and cocaine, respectively34. Mechanistically, amphetamine can induce cerebral vasculitis35,36, whereas cocaine is involved in hypertensive surges following its administration37,38. However, it was revealed that, rather than the direct effects of the drugs, the higher risk of hemorrhagic stroke in those young adults was potentially associated with underlying vascular malformations39. The proportion of patients with hemorrhagic stroke has not been well investigated among young Asians.
The present study demonstrated inverse dose–response relationships between BMI and the risk of both ischemic (Table 3) and hemorrhagic strokes (Table 4) in Thai patients with HT, with a higher risk of stroke in hypertensive patients who had lower BMI values. These results were consistent with those of a previous study conducted in 67,086 American patients with DM40. More clinical and molecular insights are, however, still needed to explain these findings.
Heavy metals and other toxins in tobacco smoke promote vascular endothelial dysfunction and inflammation, ultimately resulting in atherosclerosis41. In addition, smoking also promotes a global procoagulant state42 which results in a decrease in cerebral blood flow43, leading to blood clot formation and ischemic stroke development. While the relationship between intracerebral hemorrhage and smoking is weak and inconsistent, an increased risk of subarachnoid hemorrhage tends to be associated with the increased incidence of aneurysms seen in smokers41. A strong association between smoking and stroke risk has been reported, with current smokers having at least a two- to fourfold higher risk of stroke than nonsmokers or ex-smokers who quit smoking more than 10 years prior41. A number of studies have indicated that ex-smokers have a lower risk of stroke than current smokers43,44,45,46 and may have the same risk as nonsmokers47,48. Nonetheless, we found that both current smokers and ex-smokers with HT had an elevated risk of ischemic (Table 3) but not hemorrhagic (Table 4) stroke. Therefore, for the greatest benefit, smoking cessation should be listed in preventive rather than therapeutic strategies for stroke. Physiologically, smoking cessation can lead to a reversal of the procoagulant state to baseline. However, the full return to the risk status of a nonsmoker depends on various factors, including the level of atherosclerosis developed during smoking, the duration of smoking, and the duration since smoking cessation41. Unfortunately, this information was not available in our database.
HT is the most common and well-established risk factor for both ischemic and hemorrhagic strokes. In ischemic stroke, HT places a strain on the blood vessels and predisposes them to damage, which ultimately causes atherosclerosis49. HT is implicated in hemorrhagic stroke when a weakened blood vessel in the brain bursts and blood leaks into the brain. In our study, uncontrolled HT was identified as a factor associated with ischemic stroke in Thai patients with HT (Table 3). Therefore, controlling blood pressure is a critical management strategy that can reduce the risk of ischemic stroke in hypertensive patients. Unexpectedly, we found that uncontrolled HT was no longer associated with hemorrhagic stroke (Table 4). This result was supported by a previous study reporting that there was no association between the use of antihypertensive drugs and the outcome of cerebral small vessel disease50. However, these findings were only described in minority reports. The pooling of data from one hundred forty-seven randomized clinical trials demonstrated that 10 mmHg systolic and 5 mmHg diastolic reduction of blood pressure was associated with an average 41% reduction in stroke in all trials51. In fact, in a systemic review, all eleven case–control studies showed a positive correlation between HT and intracerebral hemorrhage, with an overall OR of 3.68 (95% CI, 2.52 to 5.38)52. The incidence of HT increases with age; hence, HT is a more common risk factor for intracerebral hemorrhage in older people. The stronger association between younger age groups of hypertensive patients and hemorrhagic stroke in this study potentially explains the lack of a correlation between HT and hemorrhagic stroke.
DLP is known to be a risk factor for atherosclerosis-related ischemic stroke. Our study revealed an association between comorbid DLP and the risk of ischemic stroke in Thai patients with HT (Table 3), indicating that lipid profiles should be regularly tested. However, a relationship between DLP and hemorrhagic stroke was not observed (Table 4). It has been reported that attenuating cholesterol levels can reduce the risk of stroke. Regarding statins versus placebo and more versus less statin therapy, the pooled results of twenty-six clinical trials demonstrated that there was a reduction in ischemic stroke with an overall relative risk (RR) of 0.79 (95% CI, 0.74 to 0.85), whereas there was a nonsignificant increase in hemorrhagic stroke with an overall RR of 1.12 (95% CI, 0.93 to 1.35) per 1 mmol/L reduction in low-density lipoprotein cholesterol (LDL-C)53. Gemfibrozil reduces serum triglycerides and raises high-density lipoprotein cholesterol (HDL-C). In the Veterans Affairs High-Density Lipoprotein Cholesterol Intervention Trial (VA-HIT) conducted in 2,531 men with coronary heart disease, it was reported that gemfibrozil reduced strokes by 31% (95% CI, 2% to 52%), and there were five and six hemorrhagic strokes in the placebo and gemfibrozil arms, respectively54.
In AF, the chaotic rhythm may cause blood to pool in the upper chambers of the heart and form clots that can dislodge and block blood flow to other organs, including the brain. The present study identified that AF was a strong associated factor for ischemic stroke in Thai patients with HT (Table 3). This result was consistent with previous studies55,56,57,58. However, it remains unclear whether occult AF is related to stroke. According to the Prevalence of Sub-Clinical Atrial Fibrillation Using an Implantable Cardiac Monitor in Patient With Cardiovascular Risk Factors (ASSERT-II) study, the rate of occurrence of subclinical AF in those with or without a history of stroke, systemic embolism, or transient ischemic attack was not significantly different59. With regard to stroke prevention, ongoing clinical trials are evaluating appropriateness and the risks and benefits of screening for occult AF and the use of anticoagulants in occult AF patients, including the Systematic ECG Screening for Atrial Fibrillation Among 75 Year Old Subjects in the Region of Stockholm and Halland, Sweden (STROKESTOP) trial (NCT01593553) and the Apixaban for the Reduction of Thromboembolism in Patients With Device-Detected Sub-Clinical Atrial Fibrillation (ARTESiA) trial (NCT01938248).
Given its cost-effectiveness and widespread availability, low-dose aspirin is a key therapeutic option for the secondary prevention of myocardial infarction and ischemic stroke60. Aspirin at a dose of 81 mg was the main prophylactic antiplatelet medication prescribed to the patients in our study. We found that low-dose aspirin use was a risk factor for hemorrhagic stroke in patients with HT (Table 4). Therefore, patients taking prophylactic low-dose aspirin should be closely monitored. In a systemic review, the pooled results of eight randomized clinical trials showed an association between low-dose aspirin use and an elevated risk of intracranial bleeding, with an overall RR of 1.37 (95% CI, 1.13 to 1.66)61. The pooling of data from four randomized clinical trials demonstrated that the strongest relationship was between low-dose aspirin use and subdural or extradural hemorrhage, with an overall RR of 1.53 (95% CI, 1.08 to 2.18). Moreover, it was concluded that Asians were at higher risk than other ethnicities.
There were some limitations of our study. First, patients with HT visiting university hospitals were not included; therefore, it is possible that the prevalence of stroke in hypertensive patients was underestimated. Second, the data were obtained from the Thailand DM/HT study. Therefore, the diagnosis of stroke and comorbidities in this study was based on the ICD-10 codes determined by clinicians. Third, the subclassifications of ischemic and hemorrhagic strokes were not further investigated because of the limited information available from the Thailand DM/HT database. Fourth, the study employed serial cross-sectional surveys; therefore, cause-and-effect relationships could not be identified between the associated risk factors and stroke. Although there were some data missing from the surveys, this was compensated for by the recruitment of a large number of participants from all geographic regions across the country. Hence, the associations between the outcomes and the risk factors were still robust. The strength of our study was that it was a large, nationwide epidemiological study focusing on stroke in Thai patients with HT. Our results can be generalized to the entire country and similar populations.
Conclusion
We identified a constant trend in the prevalence of stroke among Thai patients with HT over the period from 2014 to 2018. Our findings suggested that the management of stroke patients who are covered by the universal health coverage scheme needs to be evaluated. Effective interventions, including promoting smoking cessation, attenuating cholesterol levels, and controlling blood pressure should be provided to all patients with HT to prevent ischemic stroke. Young adults with HT should be more concerned about the risk of stroke. The use of prophylactic low-dose aspirin should be more focused and carefully monitored to prevent hemorrhagic stroke.
Data availability
Data cannot be shared publicly because the data set contains identifying information, additionally, the data belong to the Thailand DM/HT study of the Medical Research Network of the Consortium of Thai Medical Schools (MedResNet); thus, there are ethical restrictions on the data set. Data are available from the Thai National Health Security Office (NHSO), Bangkok, Thailand (contact via sirikorn.k@nhso.go.th) for researchers who meet the criteria for access to confidential data. After permission, the researchers will be able to access the data set and variables at http://www.damus.in.th.
Abbreviations
- HT:
-
Hypertension
- DM:
-
Diabetes mellitus
- DLP:
-
Dyslipidemia
- BMI:
-
Body mass index
- AF:
-
Atrial fibrillation
- OR:
-
Crude odds ratio
- AOR:
-
Adjusted odds ratio
- RR:
-
Relative risk
- 95% CI:
-
95% Confidence interval
References
World Health Organization. Global Health Estimates: Life expectancy and leading causes of death and disability. World Health Organization https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates (2019).
Global Burden of Disease Collaborative Network. GBD Results Tool 2017. Institute for Health Metrics and Evaluation—Global Health Data Exchange http://ghdx.healthdata.org/gbd-results-tool (2018).
Avan, A. et al. Socioeconomic status and stroke incidence, prevalence, mortality, and worldwide burden: an ecological analysis from the Global Burden of Disease Study 2017. BMC Med. 17, 191 (2019).
Kosulwat, V. The nutrition and health transition in Thailand. Public Health Nutr. 5, 183–189 (2002).
Suwanwela, N. C. Stroke epidemiology in Thailand. J. Stroke 16, 1 (2014).
Nilanont, Y. et al. Quality of acute ischemic stroke care in Thailand: a prospective multicenter countrywide cohort study. J. Stroke Cerebrovasc. Dis. 23, 213–219 (2014).
Viriyavejakul, A. et al. Epidemiology of stroke in the elderly in Thailand. J. Med. Assoc. Thai. 81, 497–505 (1998).
Hanchaiphiboolkul, S. et al. Prevalence of stroke and stroke risk factors in Thailand: Thai Epidemiologic Stroke (TES) Study. J. Med. Assoc. Thai. 94, 427–436 (2011).
Turana, Y. et al. Hypertension and stroke in Asia: A comprehensive review from HOPE Asia. J. Clin. Hypertens. (Greenwich) 23, 513–521 (2021).
Yi, X. et al. Prevalence of stroke and stroke related risk factors: A population based cross sectional survey in southwestern China. BMC Neurol. 20, 5 (2020).
Wajngarten, M. & Silva, G. S. Hypertension and stroke: Update on treatment. Eur. Cardiol. 14, 111–115 (2019).
O’Donnell, M. J. et al. Risk factors for ischaemic and intracerebral haemorrhagic stroke in 22 countries (the INTERSTROKE study): A case-control study. Lancet 376, 112–123 (2010).
Feigin, V. L., Norrving, B. & Mensah, G. A. Global burden of stroke. Circ. Res. 120, 439–448 (2017).
Feigin, V. L. & Krishnamurthi, R. Public health strategies could reduce the global stroke epidemic. Lancet Neurol. 9, 847–848 (2010).
Ogunbode, A. M., Owolabi, M. O., Ogunniyi, A. & Ogunbode, O. O. “Weight control, alcohol reduction, smoking cessation, health promotion, exercise and diet (WASHED)”: A mnemonic for lifestyle modification in obesity. Niger. J. Clin. Pract. 18, 831–832 (2015).
Sakboonyarat, B. et al. National trends in the prevalence of glycemic control among patients with type 2 diabetes receiving continuous care in Thailand from 2011 to 2018. Sci. Rep. 11, 14260 (2021).
World Health Organization. ICD-10 ICD-10: International Statistical Classification of Diseases and Related Health Problems—Tenth Revision, Fifth Edition (WHO Press, Geneva, 2016).
NCHS. Adult Tobacco Use Information - Glossary. Centers for Disease Control and Prevention https://www.cdc.gov/nchs/nhis/tobacco/tobacco_glossary.htm (2017).
Gijón, T. et al. Stroke prevalence and risk factor control in hypertensive patients: PP4149. J. Hypertens. 28, e92 (2010).
Silva, E. S., Borges, J. W. P., Moreira, T. M. M., Rodrigues, M. T. P. & Souza, A. C. C. Prevalence and risk factors associated with stroke in hypertensive patients: A hierarchical analysis. Revista de Enfermagem Referência 5, e20014 (2020).
Suwanwela, N. C., Phanthumchinda, K., Suwanwela, N., Tantivatana, J. & Janchai, A. Thrombolytic treatment for acute ischemic stroke: A 2 year-experience at King Chulalongkorn Memorial Hospital. J. Med. Assoc. Thai. 84(Suppl 1), S428–S436 (2001).
Areechokchai, D., Vijitsoonthornkul, K., Pongpan, S. & Maeakhian, S. Population attributable fraction of stroke risk factors in Thailand: Utilization of non-communicable disease surveillance systems. Outbreak Surveill. Investig. Rep. 10, 1 (2017).
Peters, S. A. E., Carcel, C., Millett, E. R. C. & Woodward, M. Sex differences in the association between major risk factors and the risk of stroke in the UK Biobank cohort study. Neurology 95, e2715–e2726 (2020).
Girijala, R. L., Sohrabji, F. & Bush, R. L. Sex differences in stroke: Review of current knowledge and evidence. Vasc. Med. 22, 135–145 (2017).
Mozaffarian, D. et al. Heart disease and stroke statistics-2016 update: A report from the American heart association. Circulation 133, e38–e360 (2016).
Schmidt, R. et al. Estrogen replacement therapy in older women: A neuropsychological and brain MRI study. J. Am. Geriatr. Soc. 44, 1307–1313 (1996).
Wei, J. W. et al. Comparison of recovery patterns and prognostic indicators for ischemic and hemorrhagic stroke in China: The ChinaQUEST (QUality evaluation of stroke care and treatment) registry study. Stroke 41, 1877–1883 (2010).
Venketasubramanian, N. et al. Prevalence of stroke among Chinese, Malay, and Indian Singaporeans: A community-based tri-racial cross-sectional survey. Stroke 36, 551–556 (2005).
Sridharan, S. E. et al. Incidence, types, risk factors, and outcome of stroke in a developing country: The Trivandrum stroke registry. Stroke 40, 1212–1218 (2009).
Marini, C. et al. Stroke in young adults in the community-based L’Aquila registry: Incidence and prognosis. Stroke 32, 52–56 (2001).
Jacobs, B. S., Boden-Albala, B., Lin, I. F. & Sacco, R. L. Stroke in the young in the northern Manhattan stroke study. Stroke 33, 2789–2793 (2002).
Gandolfo, C. & Conti, M. Stroke in young adults: Epidemiology. Neurol. Sci. 24(Suppl 1), S1–S3 (2003).
Griffiths, D. & Sturm, J. Epidemiology and etiology of young stroke. Stroke Res. Treat. 2011, 209370 (2011).
Westover, A. N., McBride, S. & Haley, R. W. Stroke in Young Adults Who Abuse Amphetamines or Cocaine. Arch. Gen. Psychiatry 64, 495–502 (2007).
Shibata, S., Mori, K., Sekine, I. & Suyama, H. Subarachnoid and intracerebral hemorrhage associated with necrotizing angitis due to methamphetamine abuse—An autopsy case. Neurol. Med. Chir. (Tokyo) 31, 49–52 (1991).
Selmi, F., Davies, K. G., Sharma, R. R. & Neal, J. W. Intracerebral haemorrhage due to amphetamine abuse: Report of two cases with underlying arteriovenous malformations. Br. J. Neurosurg. 9, 93–96 (1995).
Fessler, R. D., Esshaki, C. M., Stankewitz, R. C., Johnson, R. R. & Diaz, F. G. The neurovascular complications of cocaine. Surg. Neurol. 47, 339–345 (1997).
Nolte, K. B., Brass, L. M. & Fletterick, C. F. Intracranial hemorrhage associated with cocaine abuse: A prospective autopsy study. Neurology 46, 1291–1296 (1996).
McEvoy, A. W., Kitchen, N. D. & Thomas, D. G. Intracerebral haemorrhage and drug abuse in young adults. Br. J. Neurosurg. 14, 449–454 (2000).
Shen, Y. et al. Association between body mass index and stroke risk among patients with type 2 diabetes. J. Clin. Endocrinol. Metab. 105, 96–105 (2020).
Shah, R. S. & Cole, J. W. Smoking and stroke: The more you smoke the more you stroke. Expert. Rev. Cardiovasc. Ther. 8, 917–932 (2010).
Bhat, V. M. et al. Dose-response relationship between cigarette smoking and risk of ischemic stroke in young women. Stroke 39, 2439–2443 (2008).
Rogers, R. L. et al. Cigarette smoking decreases cerebral blood flow suggesting increased risk for stroke. J. Am. Med. Assoc. 250, 2796–2800 (1983).
Kawachi, I. et al. Smoking cessation and decreased risk of stroke in women. J. Am. Med. Assoc. 269, 232–236 (1993).
Prescott, E. et al. Mortality in women and men in relation to smoking. Int. J. Epidemiol. 27, 27–32 (1998).
Robbins, A. S., Manson, J. E., Lee, I. M., Satterfield, S. & Hennekens, C. H. Cigarette smoking and stroke in a cohort of US male physicians. Ann. Int. Med. 120, 458–462 (1994).
Myint, P. K. et al. Risk factors for first-ever stroke in the EPIC-Norfolk prospective population-based study. Eur. J. Cardiovasc. Prev. Rehabil. 15, 663–669 (2008).
Dagenais, G. R. et al. Impact of cigarette smoking in high-risk patients participating in a clinical trial. A substudy from the Heart Outcomes Prevention Evaluation (HOPE) trial. Eur. J. Cardiovasc. Prev. Rehabil. 12, 75–81 (2005).
Alexander, R. W. Theodore Cooper Memorial Lecture Hypertension and the pathogenesis of atherosclerosis. Oxidative stress and the mediation of arterial inflammatory response: A new perspective. Hypertension 25, 155–161 (1995).
Gyanwali, B. et al. Risk factors for and clinical relevance of incident and progression of cerebral small vessel disease markers in an Asian memory clinic population. J. Alzheimers Dis. 67, 1209–1219 (2019).
Gaciong, Z., Siński, M. & Lewandowski, J. Blood pressure control and primary prevention of stroke: Summary of the recent clinical trial data and meta-analyses. Curr. Hypertens. Rep. 15, 559–574 (2013).
Ariesen, M. J., Claus, S. P., Rinkel, G. J. & Algra, A. Risk factors for intracerebral hemorrhage in the general population: A systematic review. Stroke 34, 2060–2065 (2003).
Cholesterol Treatment Trialists’ (CTT) Collaboration. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet 376, 1670–1681 (2010).
Bloomfield Rubins, H. et al. Reduction in stroke with gemfibrozil in men with coronary heart disease and low HDL cholesterol: The Veterans Affairs HDL Intervention Trial (VA-HIT). Circulation 103, 2828–2833 (2001).
Wolf, P. A., Abbott, R. D. & Kannel, W. B. Atrial fibrillation as an independent risk factor for stroke: the Framingham Study. Stroke 22, 983–988 (1991).
Vanassche, T. et al. Risk of ischaemic stroke according to pattern of atrial fibrillation: Analysis of 6563 aspirin-treated patients in ACTIVE-A and AVERROES. Eur. Heart J. 36, 281–287a (2015).
Glotzer, T. V. et al. The relationship between daily atrial tachyarrhythmia burden from implantable device diagnostics and stroke risk: The TRENDS study. Circ. Arrhythm. Electrophysiol. 2, 474–480 (2009).
Nuotio, I., Hartikainen, J. E., Grönberg, T., Biancari, F. & Airaksinen, K. E. Time to cardioversion for acute atrial fibrillation and thromboembolic complications. J. Am. Med. Assoc. 312, 647–649 (2014).
Healey, J. S. et al. Subclinical atrial fibrillation in older patients. Circulation 136, 1276–1283 (2017).
Gorelick, P. B. & Weisman, S. M. Risk of hemorrhagic stroke with aspirin use: An update. Stroke 36, 1801–1807 (2005).
Huang, W. Y. et al. Frequency of intracranial hemorrhage with low-dose aspirin in individuals without symptomatic cardiovascular disease: A systematic review and meta-analysis. JAMA Neurol. 76, 906–914 (2019).
Acknowledgements
The authors would like to thank staff members of the Department of Pathology and the Department of Military and Community Medicine, Phramongkutklao College of Medicine for their support in completing this Study.
Funding
The authors received no specific funding for this work.
Author information
Authors and Affiliations
Contributions
W.C. developed the concept, and wrote and revised the manuscript. J.C. developed the concept and edited the manuscript. R.R. and M.M. supervised the project. B.S. developed the concept, analyzed the data, and edited the manuscript. All authors contributed and approved the final version.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Chantkran, W., Chaisakul, J., Rangsin, R. et al. Prevalence of and factors associated with stroke in hypertensive patients in Thailand from 2014 to 2018: A nationwide cross-sectional study. Sci Rep 11, 17614 (2021). https://doi.org/10.1038/s41598-021-96878-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-96878-4
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
